
Abstract
Electronic medical records (EMRs) are associated with higher-quality healthcare; however, they also raise concerns about patient information privacy and security. Existing studies have strongly linked these privacy concerns to patients withholding their information, indicating perceived risks with EMRs. Furthermore, studies devoted to EMR usage in hospitals are lacking, particularly those on the EMR system in the contexts of clinical and privacy concerns based on multi-criteria perspectives. The proposed framework is based on how clinical factors and security and privacy determinants influence the use of EMR, utilizing data derived from chronic disease patients in the USA as a frame of reference. In this study, information forage theory is adopted. This research not only objectively analyzes the information privacy aspects of EMRs but also investigates the perceptions of patients with chronic diseases regarding online health information technology and offline patient–provider interactions. These are considered as clinical factors to understand the frequency of EMR adoption across Health Information National Trends Survey (HINTS) data from 2014 (N = 2,415), 2017 (N = 2,253), and 2018 (N = 2,443). The study finds that the rate of information withholding, as a manifestation of information privacy and security concerns, has decreased over the three waves. In contrast, the frequency of EMR usage is found to have continually increased at the three assessment points. Additionally, factors such as confidence in EMR safeguards, electronic medical information maintenance, and the frequency of visiting healthcare providers are significant predictors of EMR utilization over time. The study concludes that addressing online privacy concerns over EMR as part of health information technology and considering offline clinical factors must occur together in order to achieve higher-quality healthcare among patients with chronic diseases and to transform the healthcare system overall.
Keywords
Introduction
Communication is an essential element in providing high-quality healthcare services. Once effective communication is established, it can lead to significant healthcare provision and positive outcomes, which can improve the physiological and functional status of chronic disease patients. Communication, in terms of information exchange, between chronic disease patients and healthcare providers is not only limited to the visit but is also facilitated via information communication technologies such as electronic medical records (EMRs).
EMRs are used by hospitals and healthcare providers to improve care quality as well as the efficiency of the healthcare system overall. Electronic healthcare systems enable healthcare providers to access patient data directly, which expands the automation of healthcare services (Lee et al., 2013). Research since 2017 indicates that one in four US adults suffer from two or more chronic conditions, such as diabetes, cancer, arthritis, or depression, while over half of older adults have three or more chronic illnesses (Tinker, 2017). The risk of developing these chronic conditions increases with age. Given the current US demographics, with 10,000 Americans turning 65 every day until the end of 2029 (Tinker, 2017), it is expected that the total number of individuals with chronic illnesses will rise significantly. Chronic conditions require healthcare providers and caregivers in clinical settings to offer a high quality of continuous medical services (Kruse et al., 2015). For chronic disease patients who require continuous care and sustainable self-management, EMRs serve as information and communication tools to store tracked medical history as well as test results in an electronic format, which enables better patient–provider communication and self-management (Jung et al., 2014).
Despite the benefits of EMRs for chronic disease patients, there is a gap between the anticipated benefits of EMR systems (e.g., real-time data access, clinical decision support, enhanced monitoring, and simplified administrative work) and actual usage. What is still missing is that the EMR adoption rate in the United States remains quite low (El-Yafouri et al., 2022). While 96% of hospitals in the USA have had federally certified EMR programs in place since as early as 2008, and 80% of office-based physicians have an EMR system in the workplace, by 2012 the rate of EMR adoption had increased to only approximately 15% (Lee et al., 2013). In 2013, for instance, only three out of 10 patients had access to medical records (Elkefi et al., 2021). However, the use of online medical records has seen significant growth in recent years, and technological improvements have been made to improve usability and implementation (Elkefi et al., 2021). Yet, despite greater availability, patients still avoid using online medical records.
From the extant health information technology literature, little is known about what factors impact the relationship between chronic disease patients’ perceptions and the frequency of EMR utilization. Apart from this lag in EMR adoption, privacy concerns over EMRs temper widespread enthusiasm of using EMRs for chronic patients (Keshta & Odeh, 2021; Pankomera & Van Greunen, 2016; Saad, 2019). In particular, when they perceive that their personal health data are at risk of being seen by an unauthorized party, patients possibly feel overwhelmed ( Pankomera & van Greunen, 2016). Such privacy concerns constrain chronic disease patients' information disclosure to healthcare providers and reduce the frequency of using EMRs to communicate with healthcare providers. Under this status quo, patients are prone to limiting disclosure to healthcare providers as a way of controlling such privacy threats (Campos-Castillo & Anthony, 2015). Therefore, when patients are concerned about the security of sensitive information as it is stored and transferred across the healthcare system, a decrease in the willingness to use EMRs is one manifestation of health information protection (Saad, 2019).
In addition to the privacy concern barrier of EMRs, scholars have also expressed worry that EMRs may hinder communication for chronic medical patients (Benda et al., 2017). It has been found that even in an environment where EMRs are implemented, visiting healthcare providers in clinical settings to have “real-time” communication between patients and healthcare providers continue to be indispensably used for a wide variety of purposes. It is hypothesized that patients who rarely visit or have not visited healthcare providers in clinics are unlikely to use health information technology, including EMRs, to communicate with healthcare providers.
Third, organizational theorists have pointed out that in the clinical environment, patient-centered communication (PCC) allows both patients and doctors to observe and react to verbal and non-verbal cues (e.g., Knowles et al., 2023). Nuances associated with facial expressions, tone of voice, and hand gestures convey important information that is not captured in electronic formats yet are essential for understanding patients' current health conditions. Additionally, using unprotected or unrestricted electronic health information (referred to as public eHealth) has a negative association with patient-centered care, which adversely affects patient–provider trust (Totzkay et al., 2017). This indicates that direct communication between patients and providers, as a timely offline health information exchange, remains a current trend for addressing private and personal health needs and long-term engagement for one's own healthcare.
Last, but not least, the extant research has investigated how the meaningful use of EMRs has a positive influence on improvements in care quality and efficiency of care, moderated by the length of use. This indicates that the use of additional functionalities could bring more improvements to the quality of care and that using them for a longer period of time would make the improvement much stronger. In contrast, less extensive usage usually limits EMR performance. This may indicate that healthcare providers who integrate fundamental technologies better, such as a fully utilized EMR, provide better quality care to patients, thereby increasing the frequency of EMR usage and vice versa.
In summary, the research gaps are outlined below. First, the privacy concerns related to EMR adoption among patients with chronic diseases remain unclear. Second, the majority of existing research examining factors associated with EMR use has been limited to patient characteristics such as age, education, income, and health status (Salzl et al., 2012; Samuel, 2014; Senft et al., 2019). However, there is also a need to consider factors from various contexts. Third, existing research studies are cross-sectional (e.g., Xie et al., 2020), which limits the ability to track the impacts of privacy concerns and clinical factors over time.
To address these gaps, this study examines two contextual influences—privacy concerns and clinical factors—across different waves of responses. Given the rapid development of health information technologies and quality improvements in chronic disease management, a trend analysis is needed to monitor how EMR usage among patients with chronic diseases varies over time. Since chronic conditions require ongoing tracking of symptoms and adjustments in treatment, a trend analysis related to EMR utilization can provide continuous evidence on how EMRs, as a form of health information technology, are associated with privacy concerns and clinical factors. To fill these research gaps, this study explores associations between information withholding, confidence in EMR safeguards, electronic medical information maintenance, frequency of visiting healthcare providers, patient-centered communication, and quality of care with the frequency of EMR utilization.
Literature review
This research examines how privacy concerns and clinical factors affect the frequency of EMR adoption. To clarify the relationship between information security and EMR adoption, this paper categorizes information withholding, confidence in EMR safeguards, and maintenance of electronic medical information as key information security factors.
In the context of the present study, information privacy concerns manifest as chronic disease patients' concerns for their recorded medical information privacy regarding the use of medical facilities and medical information protection. The privacy-protective responses are related to a set of behavioral protection responses of chronic disease patients to their perception of medical information concerns associated with medical facilities’ practices. The reason for the above grouping is that in spite of widespread enthusiasm for EMR system implementation, EMRs have been commonly viewed as a double-edged sword (Campos-Castillo & Anthony, 2015; Kuo et al., 2014; Tazi et al., 2024).
For chronic disease patients, the benefits include the following: EMRs enable medical records to be stored electronically (Okolo et al., 2024), provide timely access to chronic patient health information and decision-support mechanisms, and augment the quality of decision-making in clinical services. Adoption of the EMR enables the monitoring of disease changes over time in clinical practice and engages patients in the process of disease management (Milani et al., 2016).
However, despite the benefits of EMRs, it is inevitable that the patients raise privacy concerns, with chronic disease patients perceiving threats from the collecting, recording, and analyzing of their personal medical data.
Meanwhile, patient-centered communication, quality care rating, and the frequency of visiting providers are grouped together as clinical factors affecting the frequency of EMR usage. Clinical factors are embedded into patients' and healthcare providers' potential for shared knowledge and interests in clinical settings, mutual understanding of exchanged information for both patients and healthcare providers in clinical settings, organizational environment of clinical settings, and the reciprocal relationship between patient and physician containing the typification of expected behaviors in clinical settings (Kim et al., 2024). Therefore, offline patient-centered communication with doctors in hospitals, the quality of care chronic disease patients receive from clinicians, and the frequency of chronic disease patients visiting healthcare providers regularly in clinics can be included in the scope of clinical factors.
While information privacy concerns may restrain the frequency of EMR use, an expected increase in care quality encourages patient disclosure to healthcare providers via face-to-face situations (Campos-Castillo & Anthony, 2015). In healthcare settings such as clinics, the relationships between patients, healthcare providers, and information systems should be understood in a comprehensive manner.
Given the complexity of the relationship between EMRs and patient information disclosure, information foraging theory (IFT) offers a valuable lens for understanding the factors that influence the use of EMRs among chronic disease patients, particularly when considering information security and clinical factors. IFT suggests that individuals behave similarly to foragers in the wild, seeking to optimize their information gain while minimizing the effort and risks associated with obtaining that information (Hong et al., 2020; Olsson & Brown, 2006).
This approach is highly relevant for analyzing EMR usage, as patients constantly balance the benefits of accessing valuable health information against perceived threats to their privacy and the effort required to navigate digital systems. Patients with chronic conditions often express concerns over the security of their personal health data, fearing unauthorized access and potential misuse. These privacy concerns can result in information withholding behaviors, where patients choose not to disclose certain health details to their providers, affecting the overall quality of care they receive. Applying IFT helps clarify why some patients are reluctant to fully utilize EMRs.
From an IFT perspective, patients engage in a cost–benefit analysis, weighing the perceived security of EMRs (a “cost”) against the benefits of comprehensive health monitoring and management (an “information reward”). In terms of clinical factors such as PCC, quality of care, and the frequency of visiting healthcare providers, IFT provides insights into how these factors influence a patient's engagement with digital health tools. Patients are more likely to “forage” for information in EMRs if they perceive that their interactions with healthcare providers will be enhanced by the digital tool, allowing for improved communication, better understanding of their health status, and more personalized care. Effective communication and frequent interactions with providers serve as motivators, increasing the perceived informational value of EMRs and justifying the potential cognition and emotion effort required to engage with them. When clinical factors align with patient needs, the :information patches” (i.e., the resources provided) available through EMRs are seen as more valuable, encouraging greater usage.
Information security related to EMR
Information withholding
EMR software is common in health settings. However, data privacy and security challenges persist and impede patients' willingness to disclose health information to their clinicians (Ajayi et al., 2023). Consequently, a lack of confidence that providers are able to protect chronic disease patients' persistent medical information may result in their withholding information from the provider (Agaku et al., 2014). Although patients withholding information from health providers may undermine medical treatment and create barriers for appropriate diagnoses, individuals are still more likely to withhold their medical information when there are increased concerns about information security.
Privacy concerns towards information confidentiality is not a new phenomenon. With the advent of the information era, patients' privacy concerns have grown about information collection, the possible second-hand use of recorded information, and unauthorized access to private health information, thereby compressing EMR adoption (Kuo et al., 2014). Often, chronic patients' medical records contain sensitive information about blood pressure readings, weight readings, even sexually transmitted diseases, abortions, and emotional issues, all of which are stored in EMRs (Keshta & Odeh, 2021). Therefore, the inference is that if chronic patients perceive a threat to their personal health information from advanced information technologies such as EMRs, they will adopt behaviors to withhold their information to mitigate the privacy risk. Therefore, in light of information privacy concerns, the frequency of using EMRs may be affected. Thus, we hypothesize the following:
Confidence in EMR safeguards
Previous studies have indicated that a majority of individuals are very concerned about the impact of EMRs on privacy and security (Luo et al., 2021). Patients are concerned about the privacy of their information and its security as it is stored and transferred across the healthcare system (Enaizan et al., 2020). How individuals seek out and obtain health information affects their perceptions related to the privacy and security of their medical information. If individuals believe their health providers are using electronic modes of storing or sharing health information, their levels of confidence are more like to be impacted (Alaqra et al., 2018).
Prior health information research has documented that healthcare providers can mitigate privacy and security concerns by developing more effective privacy safeguards to prevent security attacks and unauthorized access to information (Kisekka & Giboney, 2018). In the context of health information research, the factor of safeguards (“How confident are you that safeguards, including the use of technology, are in place to protect your medical records from being seen by people who are not permitted to see them?”) has been examined, and the results confirm that healthcare providers need to reinforce technological safeguards, such as secure and encrypted communication, and clearly communicate how patients' medical information is accessed, stored, and used in order to honor patient privacy preferences and potentially address patients' concerns in this area (DePuccio et al., 2020).
Therefore, healthcare providers should be transparent with patients by providing clear information about how the security and privacy of patient data are preserved, under what circumstances data is shared, and with whom (Kisekka & Giboney, 2018). Additionally, this factor is part of the service quality of the healthcare system; thus, an increase in confidence around information security enables an increase in the use of EMRs (Enaizan et al., 2020). Based on this research avenue, the stronger the perception of information safety that patients hold, the higher the frequency of EMR adoption. Thus, it is hypothesized that:
Electronic medical information maintenance
Electronic medical information maintenance is the assessment of whether or not chronic disease patients believe their medical records are maintained by their providers through EMR systems. Prior research indicates that the majority of patients believe providers maintain EMR systems, where their medical information is stored (Finney Rutten et al., 2014; Gejdos et al., 2011).
Although using EMR systems has the potential to enable patient engagement and healthcare quality improvement (Finney Rutten et al., 2014), EMR adoption requires prudence: in order to maximize the potential benefits, healthcare for patients should be assessed through the providers' use of EMR to ensure that this health information technology is capable of facilitating healthcare processes and improving healthcare outcomes. Based on the existing literature, the first step in evaluating patient perceptions of the providers' use of EMR systems is examining the influence of EMRs on patients' engagement experiences (Hesse & Shneiderman, 2007). A prior study revealed that the majority of patients (86%) believe that their providers maintain an EMR (Finney Rutten et al., 2014). Other relevant studies have documented that greater numbers of patients receive healthcare services from different types of care settings that are more likely to maintain EMRs (Medical Group Management Association, 2010) and show a positive evaluation of the meaningful use of EMRs in healthcare maintenance organizations (Manca, 2015). Therefore, we hypothesize that:
Clinical factors
Quality of care
Quality of care reflects the patient's satisfaction level with their healthcare and aims to examine healthcare delivery quality (Chou et al., 2010; Rosenthal & Shannon, 1997; Urden, 2002).
Patients' self-reported ratings of the quality of care they receive is representative of enabling quality and equitable healthcare delivery (Chou et al., 2010). In existing studies, patients' quality of care ratings are compiled using the strategy of evaluating specific health practices and health interventions (Patwardhan & Patwardhan, 2009; Rosenthal & Shannon, 1997). Importantly, chronic disease patients who tend to avoid healthcare providers downgrade the rating of healthcare quality, which is a salient implication for quality of care and emphasizes that healthcare teams need to increase patients’ involvement in their care, especially for chronic disease patients (Arora et al., 2009; Epstein & Street, 2007). Prior studies also show that patients without active engagement in their care are less likely to utilize preventive services and more likely to experience poor health outcomes (DeVoe et al., 2003; Finney Rutten et al., 2014). Furthermore, concerning the association between the quality of care rating and EMR adoption, previous studies have indicated that when assessing patients' perceptions of EMRs, the ratings for quality of care were higher for patients who got involved with patient-use EMR utilization when compared with those whose healthcare providers who did not maintain EMRs (Smith & Bartell, 2004). This indicates that through the use of EMRs, patients' healthcare quality satisfaction can be improved and, subsequently, they may continue using EMRs. Therefore, we hypothesize that:
Patient-centered communication
Patient-centered communication (PCC) is a diverse aspect of the provider–patient relationship, including patient-as-a-person, the provider sharing power with the patient, mutual therapeutic alliances, patient engagement in healthcare, routine patient feedback to doctors, integrated team care, and clinical information systems supporting higher quality care for the patient (Davis et al., 2005; Liu et al., 2023; Mead & Roland, 2009; Vikkelsø, 2010).
Whether PCC and EMRs jointly benefit one another, either in chronic disease patients or in patient–healthcare provider relationships, is not known well. The extant research presents contrasting opinions of PCC and EMR interaction. Holden and Karsh (2009) found no evidence that either patient–healthcare provider interaction or EMR adoption influenced the final heath outcome of diseases. Other researchers have indicated that the utilization of EMRs diminishes nonverbal behaviors, thereby worsening patient–provider interaction (Street et al., 2014). According to the above complex research results, it is necessary to link back to the definition of PCC and then draw out relevant cues.
In the context of communication, PCC occurs when patients perceive that they have a shared understanding of their health issues with their healthcare providers and shared power in health decision-making (Epstein et al., 2005; Epstein & Street, 2007). In other words, PCC expands patient choice and communication channels with providers, while EMRs empower patients to access to their own health information and also open communication channels (Epstein et al., 2005). Under this status quo, patients perceive that EMRs are an important means of assisting them at the point of care through their use (Shachak & Reis, 2009). If healthcare providers are experienced at facilitating the interaction with patients and EMRs, the effectiveness of using EMRs will be realized (Shachak et al., 2009). To follow the above research dimension, it can be hypothesized that:
Frequency of visiting healthcare providers
The frequency of visiting healthcare providers literally assesses whether chronic disease patients access healthcare providers on a regular basis (Senft et al., 2019; Sudore et al., 2006). The effective self-management of chronic health issues needs a relatively high level of understanding of healthcare providers, proper access, and continuous medication care (Senft et al., 2019). In the treatment process, having a regular doctor or health source is crucial for patients. Extant research indicates that when dealing with chronic conditions, physicians need good health facilities and positive relationships with patients (Manca, 2015). Therefore, the process of patients visiting regular providers offers a greater likelihood of building close relationships with healthcare providers, which assists patients in achieving better chronic disease management (Kern et al., 2013; Manca, 2015). A prior study suggested that providers need tools to improve access to information and relationships (Finney Rutten et al., 2014). Here EMRs, as an associated information technology, provide access to information and resources. Additionally, researchers have shown that patients who have not visited or seldom seen healthcare providers are less likely to use health information technologies, including EMRs, to communicate with healthcare providers (Sudore et al., 2006). From the above, it is hypothesized that:
As a new heath information technology, EMRs are only now beginning to be widely used in clinical settings. Consequently, there is little published research about the effectiveness of using EMR, which requires mixed and integrated rationales to explain and predict it. Faced with this complexity, the purpose of the present research is to understand how the above factors affect the frequency of EMR use and how these factors change over time to impact on the frequency of EMR adoption (see Figure 1).
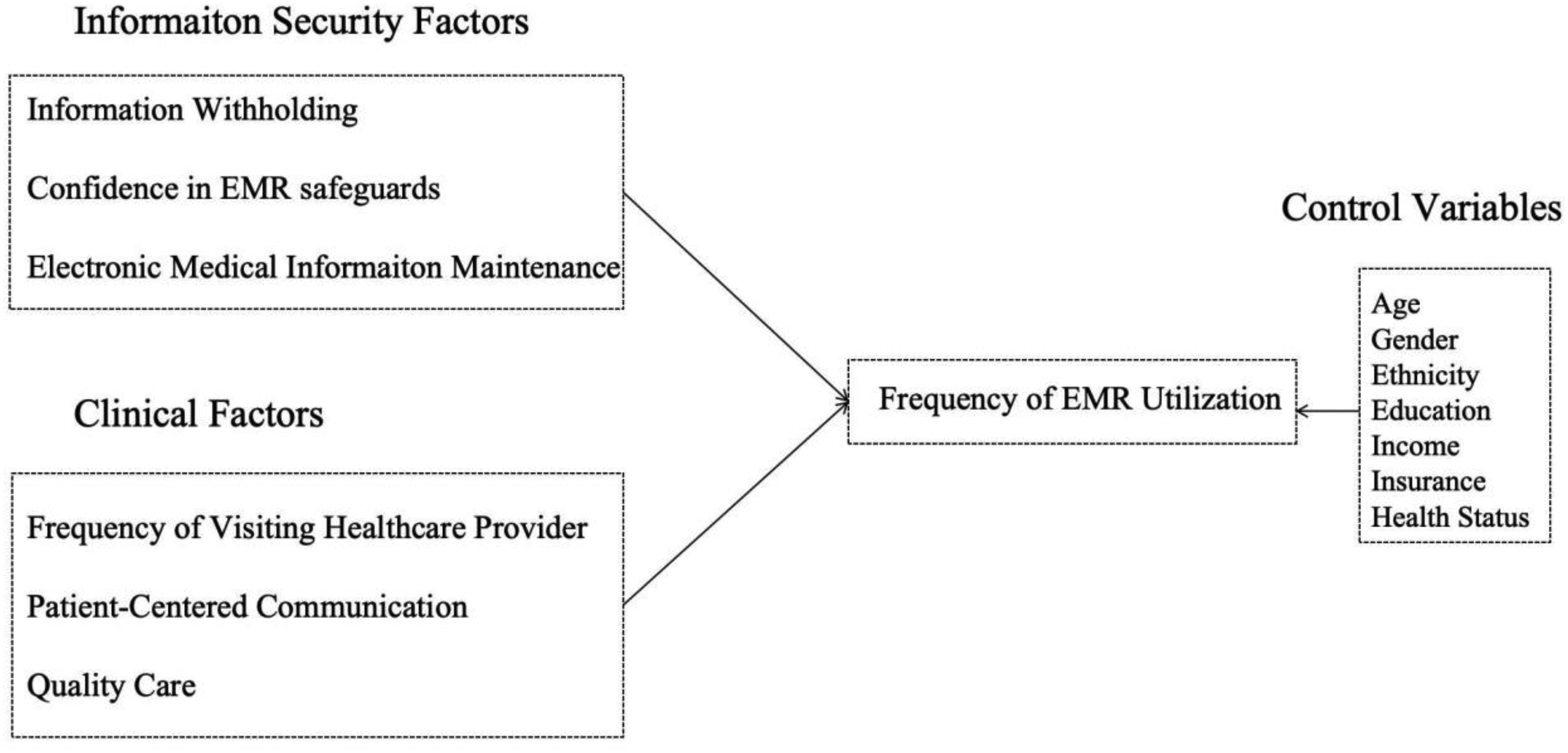
Research model.
Method
Data source
Data from the three administrations of the US-based Health Information National Trends Survey (HINTS) fielded from 2014 to 2018 were analyzed. The study analyzed the data from HINTS 4-Cycle 4 in 2014 (fielded 20 August–17 November; response rate = 34.44%), HINTS 5-Cycle 1 in 2017 (fielded 25 January–5 May; response rate = 32.39%), and HINTS 5-Cycle 2 in 2018 (fielded 26 January–2 May; response rate = 32.85%). As the study revolves around the frequency of using EMRs, participants were included who suffered from any of the following six types of chronic illness: diabetes, high blood pressure, heart condition, lung disease, arthritis, and depression. The participants from each wave had similar characteristics, and the survey items were the same across the three waves.
To examine whether these predictors were constant over the years, hierarchical multiple regression models were employed to predict the frequency of EMRs usage in the three waves of HINTS. In all the regression models, social demographic characteristics were first entered as control variables, followed by information-privacy-concern-related factors and clinic-related enablers as independent variables, and frequency of EMRs usage was treated as the dependent variable. The consistency observed across the three survey waves is attributed to the participants’ similar characteristics and the use of the same survey items and questions in each round.
Study variables
Information withholding
In each survey year, this was measured by one binary item. Here, a determinant question emerging from patients’ privacy concerns is related to the collection, use, disclosure, and control of their private health information with EMRs (Caine & Hanania, 2012). The dichotomous item of privacy within patients’ medical records is “Have you ever kept information from your healthcare provider because you were concerned about the privacy or security of your medical record?” (1 = Yes; 0 = No).
Confidence in EMR safeguards
For this variable, the first source of information was assessed in 2014, 2017, and 2018 with the following item: “How confident are you that safeguards (including the use of technology) are in place to protect your medical records from being seen by people who aren’t permitted to see them?” Responses were scored on a 3-point Likert scale (1 = Very confident; 3 = Not confident). In the process of data cleansing, the scale was reverse coded, with “Not confident” coded as 1 while “Very confident” was coded as 3.
Electronic medical information maintenance
This study variable was measured by employing a binary item. Respondents were asked the following question to assess whether they believed that healthcare providers maintained patients’ medical records in an electronic system: “As far as you know, do any of your doctors or other healthcare providers maintain your medical records in a computerized system?” (1 = Yes; 0 = No).
Quality of care
This variable was assessed by constructing five items that asked the respondents to rate the quality of their healthcare in the preceding 12 months. As can be seen, this variable was based on the individual’s overall rating of healthcare quality (Chou et al., 2010). The question was phrased as: “Overall, how would you rate the quality of healthcare you received in the past 12 months?” To improve interpretation, the scale was treated as interval, and scores were reverse coded (1 = poor; 5 = excellent).
Frequency of visiting healthcare providers
For this variable, the item was aiming to see whether offline behaviors and the frequency of visiting doctors or other health professionals had an influence on the use of EMRs. Respondents were asked to select the number of times they visited their doctor or other healthcare provider (0 = none; 1 = 1 time; 2 = 2 times; 3 = 3 times; 4 = 4 times; 5 = 5–9 times; 6 = 10 or more times).
Patient-centred communication
PCC was assessed using seven items used in patient-centeredness measures from the past HINTS datasets (Jiang & Street, 2016). These seven different items asked about interactions with health professionals in the preceding 12 months. Respondents were asked to identify the degree to which they agreed with the following statements: “How often did they give you the chance to ask all the health-related questions you had?,” “How often did you get the attention you needed for your feelings and emotions?,” “How often did they involve you in decisions about your healthcare as much as you wanted?,” “How often did they make sure you understood the things you needed to do to take care of your health?,” “ How often did they explain things in a way you could understand?,” “How often did they spend enough time with you?,” and “How often did they help you with feelings of uncertainty about your health or healthcare?” Responses included always (1), usually (2), sometimes (3), and never (4), which were reverse coded.
Frequency of EMR utilization
One item was selected to measure the frequency of using EMRs. Respondents were asked: “How many times did you access your own personal health information online through a secure website or app in the last 12 months?” (0 = None; 1 = 1 to 2 times; 2 = 3 to 5 times; 3 = 6 to 9 times; 4 = 10 or more times).
Sociodemographic and health-related variables
These were viewed as controls to decrease possible confounding effects. Sociodemographic variables included gender, age, education, ethnicity, and income. Health-related variables included health insurance and health status. All items are available on the HINTS website (hints.cancer.gov).
Data analysis
SPSS (version 23) was used to complete the descriptive analysis, one-way ANOVA, and hierarchical multiple regression. Demographic characteristics and the focal variables were compared by evaluating changes in the means and standard deviations. The relevant results are displayed in Table 1. The one-way ANOVA revealed significant changes, as presented in Table 2. Finally, the hierarchical multiple regression model for testing variables was used for each wave (Table 3). Regarding missing values, the grand mean was utilized to replace these to generate complete datasets from the three waves.
Results
Sample characteristics
The sociodemographic statistics from 2014 to 2018 are presented in Table 1. The total sample sizes in the three surveys were 2,415, 2,253, and 2443 in 2014, 2017, and 2018, respectively. Overall, no significant changes were observed in the means of education, age, or income between the three waves. Additionally, the majority of participants were white (68.6% in 2014, 71.8% in 2017, and 70.4% in 2018). Importantly, the variable Frequency of EMR Utilization increased two-fold between 2014 and 2018.
Main Variables and Their Descriptive Statistics Across Trends.
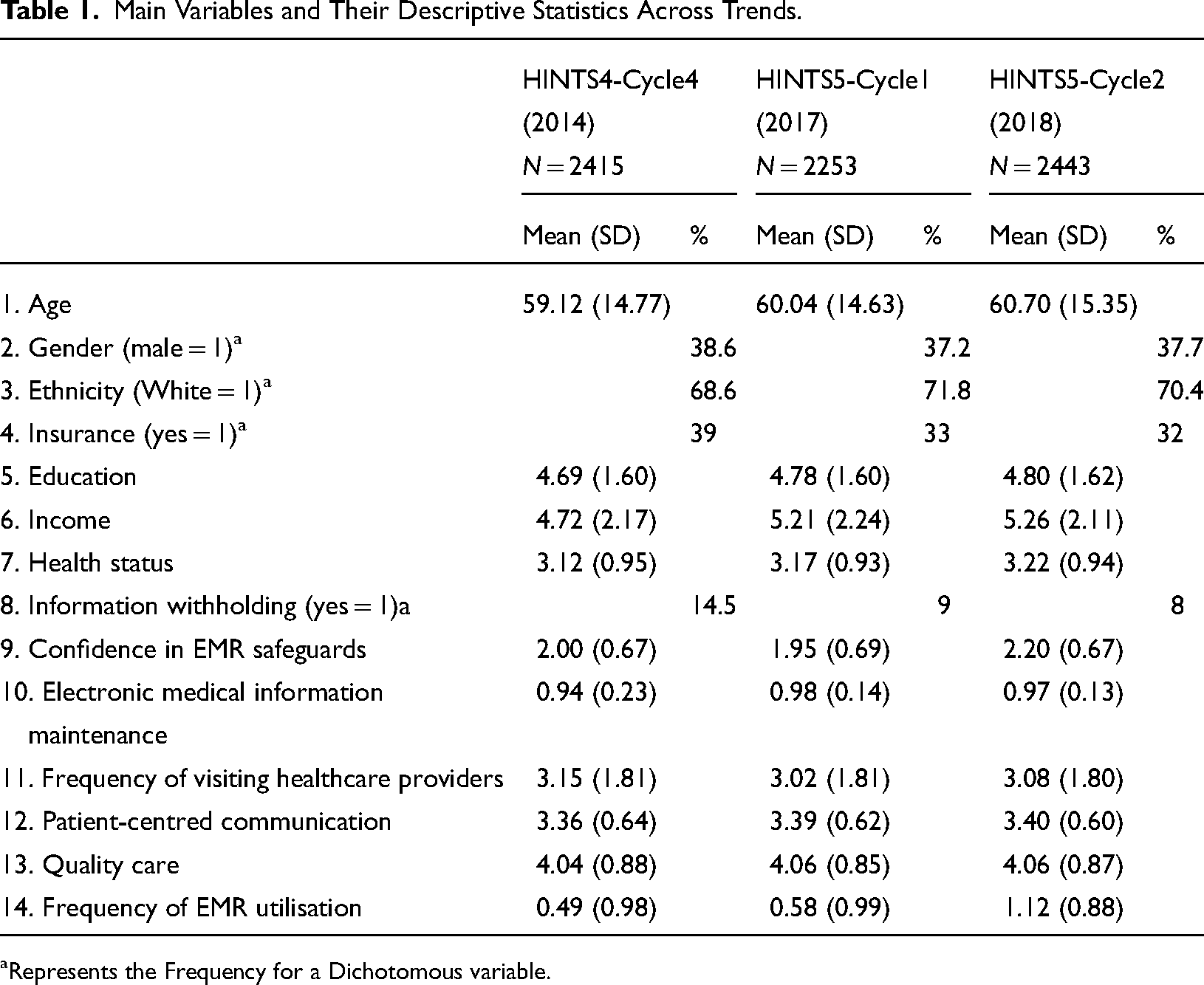
Represents the Frequency for a Dichotomous variable.
Trends of EMR utilization
Table 2 depicts the results of the variables predicting Frequency of EMR Utilization.
Hierarchical Multiple Regression Models Predicting Frequency of EMR Utilization across Trends.
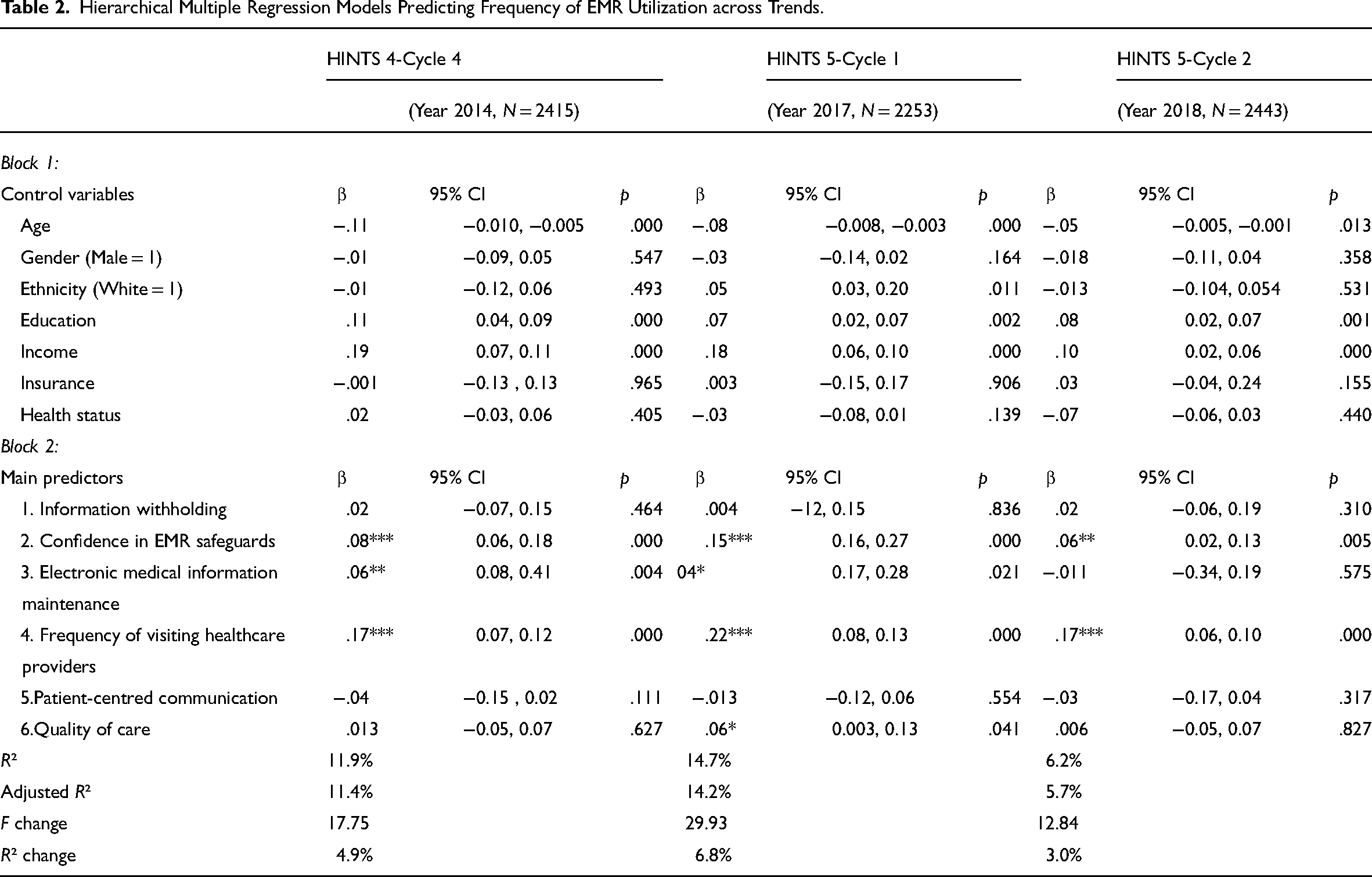
In terms of the demographic characteristics, age, education, and income were significantly related with frequency of EMR utilization in all three waves. Over time, among EMR users with chronic diseases, ethnicity was only significantly associated with the frequency of using EMRs in 2017. By contrast, insurance, gender, and health status were not related to the frequency of EMR utilization in 2014, 2017, or 2018.
Regarding focal factors, confidence in EMR safeguards and the frequency of visiting health providers were significant predictors in 2014, 2017, and 2018, affecting the frequency of EMR utilization differently over time. Quality of care showed a significant and linear correlation with the frequency of EMR utilization in 2017, but not in 2014 or 2018. Additionally, in 2014 and 2017, electronic medical information maintenance was found to be a significant predictor towards the frequency of using EMR, but this was not found to be the case in 2018. However, factors such as patient-centered communication and information withholding were insignificantly related with the frequency of EMR utilization in 2014, 2017, and 2018.
As shown in Table 3, information withholding, confidence in EMR safeguards, electronic medical information maintenance, frequency of visiting health providers, and frequency of EMR utilization varied significantly over time. From the results so far, it can be seen that there are statistically significant differences between the waves as a whole. As shown in Table 4, multiple comparisons reveal which factors in which waves differ from each other. Through the post hoc test, information withholding and electronic medical information maintenance were found to have statistically significant differences between 2014 and 2017, as well as between 2014 and 2018. However, between 2017 and 2018, the above factors showed no significant differences. Importantly, in each of 2014, 2017, and 2018, information safety and frequency of EMR utilization were found to have statistically significant differences.
Descriptive Statistics and One-way ANOVA Results for Trends.
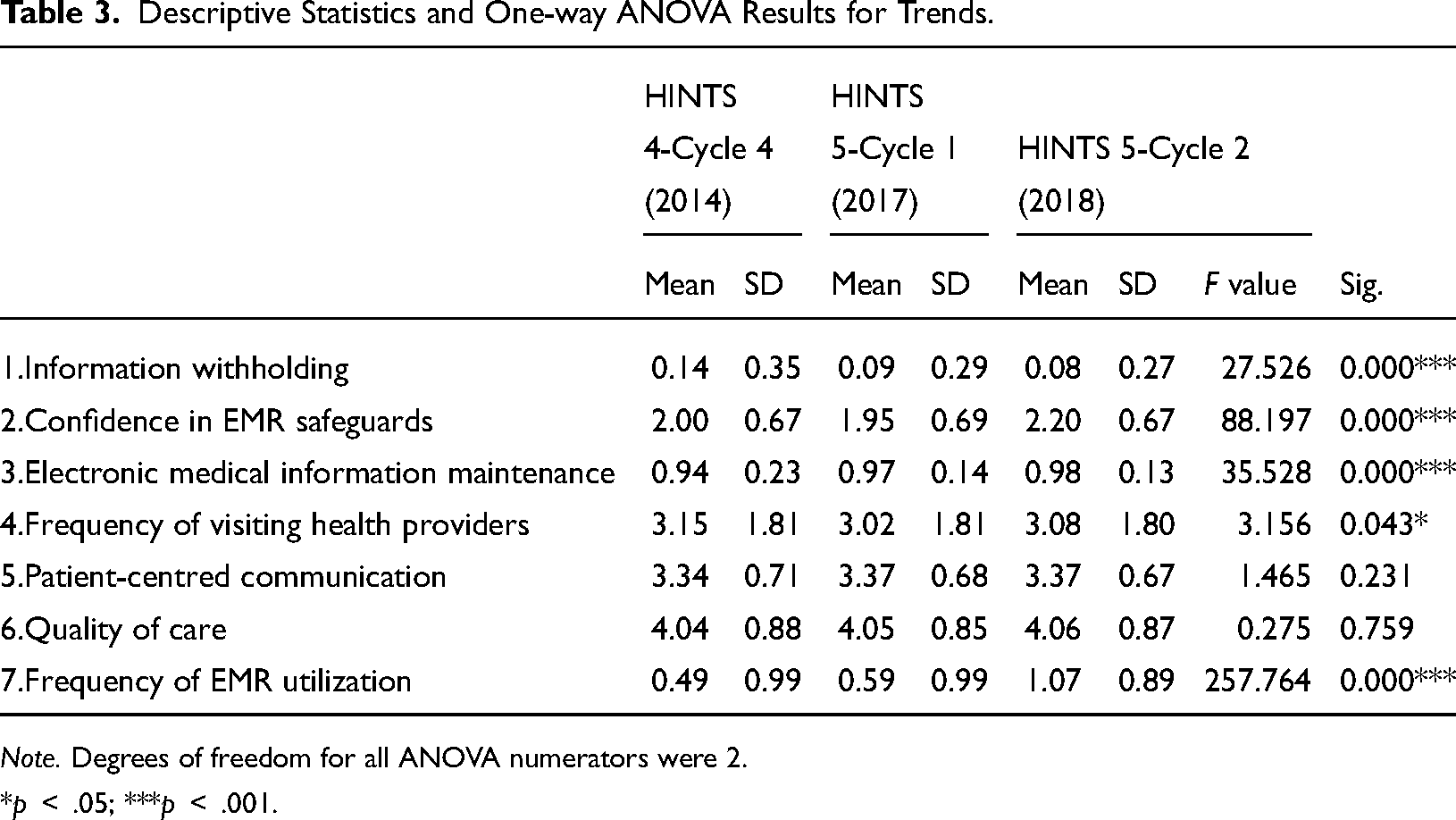
Note. Degrees of freedom for all ANOVA numerators were 2.
*p < .05; ***p < .001.
Post Hoc Tukey Test Results for ANOVA for Trends.
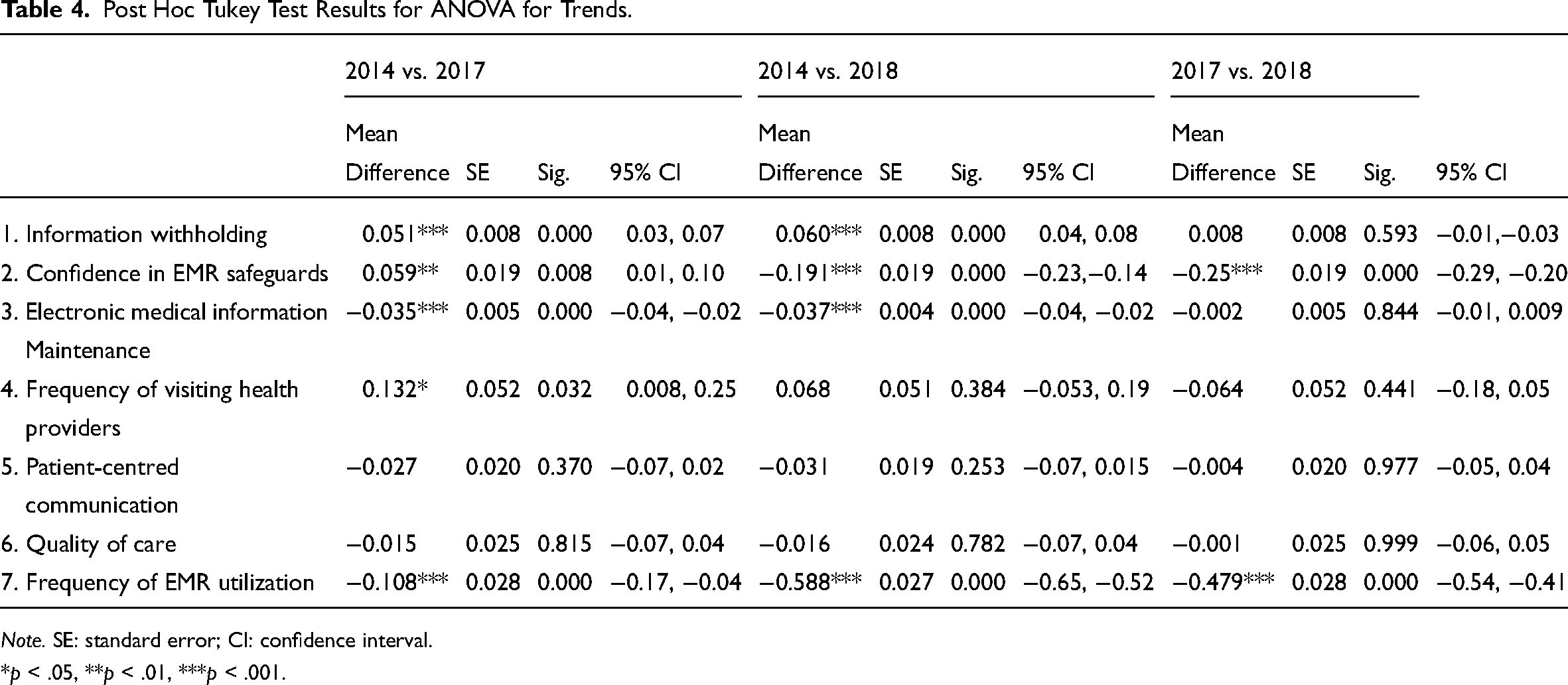
Note. SE: standard error; CI: confidence interval.
*p < .05, **p < .01, ***p < .001.
Discussion
Principle findings
This study builds on prior research by extending the focus beyond traditional privacy concerns to include both technological and clinical factors that influence the use of EMRs by chronic disease patients. Drawing on information foraging theory (IFT), this research positions EMR usage as an adaptive behavior driven by the patient’s need to retrieve relevant health information while minimizing effort and risk. The primary goal of this study was to explore how these factors—such as confidence in EMR safeguards, the frequency of visiting healthcare providers, and the quality of care—shifted over time and contributed to increased EMR utilization in 2014, 2017, and 2018. The study’s findings indicate that chronic disease patients increased their usage of EMRs over time, driven by the dual forces of technological assurance (such as confidence in EMR safeguards) and clinical interaction (such as frequency of visiting healthcare providers). This aligns with the IFT premise that information receivers (patients) will continuously forage in an environment where the benefits of acquiring information—such as improved health literacy and management.
Changing factors influencing frequency of EMR utilization
Chronic disease patients’ perceptions of medical information security are essential indicators of whether or not they will adopt the frequent use of electronic health information technology. From the results of the present study, it can be seen that increasing utilization of EMRs among chronic disease patients occurred in 2014, 2017, and 2018. This indicates that, on the one hand, EMRs provide chronic disease patients with the tools to better understand their health status, while on the other hand, confidence in EMR safeguards and electronic medical information maintenance and offline mutual patient–provider interaction may buffer information privacy concerns, thereby motivating patients’ activation of using EMRs.
On the basis of the above analysis, confidence in EMR safeguards—in that safeguards were in place to protect patients’ medical information from being accessed by unauthorized persons—were continuously and positively associated with patient-use EMR across the years of study. This finding suggests that in spite of the rise in ubiquity of EMR-based public health information privacy breaches, a growing confidence in healthcare providers to protect their medical records in their computerized systems outweighs any information privacy concerns. A plausible explanation for this is that trust towards healthcare providers may augment chronic disease patients’ confidence because patients who engage with medical professionals on a regular basis have a relatively higher degree of trust in their doctors or physicians (Kuo et al., 2014).
When it comes to building trust, during ward rounds, the use of the EMRs tends to peak between 6:00 am and 10:00 am, coinciding with the start of routine work. Information access via desktop PCs is often limited during the early hours, making it inconvenient for doctors to track investigation statuses and monitor chronic disease patients (Kim et al., 2017). In this context, EMRs become essential for recording sensitive patient information and facilitating communication between doctors and patients, but not unauthorized individuals. By providing immediate access to investigation results and patient conditions, EMRs greatly assist in clinical decision-making. Moreover, the secure handling of sensitive information through EMRs fosters trust among patients, as they feel reassured that their data is well protected. This data security strengthens patients’ confidence in the system, reinforcing the value of EMRs in healthcare settings.
The regular interpersonal interactions between chronic disease patients and their healthcare providers fosters a collaborative approach to care. EMRs facilitate this communication by ensuring that doctors and patients have real-time access to updated health records. Each visit encourages the active use of EMRs to review past treatments and plan future care, enhancing communication efficiency during consultations. Moreover, EMRs support patient engagement by providing portals for patients to access their medical records, lab results, and treatment recommendations between visits, which can improve compliance and understanding of their chronic disease management plans (Dendere et al., 2019).
At the same time, EMRs enable healthcare providers to easily check previous test results and treatment histories, minimizing the likelihood of repetitive testing, thus optimizing care efficiency. What is more, chronic diseases such as diabetes require long-term tracking of various health metrics. Frequent visits lead to more detailed and cumulative data stored in the EMR. This data accumulation allows doctors to spot trends, predict disease progression, and adjust treatment plans accordingly.
In line with prior studies, this study found no direct effect of patient-centred communication (PCC) on the frequency of EMR utilization (Jiang & Street, 2016; Totzkay et al., 2017). One plausible explanation is that both PCC and EMR utilization may be need-supportive, with patient activation and involvement as mediators. Specifically, PCC offers patients choices and fosters communication engagement, while EMRs empower patients with access to health information and various communication platforms—both of which require patient activation. Patient activation, as a mediator, can be influenced by PCC and, in turn, affects self-determined health behaviors, such as using EMRs. This points to a mediated relationship between PCC and EMR utilization rather than a direct effect. Instead of a direct effect, PCC can be viewed as a need-supportive communication process that indirectly influences the self-determination of EMR usage. The findings suggest that, in the future, healthcare providers should prioritize patient activation through PCC and then promote EMR adoption as part of adherence to recommendations.
Previous research using 2011 HINTS data documented that patients who had concerns about the security of faxed and electronic data were more likely to withhold medical information from their healthcare providers, potentially compromising the effectiveness of health surveillance systems (Agaku et al., 2014).
Unlike Agaku’s (2014) study, the present research found no such relationship in the 2014, 2017, or 2018 data, and we specifically focused on individuals with chronic diseases, which may account for the difference in findings. The maintenance of electronic medical information, where providers store patients’ medical information in computerized systems, was associated with the frequency of EMR use in 2014 and 2017 but not in 2018. From these findings, despite concerns over information privacy, it appears that patients may prioritize their need for healthcare resources and view the delivery of higher-quality care as a sign that providers are handling their private medical information responsibly.
Early on, EMR systems were still relatively novel, and patients might have been more conscious of whether providers were using them consistently. Knowing that providers maintained these electronic records could have increased patients’ trust in EMR systems, encouraging their use. By 2017 and 2018, EMR systems had become more mainstream across various healthcare settings. Patients may have begun to assume that providers were maintaining electronic records as standard practice, reducing the influence of this factor on their engagement. As EMRs became the norm, patients’ engagement may have started depending more on other aspects of EMR utility, such as usability, accessibility, or data security, rather than the mere fact of EMR maintenance. As patients became more accustomed to EMR use, their focus may have shifted toward specific features like data security, ease of access, and interoperability between providers.
In 2017 and 2018, the factor, confidence in EMR safeguards emerged as a stronger predictor, suggesting that patients were more concerned about the security and reliability of these systems, rather than just their existence. What is more, the policy changes between 2014 and 2018 may also help to reshape how patients perceived and interacted with EMR systems, affecting the role of electronic medical information maintenance in their engagement with these systems. For example, the Meaningful Use program encouraged providers simply to adopt EMRs, and patients saw these systems primarily as digital record-keeping tools. However, by 2014, requirements under Stage 2 of Meaningful Use had started to emphasize patient access to electronic information and secure provider-patient messaging. As a result, patients became increasingly aware that EMRs could offer more than just record maintenance; they could facilitate direct, meaningful engagement with their healthcare providers. In 2017 and 2018, as EMRs became standardized for these functional aspects, patients expected these advanced features and became less focused on whether their records were simply maintained electronically.
Examining the relationship between quality of care and frequency of EMR usage, our research found that the connection between these two factors was unstable and inconsistent, appearing significant only in 2017. One possible explanation is that the study focused on patients with chronic illnesses—such as diabetes, high blood pressure, heart conditions, lung diseases, arthritis, and depression—who require continuous monitoring of health indicators, consistent reviews of treatment plans, and a high degree of self-management. These conditions often demand lifelong medical support. As a result, it can be challenging to accurately assess the quality of care received by patients over a short one-year period and to determine the continuity of improved care quality within the three assessment points. Additionally, given the positive trends in EMR adoption within healthcare settings, research findings highlight the need for continued research to monitor patient experiences with EMRs and to evaluate how these systems impact care processes.
Practice implications
Despite several limitations, this study has important practice implications. Although the benefits of EMRs in healthcare settings such as hospitals are recognized, EMR adoption is still surprisingly low in the USA. In our research, it was found that merely considering privacy breach concerns was not a sufficient reason to elucidate the tempered enthusiasm for EMR usage. On the basis of this study, technological improvements and clinical factors such as electronic communication modes and the patient–doctor relationship, both of which build trust and confidence towards healthcare providers, should go hand-in-hand and cannot be separated in healthcare ecology.
On the one hand, health information technology should be designed to be meaningfully used to support healthcare services. On the other hand, because patients care about how provider-used EMR systems store and transfer their private information across computational systems, providers and other caregivers should be responsible for providing a full explanation of EMR operation mechanisms to strengthen patient trust and mitigate negative side effects. Healthcare organizations should seek to strike a balance between patient satisfaction in terms of quality of healthcare, the workload control of using EMRs for providers, and the management of information confidentiality. All in all, electronic health systems need an integrated approach based upon appropriate measures. Our study can be an important reference for improving the quality of healthcare via electronic health systems as well as psychosocial factors.
Limitations and future research
Several limitations of our study should be noted here. First, two variables, information withholding and electronic medical information maintenance, were measured using a single and a dichotomous item, respectively. Future research should take account of multiple items to measure multidimensional health-information-related behaviors to ensure validity, reliability, and accuracy.
Second, because HINTS was administrated to institutionalized chronic disease patients, the findings might be biased for other chronic illness individuals in the outpatient environment. For future iterations of HINTS surveys, it is necessary to avoid the above bias and try to better target more chronic disease patients.
Third, all responses in HINTS were self-reported. In particular, the dependent measure asking patients how many times they had accessed their online medical records in the past 12 months may lead to inaccurate answers because of respondents’ memory recall.
Fourth, HINTS identifies relatively macro trends at the individual variable level. Future studies may look to measure information security concerns towards withholding behaviors using a more micro-level approach. Qualitative studies may use in-depth interviews to better understand how this concern affects behaviors and electronic mode utilization, and to recognize potential omitted factors.
Fifth, the variables of PCC, EMR adoption, and information holding were measured in the United States context, which may not yield the same results in other cultural contexts. To test its application, future research may seek to test the model in different contexts.
Concluding remark
This study not only offers a privacy-concern-related analysis of the frequency of EMR use but also provides a comprehensive picture including clinical factor assessment of how both online health information communication and offline patient–provider interaction affect the frequency of using EMRs among chronic disease patients over time. From our findings, we conclude that with no effects of privacy breach concerns presented as withholding behavior, the effectiveness of information safety towards technological safeguards and patient–provider interaction can buffer information privacy and security concerns. In this article, we have suggested that advanced electronic health technologies as well as clinical factors—referring to visiting healthcare providers—should work together in order to transform the healthcare system as a whole.
Footnotes
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Statement
This study was conducted with a commitment to upholding ethical standards in research. The data analyzed were collected from publicly accessible survey sources, with full respect for the privacy and confidentiality of all participants. No personally identifiable information was utilized, ensuring that individual anonymity was preserved. This research aims to contribute to the ethical enhancement of EMR systems, promoting better health outcomes and respecting patient autonomy and data privacy.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Ministry of Education General Project in Humanities and Social Sciences: "Research on Contextual Protection Mechanisms for Personal Information in the Age of Artificial Intelligence", Renmin University of China's "Double First-Class" Initiative Project on the Study of the Marxist View of Journalism [grant number (Project No.24YJC860017), (Project No. MXG202312)], Ministry of Education Major Project of Philosophy and Social Science Research on “The Basic Categories and Theoretical Context of the Autonomous Knowledge System of Journalism and Communication Studies” (2023JZDZ033).