
Abstract
Introduction:
Firearm-related injuries are the leading cause of injury-related deaths among children. This study explores the relationships between pediatric firearm injury incidence, Childhood Opportunity Index (COI) as a measure of social determinants of health (SDOH), state gun laws, and surgical specialties involved.
Methods:
The Pediatric Health Information System (PHIS) was used to identify children diagnosed with firearm injuries and required care from 2015 to 2023. Patient demographics, COI, clinical, and geographic data were examined using univariate analysis, t-tests, and logistic regression. State gun laws were categorized into restrictive, moderate, or permissive based on the Giffords Scorecard and population-adjusted analyses were conducted using U.S. Census Bureau data.
Results:
One thousand six hundred thirty-six children were included, with a mean age of 11.8 ± 5.0 years. Most injuries occurred in males (79.8%) and White children (64.8%). Mortality was positively associated with low COI scores (OR: 1.010, P = .025). Greater distance from hospitals (OR: 1.01, P = .002) had higher rates of mortality while older age was protective (OR: 0.997, P = .021). Permissive states accounted for 76.4% of injuries, 10.4% in moderate states, 13.2% in restrictive states. Population-adjusted analyses showed higher injury incidences in permissive states versus restrictive states (P < .01). Pediatric, orthopedic, and plastic surgery were the most involved surgical specialties.
Conclusions:
Pediatric firearm injuries affect children in neighborhoods with low COI scores, those living farther from hospitals, and in states with permissive gun laws. Plastic surgery was the third most utilized surgical specialty when treating these patients. Further research is needed to inform health policy aimed at mitigating this public health crisis.
Introduction
In 2019 firearm-related injuries overtook motor vehicle crashes as the leading cause of injury-related death among children. 1 As rates continue to rise in recent years, firearm-related injuries hold a tremendous physical, psychological, and societal impact. 2 Previous research regarding the etiology of pediatric firearm injuries have focused on hospital and trauma center experiences, the cost of burden, and firearm injury patterns.3-5 Although the epidemiology of pediatric firearm injuries has been examined, few have explored the intersection of neighborhood and state-level factors in this patient population through the Pediatric Health Information Systems (PHIS) database.
As firearm injuries produce an extensive amount of psychologic and bodily trauma, surgeons, and a multidisciplinary approach are essential to the care of this vulnerable population.6,7 The American Pediatric Surgical Association (APSA) has emphasized the importance of research on this topic to improve care, and advocate for prevention and policy changes to address this public health crisis. 8 As such, additional focus on the social factors and the surgical specialties caring for this patient population will shed light on the societal and clinical variables involved in this public health burden. This study aims to utilize the Pediatric Health Information Systems (PHIS) database to explore the association between reports of inpatient pediatric firearm injury incidences, state-level gun laws as measured by the Giffords Annual Gun Law Scorecard, and social determinants of health by using the Childhood Opportunity Index (COI). COI is a composite measure of the quality of multiple social factors that contribute to a child’s development in their neighborhood, and thus can serve as an indicator of risk. 9 Additionally, this study examines the surgical specialties involved in the operative management, with particular attention to plastic surgery’s role in treating pediatric injuries. Prior studies demonstrated that weaker firearm regulations and associated with increased firearm-related harm. 10 Children residing in areas with low COI and weak gun laws may face environmental stressors that increase vulnerability to violence, thus we hypothesize that children living in states with weaker gun laws and in communities with lower COI scores will experience higher rates of firearm-related injury.
Methods
This study was exempt from approval by the Institutional Review Board. The Pediatric Health Information System (PHIS), a national database containing deidentified data from participating children’s hospitals across the United States, was queried for patients 18 years and younger diagnosed with a firearm injury requiring inpatient surgical treatment. This cohort was determined based on ICD-10 codes listed in Supplemental Material. Provider specialty information from PHIS was also queried to identify the surgical subspecialties involved in operative and nonoperative cases. Subsequently, children requiring inpatient surgical treatment were exclusively studied to narrow the scope to severe injuries and focus on the most severe firearm-related injuries, which represent a subset of highest burden cases on the healthcare system.
Patient zip codes were used to identify the COI level through querying the COI 3.0 dataset. 11 COI identifies areas of disparities and ranks neighborhoods into 5 levels based on the resources and conditions within a neighborhood, such as access to quality schools, healthcare facilities, family poverty rates. The levels are the following: very low (0%-20%), low (21%-40%), moderate (41%-60%), high (61%-80%), and very high (81%-100%). Additionally, patients were matched to a Giffords Annual Gun Law Scorecard grade based on the year and state in which their injury occurred. States with A and B ratings were defined as “restrictive,” states with a C rating were defined as “moderate,” and states with D and F ratings were classified as “permissive.” From 2015 to 2023, population estimates of youths aged 18 and younger were acquired from the U.S. Census Bureau for each census tract and used to adjust for population differences in our analysis. 12 The study included data from 2015 through 2023 to ensure relevance to the latest trends in firearm injuries, COI 3.0 dataset, state-level gun laws, and using years when Giffords Annual Gun Law Scorecard was active.
Univariate analysis was conducted to describe patient demographics, including birth sex, race, ethnicity, age, insurance type, as well as distributions of patients across state gun law categories and COI levels. Continuous variables were compared using t-tests, and categorical variables, such as complication rates, were compared using chi-square tests. Multivariable logistic regression models were used to assess the factors associated with in-hospital mortality and with hospital length of stay. Odds ratios (OR) and 95% confidence intervals (CIs) were reported for each predictor. Statistical significance was defined as P < .05 and all analysis were performed in RStudio version 4.2.1.
Results
A total of 1636 patients met the inclusion criteria for operative cases. Among these patients, 1306 (79.8%) were male and 1060 (64.8%) were identified as White. Mean age at presentation was 11.8 ± 5.0 years (range 0-18 years). Additional patient demographics are summarized in Table 1. Regarding mortality, children with the lowest 20% COI score nationally was positively associated with increased mortality (OR: 1.010 95% CI: 1.004-1.013, P = .025). Whereas older age was negatively associated with mortality (OR: 0.997, 95% CI: 0.995-0.999, P = .0213). Those identified on public insurance were associated with a significantly prolonged hospital length of stay (OR: 4.77, 95% CI: 1.12-20.34, P = .0349), and increased distance from the hospital was associated with an increase in the probability of mortality (OR: 1.01, 95% CI: 1.003-1.015, P = .0020). Census region was associated with higher firearm wound mortality (OR: 1.03, 95% CI: 1.01-1.06, P = .011).
Table of the Patient Demographics, Regional Differences, and Clinical Events of Pediatric Firearm-Related Injuries in the United States.
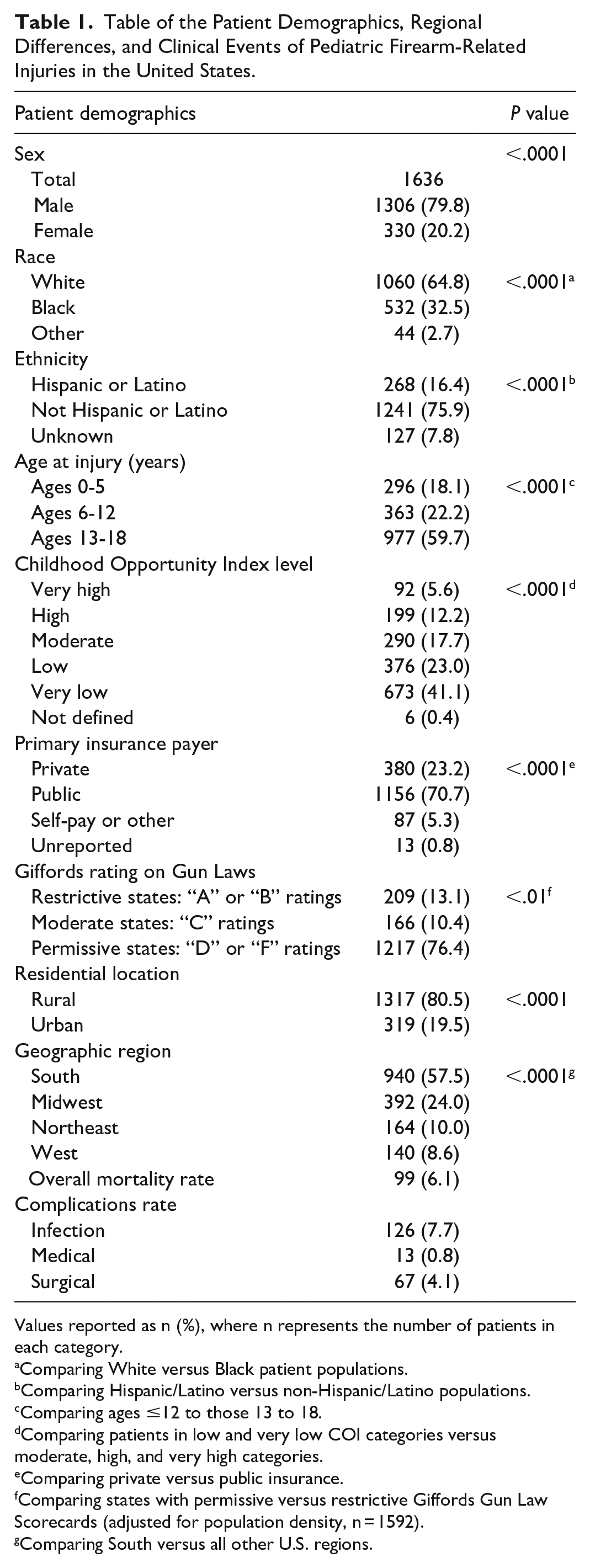
Values reported as n (%), where n represents the number of patients in each category.
Comparing White versus Black patient populations.
Comparing Hispanic/Latino versus non-Hispanic/Latino populations.
Comparing ages ≤12 to those 13 to 18.
Comparing patients in low and very low COI categories versus moderate, high, and very high categories.
Comparing private versus public insurance.
Comparing states with permissive versus restrictive Giffords Gun Law Scorecards (adjusted for population density, n = 1592).
Comparing South versus all other U.S. regions.
In this study, 1592 youths were available for Giffords Annual Gun Law Scorecard grade analysis. Most firearm-related injuries occurred in permissive (D and F ratings) states, 1217 cases (76.4%), followed by 209 (13.2%) in restrictive (A and B ratings) states, and 166 (10.4%) in moderate (C rating) states. After adjusting for differences in population density, there demonstrated a significant increase in firearm-related injury incidences in states with “permissive” gun laws when compared to “restrictive” gun laws (P < .01).
Additionally, a sub-analysis was conducted to determine specific specialty involvement in operative and nonoperative management of pediatric firearm-related injuries. This sub-analysis revealed that following pediatric surgery, orthopedic, and plastic surgery were the second and third most involved surgical specialties, respectively (Figure 1).
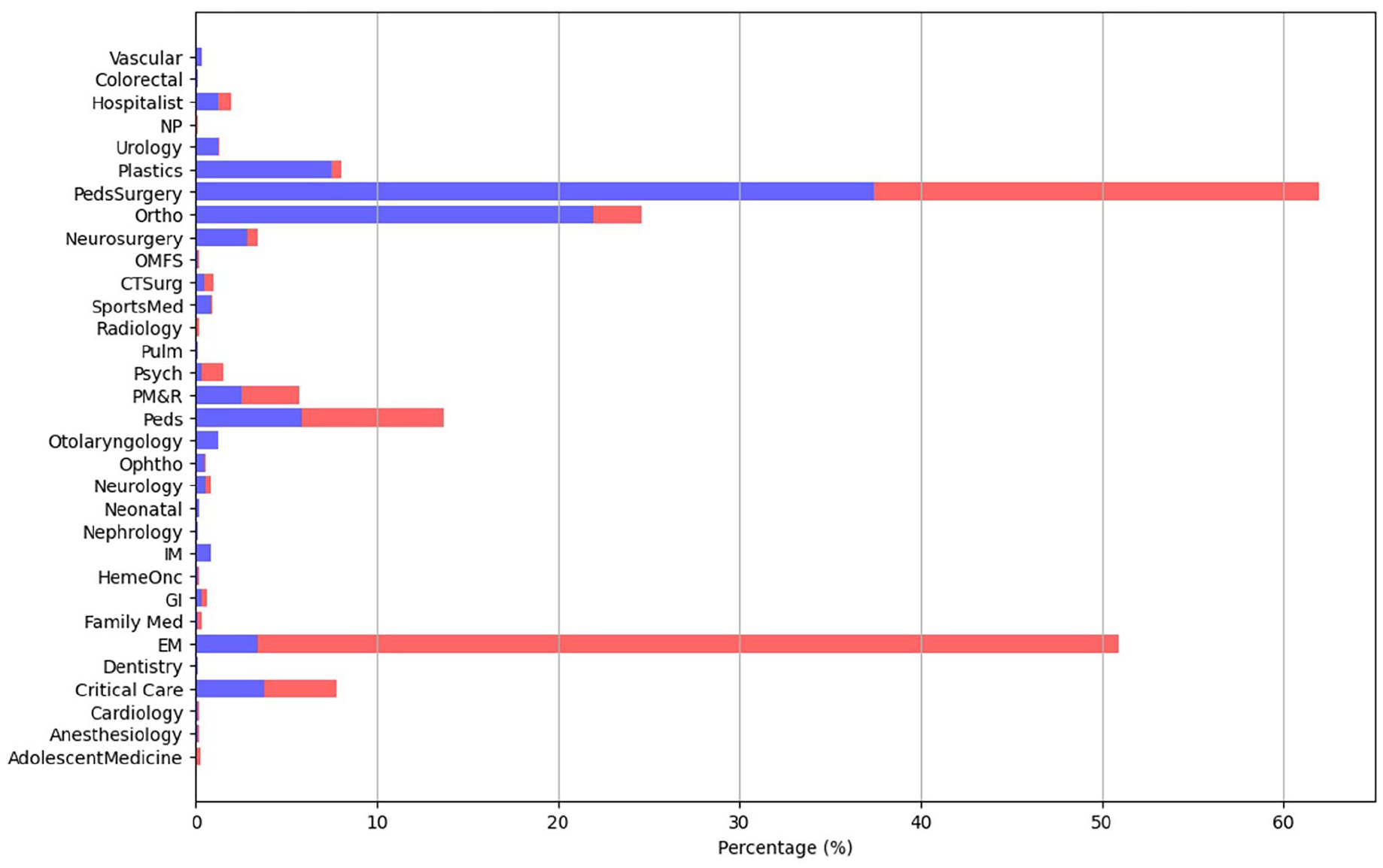
Chart illustrates the percentage of pediatric firearm injury cases managed by each specialty, stratified by OR involvement. The y-axis lists clinical specialties, and the x-axis denotes the percentage of total cases. Blue bars indicate operative management, while red bars indicate non-operative management. Among the surgical specialties shown, pediatric surgery, orthopedic, and plastic surgery were the most common involved.
Discussion
The findings of this study provide important insights into the national burden of pediatric firearm injuries and the factors influencing surgical intervention. Specifically, this study encompasses the impact of state-level gun laws and COI on the involvement of various surgical specialties in the management of these complex injuries. Children from neighborhoods with the lowest COI of 20%, 12 years or younger in age, or who lived further from a hospital were found to have significantly higher rates of mortality. These results support prior literature revealing that children residing in impoverished and resource limited areas are at higher risk of firearm-related injuries and death.2,13,14 This finding can inform community-based development efforts as well as broader interventions aimed at reducing firearm-related injuries. Further, our analysis highlights the relationship between population-adjusted incidents and Giffords Gun Law Scorecard ratings. States with permissive gun laws have lower gun control, higher rates of firearm injuries, more gun ownership, and are associated with greater counts of firearm injury and mass shooting.10,15 This trend aligns with the pediatric population and suggests that weaker gun policy contributes to worse clinical and psychological outcomes among affected children. 2
The complexity of pediatric firearm injuries and the potential reconstructive challenges they present is demonstrated through the finding that orthopedic and plastic surgery were frequently involved in inpatient management. The involvement of multiple surgical and nonsurgical specialties emphasizes the complexity of firearm injuries among children. The frequent involvement of pediatric orthopedic and plastic surgery, as well as other specialties suggests the necessity of a multidisciplinary approach during the inpatient period. This collaboration is essential for achieving optimal outcomes, especially in cases requiring staged procedures, such as skeletal stabilization followed by soft tissue reconstruction. This highlights the evolving and critical role of plastic surgeons in repairing traumatic injuries and restoring function in pediatric patients.
It has been well established that plastic and reconstructive surgeons play a role in the care of firearm-induced injuries, which remains a leading public health concern in the United States.16-19 The finding that pediatric, orthopedic, and plastic surgery are commonly involved surgical specialties suggests the complexity of these injuries, possible disparities in access to specialized care, and mirrors previous studies on specialized operative interventions required during hospitalizations.19,20 Although the dataset didn’t allow for detailed analysis on the specific reconstructive procedures performed, our findings reemphasize the literature on plastic surgery’s involvement in firearm injuries. Future research should explore whether long-term outcomes and patient costs differ between children treated at facilities with dedicated and specialized pediatric surgical teams versus general trauma centers. Firearm-related injuries present significant challenges due to their complexity and management requires a multidisciplinary team. Despite advancements in treatment, there are disparities in reconstruction for pediatric firearm injuries based on accessibility to medical centers, insurance status and U.S. geographical region. 20 Thus, plastic surgeons are uniquely positioned to contribute to prevention efforts by counseling patients on firearm safety and proper storage to potentially reduce these complex injuries. 16
This study is among the few national-scale analyses that examines both state-level and neighborhood-level associations with pediatric firearm injuries. To the best of our knowledge, this study is the first to apply COI for assessing trends in pediatric firearm injuries. Given the escalating burden of pediatric firearm injuries, the results presented further emphasizes that this injury pattern affects multiple surgical and clinical specialties. By revealing how state-level firearm laws and quality of neighborhood opportunities are associated with this injury type, this study offers valuable insights to inform healthcare providers, surgeons, and advocate for policy change.
Our study is subject to limitations, including the potential for coding errors in administrative data, difficulty extrapolating findings to communities not represented by the PHIS database. The relatively small sample is due to the minimal number of participating children’s hospitals in the PHIS database, thus generalizability is limited. Also, this study does not account for changes overtime in state gun laws and mandates. There are unmeasured variables that we did not control for, such as patients who may have crossed state lines to urban cities with pediatric trauma centers. Injuries treated in outpatient settings and levels of community violence are some confounders that should be addressed in future research to enhance the validity and generalizability of the findings. Importantly, however, findings presented in this study mirror the existing literature that demonstrate state gun laws and neighborhood disparities are associated with pediatric firearm injury and mortality. Our results contribute to the current literature by evaluating neighborhood-level factors in pediatric firearm injury outcomes. While an analysis of injury type and specific reconstructive procedures were not performed, this data offers a unique perspective on specialty involvement, and neighborhood and state-level details in gun violence within the pediatric patient population. These results may contribute to health policy development and support advocacy efforts to reduce this growing national problem.
Conclusion
This study highlights the significant burden of pediatric firearm injuries in the United States, emphasizing the associations between COI, state gun laws, and patient outcomes. Children from disadvantaged neighborhoods, younger age groups, and those living further from hospitals faced higher mortality rates, while permissive state gun laws were associated with increased injury incidence. The frequent involvement of surgical specialties, such as plastic surgery, emphasizes the complexity of firearm injuries and the necessity of a multidisciplinary approach for optimal care during the inpatient period. This study provides valuable insights to inform health policy, guide advocacy, and support ongoing efforts to address this public health crisis.
Supplemental Material
sj-docx-1-fac-10.1177_27325016251361334 – Supplemental material for The Intersection of State Gun Laws and Child Opportunity Index in Pediatric Firearm Incidents
Supplemental material, sj-docx-1-fac-10.1177_27325016251361334 for The Intersection of State Gun Laws and Child Opportunity Index in Pediatric Firearm Incidents by Lana Mamoun, Sierra Willens, Joseph Mocharnuk, Dana Meshkin and Miles J. Pfaff in FACE
Footnotes
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Considerations
Institutional Review Board approval was not required.
Consent to Participate
Not applicable.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data is available upon request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.