
Abstract
Cumulative motion injuries and burnout contribute to an international shortage of signed language interpreters (SLIs). Studies using the Job Content Questionnaire, a well-validated measure of occupational health risks, indicate that risk levels differ among SLI work settings. Specifically, video relay service (VRS) and primary and secondary educational settings (K–12) are associated with greater health risks. The current study validated those results by analysing the diurnal rhythm of salivary cortisol levels. Anomalies in diurnal cortisol rhythms are associated with an array of health problems. Our full-time SLI participants included VRS workers (N = 20), K–12 workers (N = 18), and SLIs who worked in other settings (N = 23). Non-interpreters using sign language daily at work (N = 18) comprised a fourth group. Saliva samples were collected four times daily over 2 working days. The VRS and K–12 SLIs demonstrated lower morning peak cortisol levels and flatter diurnal cortisol slopes from morning peak to subsequent diminution. Both findings are associated with chronic stress and greater health risks. The VRS and K–12 groups’ diurnal cortisol patterns closely resembled each other, while the Other SLI group’s curve closely resembled that of the Non-Interpreter group. Implications for SLI health, education, and job redesign are discussed in the context of the demand control schema.
Keywords
Introduction
Occupational health problems that plague signed language interpreters (SLIs) are a major cause of the interpreter shortage in the United States and elsewhere (Jackman, 1999; Matthews, 1994; McCartney, 2016; Wessling, 2020). Interpreters suffer high rates of cumulative motion injury (CMI), burnout, and departure from the field (Bower, 2013, 2015; DeCaro et al., 1992; Feuerstein et al., 1997; Fischer & Woodcock, 2012; Registry of Interpreters for the Deaf, 1997; Sanderson, 1987; Schwenke et al., 2014; Stedt, 1992; Sweeney et al., 1984; Wessling, 2020). Most studies regarding this problem focus on CMI and presume that the causes and potential solutions lie in the mechanics of signing (DeCaro et al., 1992; Feuerstein et al., 2000; Norris, 1996; Registry of Interpreters for the Deaf, 1997; Sanderson, 1987). However, research also suggests that psychological stress, rather than signing mechanics alone, plays a significant role in SLI occupational health problems (Bower, 2013, 2015; Dean & Pollard, 2001; Fischer & Woodcock, 2012; Heller et al., 1986; Qin et al., 2008; Schwenke et al., 2014). Furthermore, most prior studies fail to differentiate among SLIs in relation to the specific environments in which they work, treating health risks as if they are homogeneous among SLIs. However, two studies reported by Dean et al. (2010) demonstrated that SLI health risks vary as a function of the specific work setting in which they are employed. In these studies, video relay service (VRS), and primary and secondary educational settings (known as K–12 settings in the United States) were associated with greater health risks than other SLI work settings. Brunson (2011) and Caselli et al. (2020) detail difficulties that interpreters face in these two work settings, respectively. The two studies reported by Dean et al. (2010) utilised the Job Content Questionnaire (JCQ), a well-validated, self-report measure of occupational health risk (Karasek, 1985; Karasek et al., 1998).
The remainder of this article begins with an introduction to Karasek’s demand–control theory regarding occupational health risks and its relation to Dean and Pollard’s (2001, 2013) application of that theory to the field of interpreting (a.k.a., the demand control schema [DC-S]). Subsequently, a brief overview of the hormone cortisol and its relation to stress is presented, followed by our study’s rationale and hypotheses. The “Method” section details the characteristics of our study participants and the cortisol collection and analysis procedure. The “Results” section follows, describing the statistical analysis procedures utilised. The extensive “Discussion” section first addresses the cortisol findings, and then describes self-report data gathered by one of our graduate student assistants, from the same participant sample as this study, which has direct bearing on the cortisol results. Noteworthy aspects of the participants’ demographic data are discussed next. Subsequently, the study findings are aligned with demand–control theory, first in relation to VRS interpreters, then interpreters working in K–12 educational settings. Similarly, the “Recommendations” section focuses first on VRS interpreting work and then on K–12 interpreting work. It ends with an examination of how engaging in reflective practice is a growing trend in the interpreting field and how it can address problems identified in this study. The article concludes with the “Study Limitations” section and our final conclusions.
Demand–Control theory and DC-S
The JCQ was developed by Karasek, in accordance with his “demand–control theory” (Karasek & Theorell, 1990). Demand–control theory posits that occupational health problems arise from an imbalance between the “demands” of a job (the tasks and other factors a worker must contend with) versus the “controls” (e.g., physical, educational, personal, “decision latitude,” and other resources) the worker can bring to bear in response to job demands. When there is significant imbalance between demands and controls, Karasek’s studies demonstrate, this leads to stress and associated health problems. Karasek’s demand–control theory, which emerged from his research on cardiovascular illness, was a rejection of more simplistic assumptions that certain occupations, in-and-of-themselves, were high stress in nature (e.g., surgeon or air traffic controller). It was not the occupation per se, his work demonstrated, but the interaction between the job demands and the worker’s control resources which led to stress and illness when demands and controls were imbalanced versus health, learning, and job satisfaction when demands and controls were properly balanced. Karasek (1979) recommended reducing demand–control imbalance via “job redesign.”
Karasek’s theories and recommendations have been applied to many specific occupational fields. Dean and Pollard (2001, 2011, 2013) adapted Karasek’s work to the specific circumstances of the community interpreting profession. Referred to as the “demand control schema” (DC-S), theirs is an approach to interpreting work analysis and associated decision making.
Cortisol and stress
The human endocrine system produces and releases numerous hormones that regulate and otherwise influence a wide array of bodily functions, including growth, sleep, metabolism, mood, and much more. Cortisol is the primary hormone released when humans are under stress. The level of cortisol in the body follows a well-established pattern that changes throughout the day. As illustrated in Figure 1, its level rises upon awakening (termed the cortisol awakening response or CAR), reaching its peak about 30 min later, then gradually falls throughout the day (Chan & Debono, 2010; Nagamine et al., 2017).
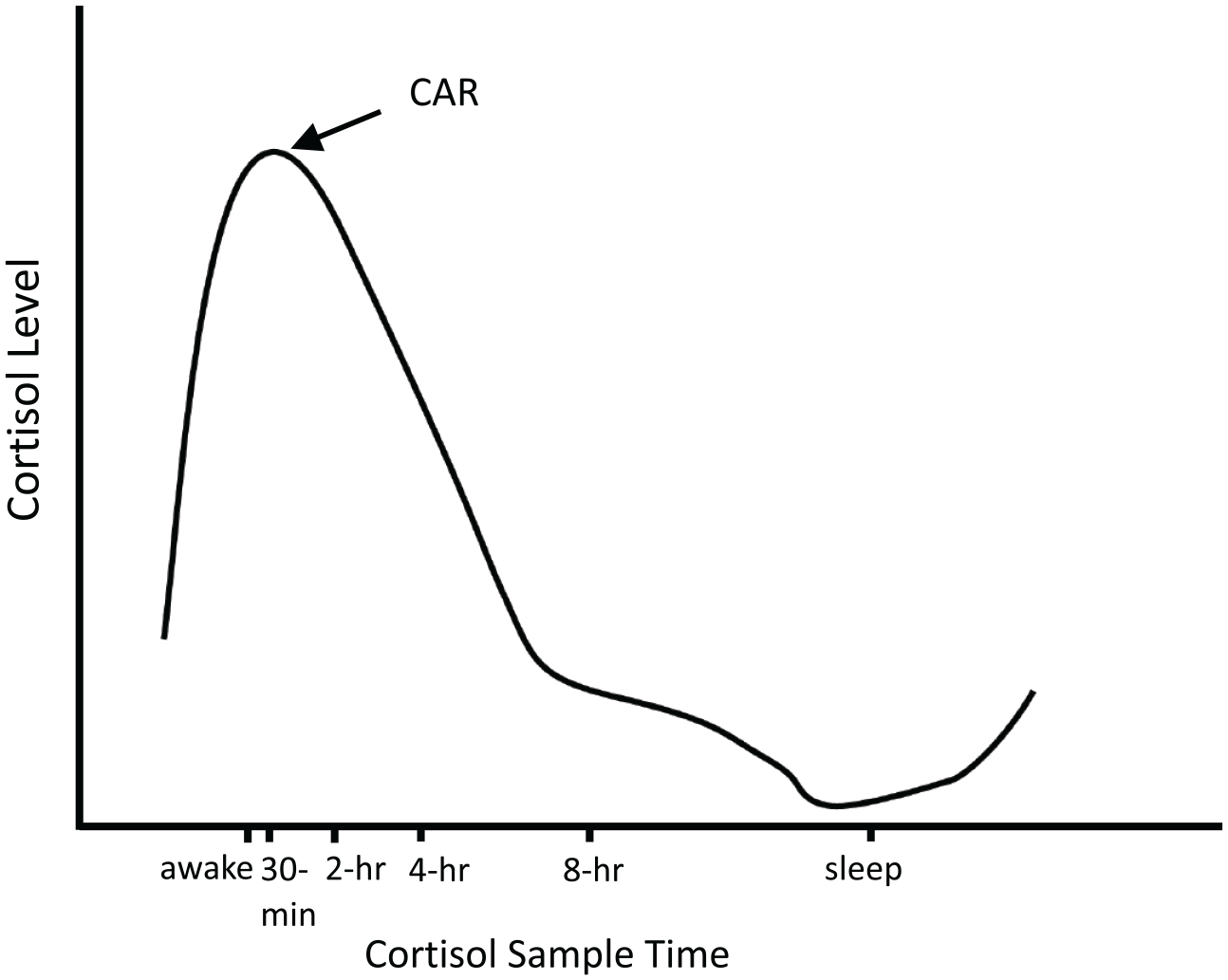
Illustration of the Normal Diurnal Cortisol Rhythm.
The CAR is indicative of one’s anticipation and preparation for the demands and activities of the day (MacDonald & Wetherell, 2019; Powell & Schlotz, 2012). The subsequent diminution of cortisol levels throughout the remainder of the day reflects one’s adaptation to the demands of the day, in particular, one’s ability to respond effectively to those demands, that is, to handle stress.
Chronic or even short-term situational stress may disrupt the normal cortisol rhythm in different ways, including abnormal increases in overall cortisol levels throughout the day, a less pronounced (“blunted”) CAR, or an atypically slow decline in cortisol levels over the course of the day. This slower decline is indicated by a “flattening” of the diurnal (that day’s) cortisol slope rather than the normal, sharp decline throughout the day, as shown in Figure 1. Studies have shown that a flattening of the diurnal cortisol slope may, at times, result from a blunted CAR and/or a general elevation in that day’s cortisol output (Lovell et al., 2011). Abnormal (a.k.a. “dysregulated”) cortisol rhythms have been linked to cancer, cardiovascular disease, metabolic disease, and other illnesses (Epel, 2009; Juster et al., 2010; Sephton et al., 2013; Thayer et al., 2009; Touitou et al., 1996). A recent meta-analysis of 80 research studies underscored the association between abnormal diurnal cortisol slopes and both mental and physical illnesses (Adam et al., 2017). Importantly, flatter diurnal cortisol slopes are associated with an increased risk of premature death (Kumari et al., 2011).
Study rationale and hypotheses
Prior JCQ findings indicated that VRS and K–12 SLIs experience greater chronic stress than SLIs who do not work in those settings (hereafter referred to as “Other SLIs” or the “Other SLI group”) and are therefore at greater risk for occupational health problems (Dean et al., 2010). The aforementioned Adam et al. (2017) meta-analytic review concluded that flatter diurnal cortisol slopes were a function of stress-related cortisol dysregulation. Combining the JCQ findings with such cortisol dysregulation data, we hypothesised that SLIs in chronic, self-reported high-stress job settings (VRS and K–12) would manifest significantly flatter diurnal cortisol slopes than Other SLIs.
To test this hypothesis, we planned to measure cortisol levels of SLIs in VRS, K–12, and an Other SLI group at four timepoints, over a period of 8 hr after waking, based on saliva samples collected at each timepoint over 2 working days. Two measurement days, or even shorter time periods, are common in cortisol studies. We planned to statistically examine the interaction between these SLI groups and the magnitude of their changes in cortisol levels over the course of these 2 days, expecting that the VRS and K–12 group would manifest flatter diurnal cortisol slopes than the Other SLI group.
We also planned to measure cortisol levels, in the same manner, in a group of hearing (non-deaf) individuals who used sign language daily at work but not in an interpreting context (hereafter referred to as the “Non-Interpreter” group). These persons also experience biomechanical demands of work-related sign language use but not the same types of cognitive and other work demands that SLIs experience. We expected this Non-Interpreter group also to display a relatively steeper (i.e., less flattened, healthier) decline in their diurnal cortisol curve than interpreters in the hypothesised high-stress VRS and K–12 work environments.
In sum, we predicted that the diurnal cortisol curves of these four study groups would reflect a high-stress, flattened pattern in the VRS and K–12 groups and a lower-stress, less flattened pattern in the Other SLI and Non-Interpreter groups.
Our focus on cortisol dysregulation, and the inclusion of the Non-Interpreter group, was intended to elucidate whether: (a) SLI occupational health risks extend beyond researchers’ common focus on CMI and (b) also extend beyond a focus on the biomechanics of signing alone. We believe that—while certainly relevant to SLI health and departure from the field—SLI researchers’ typical focus on musculoskeletal issues, and related recommendations for prevention and treatment, is too narrow in scope. That is, they fail to sufficiently account for the role of psychological stress in SLI occupational health problems and, accordingly, fail to address the broader, stress-related health risks known to be associated with cortisol dysregulation. This study, therefore, was designed to yield biological evidence potentially consistent with earlier JCQ data, demonstrating that VRS and K–12 work settings are high-demand, low-control in nature, leading to greater stress and greater, broader associated health risks than other SLI work settings. The inclusion of the Non-Interpreter group would help elucidate whether the biomechanics of signing per se is a relevant factor in cortisol dysregulation, distinct from employment as an SLI.
This study was approved by the Institutional Review Board of the Rochester Institute of Technology.
Method
Sample
A total of 79 women participated in the study, recruited from throughout the United States via social and personal networks, mailings, and flyers. The interpreting field is heavily predominated by women. As the number of additional participants that would have been necessary to examine gender and/or deaf 1 versus hearing SLI differences was prohibitive, the participant sample was limited to hearing women. Four groups of participants were recruited: SLIs working full-time in VRS settings (N = 20), SLIs working full-time in K–12 educational settings (N = 18), and SLIs working full-time in other settings, exclusive of any work in VRS or K–12 settings (N = 23). A fourth group (N = 18) consisted of women who use sign language on a daily basis at work but not in an interpreting capacity (e.g., teachers of deaf students).
Inclusion criteria were: female gender, age 18–45, pre-menopausal, not currently pregnant, absence of sleep disorders, absence of endocrine disorders (e.g., diabetes), no current usage of corticosteroid medications, no current usage of cytokine treatment (e.g., interferons), no history of Cushing’s or Addison’s disease, no history of radiation of the salivary glands, no current fever (defined as 101°F or above), no current respiratory infection, no current sore throat, no periodontitis (inflammation of the gums), active use of sign language at work a minimum of 12 hr per week, work in their current setting for 6 months or more, and the ability to participate in the study procedures over 2 consecutive working days while working between the hours of 7:00 a.m. and 7:00 p.m., local time. Participants could choose which 2 consecutive working days best fit their schedules and the cortisol measurement tasks required.
Demographics regarding the study participants are presented in Table 1.
Participant Demographics.
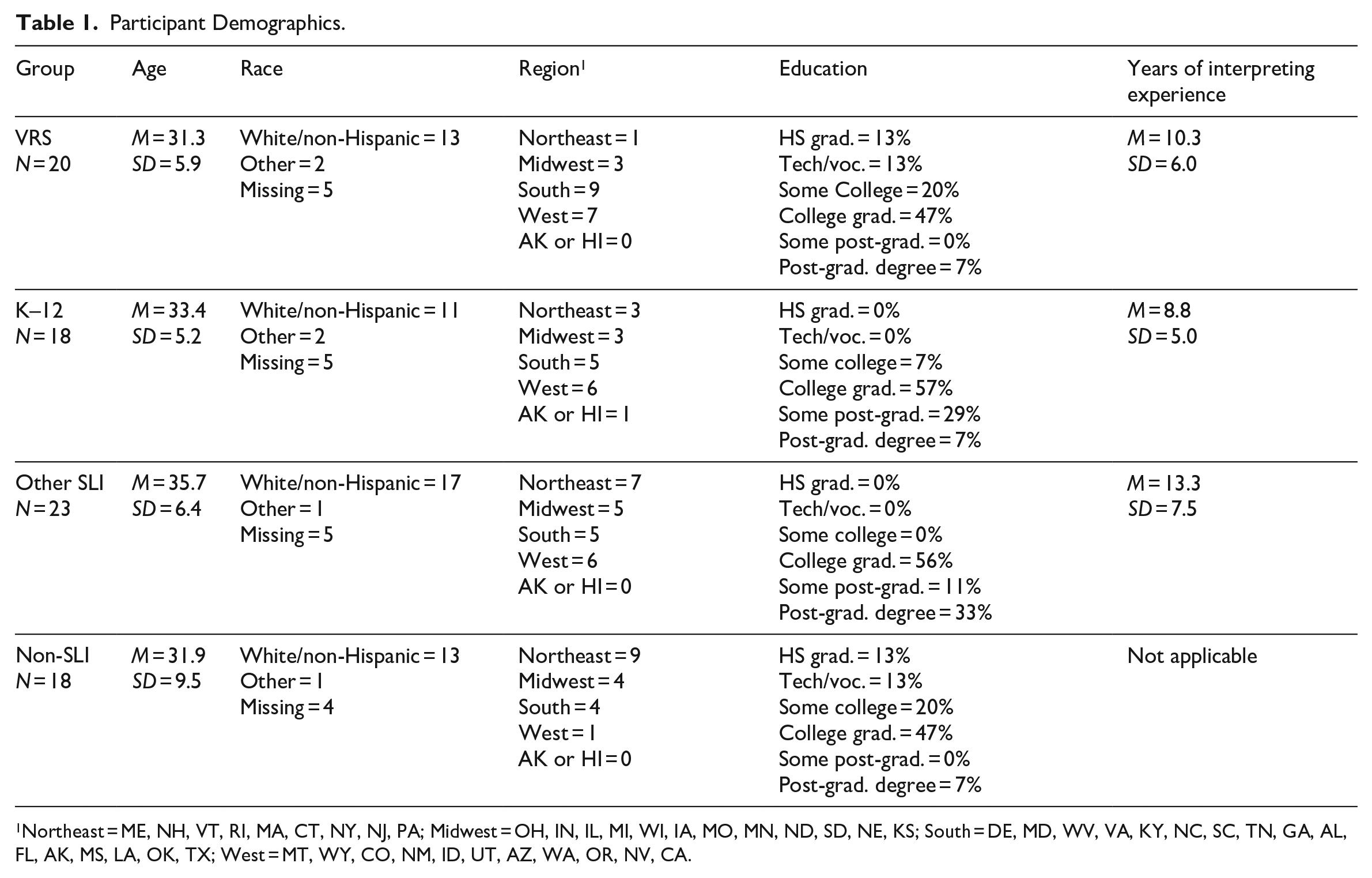
Northeast = ME, NH, VT, RI, MA, CT, NY, NJ, PA; Midwest = OH, IN, IL, MI, WI, IA, MO, MN, ND, SD, NE, KS; South = DE, MD, WV, VA, KY, NC, SC, TN, GA, AL, FL, AK, MS, LA, OK, TX; West = MT, WY, CO, NM, ID, UT, AZ, WA, OR, NV, CA.
Cortisol collection and analysis procedures
Participants were mailed a kit (or given to them in-person in a few instances) containing the necessary materials and instructions for collecting saliva samples via the “passive drool” technique (Adam & Kumari, 2009; Kirschbaum & Hellhammer, 2000) and how to return the samples by mail (postage paid) to the laboratory that conducted the cortisol analyses. Also included was an informed consent document, a data collection record (e.g., to note specific saliva collection times and other relevant information), a U.S. tax form (W-9) to allow for participant compensation (US$75), and links to a website that collected demographic information as well as several self-report measures that were a supplemental aspect of this study, of interest to our graduate student assistants. A video link featuring the principal investigator demonstrating and explaining all the materials and information involved in the study also was sent to all participants. Participants were instructed to collect saliva samples four times daily over two consecutive workdays: 30 min after awakening, 2 hr after awakening, 4 hr after awakening, and 8 hr after awakening. Cortisol level analyses for all saliva samples were conducted by a laboratory well-versed in the technique at the University of Rochester Medical Center.
Participants mailed the saliva samples, along with relevant paperwork, to the lab for analysis. Studies have shown that saliva samples are stable at room temperature for up to 4 weeks (Kirschbaum & Hellhammer, 1989; Leonard et al., 1991). At the lab, all samples were recorded on an inventory spreadsheet and frozen at −80°C until assayed. A commercially available competitive enzymatic immune assay (Salimetrics cat# 1-3002, State College, PA) was utilised to measure salivary cortisol concentrations. Following the manufacturer’s instructions, all samples were tested in duplicate. Average intra- and inter-assay coefficients of variation (CV) are 4.13% and 8.89% per the manufacturer’s documentation. Following standard procedures, cortisol values falling below the lowest standard point on the concentration curve were assigned a value of half the lowest standard. Any samples with a concentration above the highest standard were diluted and repeated. Any samples with CV of the duplicates greater than 10% were repeated. All samples that ultimately fell outside the acceptable CV values were excluded from the study.
Results
The hypothesis that high-stress SLIs (VRS and K–12) would display a flatter diurnal cortisol slope than low-stress SLIs (i.e., Other SLIs) implies a specific statistical interaction between two analysis groups—VRS and K–12 SLIs combined versus the Other SLI group—over the eight cortisol diurnal sample times (30 min, 2 hr., 4 hr., 8 hr. on both sample days). We tested for this interaction via a repeated measures Group by Sample Time design, followed by planned contrasts comparing the slopes of time periods within the cortisol curves, to isolate the source of the hypothesised interaction. Based on previous findings that stress-related flattening of the diurnal cortisol rhythm can entail both a blunted CAR (occurring at approximately 30 min after wakening) and elevated mean cortisol levels at later time points (Lovell et al., 2011), we used directional planned mean contrasts to test group mean differences at specific time points after obtaining a significant group slope difference.
Figure 2 displays the diurnal cortisol patterns and statistical results for the two planned contrast SLI groups. The figure shows that the Group by Time interaction was significant and resulted from the VRS + K–12 group’s flatter cortisol slope compared with the Other SLI group, as predicted. This interaction was characterised by a significantly more rapid diminution towards a daily plateau for the Other SLI group compared with the VRS + K–12 group in the period from 30 min to 2 hr, as indicated by the significant group slope differences in that period. The significant group slope differences in the 30 min to 2 hr period and the 2-hr to 4-hr period stemmed from the VRS + K–12 group’s cortisol levels being blunted at 30 min (t[58] = –2.66, p = .05) but elevated at 2 hr, t(58) = 1.57, p = .06, compared with the Other SLI group’s cortisol levels. In other words, the VRS + K–12 group’s cortisol levels were lower than the Other SLI group’s cortisol level shortly after waking (suggesting a blunted CAR) and their cortisol levels dropped more gradually over a longer time period (i.e., their curves were flattened) only to reach a plateau by 4 hr after waking.
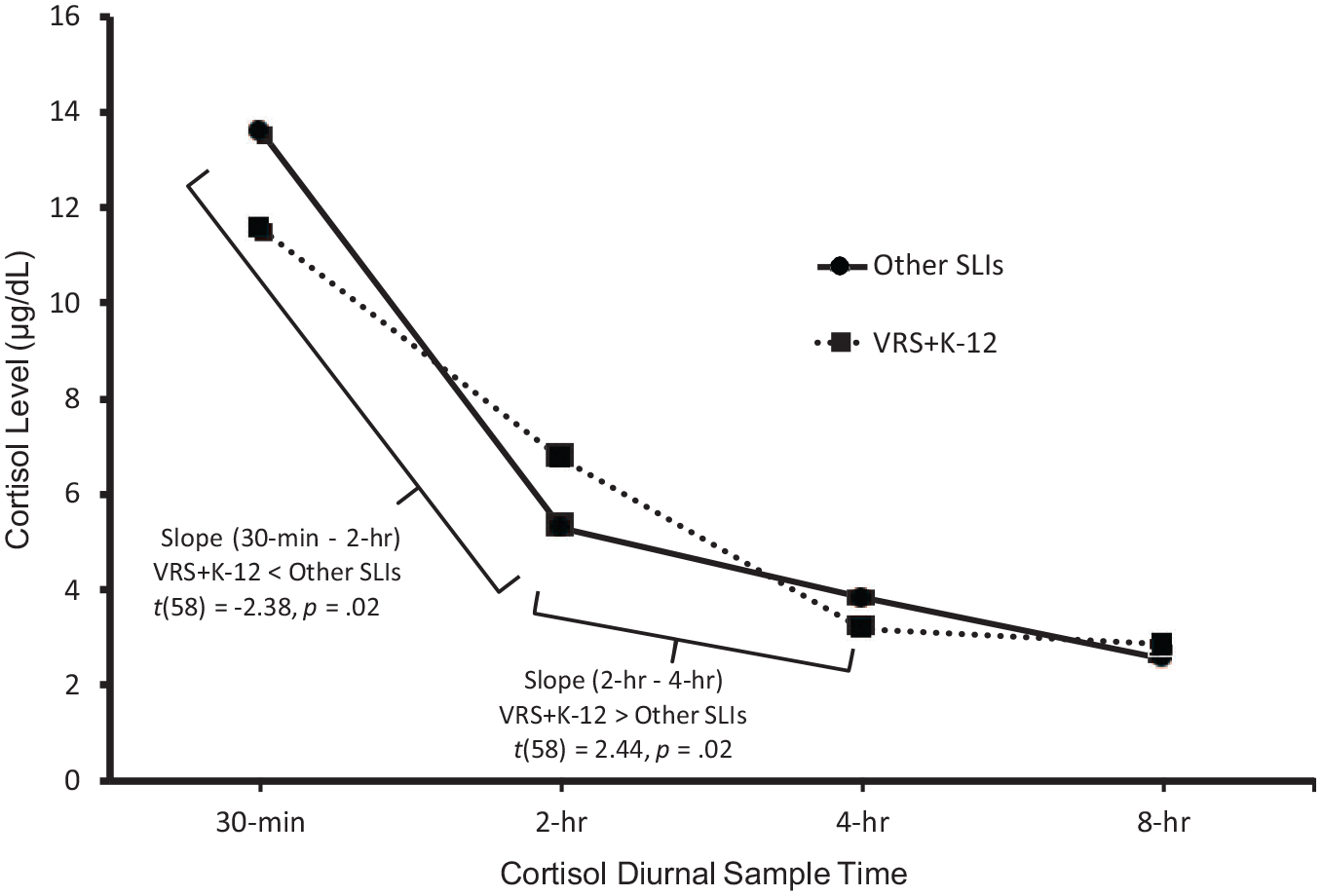
Group (VRS + K–12 Versus Other SLIs) × Sample Time Interaction: F(3, 56) = 4.00, p = .012.
Figure 3 displays all four groups’ diurnal cortisol levels. It is evident that the Other SLI group’s curve closely tracked the Non-Interpreter group’s curve. Likewise, the VRS group’s curve closely tracked the K–12 group’s curve. Adding the Non-Interpreter group to the analysis model confirmed that the planned contrast interaction of Group (VRS + K–12 versus Other SLI + Non-Interpreter) by Time was significant and resulted from the VRS + K–12 group’s flatter cortisol slope compared with the Other SLI + Non-Interpreter group’s curve. The follow-up group slope comparisons also confirmed the pattern for the high stress group (VRS + K–12) compared with the low stress group (Other SLI + Non-Interpreter) of a more gradual drop in cortisol levels from a blunted early-day level at 30 min to a lower plateau at 4 hr after waking.
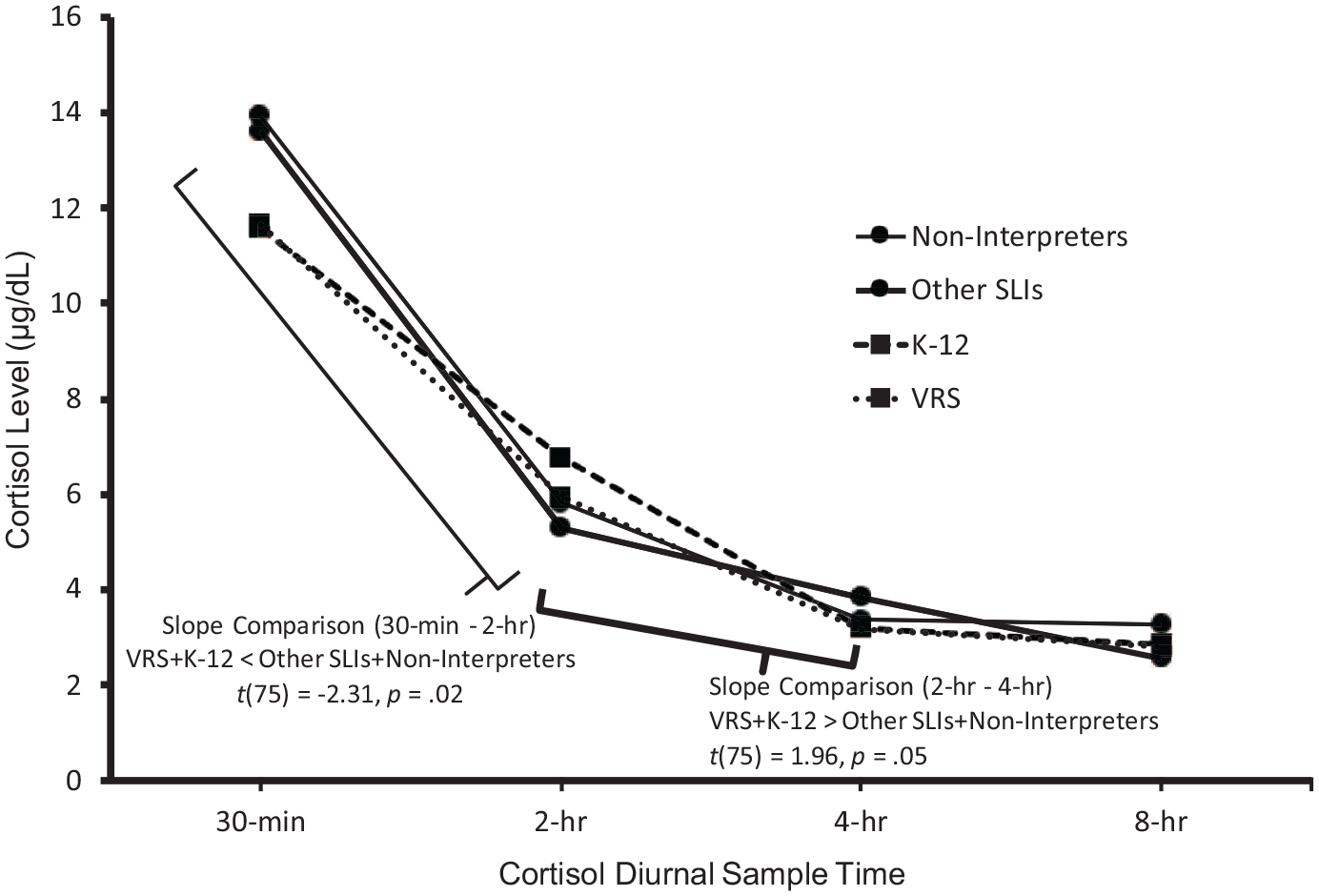
Group (VRS + K–12 Versus Other SLIs + Non-Interpreters) × Sample Time Interaction: F(3, 73) = 2.82, p = .045.
Discussion
Cortisol findings
The pattern of the interactions we identified, and the bulk of the statistical evidence, suggests there were two distinct types of cortisol dysregulation manifested in the VRS and K–12 groups in comparison to the other two participant groups. The first is associated with the CAR and the second with the overall diurnal cortisol pattern. The CAR is a separate functional component of the overall cortisol pattern but is superimposed on the longer diurnal cycle. The present data do not allow us to definitively disentangle the CAR from the diurnal cortisol cycle at the 30 min timepoint because we did not have cortisol measures immediately upon awakening. However, the lower cortisol level of the VRS + K–12 group at 30 min is consistent with a blunted CAR, while their significantly flatter slope (indicating an elevated cortisol level) at 2-hr is consistent with higher total diurnal cortisol levels. Either of these findings—a blunted CAR or a higher total diurnal cortisol level suggestive of chronic stress and its associated health problems (Friedman et al., 2012; Juster et al., 2010; Thayer et al., 2009)—is concerning. Even more concerning is the evidence that both types of dysregulation were occurring in the VRS + K–12 group. “Reduced or blunted CARs are typically observed in chronically stressed populations and are characteristic of burnout and fatigue” (MacDonald & Wetherell, 2019, p. 1) whereas higher levels of cortisol demonstrated at or beyond the 2 hr mark are suggestive of chronic stress and its associated health problems (Friedman et al., 2012; Juster et al., 2010; Thayer et al., 2009).
As noted, the negative health consequences associated with dysregulated cortisol rhythms are numerous and well established in the medical literature, including increased susceptibility to cancer, cardiovascular illness, cognitive difficulties, and more (Adam et al., 2017; Epel, 2009; Juster et al., 2010; Kumari et al., 2011; Sephton et al., 2013; Thayer et al., 2009; Touitou et al., 1996). Herriot et al. (2020) specifically emphasised the negative long-term health consequences of flattened diurnal cortisol slopes. This broad array of morbidity and mortality risks goes far beyond the risk of CMIs and other musculoskeletal problems that have been the overwhelming focus of research on SLIs’ health risks to date.
Supporting data
The Basic Need Satisfaction at Work Scale (BNS-W; Deci & Ryan, 2000) was one of the self-report instruments completed by participants in the supplemental aspect of our study conducted by our graduate student assistants. The BNS-W is based on self-determination theory, which asserts that all humans require a sense of competence, autonomy, and relatedness to develop and function in optimal ways. The 21-item scale has been used in various studies of the work environment (e.g., Ilardi et al., 1994) and yields scores regarding competence, autonomy, and relatedness, respectively. Knigga (2018) noted that the BNS-W scales have direct parallels with Karasek’s JCQ scales (Karasek, 1985; Karasek et al., 1998). Specifically, the BNS-W’s autonomy scale parallels the JCQ’s scales of decision latitude and decision authority whereas the BNS-W’s competence scale parallels the JCQ’s skill discretion scale. Knigga (2018) analysed the BNS-W responses of our study cohort and found that the VRS respondents reported a significantly lower degree of autonomy than the other three participant groups (p < .023) whereas the K–12 group reported a significantly lower degree of competence than the other three groups (p < .033). No group differences were found regarding the BNS-W’s relatedness scale. We return to these important findings below, in the section linking our study’s findings to Karasek’s demand–control theory.
Demographic data
The demographic data presented in Table 1 fail to suggest that group differences in racial background, U.S. region of residency, or years of interpreting experience were significant enough to explain our study’s findings of greater cortisol rhythm dysregulation among the VRS and K–12 SLI groups compared with the Other SLI group. This is also the case regarding the VRS and K–12 groups compared with the Non-Interpreter group, although data regarding years of interpreting experience are not applicable to that group.
There were, however, notable differences in educational attainment between the study groups. If we distinguish between college graduates (and above) and non-college graduates (and below), the VRS and Non-Interpreters’ data are identical (54% attaining college degrees or further education and 46% not attaining college degrees). The K–12 and Other SLI groups’ educational attainment was notably higher than the VRS and Non-Interpreter groups, though not identical to one another (see Table 1). These findings do not correspond to the four groups’ cortisol rhythm patterns. The VRS and K–12 groups, whose cortisol rhythms were the most dysregulated and quite similar, reported marked differences in educational attainment, with VRS SLIs having notably lower educational attainment than the K–12 group. Likewise, the much lower educational attainment of the Non-Interpreter group compared with the Other SLI group fails to explain why their cortisol rhythms were so similar. The implication is that these substantial differences in educational attainment were not a relevant factor in the cortisol findings.
However, that does not mean these educational differences are not interesting in other ways. In particular, in this study sample, why were VRS SLIs much less educated than their K–12 and Other SLI counterparts? Might this be a factor in their high stress levels, even though the somewhat more educated K–12 SLIs also demonstrated high stress levels based on these two groups’ cortisol data? In other words, might there be differences in the VRS versus K–12 work environments where lower educational attainment matters more in the VRS setting than in the K–12 setting? Finally, why are the most highly educated SLIs found in work settings other than VRS and K–12 settings? These questions require further study, especially because our participant numbers in each group were not large.
Another aspect of the demographic data worthy of note is the large standard deviation around the mean age of the Non-Interpreter group (9.5 years) compared with all three SLI groups (ranging from 5.2 to 6.4 years). This Non-Interpreter group used sign language on a daily basis at work, just as the SLI groups did. While these data could simply reflect that the SLI participants tended to be younger than the Non-Interpreter participants, it could also be conjectured that this is evidence of earlier departure from the SLI field compared with occupations where sign language is regularly used but not in an interpreting context (i.e., that workers stay in these non-SLI fields longer, until they are older than SLIs). The concern regarding burnout and early departure from the SLI field is well-documented in the literature (Wessling, 2020). This finding could be viewed as reinforcing our contention that the reasons for early departure from the SLI field lie beyond the common focus on signing biomechanics and very likely include the influence of stress and its well-known associations with a much broader array of negative health consequences.
Linking the study findings to Demand–Control theory
VRS interpreters
VRS has long been characterised as a high-demand, low-control environment for a number of reasons. Brunson (2011) and Peterson (2011) are highly critical of the policies and procedures common in VRS work settings compared with community interpreting settings. “Given the remarkable difference between what interpreters do in the community and what they do in VRS, I believe it is inaccurate, unethical, and misleading to call work done in VRS under federal and corporate constraints ‘interpreting’” (Peterson, 2011, p. 215, emphasis added). Brunson (2011) offers similar opinions. Peterson specifically points to “profit concerns [that lead to] industry constraints [which] impact the quality of access that VRS is intended to provide” (p. 214). In demand–control theory parlance, the “constraints” Peterson and Brunson both refer to are policy-based restrictions on interpreter control options.
For example, Peterson asserts that VRS interpreters “widely” (p. 205) believe that they “must without exception accept any and all calls” (p. 205) which may include calls where they don’t understand the signer very well or don’t understand the subject matter at hand, or other high-demand situations such as calls for emergency medical, fire, or police assistance. Maffia (2015) addresses the common belief that VRS interpreters must work for at least 10 min on a given call before determining that they are not qualified to continue; only then may they transfer the call to a colleague. Although Maffia indicates that the U.S. Federal Communications Commission (FCC, which oversees the U.S. VRS industry) has modified its policies to lessen extreme perceptions of VRS rules, he asserts that such modifications are not widely known by VRS interpreters. In addition to the widespread belief in this “10 minute rule,” both Peterson (2011) and Maffia (2015) assert that it is widely believed that VRS interpreters cannot enquire about the nature of an incoming call and, accordingly, cannot prepare for the situation nor assess their qualifications or “fit” for mediating the call until both parties (the caller and the recipient of the call) are connected.
Of note, VRS companies are not reimbursed by the FCC until the moment that parties are connected to one another by the VRS interpreter. Peterson’s reference to “profit concerns” could be the impetus driving policies that restrict interpreters’ discretion or, in Karasek’s terms, decision latitude and decision authority, regarding pre-connection enquiries and interpreters’ judgement as to their fitness to handle a given call. In the United States, emergency calls initiated by deaf persons (i.e., via dialling 911) are routed to the first available VRS interpreter (D. Maffia, personal communication, March 29, 2021), not to individuals with special training to mediate such calls. Both Peterson (2011) and Maffia (2015) point out that such policies, practices, and widespread beliefs prevent interpreters from fulfilling their ethical responsibility to “accept assignments using discretion with regard to skill, communication mode, setting, and consumer needs” (Registry of Interpreters for the Deaf, 2005).
More dramatic demand–control imbalance issues in VRS settings are exemplified by pilot data we have collected for an upcoming study, involving callers who make abusive comments to VRS interpreters and other serious stressors VRS interpreters experience. VRS interpreters have reported to us that they have been sexually harassed, racially harassed, or harassed for other reasons (e.g., age, weight). Others have reported distress associated with having to mediate VRS calls involving drug deals, financial scams, sexual conversations (including sex phone line services), or visually or auditorily witnessing child abuse or partner violence during VRS calls. Interpreting for drug deals, financial scams, or witnessing acts of violence raise the question of whether VRS interpreters could be judged complicit in, and therefore, liable regarding, such crimes.
VRS interpreters also witness violations of VRS/FCC policy when the interlocutors are in the same physical location. In the United States, the FCC reimburses VRS companies for VRS calls because they are akin to telephone calls where the interlocutors are in different locations. When signing and non-signing interlocutors are in the same location, and require a video-based interpreter, this is a video remote interpreting (VRI) situation, not a VRS situation. VRI calls are not funded by the FCC. Accordingly, VRS companies prohibit interpreters from engaging in such calls; they are required to disconnect when it is apparent that the interlocutors are in the same location. This is another type of demand–control imbalance and a potential source of considerable stress. This is particularly the case in high-demand situations, where disconnecting leaves the parties unable to engage in effective communication, such as during an emergency or an arrest, where first responders have arrived at the home of a deaf person who has initiated a VRS call because a VRI option is unavailable.
Our emphasis here is on how the VRS work environment seriously constrains the control resources of VRS interpreters both prior to working on a call as well as during a call. Nothing like this equates to the nature of community interpreting, where interpreters (and/or interpreting referral agencies) have much greater latitude to assess the situation into which they are being invited and properly match interpreters (and their control resources) to the job demands. Knigga’s (2018) finding that VRS interpreters report significantly lower autonomy on the BNS-W scale than the other three study groups reinforces this, as well as supporting the results of the current cortisol dysregulation study and the previous JCQ studies (Dean et al., 2010) in which VRS interpreters’ data suggested high levels of risk for occupational health problems.
K–12 interpreters
In contrast, Knigga (2018) found that the K–12 interpreters in our study reported significantly lower perceptions of competence, rather than autonomy, on the BNS-W than the other three study groups. This suggests a different, but equally significant demand–control imbalance. We assert that the K–12 cortisol dysregulation findings in our study, and Knigga’s findings with the same cohort, are a result of many K–12 interpreters bringing a lesser degree of control resources to the job situation, rather than their controls being constrained by their employers or other authorities.
There is a significant literature citing inadequate performance by interpreters in K–12 educational settings (Caselli et al., 2020; Johnson, 1991; Jones, 2005; Jones et al., 1997; Kurz & Caldwell Langer, 2005; Marschark et al., 2005; Ramsey, 1997; Schick et al., 1999; Winston, 2005). In a study of 59 K–12 interpreters, Schick et al. (1999) concluded that “less than half of the educational interpreters assessed in this study performed at a level considered minimally acceptable” (p. 144).
There are a number of potential reasons underlying K–12 interpreter performance inadequacies reported in the literature and the related competence concerns expressed via the BNS-W data in Knigga’s (2018) study. First, many K–12 interpreters lack professional training. Schick et al. (1999) reported that 14% of their study cohort had learned sign language from workshops or in-service presentations alone, rather than via sign language classes or formal interpreter training programmes. Another 14% reported having received no sign language training at all. Second, most individuals serving in these K–12 roles are not certified as interpreters per se (e.g., by the Registry of Interpreters for the Deaf [RID] or the National Association of the Deaf [NAD] in the United States). Rather, a separate assessment method was developed specifically to evaluate K–12 educational interpreters in the United States. The Educational Interpreter Performance Assessment (EIPA; Schick & Williams, 1994) is a process involving the review of videotaped samples of an interpreter’s expressive and receptive sign skills evidenced during work with a specific teacher, a particular classroom lesson, and a particular deaf student (Schick et al., 1999). The EIPA results in a Likert-type scale score ranging from 0 to 5. Obtaining an EIPA score is not a form of certification. Unlike certification of sign language interpreters by the RID or NAD, there are no continuing education requirements associated with an EIPA score. For these and other reasons, many consider the EIPA score to be significantly less rigorous evidence of interpreting competency than RID or NAD certification. For example, the Division of Services for the Deaf and Hard of Hearing in the state of Utah restricts interpreters who only have an EIPA score from working in any setting other than K–12 environments (State of Utah, Workforce Services, Rehabilitation Division, 2021).
Another, somewhat related, factor is that in many regions of the United States, especially rural regions, the availability of qualified SLIs (certified or not) is severely limited. Yet, access to a “free and appropriate” public education is a legal right for U.S. students with disabilities (National Education Association of the United States, 1978). For deaf students, this standard suggests the need for a qualified SLI, if not a credentialed “teacher of the deaf.” Lacking qualified SLIs to serve in such positions, especially at much lower salary levels than certified, experienced SLIs can command, many schools resort to hiring persons who have some sign language abilities or simply are willing to learn sign language, into K–12 interpreter positions (Schick et al., 1999). Although not substantiated by published literature we are aware of, reports of K–12 “interpreters” looking up signs, while on-the-job, via a sign language dictionary placed on their lap, are legendary.
It is also important to note that approximately 95% of deaf children are born to hearing parents, most of whom do not learn sign language or fail to learn it well enough to impart sign language to their deaf child in any substantive way. Accordingly, one of the most significant demands of a K–12 environment is that most deaf children are learning signs (much less sign language in the more linguistically complex sense) from their classroom SLI—an obvious impediment to effective communication that presents a demand–control imbalance of its own. Caselli et al. (2020) distinguish between the value of K–12 interpreters when a student is proficient in sign language versus the harm that can be caused when presuming that interpreters are an appropriate accommodation for deaf students who arrive in elementary education settings without proficiency in sign language. The authors argue that this common situation aggravates the “language deprivation” problem (see Hall et al., 2017 and Glickman & Hall, 2018) that these students contend with when their primary or only sign language model is an interpreter. SLIs cannot serve as an interpreter for a child lacking in sign fluency nor function as a formal sign language instructor for the child with any real effectiveness in either respect. It is grossly unfair for a deaf child to be deprived of language development and related academic learning when the SLI in their classroom is their only source of sign language exposure, especially when that SLI is not fluent in sign language themselves. Years of language and cognitive development should not be lost or hindered, while a minimally qualified SLI slowly works on improving their sign skills. Nor is it fair for K–12 SLIs to be put in such situations when they may not only lack sign fluency, but their job is not structured to serve as a sign language teacher or role model.
Recommendations
We believe the results of this study should engender a call to action to mitigate the health risks associated with VRS and K–12 interpreting work, based on voluminous scientific evidence of myriad, serious health problems associated with cortisol dysregulation, as well as the other data and information conveyed above. It must now be recognised that the biological consequences of chronic stress endanger the health of SLIs beyond the high incidence of CMIs alone. Accordingly, CMI risk mitigation strategies such as rest periods, stretching, warming up, or recommendations regarding specific musculoskeletal positioning are likely inadequate for addressing the broader health risks raised by this study and others citing the incidence of stress in the SLI workforce. In contrast to commonly recommended CMI risk mitigation strategies, the onus for change that we here emphasise extends beyond SLIs themselves and implicates the role that SLI employers, particularly those associated with VRS and K–12 work, must play in addressing the SLI occupational health crisis.
At a macro level, SLIs and their employers must explore and implement job redesign strategies (Karasek, 1979) aimed at achieving a healthier, more balanced relationship between job demands and the controls that SLIs are able (or allowed by policy or perceptions thereof) to bring to bear in response to job demands. This will require concerted dialogue among employers and employees, as well as policy and oversight bodies such as the FCC and its National Exchange Carrier Association, which are so influential in the U.S. VRS business (Bower, 2015). Unfortunately, key policy makers associated with VRS and K–12 SLI work are often insufficiently knowledgeable about, or influenced by, the greater balance between demands and controls common to community interpreting environments (Dean & Pollard, 2013). Accordingly, they cannot effectively participate in job redesign strategies without learning from and engaging in such efforts with SLIs directly. Collaboration with researchers and improved research-based methods for improving SLIs’ occupational health also are necessary.
VRS interpreters
We call for a “consensus planning conference,” common in the sciences, even in the deafness field (e.g., Glickman & Pollard, 2012; Pollard, 1995). Such conferences take place when disclarity or differences of opinions exist regarding a particular, important issue, and there is a sufficient body of scientific literature to potentially move a field forward past a state of disunity or divisiveness. Such a conference must include key stakeholders, including representatives from the FCC, the major VRS companies, VRS workers themselves, deaf and hearing consumers of VRS services, and researchers in the field. Such a conference would optimally result in VRS job redesign strategies that will mitigate the morbidity and mortality associated with excessive occupational stress in the VRS environment that stems from a marked demand–control imbalance.
K–12 interpreters
Our recommendations regarding mitigation of the demand–control imbalance in K–12 settings are different. Here, the focus must be on addressing the competence problem commonly associated with those who are hired to work as SLIs in educational settings. A useful approach would be to subject educational interpreting demands to a “job task analysis” (Carlisle, 1983) and use those results to rebalance the demand–control dynamic and guide job redesign accordingly. Job task analysis (JTA) techniques are used widely to determine, in significant detail, the true requirements of a job, seek employees capable of meeting those job demands, and even devise methods for assessing workers’ qualifications and performance. The current RID certification examination (National Interpreter Certification) was designed after such a JTA process.
A JTA of educational interpreting settings may well reveal complexities of the position that cannot be fulfilled satisfactorily by a single individual. That is, a JTA may reveal that the complex array of skills and abilities (control resources) needed to satisfy the demands of educating deaf students appropriately in K–12 environments would best be achieved by dividing those responsibilities among differently qualified workers and/or resources. Some of the desired skills and abilities would likely be less rigorous than those needed for RID or NAD certification, but could prove quite useful in working with deaf students, particularly in the early grades when the complexity of the instructional content is modest. Such positions, which may require sign skills but not formal interpreter training, would also serve to reduce the shortage of personnel able to work in K–12 settings by reducing the higher standards and higher salary levels typical of certified interpreters. Then, when more complex instructional or other content is being conveyed that is beyond the capability of non-interpreter assistants to facilitate, well-qualified VRI interpreters could be brought into classrooms remotely. This has a fiscal advantage as well. As VRI services are paid for based on usage time, schools would not have to hire highly qualified interpreters as employees, nor entice them to move to locations that may be unpopular. To address the issue of deaf children faced with learning sign language from less-than-fluent educational assistants (or interpreters), local, sign-fluent deaf individuals could be hired (full or part-time) to collaborate with teachers, students, interpreters, educational assistants, and families. This approach would likely increase hearing K–12 educational personnel’s sign language fluency, allow deaf employees to reinforce the educational or other content conveyed through VRI services, and serve as language and cultural role models to deaf students. Hiring certified deaf interpreters to fulfil these and other functions would be an even better approach.
The beneficial role of reflective practice
Until the recommendations above become fruitful, what can SLIs do to address chronic stress and its associated health risks? We advocate and have implemented “reflective practice” methodologies that increasing numbers of interpreters report as highly effective in reducing stress and facilitating more effective responses to job demands, even yielding restorative effects (Curtis, 2017; Dean & Pollard, 2011, 2018; Hetherington, 2011, 2012) These efforts have taken particular root in the United States, the United Kingdom, Europe, and Australia. Through engaging in formal case conferencing, structured supervision, even internship or apprenticeship periods prior to independent practice, SLIs are embracing the concept that their training and professional development should mirror approaches that are common in other “practice professions” such as medicine, law enforcement, and teaching (Dean & Pollard, 2011, 2013) Wider implementation of such methods or, better yet, mandating such practices as a requisite for SLI credentialing would do much, not only to mitigate the risks of occupational health problems and early departure from the SLI field, but to yield more effective work on behalf of SLI service users.
Study limitations
First, the number of study subjects was modest, restricted by our fiscal resources. Future research with larger sample sizes is desired, perhaps allowing greater differentiation between the VRS and K–12 groups’ similar cortisol rhythms and the Other SLI and Non-Interpreter groups’ similar cortisol rhythms. Of note, we did not conduct a power analysis to estimate sample size for this study. To do so, one needs an estimate of effect size. As this was the first study of its kind, there were no prior data on which to base an accurate estimate of effect size. Fortunately, the effect size obtained in our study was large enough to verify it statistically. Accordingly, researchers can use our effect size data to calculate optimal sample sizes in the future.
Second, variations, additions, or nuances in our findings might be discovered if future research could examine differences between “teamed” or co-worked versus solo interpreting work, cortisol patterns manifested by K–12 interpreters working with different K–12 grade levels or extending the length of our 2-day sampling period. A lengthier sampling period might mitigate shorter-term variations in stress over working days.
Third, collecting specific health and disease-related data from study subjects would potentially strengthen the presumed link between the cortisol dysregulation observed in this study and associated health risks documented in the scientific literature.
Finally, our participants did not provide saliva samples immediately upon awakening (i.e., “time zero”) over the 2 collection days. This limited our analyses of the CAR, as studies suggest that the CAR is independent of, though superimposed on, a person’s overall diurnal cortisol rhythm. However, the results of this study, as well as results from other studies of high stress populations (e.g., Lovell et al., 2011), are consistent with our conclusion that VRS and K–12 work settings are associated with higher stress and subsequent dysregulation of the mechanisms underlying the CAR as well as those underlying the complete diurnal cortisol pattern.
Conclusion
The results of this study affirmed our hypothesis that the VRS and K–12 SLI groups would demonstrate significant patterns of cortisol dysregulation in comparison to the Other SLI group. Knigga’s (2018) analyses of the BNS-W results collected from our study cohort supplement these findings, indicating that SLIs in VRS settings struggle with demand–control imbalances pertaining to autonomy, while SLIs in K–12 settings struggle with demand–control imbalances pertaining to competence. Our cortisol dysregulation findings reinforce the aforementioned JCQ studies’ results (Dean et al., 2010) and Knigga’s BSN-W findings, demonstrating greater occupational health risks associated with VRS and K–12 work settings—but with biometric data rather than self-report data. The current study strongly highlights the broad array of occupational health risks associated with VRS and K–12 work settings, given the well-known associations between cortisol dysregulation, morbidity, and mortality. Thus, we assert that SLI health researchers’ usual focus on CMI is too narrow and that SLI health risks should not be studied without differentiating among the settings in which they work. Finally, our finding that the Other SLI group’s diurnal cortisol pattern closely tracked the pattern of the Non-Interpreter group suggests that it is not the biomechanics of signing alone that leads to chronic stress and its associated health risks but the particular dynamics at play in VRS and K–12 work settings, presumably a marked imbalance between occupational demands and worker controls in those settings. This imbalance can be addressed through JTA-driven job redesign in both these work settings, accentuating the responsibilities of those who employ SLIs, not just the SLI’s themselves, in preventing or minimising occupational health problems, burnout, and SLI departure from the field. In the meantime, SLIs are learning the value of reflective practice methods in reducing stress, improving work quality, and likely mitigating longer term health risks.
Footnotes
Acknowledgements
The authors wish to thank Alaine Thibault and Andrea Sinden, then students at NTID, who provided helpful assistance in carrying out aspects of this study. Jennifer Carnahan, of the University of Rochester Medical Center (URMC), led the cortisol sample analyses. Jan Moynihan and Wilfred Pigeon, also of URMC, provided valuable information regarding study procedures and this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by funding from the National Technical Institute for the Deaf (NTID).