
Abstract
Refugee-background communities have been a significant part of Aotearoa New Zealand’s multicultural population for decades. Despite the documented relevance of communication for newly arrived refugees, local reports over the years have found significant gaps in effective communication between culturally and linguistically diverse (CALD) populations and public service providers. This article presents findings from a study exploring interpreting in refugee contexts (IRCs) in Aotearoa New Zealand, along with the applicability and suitability of trauma-informed interpreting as a positive approach to interpreting services. Relying on interviews with refugee-background clients, the research outlined below suggests that language barriers and negative experiences when using language assistance services are often (re)settlement stressors for this population. The study further found challenges related to interpreter availability and acceptability for refugees, which were linked to client dissatisfaction and potential (re)traumatisation. The detailed discussion of findings leads to a call to embed trauma-informed principles in good practice guidelines for all professionals, including interpreters, working with potentially traumatised clients. To that end, it is imperative that interpreter education programmes provide trauma-informed training and that public service authorities ensure the use of qualified language professionals.
Keywords
1. Introduction
Aotearoa New Zealand 1 is a “superdiverse” country (Chen, 2015), with 27.4% of its population born overseas, as shown in the latest national census (Statistics New Zealand, 2019). This diversity manifests in daily life, with over 160 ethnic groups making up a multicultural and multilingual society (Statistics New Zealand, 2020). To ensure access to essential services for people with English as a second language, lawmakers recognised the right to communicate effectively with public service providers in several provisions (Bill of Rights Act, 1990; Health and Disability Commissioner Regulations, 1996; Immigration Act, 2009).
However, several publications have documented communication gaps in language support for migrants and refugees (e.g., Ho et al., 2000; Ministry of Business, Innovation and Employment, 2016; Shrestha-Ranjit et al., 2020). Continued reports have identified problems related to the availability and uptake of qualified interpreters in healthcare and other settings. Moreover, controversial solutions to bridge the language gap include the use of bilingual staff, family members, and even children (Gray, 2019; Seers et al., 2013).
In response to such reports, the government developed the Language Assistance Services programme. The project—undergoing implementation at the time of writing—seeks to improve access to language support for culturally and linguistically diverse (CALD) clients and ensure the use of qualified interpreters across government agencies. Nevertheless, a lack of consultation with migrant and refugee groups in the development and implementation of the project challenges the suitability of the service for vulnerable and potentially traumatised clients. This gap in available knowledge is further mirrored by the scant number of studies by local scholars relying on the perspectives of interpreting service users (e.g., Marianacci, 2022).
This article relies on data collected as part of a larger research project to explore the views and experiences of refugee-background clients concerning their communicative needs to access public services and integrate successfully into New Zealand society. The data used for this publication comprise eight semi-structured, episodic interviews (Flick, 2018) conducted with refugee-background clients who had previously relied on interpreters to communicate with public service providers. The coding principles of grounded theory (Charmaz, 2014) were applied to the data to find emerging themes, as explored in the relevant methodology section.
Section 2 details the pathways allowing the arrival of refugees to Aotearoa New Zealand and the differences between such refugee-background groups. Subsequently, Section 3 reviews the literature concerning forced migration and the experience of flight, as well as the role of trauma-informed interpreting in this context. The study’s method and findings are discussed in Sections 4 and 5, respectively. Finally, Section 6 provides conclusions and implications for future research and policymaking.
2. The New Zealand refugee system
The arrival of refugees in Aotearoa New Zealand began after World War II. However, as in other countries, policy in this regard has been deeply influenced by administration changes and tendentious statements by high-profile politicians (Beaglehole, 2013; Spoonley & Bedford, 2012). From a legal perspective, the country is a signatory of the two primary international instruments governing forced migration, namely, the 1951 Convention relating to the Status of Refugees, and its 1967 Protocol. In addition, since 1987, the government joined the United Nations High Commissioner for Refugees (UNHCR) resettlement programme to receive refugees from different locations worldwide. In effect, this resulted in two broad and distinct refugee groups, namely “quota refugees” and “refugee status claimants” (asylum seekers). 2
Quota refugees are the largest group of arrivals, with a current allocation for UNHCR resettlement of 1,500 refugees per year 3 (New Zealand Government, 2018). The programme seeks to assist refugees whose status has been previously recognised by UNHCR and who experience high vulnerability due to their circumstances (e.g., women, elderly, disabled persons). Moreover, it is estimated that 86% of refugees under UN mandate in urgent need of resettlement are trauma and/or violence survivors (UNHCR, 2021).
Conversely, refugee status claimants may arrive in the country on various visas and subsequently lodge a refugee or protection status claim before a competent local authority (Immigration New Zealand, 2015). The claim is assessed by an immigration official in relation to the 1951 Refugee Convention, and in the event of a successful outcome, claimants are recognised as “convention refugees.” Several publications have identified notable and unjustified differences between quota refugees and refugee status claimants, mainly regarding social support and legal status (e.g., Bloom & Udahemuka, 2014; Human Rights Commission, 2017; Marlowe, 2021). Such differences result in limited access to social services, including language support, for refugee status claimants, effectively discriminating against this group and adding to their settlement ordeal. For example, due to their exclusion from the quota settlement programme, claimants cannot readily access mental health support and other critical services, and must instead rely on non-government services, which lack a budget for interpreting support (New Zealand Red Cross, 2021).
Figure 1 compares processes and support available for quota refugees and refugee status claimants. Other groups arriving under family reunification or community-sponsored programmes are not included in this overview, as their entitlements resemble those of quota refugees.
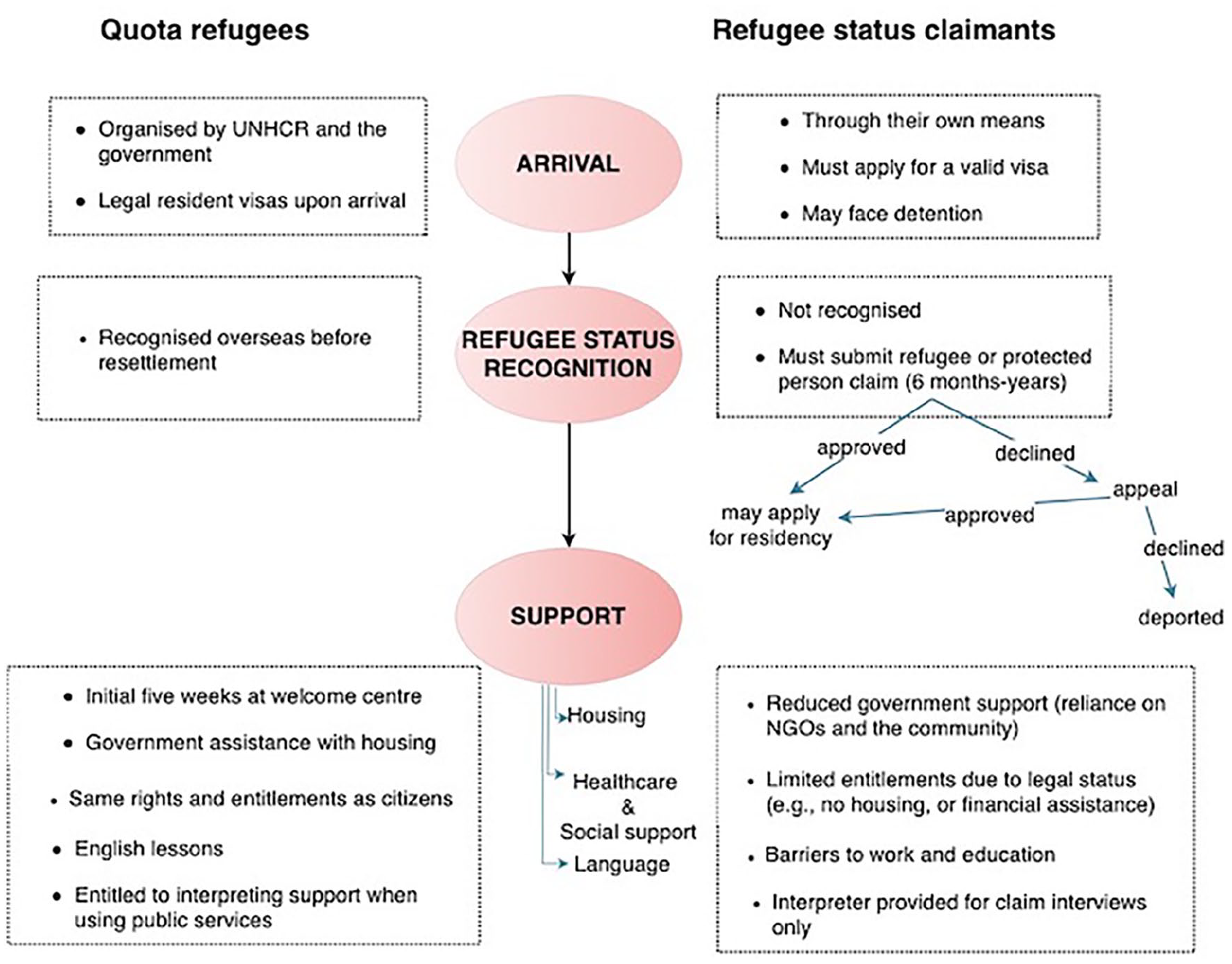
Comparison of Available Processes and Support for Refugees.
3. Trauma in refugee (re)settlement and intercultural communication
The prevalence of trauma in work with refugee-background populations has been discussed by international scholars from such diverse fields as healthcare, social sciences, psychology, and translation and interpreting studies (e.g., Bambarén-Call et al., 2012; Berthold & Fischman, 2014; Poole & Swan, 2010). Refugees often experience traumatic events in their country of origin or during flight, including loss, separation, and sometimes even abuse (Carswell et al., 2011; Kotovicz et al., 2018). Adding to this ordeal, resettlement in a foreign country poses new challenges related to language and communication, adaptation to a new culture and system, lack of support, and so on. For refugee status claimants, the uncertainty of the claim process, lack of access to essential services and sometimes detention upon arrival have been indicated in local reports as added stressors that could lead to (re)traumatisation (Marlowe, 2018; Ministry of Health, 2012).
Trauma is a broad term that refers to a psycho-emotional reaction resulting from “violence, traumatic experiences, abuse, neglect, loss, disaster, war and emotionally harmful experiences” (Substance Abuse and Mental Health Services Administration [SAMHSA]’s Trauma and Justice Strategic Initiative, 2014, p. 2). It is subjective and may manifest differently and at various times in each person, yet many scholars suggest a higher presence among displaced people, including refugees (Bhugra et al., 2010).
The prevalence of trauma among refugees and other vulnerable populations has led to a new service provision paradigm which recognises trauma and seeks to protect clients and service providers. In the fields of healthcare and mental health, for example, there is an increasing awareness of trauma-informed care practices that “enhance the quality of services to trauma survivors” (Bancroft, 2017, p. 198). Specifically, trauma-informed care represents client-centred services that understand the potential history and effects of trauma and promote client autonomy (e.g., Migrant & Refugee Women’s Health Partnership, 2019). While not all displaced people may suffer or present trauma symptoms, studies suggest that professionals who work directly with refugees should receive trauma training to provide adequate support (e.g., Briggs, 2012). Unfortunately, trauma-informed care remains mainly restricted to the healthcare sector (Donaldson et al., 2018).
In relation to language support, research conducted in the United States by Bambarén-Call et al. (2012) underscored gaps in interpreters’ preparation to work with vulnerable populations, often leading to professional stress and client disempowerment. This report was then used to develop the most comprehensive and seminal trauma-informed interpreting material to date, undertaken by one of the researchers in the initial project (Bancroft et al., 2016). Trauma-informed interpreting is thus considered a new interpreting paradigm that can both improve service provision and enhance the interpreters’ working experiences (González Campanella, 2022).
Trauma-informed interpreting combines elements that seek to empower traumatised clients and protect the interpreters from experiencing adverse psycho-emotional effects due to their exposure to client trauma (Crezee et al., 2011; Valero-Garcés, 2015). An understanding of refugee backgrounds, awareness of the specific needs of traumatised clients, controlled empathy, and self-care techniques are all part of trauma-informed interpreting practice. It is thus essential for interpreters working with vulnerable and traumatised populations to ensure, among other things, the autonomy of the communicative parties (client and service provider), the transparency of the information conveyed, and a non-judgemental, unbiased attitude. Interpreters who lack these skills may inadvertently and even with good intentions (re)traumatise refugee clients (Bancroft et al., 2016).
Owing to the incipiency of the approach (Bancroft, 2017) and its general restriction to healthcare services, trauma-informed interpreting remains “a neglected aspect of interpreter education and professional development” (Tipton & Furmanek, 2016, p. 106). No studies have been conducted to date portraying the impact or benefits of trauma-informed interpreting on service provision. Nevertheless, increasing calls from experts to provide culturally appropriate, trauma-informed services to vulnerable populations, including refugees, suggests a gap in best practice awareness (Miller et al., 2019).
Despite the abovementioned new government programme directed at improving and standardising interpreter training in Aotearoa, policy and emerging interpreter training opportunities continue to disregard this key area of knowledge. Specifically, there are no opportunities for dedicated trauma-informed interpreting training at the time of writing.
Based on the above discussion and the gaps identified in awareness of trauma-informed support in refugee contexts in Aotearoa New Zealand, I designed a research project to explore the provision of language support to refugee-background clients through the lens of trauma-informed interpreting. The remainder of this article discusses the study in relation to the data collected from a group of refugee-background clients and their experiences accessing public services upon resettlement.
4. Method
The findings presented in this article are part of a doctoral research project on interpreting in refugee contexts (IRCs) in Aotearoa New Zealand. 4 The qualitative case study (Thomas, 2016) relied on the insights shared by the various parties in the interpreter-mediated encounter, that is, interpreters, refugee-background clients, and service providers. In addition, other key stakeholders, such as policymakers and interpreting service coordinators also participated in the study. The resulting thesis presents the views and experiences of the various participants regarding interpreting services in Aotearoa New Zealand. Findings from the interpreter group have been previously published elsewhere (González Campanella, 2022).
The encompassing study was guided by two research questions. The first question sought to explore the key features of interpreting support for refugee-background clients in the local context. Then, a second research question focused on the participants’ perceptions and experiences, which were analysed in relation to trauma-informed practices.
The findings presented in this article result from a co-construction of knowledge with eight refugee-background participants through semi-structured interviews. Owing to the intrinsic vulnerability of the refugee-background clients group, participants could not be contacted directly. Rather, 11 organisations working with refugees were identified and contacted to act as gatekeepers, providing information about the research project to the clients, and facilitating the researcher’s contact details if they wished to participate. Unfortunately, only three organisations agreed to collaborate, which significantly impacted access to the community. The challenges of collaboration between academia and non-governmental organisations (NGOs) working with vulnerable populations have been documented by other authors (e.g., McAreavey & Das, 2013) and warrant a deeper reflection into academic requirements, such as standardised ethics approvals, to truly meet the needs of the community.
Despite the reduced number of participants, data were not limited to a single ethnic population. Table 1 presents participants’ varied backgrounds, languages, and time in the country since resettlement. To prevent participant identification, demographic information was limited to these three categories.
Participants’ Demographics.
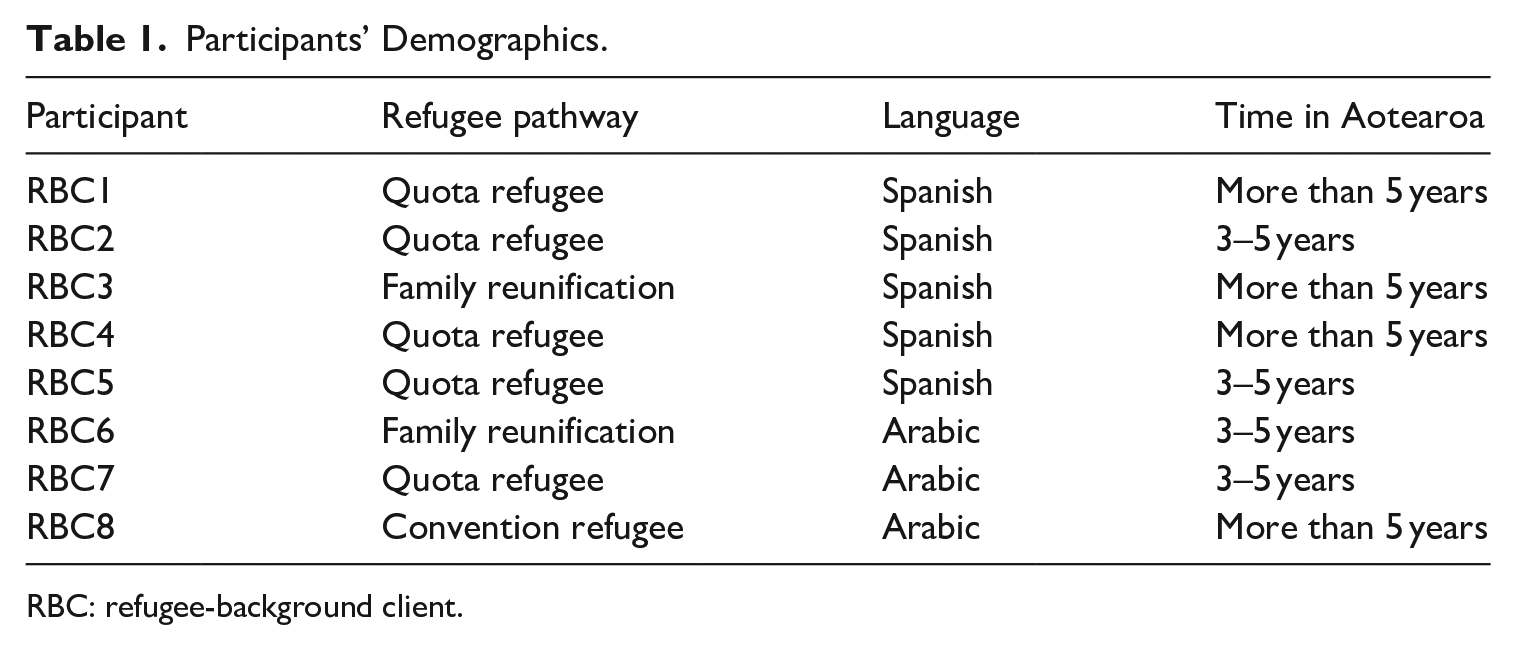
RBC: refugee-background client.
To enhance trust, interviews were conducted at a place designated by participants and followed a conversational style without fixed questions. Participants were asked to narrate their experiences communicating with service providers in Aotearoa New Zealand, and their use of interpreters whenever applicable. Follow-up questions arose from the information offered by each participant, and the interviews always ended with an opportunity to comment freely on any topic relevant to the participant. It was paramount in the study design to ensure that refugee-background participants felt comfortable and understood their rights in relation to the study. Therefore, interviews were conducted only in English or Spanish—two languages spoken by the researcher—to reduce the need to introduce third parties. The recordings were transcribed and translated, when appropriate, by the researcher. 5 The data were analysed using NVivo 2020, following the coding principles of constructivist grounded theory, including initial and selective coding (Charmaz, 2014).
5. Findings and discussion
This section explores the compounded difficulties of (re)settlement in a foreign language. It illustrates the experience of communicating and accessing interpreting services as a refugee in Aotearoa New Zealand and the role of trauma-informed care in this context. The salient theme suggests the ordeal of creating a new life in a new country, significantly increased by the difficulty in communicating in the predominant language and the ongoing risks of (re)traumatisation. The impact of communication barriers on a vulnerable population (see Section 5.1), the critical role of language support (see Section 5.2), the negative experiences using interpreters and the resulting mistrust (see Section 5.3), and desired interpersonal skills for interpreters (see Section 5.4) are explored below.
The emerging theme from the interviews with refugee-background clients relates to the myriad of personal, social and cultural challenges of (re)settlement in Aotearoa New Zealand, generally increased by the communication gap and the need for language assistance to access services. The participants expressed varied views regarding the type of language support that they expected. In addition, problems encountered in accessing or using interpreters sometimes led participants to rely on ad hoc support.
As summarised in Figure 2, the present study reinforced the emotional impact of acculturation and language barriers on refugee-background groups. The communication barrier exacerbates the need for language support in this context. However, ongoing problems with interpreter availability and acceptability can increase the ordeal for refugees needing to communicate effectively with service providers. Such experiences, combined with conflicting views about the skills desired in their interpreters, may lead clients to rely on unqualified language assistance, ultimately increasing the emotional risk.
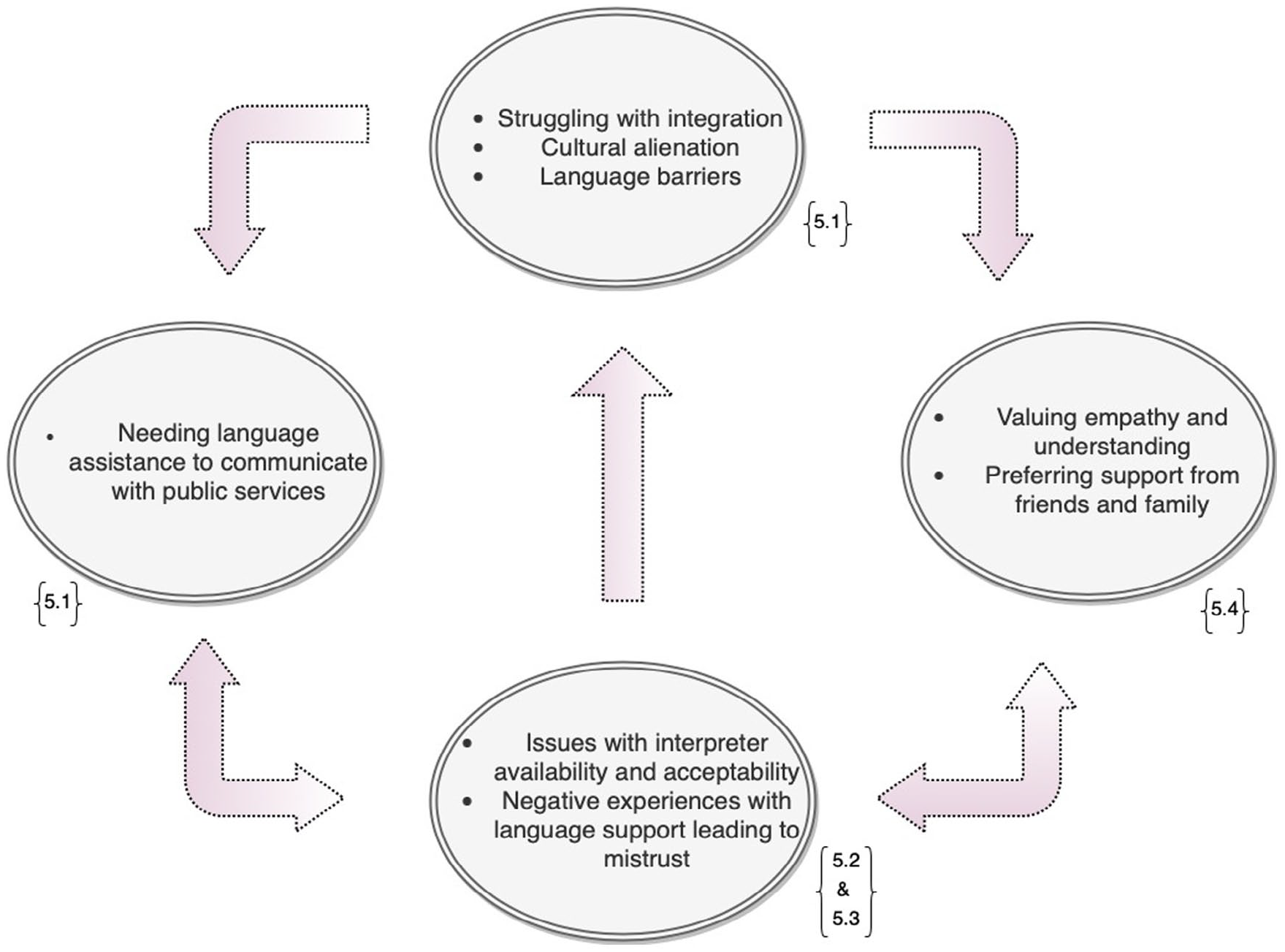
Summary of Findings.
5.1 “You feel like you’re mute”
In line with previous research (e.g., Carswell et al., 2011; Kotovicz et al., 2018), the participants interviewed for this study readily mentioned the psycho-emotional challenges associated with their experience of beginning a new life in a foreign country. In this regard, four participants characterised the initial stages of the journey in the host society
6
as marked by displacement and grief. Coupled with this, refugees frequently felt overwhelmed by the new culture (Marlowe, 2018; Miller et al., 2019) and the language barrier: RBC7: . . . back home, we had friends, families, the schools, and the language we knew, you know? . . . But when we moved here, everything was so hard . . . I just looked around, I was like, “is this my home?” Like, you know? “What am I doing here? I just wanna go back.”
In the case of Latin American interviewees, the main connection points to their new life were religion and the wider migrant community. In one case, the feelings of alienation were significantly mitigated by an engagement with Māori culture, whose strong community values allowed a less traumatic adjustment. This unexpected finding could suggest a need to consider the beneficial effect of more collaboration with indigenous leaders and groups in the refugee resettlement strategy to promote integration and belonging. Moreover, similar calls have recently appeared in the media and expert reports (Chanwai-Earle, 2018; Marlowe, 2021).
The lack of language competency was often the most evident and significant alienating element for resettled refugees. Since the vast majority of the participants (6/8) did not speak English on arrival in Aotearoa New Zealand, data in the study indicated that the constant language barrier increased their stress level and created a sense of helplessness. Support for quota refugees was available through Red Cross volunteers, who were unfortunately often unable to communicate in a shared language. Under those circumstances, the data in the study suggested a critical need for interpreters—and other forms of language support—to enable refugees at different stages of their settlement journey to access essential services and communicate with public service providers.
5.2 “[The interpreter] is essential to me”
Suitable interpreting support for refugees allows them to exercise their rights and integrate into the new society in meaningful ways (e.g., Crezee et al., 2011; Jiménez Ivars & León-Pinilla, 2018). As outlined above, most participants could not communicate effectively in English on arrival. In several cases, they continued to experience difficulties several years after resettlement (see Holt et al., 2001). In particular, five interviewees continued to require or prefer language support when accessing essential services like healthcare after years living in the country.
Despite such a clear need for interpreter-mediated communication, the participants’ experiences portrayed heterogeneous access to professional interpreters. This runs counter to official provisions (e.g., Right 5 in the Code of Health and Disability Services Consumers’ Rights, [Health and Disability Commissioner Regulations, 1996]). This gap in service provision appeared to result from a combination of aspects, including the refugees’ unawareness of their language rights or the processes for obtaining language support and the service providers’ inattention to the needs of CALD clients. For example, the use of Google Translate during medical consultations, a lack of information about booking interpreters, and unavailability of language support for important appointments were all part of the participants’ experiences in Aotearoa New Zealand. Yet the consequences of such breaches to legally recognised entitlements can be quite serious and range from inability to access a service to disempowerment and (re)traumatisation. The following quotes illustrate the impact on the emotional wellbeing of two participants due to poor communication: RBC2: For me, it’s been about four appointments [without interpreter] that have really left a mark because I came out of them very frustrated and emotionally distressed. RBC4: I got sick and was hospitalised for eight days in [city name], and I never had a translator, never . . . And, for me, it was very depressing, very sad, because I was dying. I was there for eight days, and they gave me so many antibiotics that even now, after three years, my body is still bearing the consequences of those antibiotics; my body is still getting rid of them, and I’ve had several issues because of that. And for example, they gave me a lot of morphine because the pain was so strong. So, I’d say, “argh,” and they would immediately give me morphine. Okay, that’s fine, but I was never able to say anything to anyone, to say, “I don’t want morphine, please give me Panadol or something less strong because I need to stay conscious,” never. I mean, they would come and give me morphine, and I couldn’t say “yes” or “no.”
Besides interpreter availability, the participants spoke about issues concerning the acceptability of such service. For instance, the participants’ preference for in-person interpreters was generally dismissed in favour of telephone interpreting. Despite the widespread use of telephone interpreting, refugee-background clients in this study preferred the support provided by face-to-face language assistance. The problems narrated by participants included both technical issues and the lack of human contact and empathy. Interestingly, the preference for in-person interpreting appeared across all interviews: RBC8: [Telephone interpreting] makes it very hard; is even harder with that. I don’t know; face-to-face is . . . you know? You use the, how to say? The gestures or something make it clear, but when it is over the phone is really not that easy. I don’t think it’s very useful.
Other international scholars have observed the predominant reliance on remote interpreting for CALD clients (e.g., Albl-Mikasa & Eingrieber, 2018; Al-Salman, 2016). In Aotearoa New Zealand, phone and video interpreting are the primary forms of interpreting support for communication with public services. In addition to the lower cost of these services, the government highlights the benefits of having “interpreters available 24 hours a day, seven days a week, in over 180 languages” (Ministry of Business, Innovation and Employment, 2022). However, in light of the above, it may be worth reviewing whether this approach can be a “one size fits all” solution or if, on the contrary, there is a need for more nuanced decisions that better balance resource use and clients’ preferences.
The interviewees also shared past experiences where their need for language support was resolved unacceptably, often because of a limited pool of interpreters in specific languages or dialects. Sometimes, providers expected participants would agree to use interpreters from the opposite gender or who spoke different dialects. Moreover, in two cases, the same interpreters were redeployed even after the clients expressly complained about them. Such examples suggest large gaps in the provision of language support concerning availability and acceptability. Since the participants belong to two of the largest community language groups in Aotearoa New Zealand (Ministry of Business, Innovation and Employment, 2021), the above experiences do not seem to correspond with an internationally recognised lack of qualified interpreters for languages of limited diffusion (LLDs) (e.g., Hale, 2011a; Lai & Mulayim, 2010). On the contrary, such gaps suggest an interpreting landscape marked by interpreter under-professionalisation, as supported by previous local publications (e.g., Clark et al., 2009; Enríquez Raído et al., 2020; Gray, 2019; Seers et al., 2013): RBC6: [The use of that interpreter] didn’t make me feel like comfortable and well. But if I have to, if there’s no one instead of her . . . If I have to like . . . yeah, because like the appointment only is 30 minutes, so if there’s no one, I have to [use that interpreter].
The participants’ experiences also underscored problems in the way that public service providers construe and approach the communicative needs of refugees and other migrant groups, as previously identified in the literature (see Crezee et al., 2011, 2020) Examples of service providers directing their messages to the interpreters and asking them to relay the information almost as “communication brokers” contravene express best practice guidelines for professionals working with interpreters (e.g., Waitemata District Health Board eCALD® Services, 2020). Therefore, the findings from this study confirm an inconsistency between government and scholarly recommendations for effective interpreter-mediated communication, on one hand, and actual interpreter-mediated encounters on the other. Such inconsistency suggests gaps in the level of training on and understanding of how to work with interpreters. The above also suggests unawareness of potential (re)traumatisation due to inadequate language support and client disempowerment. These issues are further explored in the following section.
5.3 “Please, just interpret what I’m saying”
Beyond the need to overcome language barriers, the above discussion hinted at additional, non-linguistic aspects that underpin acceptable and safe language support. From the point of view of the interpreter-mediated encounter, scholars have reflected on the difficulty of establishing trust with CALD communities (e.g., Edwards et al., 2005). In this regard, a 63% of refugees interviewed in this study (5/8) had experienced adverse incidents with interpreting services, sometimes leading to mistrust in the profession as a whole. For example, participants recalled identifying inaccurate renditions from interpreters as they became more fluent in English, and even noticed their interpreters struggle to understand the source message, which affected their ability to interpret it correctly: RBC7: . . . my parents can catch words, and like whenever they say something in Arabic, and they ask the translator to translate it, they don’t translate it the way we want it. So, like, for example, we would say a sentence, and they would say like two or three words of it to just summarise the whole thing.
Besides querying the linguistic competency of interpreters, the participants also observed other practices generally perceived as unethical among interpreting professionals, such as filtering messages, judging what the clients said, offering advice and even breaching the duty of confidentiality: RBC5: . . . when [the interpreter] arrived, she said something like, “this is confidential and will remain secret.” And then it turned out that, when I was living with my mother-in-law, she already knew all about my problem. So, like [the interpreter] was the only one, because there was nobody else in the consultation.
Most professional codes of ethics for translators and interpreters—including the one adopted by the New Zealand Society of Translators and Interpreters (NZSTI, 2013)—include accuracy and confidentiality among their principles (for a detailed discussion of codes, see Hale, 2011b; Phelan et al., 2019). In this study, refugee-background participants mentioned transparent communication and interpreter accuracy, neutrality, and confidentiality as some of the most critical elements in an interpreter-mediated encounter. However, an interesting difference appeared within the group, which correlated with the participants’ cultural backgrounds. In the case of Arabic-speaking refugees, accuracy and clear role boundaries that limited interpreters to communication facilitators were paramount. Conversely, Spanish-speaking refugees in the study placed a higher weight on empathy and receiving additional support from their interpreters. Such contrasting views could relate to cultural nuances impinging clients’ expectations and warrant further exploration in larger and more diverse research projects.
The examples and findings explored in the previous paragraphs indicate two concerning aspects of interpreter practice. On one hand, the use of untrained interpreters identified by other New Zealand-based scholars (Enríquez Raído et al., 2020; Fenton, 2004; Seers et al., 2013) point to clear gaps in the procurement and availability of qualified, professional interpreters. On the other hand, interpreter practice denotes discrepancies between ethical standards and actual performance (see Jiménez Ivars, 2020). The discrepancies also align with findings from the interpreter group in the same study, as published elsewhere (González Campanella, 2022). Consequently, the participants’ experiences suggest an urgent need to ensure suitable, pre-service interpreter training and supervision to improve the quality of the support provided to vulnerable clients.
5.4 “I prefer [an interpreter who is] friendly and kind”
The study indicates that refugees value affective skills in their interpreters, which sometimes conditions the perceived acceptability of the service. Interpreters’ psycho-affective skills continue to receive limited attention in research and training, despite the number of scholars who have identified the potential emotional impact on interpreters as a result of their work with vulnerable clients, such as refugees (e.g., Miller et al., 2005; Roberts, 2015; Splevins et al., 2010; Valero-Garcés, 2015). The broader study that encompasses the present findings suggested a conflict between interpreters’ natural empathy and compassion on one hand, and the lack of sufficient training and an emphasis on deontological ethics, on the other hand (see Todorova, 2019). Beyond the internal struggle and potential psycho-emotional consequences of such conflict, the findings from this group of refugees underscore the importance of adequately recognising and utilising these skills.
Interpreter “empathy” or “kindness” played a crucial role for most refugee-background clients (5/8) in their interaction with a service provider, as it affected their perception of the service as a whole and their level of trust. The interviewed refugees generally felt most comfortable with interpreters who expressed a certain level of empathic response and understood their culture and journey as refugees. However, when asked about specific actions that would fit these criteria, the participants mentioned embodiments ranging from “being nice” and accommodating to potentially offering advice and emotional support. This finding then suggests conflicting expectations placed on interpreters, which was reinforced in the findings from the interpreter group in the study (González Campanella, 2022). It also indicates that refugees do not receive adequate information about the interpreter’s role, which, in turn, results in the abovementioned conflicts and can negatively impact client trust: RBC2: No, well, in those moments when you’re really distressed, I feel like it’s very important in those moments like to know that [the interpreters] are there for you. Not just to like help with translation but also like “I understand what you’re going through, it’s okay.” RBC7: . . . sometimes you would be really going through a very hard, hard, hard, hard time, and you can’t like speak to an English person, and you don’t speak English, then you would need an interpreter. Then you would need that interpreter to really understand you as a refugee, what you’re going through.
The expectations of some participants that interpreters provide additional support beg the question whether there is a need to revisit interpreter role definitions in Aotearoa New Zealand. More particularly, the findings suggest the potential suitability of a specific type of intercultural mediation to meet this need, similar to the image often presented in some European countries (see Pokorn & Mikolič Južnič, 2020; Rubio & Nogués, 2017), and the impact of such role on the interpreter.
However, in the case of vulnerable and potentially traumatised clients, practices like offering advice, emotional support or explanations run counter to the principles of trauma-informed interpreting, as they effectively undermine the power and autonomy of the other parties. It is thus imperative that, aside from general interpreting skills, within the context of trauma-informed interpreting, interpreters develop what Yaseen and Foster (2019) call “cognitive empathy” (p. 7). As human beings, interpreters cannot simply turn off their natural empathic response—which, the study indicates, plays an important role in promoting positive outcomes. Suitable training would allow interpreters to distinguish between emotional and cognitive empathy, thereby being able to empathise with their clients from an emotional distance that protects both clients and themselves. This ability could, in turn, enhance how interpreters effectively ascertain and maintain role boundaries.
The issues related to role boundaries and unethical behaviour may increase when community members or relatives are used as interpreters (e.g., Seers et al., 2013; Shrestha-Ranjit et al., 2020). Nevertheless, the data from this study group showed an interesting juxtaposition between participants who used family members as a last resort in the absence of professional interpreters, and others who preferred this type of support, mainly due to trust issues (see Edwards et al., 2005). Notably, two participants spoke of acting as interpreters for other family members—particularly their parents—as the only acceptable recourse in their household. This practice has been flagged in several international publications as inadequate and problematic for the ad hoc interpreter on a psycho-emotional level (Miller et al., 2019), particularly in the case of minors. Therefore, the continued use of children and other vulnerable untrained bilinguals further evidences unawareness of trauma-informed care and can endanger both the client and the acting interpreter: RBC6: Yes, my mom got pregnant twice during the three years, and I was attending all her meetings and like all, each time she go to the hospital, see doctor or nurse, especially when she gave birth, I was the translator for her. Even like my English was like very basics, but I was the one because only me, like there was no one.
The use of ad hoc interpreters (e.g., family, friends, bilingual staff) underscores a discrepancy between official provisions (e.g., Health and Disability Commissioner Regulations, 1996) and actual practice. Several elements could help explain this discrepancy, including an apparent lack of clear information for clients and service providers about the use of interpreters. However, besides such lack of information, the participants’ experiences suggest the need for official guidelines that consider the actual needs of CALD clients. More research incorporating the views of interpreting clients (e.g., Marianacci, 2022) could help bridge this gap.
6. Conclusion
Refugees are often unable to communicate effectively in the host country’s predominant language (Holt et al., 2001). This article argues that the culture and language barriers experienced by refugees in Aotearoa New Zealand compound with the inherent ordeal of (re)settlement and increase the risk of (re)traumatisation. Given the scarcity of Public Service Interpreting research focusing on the views and experiences of the clients (e.g., Marianacci, 2022), this article explores the perspectives of refugee-background clients concerning their need for and use of interpreters for accessing public services.
Interpreters represent a critical connection between refugee-background communities and the country of resettlement. They enable access to essential services, such as healthcare, legal representation, and mental health support. Repeated examples of unavailable or unacceptable language support can therefore cause significant emotional distress to a vulnerable and potentially traumatised group, and evidence an institutional unawareness of adequate trauma-informed care.
The experiences of refugee-background clients using professional interpreting across public services also presented some alarming signs of inappropriate practices, including interpreters who offered explanations or advice and breached their confidentiality duties. Such incidents had a negative psycho-emotional impact on clients and increased their mistrust of language professionals. In other cases, client discomfort derived from a desire for more interpreter empathy. Both situations led to some refugees preferring family members as interpreters, in contrast to professional recommendations. However, using ad hoc interpreters, including children, without the necessary training can also create a risk for these interpreter’s psycho-emotional wellbeing. Therefore, the study underscores the need to embed psycho-affective skills like cognitive empathy in interpreter training and ensure the engagement of duly trained language professionals.
The small number of study participants and resulting limited diversity within the group limits the scope of the study findings. Further research with larger and more diverse participant groups is needed to expand this knowledge, including exploring possible correlations with specific ethnic communities. Nevertheless, the study contributes to a gap in existing knowledge about the challenges and experiences of refugee-background clients using interpreters to communicate with public service providers across settings in Aotearoa New Zealand.
The institutional misunderstanding of the communicative needs of potentially traumatised refugees translates into disempowering practices that endanger (re)traumatisation and fail to support refugees’ healing journey. Therefore, the study offers valuable knowledge about existing gaps in current interpreting service provision in light of trauma-informed best practices. It remains to be seen whether future changes in language support implement actions that align with linguistically and culturally acceptable trauma-informed approaches. Meanwhile, this article calls for the implementation of trauma-informed interpreting in interpreter training and as standard practice with refugees and other vulnerable populations, as well as for more interdisciplinary work to create acceptable communicative solutions for migrants and refugees.
Footnotes
Acknowledgements
This research would not have been possible without the kindness of the participants who shared their experiences with the goal of improving language support for other refugees.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/ or publication of this article: This work was supported by the University of Auckland Doctoral Scholarship.