
Abstract
Introduction
Five billion people in the world lack access to needed surgical care, with only 6% of all procedures performed in the poorest countries—home to a third of the world’s population. 1 In the past 2 decades, global health advances have focused largely on treatment and prevention strategies of communicable diseases, such as HIV/AIDS and tuberculosis. 1 However, data show that an estimated 32% of deaths worldwide are attributable to conditions requiring surgical care, greater than the combination of deaths from HIV/AIDS, tuberculosis, and malaria combined. 1 Until recently, though, it was believed that expansion of surgical efforts into low and middle income countries (LMIC) was expensive and resource-intensive, therefore implausible and unsustainable. 2 In 2014, the Lancet Commission on Global Surgery was launched to help understand and ameliorate this concern. This multidisciplinary panel of leaders found that investing in surgical care in LMIC not only reduces mortality and morbidity, but is also cost effective, considering the cost burden of diseases requiring surgical care. 1 Additionally, upfront investment to establish more robust surgical care may promote economic growth through increased job opportunities.
One such opportunity for improvement in global surgery is orofacial clefting, commonly known as cleft lip and palate. Cleft lip/palate is the most common congenital craniofacial anomaly, and lack of repair and appropriate postoperative care can have devastating consequences. 3 Without care, cleft lip/palate malformations can impact many areas of a child’s health and development, including speech, mastication, breathing, and overall ability for societal integration. Further, children with these malformations are more likely to be subject to social stigma and decreased self-esteem, an increasingly recognized phenomenon. 4 As cleft lip/palate care continues to drastically improve in developed countries, so, too, has patients’ quality-of-life following this care, with some patients rating their quality-of-life significantly higher than before. 5 Despite these successes, access to this necessary multi-year care is not always attainable. One of the major limitations is the financial burden of cleft/lip palate repair, which requires multi-subspecialty collaboration efforts. With no concrete current estimates of cleft care, we can only base our assumptions of current lifetime costs from a presumable increase of a previously estimated $101 000 per each new case recorded from a 1988 cohort study. 6
Despite the existence of validated multidisciplinary cleft care in the first world, the adoption of sustainable and effective team-based care in low resource countries continues to prove difficult. A robust body of literature demonstrates the importance of a multi-specialty collaborative approach in cleft lip/palate repair to ensure that children with these congenital abnormalities can become functioning members of society. Contrary to prior decades, in which fragmented care was provided by private plastic surgeons and orthodontists, the current standard-of-care in the United States and other first-world countries consists of a coordinated, integrated, and multidisciplinary team approach. 7 According to the American Cleft Palate-Craniofacial Association, cleft teams may be composed of plastic surgeons, often with additional craniofacial training, orthodontists, otolaryngologists, social workers, psychiatrists, and speech-language pathologists, among others, as seen fit for each case. 8 However, the prohibitive effects of cost, specialty trained surgeons, and appropriately staffed and stocked facilities are only some of the difficulties of adopting this same approach in the developing world.
During the late 1980s, the need for cleft care in the developing world was increasingly recognized, leading to the creation of multiple non-governmental organizations dedicated to addressing this demand. 9 At the inception of Operation Smile, Hands Across the World, and other similar organizations, the longitudinal and collaborative model of team based care for cleft lip/palate was neither fully developed nor adopted in the United States, and was therefore not a model that was followed by these organizations. Instead, they led medical mission trips which adhered largely to what is now referred to as a vertical model of care. 10 The vertical, or disease-specific, model of care focuses on specific operations performed by providers who take limited trips to the host country. Coincident with this model, organizations like Operation Smile relied on short-term trips to developing countries, during which initial repair of cleft deformities were performed by surgeons often without fellowship training in cleft surgery. While we now realize this model does not lead to long term care system development within LMICs, these efforts, which highlighted the importance of cleft lip/palate care in LMIC, were beneficial, nonetheless. For example, out of the 1142 reconstructive cleft lip/palate efforts in Ecuador by Hands Across the World from 1996 to 2011, it has translated to a $4.7 million economic benefit when calculated from a human capital approach, where researchers contextualized an individual’s disease in relation to their potential economic contribution to society. 2
In the late 1990s, with the founding of Smile Train, a different approach to global cleft care was emphasized in their initiative under the horizontal model. Within this model, rather than sending a team of foreign surgeons to provide care, a sustainable system is created through mentorship and training that empowers local physicians. Teaching takes place through virtual simulations, access to medical resource libraries, and conferences so that local physicians can become equipped with the most up-to-date knowledge and techniques to provide cleft care within their own communities. 11
Under each of these models, these organizations have been able to provide care that otherwise would have not been accessible. However, they are not without their limitations. The vertical model of care may benefit individual patients in the short term, but fails to: (1) address the full scope of the disease process, and (2) incentivize host country autonomy, perpetuating the paucity of specialty-trained personnel and an inability to maintain appropriate surgical care following the departure of the medical mission. 12 The horizontal model, on the other hand, has been less attractive to missions historically due to the time needed to effectively implement, greater funding required, and dependency on a functional government. 12 To help address these issues, an oblique, or diagonal approach to medical care in LMIC has been implemented in some sectors of global health work. This model integrates both vertical and horizontal approaches to global care in a way that enriches the LMIC to build sustainable, local health delivery services. Vertical inputs have enabled notable successes among global infectious disease initiatives, such as HIV treatment and vaccination implementation, where necessary supplies, medications, and equipment can be efficiently delivered for urgent humanitarian responses. 10 The horizontal model emphasizes long-term healthcare investments through expansion of local infrastructure and primary care systems. Combining these 2 approaches through the diagonal model hopes to achieve synergy between the immediate advantages of the vertical model with the long term aims of the horizontal model. 12
The emergence of the oblique model of care in LMIC and the improved understanding of the vertical and horizontal models’ shortcomings has provided an opportunity to describe the development of a sustainable and longitudinal approach to cleft lip/palate repair. The goal of this paper, therefore, is to reflect on the implementation of the oblique model of cleft care in El Salvador, creating a potential model for expansion of effective cleft care in the developing world.
The Cleft Care Continuum in the United States
The care of a child with a cleft lip/palate starts before and extends far beyond the initial lip or palate repair performed by the plastic surgeon. The timing and order of each intervention is paramount to the child’s health and development. 3 In addition to esthetic considerations, which have profound psychosocial implications, infants and children with cleft lip/palate are at a significantly increased risk for delays in cognition, comprehension, and expressive language abilities. 13 To help reduce these risks, the American Cleft Palate-Craniofacial Association (ACPA) has detailed a Standard of Care to coordinate care between different healthcare disciplines (Figure 1).
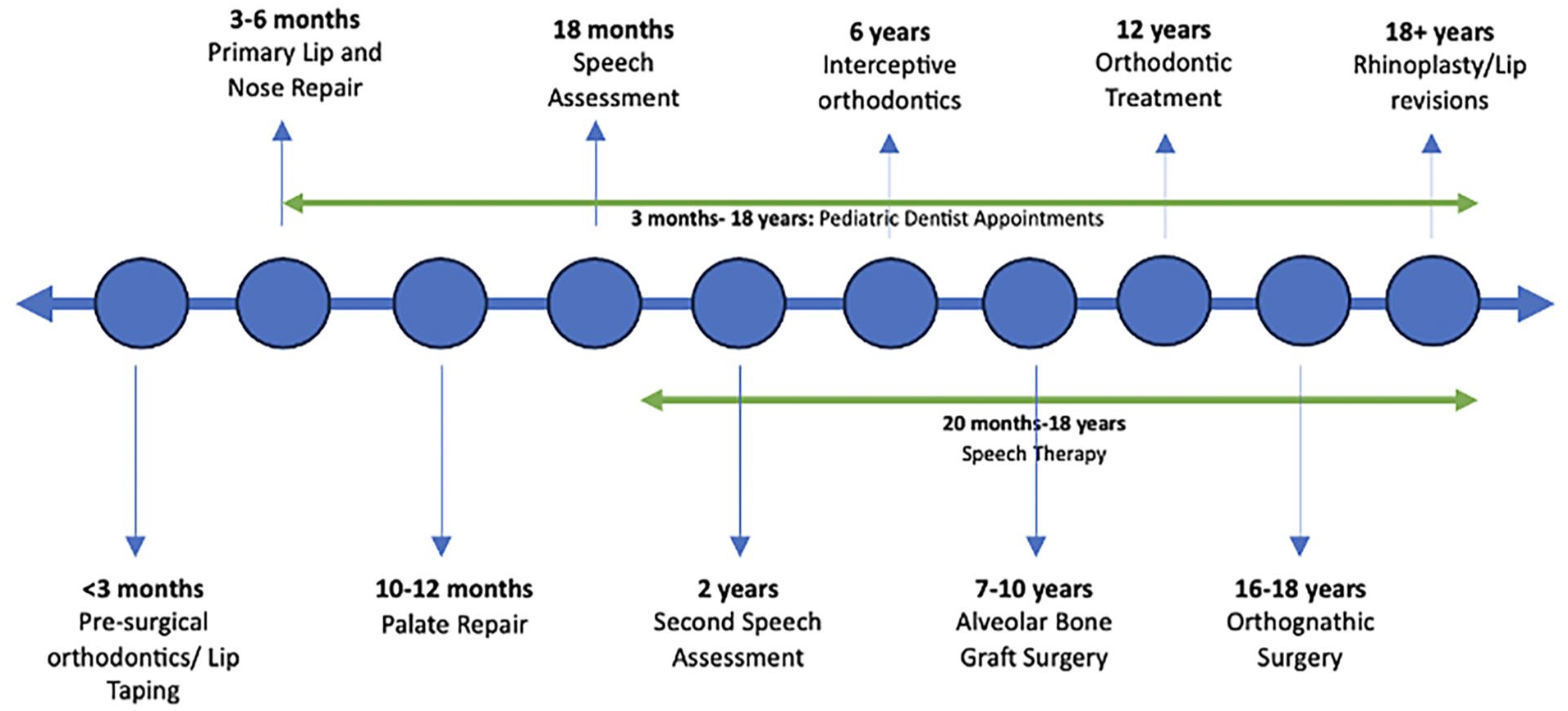
Timeline of cleft care over child and adolescent years. 30
Intervention is often started within the first few weeks of life and includes presurgical infant orthodontic treatment (PSIOT) performed by an orthodontist or specialty trained pediatric dentist. 3 Following this, a fellowship trained cleft surgeon performs the primary cleft lip or palate repair, typically in infancy. Speech assessment occurs next, followed by years of speech therapy visits, and potential velopharyngeal surgery, followed by initiation of phase I orthodontic treatment. 3 Multiple other surgeries, including alveolar bone grafting, revision surgeries to the nose and lip, also occur, often culminating in corrective jaw surgery and septorhinoplasty. This continuum of care takes the patient from infancy through their mid to late teen years (skeletal maturity). Concurrent with these interventions, patients often have additional consults with psychiatry, social work, speech pathologist, genetic counselors, and otolaryngology. 8
Multidisciplinary team care for cleft lip/palate has become the standard within the United States, with even more local hospital systems integrating it into their plan of care for patients. Even in rural communities, the introduction of Telehealth during the pandemic provides an avenue where differing specialists can interact and collaborate with patients during every step of their care. But the differing alignments on healthcare rules, policies, and support systems in LMIC result in a dearth of well-established multidisciplinary teams, often leading to missed opportunities, lower patient outcomes, and increased healthcare costs.
Optimizing the Cleft Care Continuum in the US and Beyond
When discussing improvement of cleft care outcomes, it has been found that optimal results come from a unified treatment protocol agreed upon by a multidisciplinary team combined with high quality surgical care. This was demonstrated through the Americleft Study, a large retrospective cohort study that assessed craniofacial morphological relationships using conventional cephalometric analysis across multiple centers to evaluate treatment protocols and evidence-based practice decisions. Agreement between experienced and specialized physicians on simpler, less burdensome protocols achieved more favorable outcomes. 14 Ultimately, the combination of high-level surgical care alongside a coordinated team protocol were deemed the 2 most important determinants of good cleft outcomes and are pillars of what we are trying to uphold in our model in El Salvador.
In the United States, outcomes in cleft care have improved due to sub specialization and multi-disciplinary care. Orofacial cleft surgery is now routinely performed by craniofacial surgeons or other subspecialized surgeons. Fellowship training in cleft surgery allows for achievement of high-level surgical care necessary for surgical outcomes of the cleft care continuum. 15 While there are many fellowships in the United States and abroad in the first world, opportunities in the third world and developing world are limited. This kind of training is vital when seeking to administer appropriate care in a LMIC given that cases tend to be more complex in these areas, compounded by the additional challenges of nutritional deficiencies and socioeconomic hardships. Across specialties, studies show that surgical outcomes tend to be more favorable when performed by specialists within their respective fields.16-18 For example, a 2014 comparative study found that complication rates for complex pediatric appendicitis cases were more prevalent with general surgeons, as compared to specialized pediatric surgeons. 19
Despite the push toward fellowship training in many developed countries, this same shift has been less prevalent in a LMIC. Instead, surgical training in a LMIC remains focused broadly on general surgery, plastic surgery, and oral maxillofacial surgery. 20 This same structure is commonly mirrored inside hospitals, with general surgeons performing cases that would, in developed countries, be staffed by specialists like plastic surgeons, otolaryngologists, vascular surgeons, or urologists. 20 This reality is likely multifaceted, including issues of infrastructure, staffing, cost, and training. Paramount to the advancement of surgical subspecialties is resource availability, both in terms of increasingly advanced technology, such as virtual surgical planning and specialized endoscopic instruments, and in skilled mentors, who can guide the next generation of subspecialists. 21 As outlined by The Lancet Commission on Global Surgery, infrastructure and surgical workforce are 2 major pillars of effective expansion of surgical efforts in a LMIC. However, as evidenced by the estimated 11% of deaths secondary to surgically treatable conditions, it remains that neither the infrastructure nor the number of surgeons are adequate to prevent deaths, let alone perform specialized elective surgeries. 22 Because of this, the opportunity for subspecialized training in LMIC are relatively small.
Efforts have been made, however, to form partnerships between institutions in developed countries and those in a LMIC, enabling surgical graduates to participate in fellowship-style training. The fellowship-style training partnerships, termed “observerships,” consist of 1 to 2 year apprenticeships for international medical graduates (IMG), in which a surgeon from a LMIC trains at a single partner institution in a developed country. 21 In the recent years, there has been a handful of isolated international slots at established craniofacial surgery fellowships where hands on practice opportunities are available to IMGs. However, these opportunities remain severely limited as the large majority of observerships stress learning through mostly didactic lectures and surveillance of healthcare delivery. There is a greater push from the United Kingdom and Canada to integrate a more hands-on approach to medical education in their IMG trainees, but there are still restrictions to such training.
Despite the increasing opportunities available for surgeons from a LMIC to train in the first world and the invaluable exposure to multidisciplinary care, there may still be limitations upon returning to their home country. Persistent challenges surrounding financial support, sufficient technology, infrastructure, and partnerships could constrain their ability to achieve the level of success they know they can attain in cleft care. 21 Perhaps in addition to first world training, optimal training of an enthusiastic surgeon working in a developing country also arises from the learning and mentoring that takes place in their respective environment. This would necessitate that specialized surgeons travel and collaborate on cases within their country, thereby continuing to enhance their expertise and to tailor their knowledge of first world care and advanced healthcare practices to the context of the developing world, so that optimal outcomes can result without undue complication. This approach would provide valuable insight to both what is possible and what can be achieved within their own country despite limitations, utilizing their resources, healthcare systems, and infrastructure.
Experience in El Salvador
For over 10 years, the senior author, a craniofacial trained plastic surgeon, has taken humanitarian-based surgical trips to El Salvador, which form both the backbone and impetus for this paper. His accumulated experience and knowledge are the sum of over a decade of experience working with both a cleft organization (Austin Smiles Plastic Surgery Foundation) and individual mission trips to Bloom Children’s Hospital in San Salvador. In 2010, he took his first trip with Austin Smiles, an Austin, TX based nonprofit organization providing cleft lip/palate operations in developing countries. Since its inception in 1987, Austin Smiles has participated in over 100 medical trips, providing care for over 5000 patients in Brazil, Cuba, the Dominican Republic, Ecuador, El Salvador, Guatemala, Mexico, Micronesia, Nicaragua, and the Philippines. 23
When medical trips began in the 1980s, the multidisciplinary, longitudinal model of cleft lip/palate care had yet to be fully established in the United States and was therefore not implemented on the organization’s trips. Additionally, none of the plastic surgeons were specifically fellowship trained in cleft and craniofacial surgery, which limited care scope and understanding. Instead, initial missions aligned with the traditional vertical model that was more widely accepted at the time. As our senior author continued his annual trips to El Salvador with Austin Smiles, they saw the opportunity to implement the same multidisciplinary care continuum which had been adopted in the United States and push for cleft lip/palate surgeries to be performed by fellowship-trained craniofacial surgeons. The idea was to bring the first world to the developing world.
El Salvador, a Central American country of over 6 million inhabitants, has a long history of socio-political unrest, culminating in a 12 year civil war from 1980 to 1992.24,25 The continued repercussions of this backdrop have stagnated economic growth, with poverty rates remaining around 26%. 26 This is reflected in healthcare infrastructure, and at the time of our senior author’s initial trips with Austin Smiles, there was only 1 children’s hospital for the entire country. While cleft lip/palate care was being provided at this hospital, the number of patients needing care vastly overwhelmed the few plastic surgeons attempting this care. Additionally, there was no interdisciplinary cleft team, so other necessary services, such as orthodontic care, speech therapy, and oral therapy, were lacking. Further, the lack of longitudinal care meant that patients often failed to receive operations beyond the initial repair. Observing this reality in El Salvador, while participating in the successful multidisciplinary cleft care continuum paradigm shift in the United States, provided a unique vantage point for re-thinking cleft care in LMICs.
Providing medical care in a LMIC is a delicate and potentially contentious pursuit. With participation in international short-term missions significantly increasing in recent decades, an overview of criticisms directed toward these missions has emerged in recent studies under a template of the “seven sins of humanitarian medicine.” 27 A common theme underlying these criticisms involves a lack of consultation with the local population and their healthcare providers on what exactly their needs are. One failure can be highlighted through an example of an inability to match technology to local needs and abilities. A Belgian plastic surgeon who volunteered in Laos, noted American universities attempting to teach endoscopy skills to local providers who had no access to an endoscope. He commented how these efforts were viewed as an attempt to be the “first” to introduce this procedure, rather than an effort toward sustainable care. While these missions are all well-intentioned, more attention needs to be paid to how efforts could be perceived by the local community, the safety of the procedures performed, and what kinds of preparations need to be made in case complications arise. 27
Developing a beneficial and sustainable infrastructure to provide patient care relies heavily on reciprocal trust and the formation of partnerships between the host country and the foreign physicians. Culturally insensitive medical mission trips may do more harm than good, owing to disruptions in local practices and attitudes of superiority. With this understanding, the formation of partnerships in El Salvador were the result of observing the landscape and performing a socially conscious site survey. During our senior author’s many trips with Austin Smiles, careful consideration and discussion with local practitioners occurred. Alongside the explanations of what the visiting physicians can contribute, an imperative question was asked during this time: “How can I help?” In the beginning, cleft lip/palate care was performed out of a military facility with patients referred by local physicians. Once Austin Smiles started caring for these patients, the initial referring physicians began to work alongside Austin Smiles and share experiences. This is how relationships began to form in El Salvador and eventually Austin Smiles established relationships with local hospitals, surgeons, the government, the Rotary, dental school, and orthodontists in the area. The local dental school’s lab has been able to be used for preoperative evaluations and tasks. Once Zoom became more accessible as well, virtual visits were and continue to be held between local US and Salvadoran orthodontists to train them on craniofacial orthodontics, which requires additional teaching to adequately treat.
Accountability is a joint responsibility upheld by both mission and local healthcare providers in assessing the long-term outcome of surgeries performed and promoting sustainability. The specific needs of practitioners and patients in LMIC depend on factors like location, available supplies, and local practitioner availability/expertise. Only after assessing these factors was the role of the visiting physician established (ie, a teaching role, a physician liaison role, etc.) in El Salvador. As missions continue in El Salvador, there is a greater push toward expanding apprenticeships, which involve a surgeon from LMIC receiving surgical training from an institution in a developed country. Developing this partnership is a crucial next step in their goal of building a sustainable healthcare infrastructure as the best way to teach the future generation of surgeons is a combination of training within their home country and training within a first world environment.
Alongside training the future generation, subspecialty training is also being implemented into the infrastructure as it has been in the United States. During initial mission trips to El Salvador, there were children in orthodontics (cared for by local orthodontists). An attempt was being made by local providers to extend the reach further into the cleft care continuum. Orthodontic treatment of patients with cleft lip/palate requires an extensive interdisciplinary approach to optimize functional and esthetic outcomes. These patients often present with dental crossbites, dental anomalies, malocclusion, scarring, feeding, and speech difficulties. Treatment modalities vary according to developmental stage, cleft severity, and jaw discrepancy. While early surgical treatment focuses on fixing the skeletal deformities, orthodontic treatment aims to improve midfacial growth and current dental crossbites while securing the eruption of teeth. This involves techniques like nasoalveolar molding to reapproximate the maxillary alveolar segments to reduce tension on the repaired lips and improve symmetry and maxillary development. 28 Orthognathic surgeries that follow orthodontic treatment have also been incorporated into cleft care into El Salvador. Procedures like bone grafts, mandibular and midface distractions, Le Fort I osteotomies, and bilateral sagittal split osteotomies are all currently being performed at the Children’s hospital in El Salvador. More specifically, since 2015, a total of 17 Le Fort I procedures, 15 bone grafts, 6 mandible distractions and 4 BSSOs have been performed. Ultimately, by incorporating orthodontic/orthognathic care alongside other subspecialties like speech and language therapy, rhinoplasties, and lip revisions, this multidisciplinary care model can mold productive members of society.
Based on our Oblique approach in El Salvador, we have been able to implement a sustainable system founded on the principles of reciprocal trust and partnership. We have built a group of local surgeons interested in multidisciplinary care, where orthodontic and orthognathic treatment have now been successfully incorporated into the cleft care continuum. By establishing the role of visiting physicians as teachers sensitive to their needs, local physicians have been trained within their home country utilizing their own resources, while also gaining exposure to the multidisciplinary care provided in a first world environment. Training on craniofacial orthodontics has been and continues to be provided virtually. The chief of plastic surgery at the children’s hospital in El Salvador was able to visit our center to learn about multidisciplinary care and complex surgery. Fellowship-style training has also been emphasized, as 1 of the local pediatric plastic surgeons successfully completed a craniofacial fellowship at the University of Alabama, becoming the first surgeon from El Salvador to do so.
Future Discussions
Ongoing discussions remain regarding what exactly a sustainable fully functioning healthcare foundation looks like in a LMIC and what is the best way to approach building one. Based on experiences in El Salvador and other LMICs we feel that a foundation, not directly reliant on the national government for resources, would provide a sustainable model for continued development of multidisciplinary, team based craniofacial care. A foundation of such kind would be led by members of the host nation and a first world team/organization. Care would be prorated based on ability to pay. Inspiration can be taken from an ophthalmology foundation named FUDEM founded in El Salvador in 1989. This visual health program was born to provide a better life for low-income women and their families, where early motherhood and multiple births created high incidences of vision deficiencies and blindness. They initially held multiple campaigns to assess needs, collected donated lenses to build an inventory, and established mobile clinics by making agreements with the local mayors, schools, churches, social workers, and non-governmental organizations (NGOs) to identify and treat the populations with deficiencies. Once demand grew, they used local laboratories to produce glasses, and eventually opened their first FUDEM clinic in San Salvador in 2003, a permanent location for optometry, ophthalmology, and eye surgery, with their own clinical laboratory. Over time, they expanded to 256 of the 262 municipalities and entered private company markets and state institutions, setting up clinics for employees. With donations from the US, Germany, and local organizations, FUDEM has achieved the ability to run as a financially stable, fully functioning healthcare center, independent of the government, with a multidisciplinary team that incorporates subspecialty training. 29 Their approach to their success is something to make note of when considering how we can build sustainable programs for craniofacial care (Figure 2). The hope in establishing these programs is to one day reach the point where we as visitors can render ourselves useless in their healthcare infrastructure. A good first step, therefore, is to lay the foundation of a trusting relationship between local and visiting providers through understanding the local system and their needs.
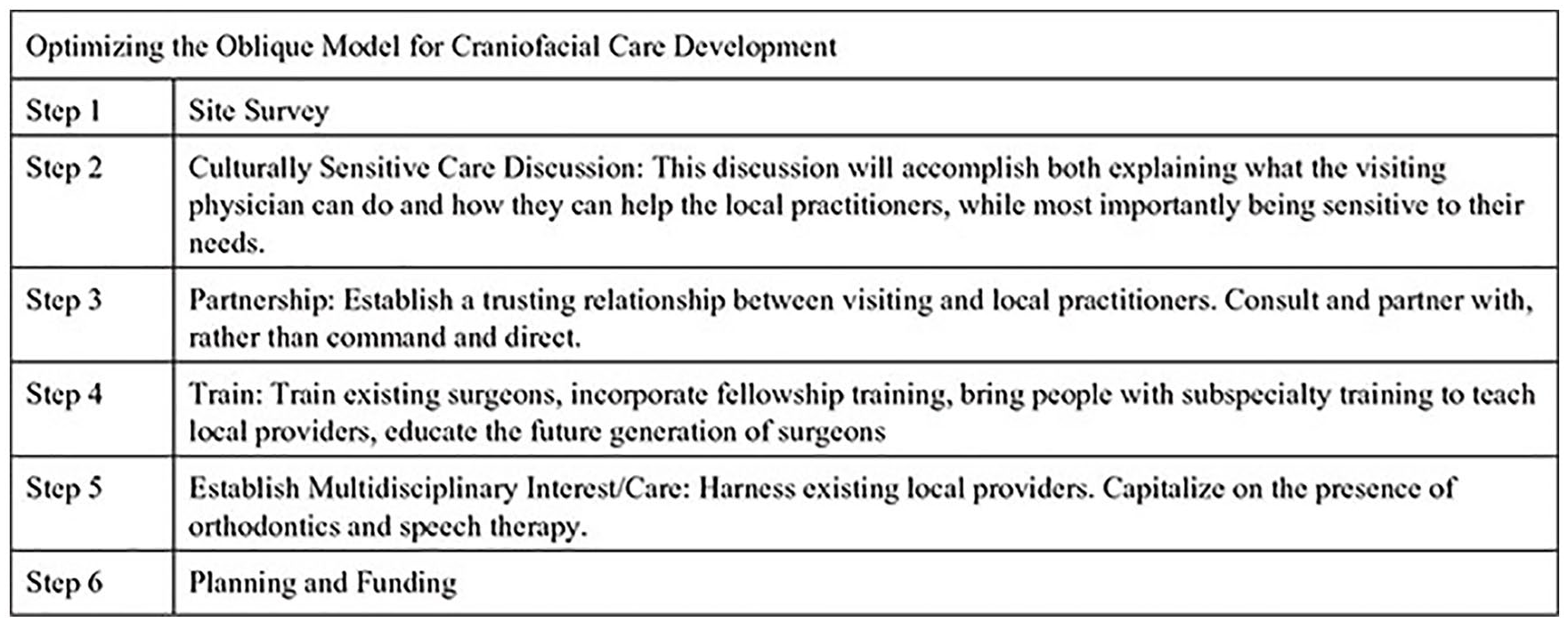
Optimizing the oblique model for craniofacial development.
Conclusion
The evolution of global surgical care in LMICs has undergone significant changes in recent decades. The vertical model, present since the early stages of global surgery and beneficial at its time, also led to growth of practices that often resulted in sub-optimal patient care. Moreover, it increased the demand for health infrastructure in LMICs by expanding specialized follow-up care that was inaccessible. Patients who received care from the vertical model of care often had to fend for themselves in finding their own medical care. The horizontal model obviates some vertical concerns by integrating IMGs into highly specialized surgical care and fostering partnerships between institutions for optimal international patient care. This model is often constrained by limited residency spots and licensing/surgical issues for IMGs. Herein, we describe our experience in constructing an oblique model of care in El Salvador to address deficiencies observed in both the vertical and horizontal models of care, aiming to enhance cleft care effectiveness in LMICs.
Footnotes
Acknowledgements
We would like to express our sincere gratitude to the following organizations for their support and invaluable collaboration. The completion of this article could not have been possible without the work of Austin Smiles Plastic Surgery Foundation and Rotary International.
Data Availability Statement
Not applicable
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Institutional Review Board approval was not required.
Consent to Participate
Not applicable
Consent for Publication
Not applicable
Informed Consent
Not applicable.