
Abstract
Social determinants of health (SDOH) are the conditions in which people are born, grow, live, work, and age that influence health outcomes, and structural and systemic drivers of health (SSD) are the social, cultural, political, and economic contexts that create and shape SDOH. With the integration of constructs from previous examples, we propose an SSD model that broadens the contextual effect of these driving forces or factors rooted in the Centers for Disease Control and Prevention’s SDOH framework. Our SSD model (1) presents systems and structures as multidimensional, (2) considers 10 dimensions as discrete and intersectional, and (3) acknowledges health-related effects over time at different life stages and across generations. We also present an application of this SSD model to the housing domain and describe how SSD affect SDOH through multiple mechanisms that may lead to unequal resources, opportunities, and consequences contributing to a disproportionate burden of disease, illness, and death in the US population. Our enhanced SDOH framework offers an innovative and promising model for multidimensional, collaborative public health approaches toward achieving health equity and eliminating health disparities.
Social determinants of health (SDOH) are the conditions in which people are born, grow, live, work, and age that influence health outcomes. 1 A wide range of SDOH (eg, educational attainment, income, food security, housing affordability, transportation access) have been linked with health inequities,2-4 resulting in a society in which not every person has the opportunity to attain their highest level of health. 5 Whereas SDOH are upstream from health behaviors and health outcomes, they are downstream from structural and systemic drivers (SSD). 6 SSD are the social, cultural, legal, political, and economic contexts that shape and create the conditions of SDOH and daily life.
Historical context is also important when considering SSD. The shared ideologies that lay the foundation for a society’s systems and structures often reflect and uphold the values of those who historically held the most power (ie, socially, politically, and financially) and have been sustained over time by existing societal multisectoral leaders or decision makers.7-11 When these ideologies or values, such as an implicit or explicit preference for one group over another as a result of racism, sexism, ableism, and/or other discriminatory beliefs, are codified into policies or practices, the result often leads to societal systems that create and then perpetuate inequities.12-17 Because such ideologies are built into the system from the start, they wield influence at every level and in every domain, resulting in systemic oppression and marginalization of some groups. Along with acknowledging populations who have been and continue to be disenfranchised by structures and systems in the United States and understanding the historical context responsible for our present societal structures and systems, we must identify upstream solutions that will eliminate the downstream health inequities that are suppressing our societal potential and increasing the societal burden of disease.
In this article, we refer to SDOH as outcomes of the SSD and use SDOH domains to refer to overall themes (eg, housing, transportation, work and economic stability, justice system, education, food system, health system, civic participation, immigration). We use systems to describe the complex, material, social, and functional realities that operate, influence, and organize interconnected societal structures, including the social, group, and institutional roles and relationships, that create the material and social conditions for the people within them. We define structures as the organization of interrelated, social systems into an often invisible societal framework that may support or hinder opportunities as people navigate through these structures throughout their life course. Put another way, systems and structures are macrosocial determinants of health that are based on and influenced by shared ideologies and power hierarchies. We also consider drivers of SDOH as the factors that influence, affect, or contribute to SDOH statuses and markers of SDOH as the indicators or something that serves to identify, predict, or characterize SDOH statuses. Public health and other sectors play a critical role in creating the conditions for equitable, healthy, and full lives, and the need for multisectoral action on drivers of SDOH has been recognized in the literature (eg, for addressing racism through public health action). 18 Therefore, recognizing the importance of societies to create the conditions and structures for all to have equitable, healthy, full lives, we refer to these conditions and structures as vital conditions.19,20
For an example in applying these terminology and definitions described, we considered structures in early education (childcare and/or preschool) from the education domain of SDOH. For early education, the structures include the processes and procedures to (1) provide a facility or location, establish an education or care approach and staffing, gather resources needed to run a facility, and address other logistical and business considerations from the infrastructure and industry perspective and (2) find and apply to the early education centers, get accepted or rejected, pay or attend at reduced cost, attend school, and consider other resources and barriers from the perspective of the community, families, or individuals interested in using the early education services. The systems of early education are how the structures are organized and operated, including where the early education facilities are located; the facility’s quality, staff training, number of staff, resources available, tuition amount, and how the processes to apply are conducted; and whether a child is or can be accepted into or rejected from a school system—along with ideological, social, and cultural ways in which the school will function. However, education facilities differ in many ways (eg, quality, accessibility, diversity and inclusiveness, other education-related factors), and not all children can attend any school. If the goal is for all children to be physically, socially, emotionally, and academically ready for school, some drivers may include household income, local zoning laws, cultural and social norms, and federal, state, and local policies and investments. Potential markers of not being physically, emotionally, and academically ready for school may include living in areas with limited resources and poor infrastructure and areas that have historically been and/or currently are excluded in the application process or other barriers to equitable education access. For example, if access to effective comprehensive early education (ie, with an inclusive and accepting environment, individually tailored educational approaches, exposure to the development of specialized social skills, exposure to diverse art and music, exposure to a range of play and physical activities) is not readily available in areas with limited resources or is expensive, some children would be excluded, thus having an effect on the developmental and educational readiness of a child to enter elementary school. This example demonstrates how exclusion from early education opportunities based on the SSD may not only affect a child’s educational readiness but, with similar SSD in the formal education system (elementary school, middle school, high school, and college), may affect the child’s educational and career path trajectory.
SSD are created by societies and their institutions, where power structures are formed and maintained over generations, creating and sustaining inequities that reinforce racism, sexism, ableism, or other discriminatory ideologies across and within communities—through historical narratives, cultural norms, systems of oppression, social and economic policies, and governance. 21 Although recent SDOH definitions include structural conditions, 1 we consider it important to distinguish SSD from SDOH as traditionally defined. 22 This distinction will allow public health practitioners and others to better assess their relationship with each other, expand the focus of public health interventions, and more readily recognize SSD as a priority to more effectively serve their community. The expansion of public health efforts to include SSD in turn supports what we consider, based on current science and discourse,21,23 a necessary reckoning with historical injustices embedded in SSD and a reimagination of structures and systems to achieve health equity.
Efforts are also needed to shift from a focus on changing individual behavior to a focus on understanding the broader context (SDOH) in which individuals make decisions about their health, including the structural, systemic, and social factors that affect those decisions.24,25 Today, efforts to address the many factors that affect health also include the need to identify and address SDOH and SSD in programs and research to get a broader picture of the health and well-being of communities and societies at large. 26 Even when SDOH are acknowledged, public health has often (implicitly or explicitly) treated health disparities and inequities as given, fixed, or unchangeable characteristics to consider in designing public health interventions.27,28 A focus on SSD may better explain the differential SDOH outcomes in the population that sustain health inequities and disparities. Put another way, although SDOH have been linked to health outcomes,29-34 more research and targeted action are needed in public health, medicine, and science to understand the associations between SSD and SDOH, especially during the life course and longer periods of time. 23 Understanding the clear associations between SSD and SDOH would help not only to identify the structural and systemic changes that would have the biggest effect on population health (eg, policy change) but also to reimagine the upstream structures and systems that would create and sustain better health and well-being for all communities and groups locally and globally.
In 2022, the Centers for Disease Control and Prevention (CDC) adopted an SDOH framework as part of its commitment to eliminate health inequities by addressing their root causes (Figure 1). 35 The SDOH framework includes 6 pillars for public health efforts: data and surveillance, evaluation and evidence building, partnerships and collaborations, community engagement, infrastructure and capacity, and policy and law.36,37 At the center of these pillars are the interconnected social and structural conditions that shape health equity. Using this center circle of CDC’s SDOH framework, we propose rooting the SSD that identify, assess, and measure structural and social conditions. To achieve health equity, public health efforts would benefit from a better understanding of the SSD that drive SDOH and affect the health of our communities both locally and globally. Our model aims to assess the interrelationships between societal structures and systems and their effect on SDOH and health outcomes. This article did not involve human or animal participants or include any data sources other than referenced literature and is not considered research based on regulation 45 CFR 46 from the US Department of Health and Human Services Office for Human Research Protections; therefore, institutional review board review was not required.

Methods
Proposed SSD Model
Our proposed SSD model highlights the multidimensional construct of structures and systems (Figure 2). For our model, we expanded and integrated concepts from the social-ecological model of health, 38 the World Health Organization SDOH framework, 1 and the National Institute on Minority Health Disparities research framework. 39 Although we included most of the concepts from these influential frameworks in our proposed SSD model, for our SSD model, we also acknowledged that the health effects that occur over time, at different life stages, and across generations (eg, weathering hypothesis40-43) are critical contributors to an individual’s or community’s experience. We recognized the unequal resources, opportunities, and consequences to the structures and systems in place for any given social determinant that influences the distribution of health and well-being of a population at different life stages (in utero, early and late childhood, early and late adulthood, and continuing to the subsequent generations through epigenetic effect44,45). Furthermore, we recognized that the unequal resources, opportunities, and consequences to these multidimensional systems and structures are accumulated throughout the life course 23 and can extend to subsequent generations (multigenerational). For our SSD model, we considered each dimension as distinct but intersecting with other dimensions in complex ways that may not be solely linear, nested, or hierarchical. As such, our SSD model is intentionally void of arrows and hierarchy in the relationships between dimensions, and the confluence of all dimensions is the manifestation of contemporary society.
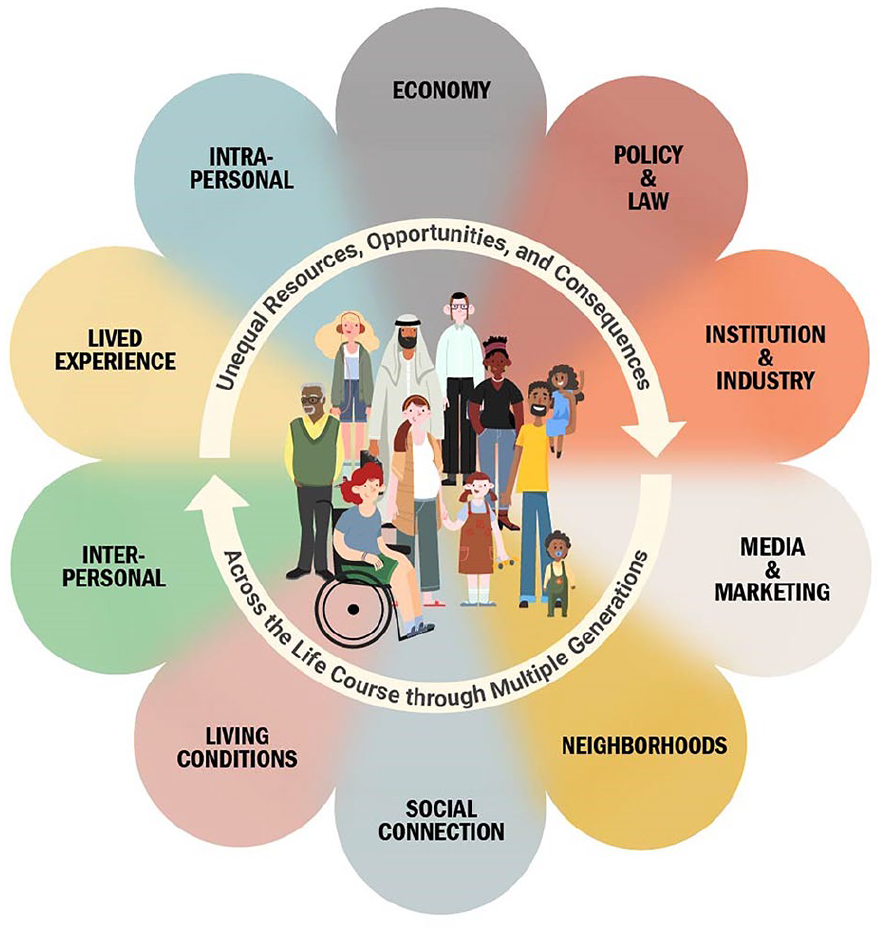
The 10 dimensions and concepts contributing to inequities from the proposed structural and systemic drivers model.
There are 10 dimensions in our SSD model. The economy dimension considers the microeconomic and macroeconomic relationships with any SDOH domain. Through policy, ordinances, and legal systems, societal systems and structures can be sustained or modified. The policy and law dimension considers the creation and differential enforcement of laws and policies toward individuals and communities historically and currently, specifically those policies that have codified racism, sexism, and ableism, along with other discriminatory ideology, into societal and policy structures. 46 For any particular SDOH domain, organizations (institutions, eg, federal, state, and local agencies; private corporations; nonprofit organizations; other organizational entities) and economic activities (industries, eg, transportation industry, housing industry, food industry, other SDOH domain–specific industries) actively participate in the systems and structures in place. The institution and industry dimension encompasses these roles and activities and highlights the reliance on and influential bidirectional relationship between institutions and industries within systems and structures. The media and marketing dimension includes the influence of narratives in all their forms on systems and structures. All forms of media (eg, social media, news outlets, entertainment, all other forms of information or value sharing) are used to develop, shape, and maintain narratives, ideologies, and stories. Historical and ongoing narratives influence social norms, common belief systems, and cultural practices. Marketing leverages and invests in narratives to advertise, educate, and build relationships that sustain existing structures and systems. The neighborhoods dimension focuses on the physical built environment of neighborhoods and communities, including environmental exposures and the population that resides there. The social connection dimension focuses on the community level and considers all the activities, programs, and resources available in the community and the population’s participation in them. Living conditions focuses on the household, family, or people level and their interaction with the physical, built environment (the housing, neighborhood, educational, and financial conditions affecting the daily life of households, families, or people). The interpersonal dimension encompasses the quality of relationships in the familial, community, school, work, and social settings that affect the quality of life. Lived experience is personal knowledge and consciousness about the world gained through differential exposures and consequences from all the aforementioned dimensions, with unequal disadvantages or advantages that have differential effects on health. The intrapersonal dimension reflects the whole person’s well-being (including the 8 dimensions of wellness47,48: social, emotional, spiritual, intellectual, physical, occupational, financial, and environmental), which is shaped by a person’s lived experience.
Operation of the Proposed SSD Model in Housing
To demonstrate the operation of the proposed SSD model, we used the housing domain, identifying housing-related aspects of each SSD dimension from the model (Table and Figure 3). Although we could not cover the full breadth and depth of the literature or historical context related to societal housing SSD, we considered that prolonged historical policies and practices contribute to housing-related inequities. For example, redlining and racial segregation have contributed to disparities and inequities for many communities across different intersections in the United States. 49 However, we will walk through each SSD dimension by applying a housing focus and discuss historical implications afterward.
Dimensions of the proposed structural and systemic drivers model, developed to broaden the Centers for Disease Control and Prevention’s 2022 social determinants of health framework, with applied examples from the housing domain
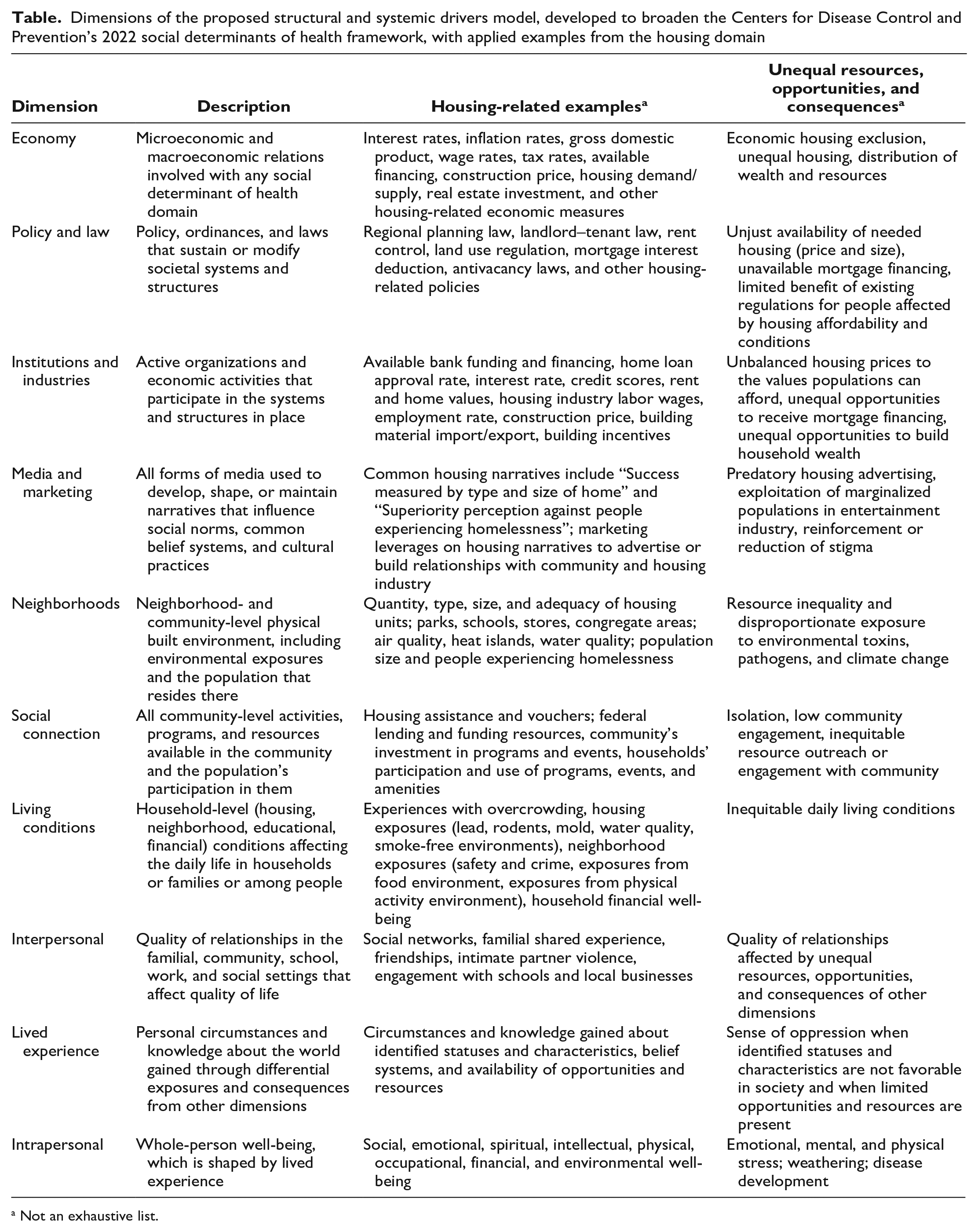
Not an exhaustive list.
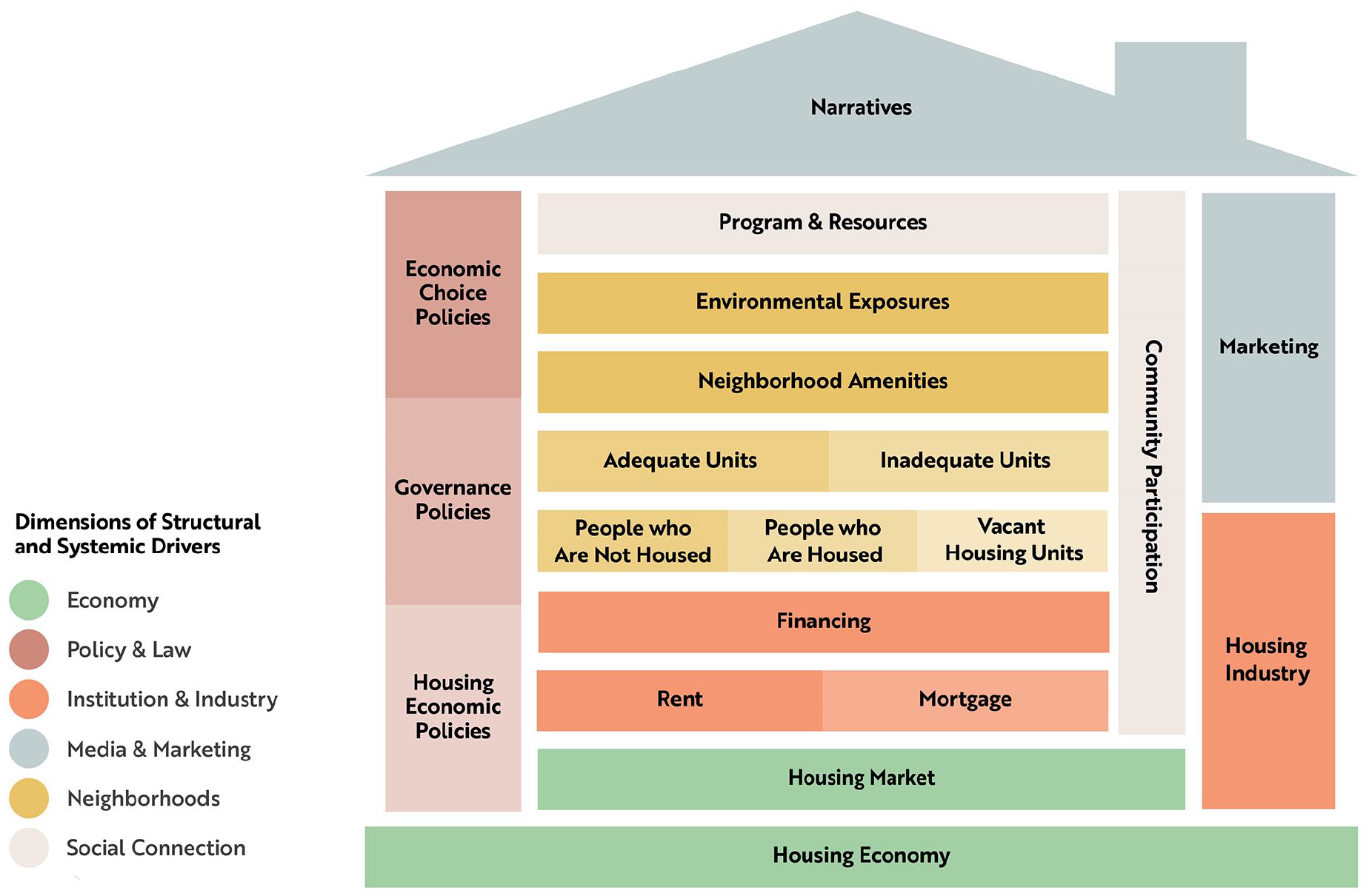
An example of the proposed structural and systemic drivers model application using the housing domain that illustrates the multidimensionality of the drivers. All dimensions represented in the housing domain example contribute to the living conditions, interpersonal, lived experience, and intrapersonal dimensions.
For the housing economy dimension, we considered that the housing market and housing prices are influenced by microeconomics and macroeconomics.50,51 From the microeconomic perspective, the housing market can be affected by housing demand, housing supply, real estate investment, mortgage financing, and real estate agencies, all of which influence housing prices. 51 Housing prices are influenced by many components of macroeconomics, including inflation rate, interest rate, wage rate, employment rate, availability of funds lending institutions have for financing mortgages, gross domestic product, and business cycles. 50
For the housing policy and law dimension, we considered a range of policies and laws that address economic choice for people (eg, federal rental assistance program, mortgage interest deduction, consumer protection against predatory lending, other economic housing-related laws for people or consumers), governance (eg, regional planning laws, land-use regulations, landlord–tenant laws, other housing governance laws), and housing economics (eg, rent control, low-income housing tax credit program, other laws affecting housing corporations) at different levels (eg, federal, state, local, private sector). 52 We also considered that creation and enforcement of policies and laws related to safe and healthy housing (eg, code enforcement, evictions, other housing policies and laws as related to safety) disproportionately affect populations that are socially or economically marginalized, creating racism, sexism, ableism, and other discriminatory policy structures, which play a role in determining equity in housing and related health outcomes.53-55
We considered that some housing institutions and industries include the home financing industry (eg, availability of funds or financing from institutions, home loan approval and interest rates, credit scores, rent values, other financing considerations), the home-building industry (eg, housing industry labor factors and employment; construction prices, market values, and profit margins; building material imports and exports, among other building considerations), and real estate and property management agencies (eg, listing prices, advertisement, other real estate service considerations).
For the housing media and marketing dimension, we considered that all forms of media (social, news outlets, and entertainment, including film, television, sports, and music) develop or sustain housing-related narratives, such as success being measured by the type or size of home, negative perceptions of people experiencing homelessness, and perceived cultural and societal norms about housing or home environments. In addition, we considered that marketing for housing is not limited to advertisement but also includes educating people on housing and financing options, building relationships with community and housing industries, and leveraging and investing in housing narratives. The media and marketing dimension is the most proximal to existing housing-related social norms and common belief systems.
For the neighborhoods dimension related to housing, we considered that the housing built environment includes the quantity and characteristics of housing units, including distribution of type (eg, apartment, condominium, single-family home, housing shelter, other types of housing), size (square footage and number of bedrooms), and structural adequacy of housing units or shelters; the neighborhood features that influence housing cost (schools, parks, stores, congregate areas [eg, town centers, community centers, other gathering areas]); the disproportionate neighborhood-level environmental exposures related to different housing values between areas; and the population (eg, number of households, distribution of household sizes and structures, household income distribution, people experiencing homelessness, other population characteristics related to housing considerations) residing in a neighborhood or community.
For the social connection dimension related to housing, we considered housing programs and resources available (eg, housing assistance and vouchers, subsidized housing, housing resources from community-based organizations, federal house lending and funding, communities’ investment in activities and events for residents, other programs or resources for housing), participation in these programs and resources by the population, and the use of existing neighborhood features in the built environment (eg, parks, libraries, schools, other neighborhood features).
For the living conditions dimension related to housing, we considered the inclusion of the disproportionate conditions that affect health and well-being from housing issues experienced by households, families, or people, including overcrowding (number of people per square foot or number of bedrooms, number of households per city block or square mile, number of people in homeless shelters [with respect to crowding]), other exposures relating to the adequacy of housing units or housing shelters (eg, lead, rodents, mold, water quality, other toxin exposures), neighborhood-related exposures experienced (eg, safety and crime, food environment, physical activity environment, other experiences related to the neighborhood), and the housing effect on financial well-being.
We posit that the dimensions of interpersonal, lived experience, and intrapersonal connect with all the SDOH domains. In our housing example, the interpersonal dimension may include the quality of relationships between landlords and tenants, neighbors, households and schools, and households and local businesses, and other relationships. The quality of these relationships also affects other SDOH domains (eg, education, employment/economic stability, food system, justice system, other domains). Similarly, the lived experience dimension and intrapersonal dimension relate not only to housing but also to other SDOH domains.
In our SSD model, the SSD dimensions are not just linear, hierarchical, or nested; rather, the SSD dimensions are multidimensional and influence each other in various ways. Using the housing example, we can begin to understand the intersectional and multidimensional nature of these systems and structures (Figure 3). Current housing units in our society may be in either an adequate or inadequate condition for healthy habitation. Our reference to adequate housing condition is the condition for optimal health for all, meaning that the inhabitant is not exposed to anything associated with adverse health outcomes. Some housing units are occupied, some housing units are vacant, and some people may be experiencing homelessness. Programs and resources may be available to help address housing-related issues, including experiencing homelessness, assisting households into housing units, or improving the habitability of vacant units. We can then begin to consider the financial aspects of housing, such as the microeconomics and macroeconomics of the housing market that influence home values. Home values affect a person’s ability to obtain financing for housing ownership and the amount of their housing payment (mortgage or rent).56,57 In addition, both neighborhood features and environmental exposures contribute to housing value.58,59 However, sustaining these systems and structures requires community participation in financial and economic structures, the inhabiting of housing units, the use of programs and resources, and engagement in neighborhood features and the environment. To maintain this level of community participation, narratives or social norms are continuously being broadcasted in multiple formats (eg, nuclear family structures, family planning, life-course milestones that may influence individuals’ or groups’ views on living and housing arrangements). 60 The housing industry depends heavily on housing economics and the narratives and social norms that continue to sustain community participation. 61 Marketing in housing is interconnected with the economy (eg, microeconomics and the role of real estate agencies), the housing industry (eg, employment, purchasing, sales), and the narratives or social norms related to housing. 62 Housing policy and laws are highly influenced by industry, marketing, narratives, and community participation in the housing programs; resources available; and the existing systems and structures related to housing.63-68 Housing affordability and availability greatly influence living conditions, quality of interpersonal relationships, lived experience, and intrapersonal risks for disease.69-72
Societal and system structures have effects across the life course and across generations. For example, living in areas with limited access to grocery stores, recreation facilities, and walkability for an accumulated amount of time contributes to the development of adverse health outcomes, such as hypertension, type 2 diabetes, and cardiovascular disease. 73 Experiences and exposures to these structures can have differential effects at different life stages, such as lead paint exposure among infants and children. Because of their size, proximity to ground dirt and indoor dust, and oral exploratory and pica behaviors, infants and children experience a higher risk of lead paint exposure than adults do. 74 Furthermore, among low-income families, infants and children tend to have higher blood lead levels than their higher-income counterparts do,75,76 most likely because of housing conditions experienced.77,78 Children of parents who pay mortgages leading to homeownership may benefit from the accumulation of familial housing wealth compared with children of rent-paying parents who may experience an increased exposure to psychological stress, depression, and other consequences of housing instability and quality, 79 and these exposures may be in addition to any of the potential epigenetic intergenerational transmission exposures.44,45
The current societal structures and systems contributing to housing inequities are, in part, the result of prolonged historical laws, policies, and practices. For example, consider the implementation of 2 key US housing laws: the National Housing Act of 1934, 80 which established the Federal Housing Administration (FHA), and the Servicemen’s Readjustment Act of 1944, 81 or G.I. Bill. After the Great Depression, the FHA was created to revitalize a struggling housing industry with goals to increase the ease of financing the purchase of a home, to improve housing standards, and to bring jobs back to the home construction industry. The G.I. Bill was enacted to help veterans prosper after World War II (WWII) and included a component that enabled WWII veterans to receive low-cost mortgages and low-interest loans, resulting in more than 2 million home loans for veterans between 1944 and 1950. 82 Both laws created an unprecedented opportunity for homeownership in the United States—for White families but not for Black or African American families. FHA regulations stipulated that, by law, FHA loans could only be sold to White families, at least until 1968 with the passage of the Fair Housing Act.83-85 Although the G.I. Bill did not explicitly state that Black veterans were ineligible, the bill was purposefully drafted to give enormous power to local officials, allowing implementation to complement existing discriminatory Jim Crow laws.84,86 Homeownership is a known vehicle for the generation of wealth and financial stability; through these laws, White families were afforded financial gains beyond the opportunities available for Black families. The laws allowed for a major disparity in wealth to grow, and subsequent policies coupled with racist practices would further that divide. 87
Many examples of repeated systemic race-specific exclusion or other forms of harm exist in the United States, both historically and contemporarily (ie, education segregation, redlining, medical testing, policing procedures, voter disenfranchisement, and other race-specific exclusion practices). 12 Although the more overtly discriminatory policies have been repealed or rendered illegal over time, policies are often still written in race-neutral language that nonetheless maintain a status quo of inequitable practices. 88 Other groups (including people living with disabilities, 89 lesbian, gay, bisexual, transgender, queer, and questioning [LGBTQ+] individuals90,91) have also experienced various forms of such systemic exclusion or harm. Although the current overall culture has become more tolerant and inclusive than historically, many of our systems and structures have not advanced at the same pace, allowing for upstream, oppressive forces (and ideologies) to continue to cause harm—particularly as we continue to focus primarily on downstream solutions.
Recommendations
From the perspective of the proposed SSD model, public health efforts have often focused on the dimensions from intrapersonal to neighborhoods (eg, infectious exposures, socioeconomic status, bullying, food security, program evaluation, air quality), including the built environment. However, the dimensions from media and marketing to economy present opportunities to bolster public health efforts (eg, reframing harmful narratives promoting false information, redirecting divisive narratives toward more inclusive messaging). Other fields, such as anthropology, sociology, and psychology, have researched many of these dimensions and can serve as models for public health.92-94 Importantly, all these dimensions contribute to the disproportionate burden of disease and illness in the population and can arguably be considered public health work.
Aside from each SDOH domain consisting of multidimensional systems and structures, the domains themselves intersect with each other (eg, connections between the housing and environment domains). To effectively address health inequities, we need to better understand how these SDOH domains and multidimensional SSD fit together. Through these efforts, we can identify the constructs of a system and structure that would not only have the biggest effect for a specific domain of SDOH but also cascading effects on other overlapping domains. For example, safeguarding household incomes aligned with costs of living would affect not only the domain of work and economic stability but also housing, transportation, the justice system, education, the food system, and other domains. Therefore, we need to understand the association between each of the SSD dimensions and their magnitude of effect on SDOH outcomes to ensure that every person can attain their highest level of health. One option for assessing, measuring, and understanding SSD relationships (with each other and with SDOH and health outcomes) is by incorporating nontraditional data sources and innovative data science techniques into the public health field. For example, for housing SSD, along with health data, we could include housing-related media narratives, Home Mortgage Disclosure Act data,95,96 housing assistance data, economic data (interest rates, bank assets), and congressional budgetary authorization in analyses. In addition, leveraging data science modeling techniques from fields such as economics, engineering, or agriculture would expand on the traditional analytical approaches in public health. This work should be guided and built in partnership with communities and individuals affected by health disparities and inequities.
Public Health Practice Implications
Embedding the SSD model within the core of CDC’s SDOH framework provides a feasible approach to assess the effectiveness of the framework’s 6 pillars in achieving health equity. Although we focused on a housing example, our model is scalable to all SDOH domains and applicable to other frameworks.
For example, similar to the SSD model, the Health in All Policies approach acknowledges that health is shaped by myriad factors beyond health care and the traditional scope of public health and highlights the importance of including health considerations in all policy decisions. Health in All Policies includes 5 essential elements: promoting health and equity, supporting intersectoral collaboration, creating co-benefits for multiple partners, engaging partners, and creating structural or process change.97,98 Health in All Policies highlights and supports the need for multidimensional collaboration or engagement among public health practitioners, communities, and community-serving organizations and partnerships across housing, transportation, education, criminal justice, and employment, to name a few.
Frieden’s Health Impact Pyramid 99 is another framework for improving public health that acknowledges the importance of SSD to public health outcomes. The Health Impact Pyramid illustrates that interventions with the greatest potential effect to the population are those that address the base level of the pyramid (socioeconomic factors), which include SSD and SDOH. Although the implementation of interventions at every level (from top to base: counseling and education, clinical interventions, long-lasting protective interventions, changing context for individuals to make healthy decisions, and socioeconomic factors) of the pyramid is ideal, focusing on interventions closer to the foundation of the pyramid requires less individual effort yet can yield greater, more equitable, and more sustainable benefits to public health than current public health experience can. Interventions at upper levels of the pyramid are focused on individual behavior change, have limited population effect, and may unintentionally reinforce or increase health disparities if the interventions are not universally and effectively applied. Therefore, increasing the population- or structural-level effect is economical and helps decrease the onus on individuals to succeed at achieving good health in contexts often built to impede, rather than support, their success.
Public health has made important efforts toward acknowledging health inequities (ie, avoidable and unfair disparities), individual social needs, and, to some extent, SDOH. Although we have become adept at measuring the magnitude of health disparities, gaps remain in our knowledge and understanding of the SSD of health inequities operating in the United States. Our model shifts the approach from one that addresses health inequities to one that examines the interconnection between traditional focus areas of public health and linkages to other societal dimensions, such as media and marketing, institutions and industry, and economy. Optimal approaches to public health consider the multiple dimensions and the ways they intersect. Application of the proposed SSD model to the housing domain demonstrated how SSD affects SDOH through multiple mechanisms that may lead to unequal distribution of health outcomes in communities. Our approach does not negate the important work of establishing how racism, sexism, ableism, and other forms of oppression are expressed in these dimensions; indeed, it opens up opportunities to explore pathways in collaboration with multiple sectors, communities, organizations, and groups that have been historically and are currently disproportionately affected by SSD, thereby advancing our understanding and efforts toward sustainable improvements in public health. Acknowledging the importance of SSD, quantifying their contribution to SDOH and health outcomes, and incorporating multidimensional, collaborative approaches into public health practice are important next steps toward achieving health equity and eliminating health disparities.
Footnotes
Disclaimer
The findings and conclusions in this article are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention or any other entity of the US government.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.