
Abstract
Background:
Cleft lip scar formation is an inevitable consequence of cleft lip repair (CLR) and is exacerbated by the dynamic movement of the middle face. Various methods to correct or prevent these deformities have been described including silicone sheeting, surgical revisions, laser therapy, and more recently, Botulinum toxin-A (Botox) and Dermabond. This study aims to analyze and compare the impact of Botox versus Dermabond on scar appearance after CLR.
Methods:
Following PRISMA guidelines, a systematic review was performed on Medline, Embase, Cochrane, and CINAHL using the following keywords: “Dermabond,” “botulinum toxin,” and “cleft lip.” Outcomes of interest were the rates of scar hypertrophy, scar width, Vancouver scar scale (VSS), visual analog scale (VAS), Hollander wound evaluation scale (HWES), and complications.
Results:
Nine studies were included of which 4 articles analyzed Botox and 5 analyzed Dermabond. Forest plots for scar width at the first and second time point supported the use of Botox to achieve a smaller scar width with P < .0001 (95% CI: −1.09 [−1.56 to −0.63] and 95% CI: −0.94 [−1.37 to −0.50], respectively). A significant increase in VAS was observed with Botox (95% CI: 1.66 [1.27-2.05], P value < .0001) and VSS was insignificant. Of the articles that analyzed Dermabond, scar appearance was comparable to the traditional suture closure group. There were no feeding complications for either intervention. Pooled forest plots for VAS comparing Botox and Dermabond supported the use of Botox with improved VAS (95% CI: 1.66 [1.27-2.05], P < .0001) compared to Dermabond (95% CI: 0.07 [ −0.48 to 0.61], P = .80).
Conclusions:
The current literature supports the use of Botox for scar improvement following CLR or revision. However, there is limited data to support Dermabond’s utility in improving scars in CLR, which highlights the need for further studies.
Introduction
Cleft lip scar formation is an inevitable consequence of cleft lip repair (CLR) and is often exacerbated by any dynamic movement of the middle face. A feared sequela of CLR is hypertrophic scarring (HS), which can lead to physical defects such as disruption of cupid’s bow or asymmetry of philtral heights, and it may also contribute to poor self-esteem and negative self-image. 1
The pathophysiology of HS following cleft lip repair has been well described previously and is thought to be the result of excess tension at the wound edges. Repetitive microtrauma prolongs the inflammatory response, which causes excess collagen and proteoglycan deposition leading to impaired extracellular matrix remodeling. 2 A variety of scar features are associated with HS including color mismatch, increased thickness, firmness, widening, and contracture without extension beyond the original incision site. 3 HS typically occurs between 3 and 6 months following surgical intervention and the incidence varies between ethnicities.4,5
Current practice lacks a standard, widely adopted technique to address HS in CLR with the available methods showing variable effectiveness. The 2 main approaches directed against HS are either active prevention or secondary intervention. As its name suggests, active prevention encompasses methods that inhibit the formation of HS and includes presurgical molding, silicone gel or tapes, and tissue adhesive. Secondary intervention targets the scar after its formation and includes intralesional steroid injections, cryotherapy, and laser therapy, CO2 laser, pulsed light therapy, fat grafting, and percutaneous scar release. 6 These interventions have also been attempted in combination with studies reporting mild improvement.7,8 However, interventions with pre-surgical molding or silicone sheets have a number of drawbacks as it requires continuous follow-up and poses a risk of ingestion of materials and aspiration. 9
Dermabond or octyl-2-cyanoacrylate is a tissue adhesive (TA) compound that has been used for various wound closures for 2 decades. 10 Since its development, Dermabond has been compared to sutures in CLR with no difference in cosmetic outcome.11 -13 Octyl-2-cyanoacrylate is composed of long alkyl chains that are hydrophobic and take years to degrade. The films are strongly adherent to skin, bacteriostatic, flexible, provide continuous coverage of the wound site, and have occlusive dressing properties. 15 The existing studies to date compare cosmesis between sutures and Dermabond for closure; however, no techniques have attempted a strict immobilization of the lip using Dermabond, despite its potential ability to do so given its strong adherence to the skin.
Recently, Botulinum toxin-A (BTA) has been explored as an alternative technique to improve HS in CLR. BTA causes transient muscle paralysis through cleavage of presynaptic SNARE proteins at the neuromuscular junction, resulting in the inhibition of acetylcholine release into the synaptic cleft. 14 This transient paralysis minimizes any facial movement that could lead to increased tension on the wound edges and thus exacerbate scarring. BTA has been used in the treatment of many medical conditions including rhytids, migraines, hemifacial spasms, and wound healing, with its use now increasingly reported in CLR14,16 -22
While previous systematic reviews have separately examined Botox and Dermabond’s impact on scar appearance given their potential to minimize tension on the closure, there has yet to be a review comparing these 2 techniques. This current investigation sought to systematically review the literature and provide a meta-analysis of the current data on the effectiveness of Botox versus Dermabond in the appearance of the lip following primary or revision cleft lip repair.
Methods
A systematic review of the literature was performed per the Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) guidelines in the following electronic databases: Medline, Embase, Cochrane, and CINAHL (Figure 1). The search strategy was conducted in September of 2022 using the search terms shown in Appendix 1.
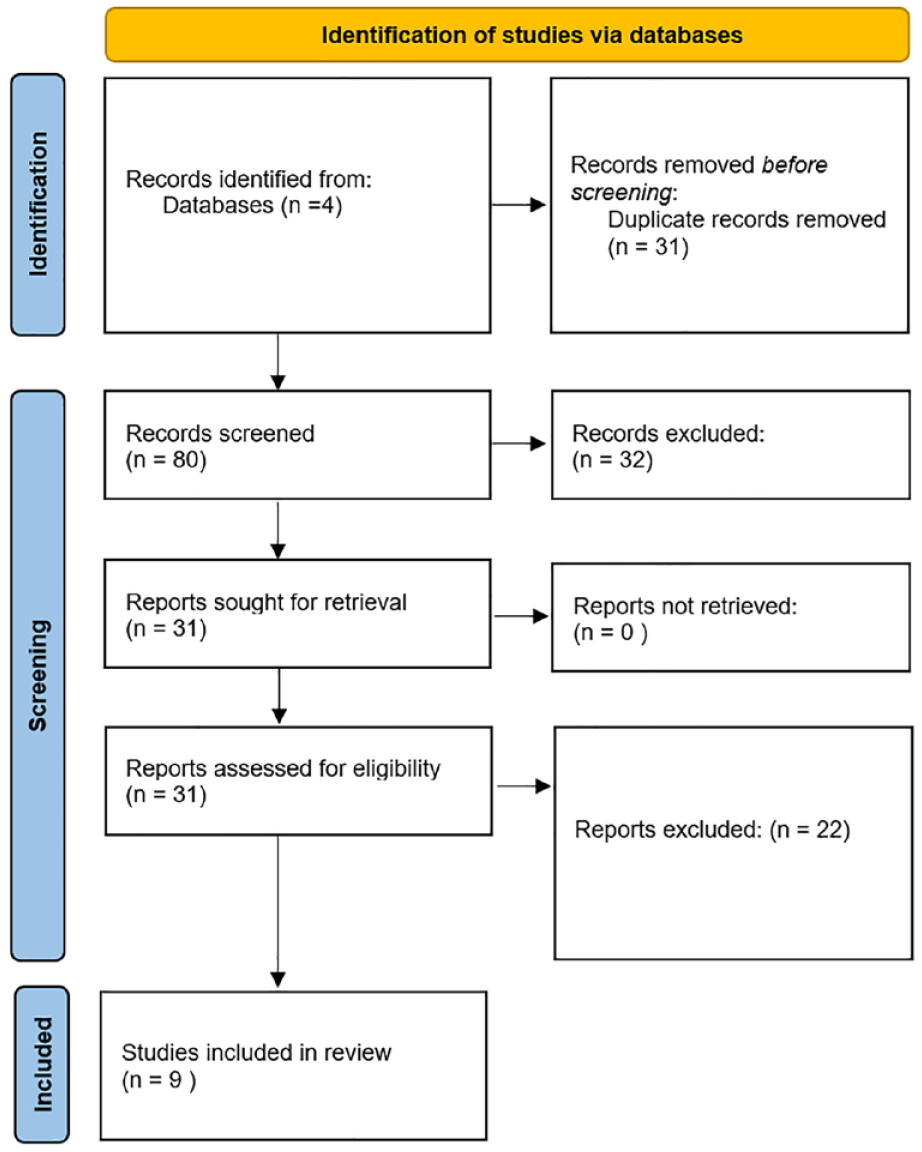
PRISMA diagram.
Study Criteria and Selection
Original articles, either cohort studies or randomized controlled trials, in English and Spanish were selected that reported outcomes of CLR using BTA or Dermabond. Literature reviews, systematic reviews, meta-analyses, opinion articles, letters, and book chapters were excluded. Two independent investigators (T.W and P.M) performed the screening. Articles were first selected based on the abstract and titles relevant to the use of BTA and CLR. Each reviewer then performed a full-text evaluation of the remaining articles using inclusion and exclusion criteria. Conflicts were identified and resolved by the 2 authors. Qualified studies were cross-referenced until the search strategy was exhausted.
Review Software
The review and selection of articles were processed on Covidence systematic review software, Veritas Health Innovation, Melbourne, Australia, which is available at www.covidence.org.
Data Extraction
The following data was extracted by 2 of the authors (T.W and P.M) from the included studies: authors, journal of publication, year of publication, study type, intervention type, primary outcomes, number of intervention and control patients, patient diagnosis, primary or revision surgery, surgical technique, gender and mean age of patients and timing and dosage of BTA injection. The outcomes of interest were the rates of scar hypertrophy, scar width at the first time point (FP) and second time point (SP), Vancouver scar scale (VSS), visual analog scale (VAS), Hollander wound evaluation scale (HWES), and complications. The methodological index for non-randomized studies (MINORS) was used to determine the study quality. The ideal score is 24 for comparative studies so scores of 0 to 8 were defined as low quality, 9 to 16 as moderate quality, and 17 to 24 as high quality. All of the studies were deemed to be of moderate quality.
Statistical Analysis
The data for the primary outcomes of interest were summed into forest plots so that the standard mean differences could be assessed using the Review Manager 5.4 software. Study heterogeneity was defined using I2 with P < .10 indicating significant heterogeneity.
Results
Literature Search
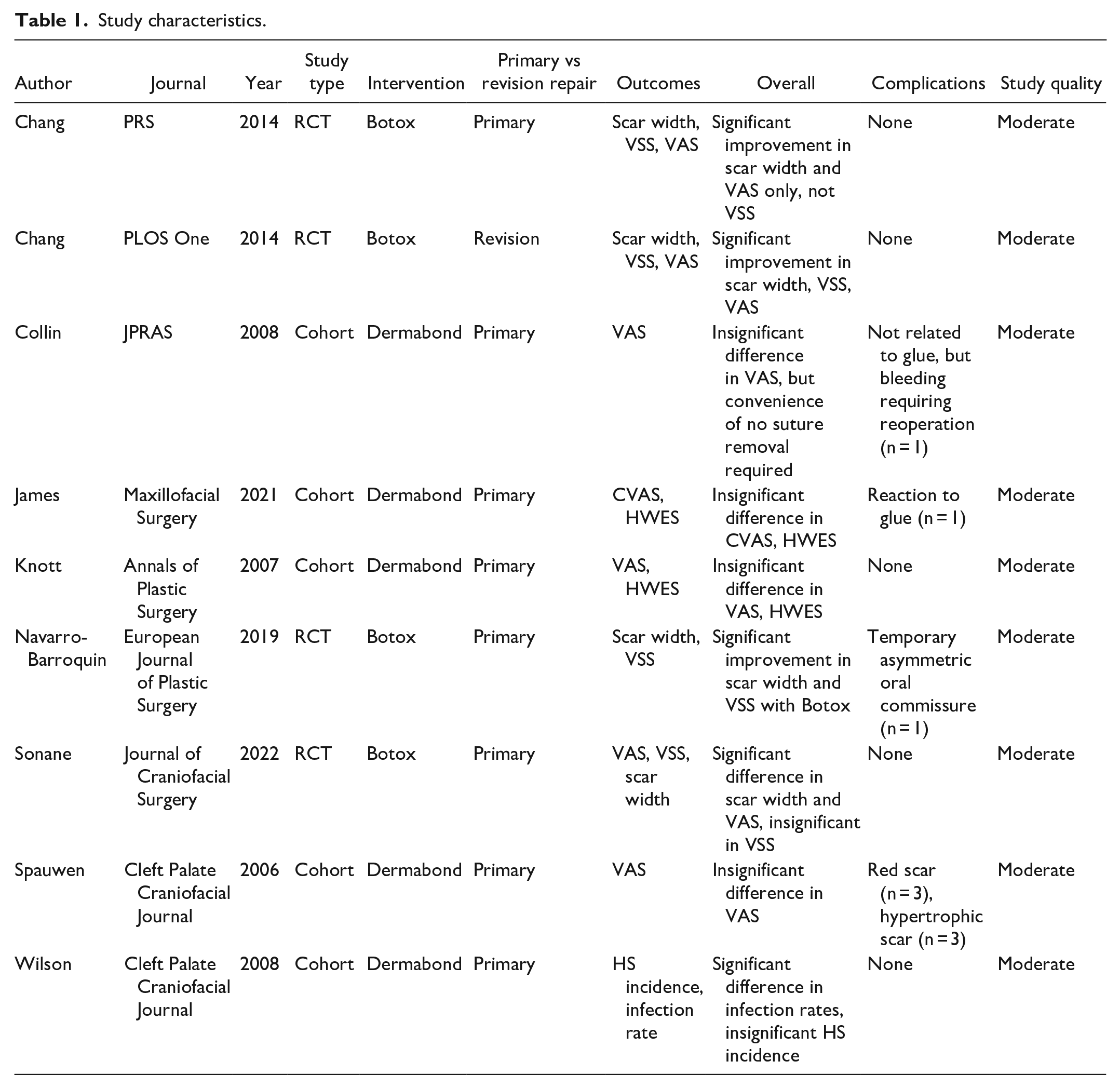
Eighty articles were screened and 9 were ultimately selected for analysis, all of which were in English. Eight articles focused on primary repair of cleft lip, while 1 focused on cleft lip revision. Four of the selected articles analyzed the chosen outcomes of interest, namely the rates of scar hypertrophy, scar width at the first time point (FP) and second time point (SP), Vancouver scar scale (VSS), visual analog scale (VAS), Hollander wound evaluation scale (HWES), and complications, after the use of Botox and 5 analyzed those outcomes of interest following the use of Dermabond. Study characteristics are listed in Table 1.
Study characteristics.
Outcomes
Forest plots demonstrated a significant increase in VAS with BTA (Figure 2) (95% CI: 1.66 [1.27-2.05], P value < .0001) and were insignificant for VSS (95% CI: −.53 [−1.21 to 0.15], P = .12). The outcome of VAS did not have significant heterogeneity (P = .45, I2 = 0%), but there was significant heterogeneity for VSS (P = .006, I2 = 76%).

Forest plot of Botox’s impact on VAS.
Forest plots for scar width at FP (Figure 3) and SP (Figure 4) supported the use of BTA for achieving a smaller scar width with P < .0001 for both (95% CI: −1.09 [−1.56 to −0.63] and 95% CI: −0.94 [−1.37 to −0.50], respectively). There was no significant heterogeneity for scar width at either time points, (P = .14, I2 = 45% and P = .17, I2 = 40%, respectively).
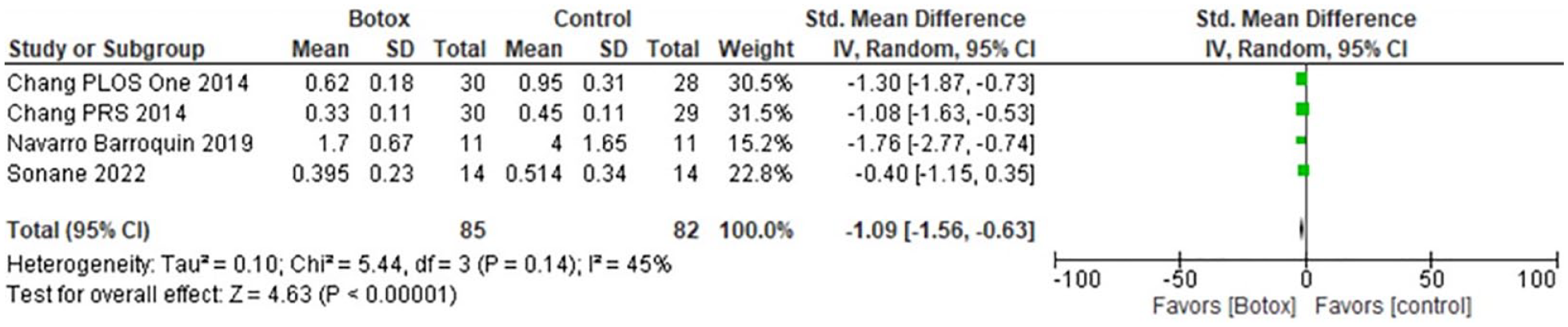
Forest plot of Botox’s impact on scar width at the first time point (FP).
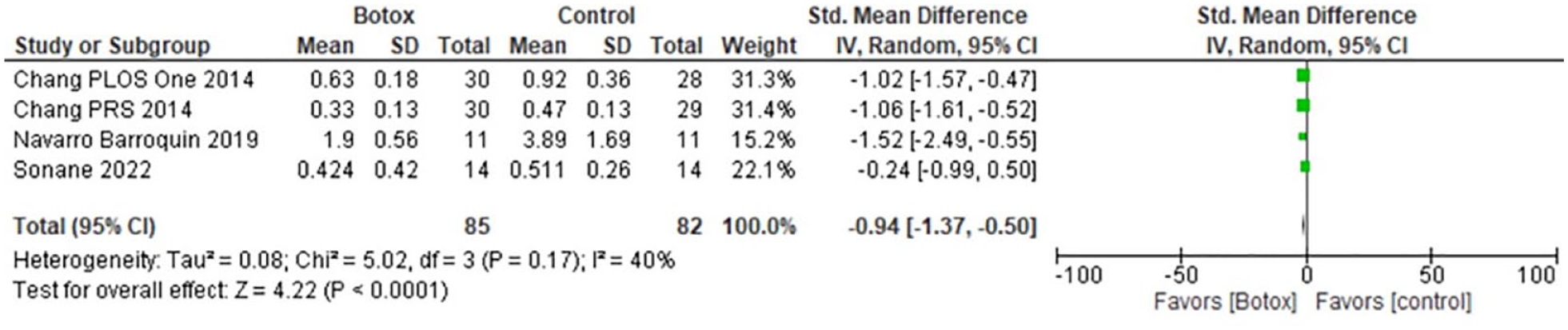
Forest plot of Botox’s impact on scar width at the second time point (SP).
Pooled forest plots for VAS comparing BTA and Dermabond supported the use of BTA with improved VAS (95% CI: 1.66 [1.27-2.05], P < .0001) when compared to the use of Dermabond (95% CI: 0.07 [−0.48 to 0.61], P = .80). There was no significant heterogeneity for VAS for BTA (P = .45, I2 = 0%) or Dermabond (P = .82, I2 = 0) (Figure 5).
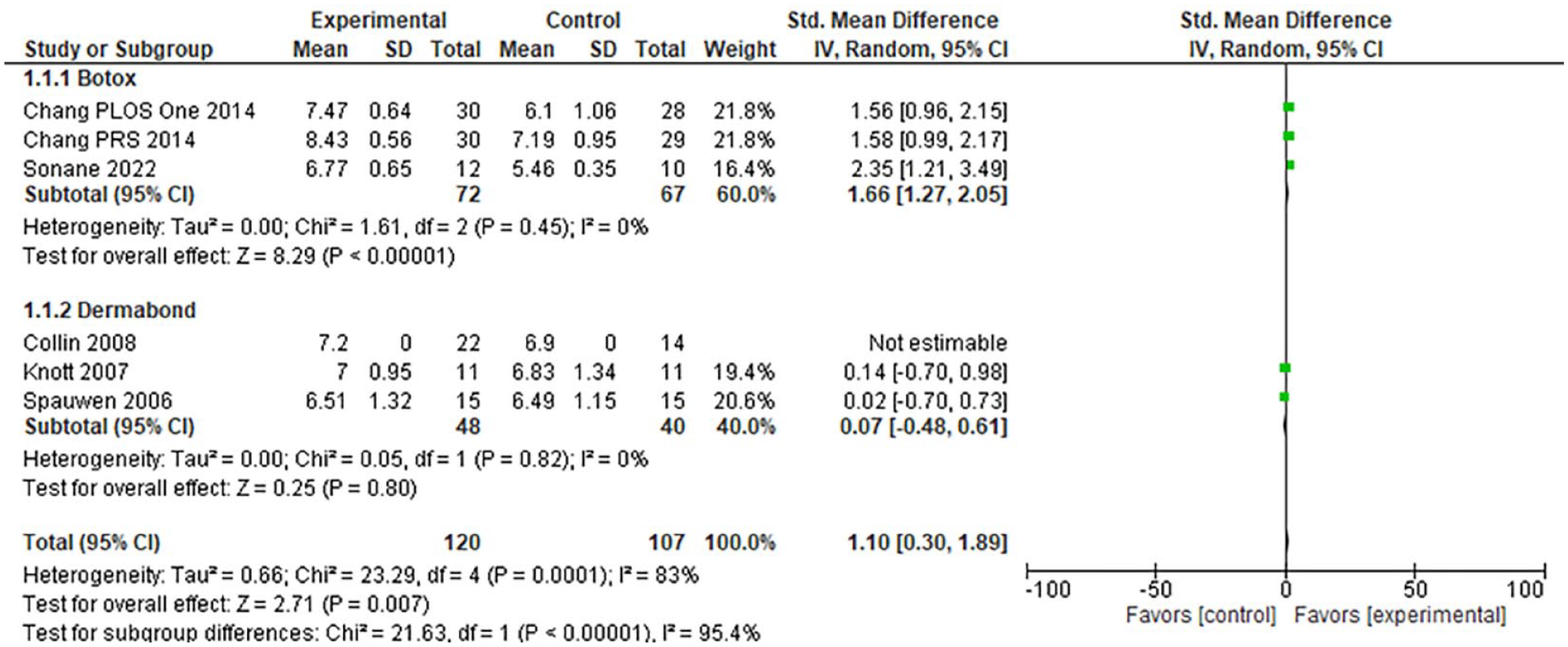
Pooled forest plot of Botox and Dermabond’s impact on VAS.
Of the articles that analyzed Dermabond, scar appearance in the form of VAS, HWES, or CVAS was not statistically or clinically significant with regard to the traditional suture closure group, and as such forest plots were not created for those outcomes.
Complications after the use of BTA included one incidence of temporary asymmetric oral commissure and none of the articles reported feeding issues. Complications associated with Dermabond included one incidence of a superficial skin reaction to the glue, 3 instances of a red scar, and 3 instances of a hypertrophic scar. The rates of scar revision were reported in 2 studies, Knott and Wilson. Knott reported no revision in the Dermabond group compared to 10% rate for the traditional suture group. Wilson reported no revisions required in the Dermabond group versus 6% rate in the steri-strip group.
Discussion
We sought to compare the roles of Botox and Dermabond in improving scar appearance in CLR. These 2 methods have previously been documented separately, but have not yet been compared. Our meta-analysis revealed that Botox improved subjective and objective esthetic measurements, whereas Dermabond showed no significant improvement in these measures.
Botox is postulated to improve scar quality by 2 mechanisms: the first is by reduction of the mechanical load at the wound edges through chemoimmobilization of the perioral muscles.17,18,21,22 The second more recently described mechanism is through the inhibition of TGF-b1/SMAD and ERK pathways as demonstrated in hypertrophic scar fibroblast cell line studies.23,24 The latter suggests that further research should be conducted to understand the cellular pathways by which Botox impacts wound healing.
Dermabond has historically been used for closure in a variety of surgical and traumatic wounds since its FDA approval in 1998. Not only does it provide a bacteriostatic barrier from the patient’s physical environment, but also when used in the setting of cleft lip repair can act as a physical immobilizer to decrease tension at the wound edges. In 2001, Shapiro et al. measured the tensile strength of Dermabond versus interrupted subcuticular absorbable sutures and found no difference in the strength of closure. 25 Its application has broadly been used in sternotomy closures, nail bed injuries, blepharoplasty closure, and reduction mammaplasty; the studies have shown similar scar quality in comparison to sutures.26 -29 In primary and secondary CLR, Dermabond has been reported to have excellent cosmetic outcomes similar to suture use, as well as simplified incision care and decreased infection rates.30 -32 Dermabond may be preferential to other techniques because the adhesive film is nontoxic and infants can begin feeding normally in the postoperative period (International Standards Organization ISO). The film can be left in place until it sloughs off the skin in 7 to 20 days. 30
To date though, researchers have only studied Dermabond as a replacement or adjuvant to sutures, rather than as a “stiff mold” to decrease tension on the wound edges. Studies have shown lower infection rates and similar hypertrophic scar rates when Dermabond was compared to Steri-Strips in unilateral CLR. 30 At our institution, Dermabond is uniquely applied over absorbable sutures in the form of a physical immobilizer at the end of wound closure to provide a protective barrier, allow normal feeding, and potentially decrease the tension at the wound edges by serving as a cast that mechanically immobilizes the lip. However, in our meta-analysis, we found that the data is potentially skewed in the favor of Botox because it has been intentionally used for scar appearance whereas Dermabond is used as an adjuvant or replacement of sutures rather than also as an immobilizer. Given the current evidence that suggests Dermabond has superior scar cosmesis 31 and our institution’s technique to immobilize the lip using Dermabond, future research is needed to characterize the utility and outcomes using TAs in improving scar quality.
One of the key components in identifying a tool to improve scar quality in CLR is safety. The intervention should not pose a greater risk than the surgery itself or comparable standard techniques. For studies examining Botox in CLR, one study reported a single incidence of temporary asymmetric oral commissure that resolved. 33 Other than this study, there have been no additional reports of a negative impact of Botox on infant feeding or reports of additional toxicity. In the studies we included for Dermabond, 1 patient had a reaction to the TA 14 days after application. 10 Regardless of the limited reports of toxicity, extra care should be taken when using either Botox or Dermabond in the infant population. For Botox, a miscalculation can lead to the feared complications of systemic absorption or temporary effects on feeding secondary to paralysis, and for Dermabond, the low viscosity and excess runoff has the potential to seal portions of the eyelid.34,35
Additionally, socioeconomic factors, cost burdens, and treatment-related toxicity should be considered when choosing adjuvants for scar quality in CLR. Therapies utilizing presurgical molding, such as nasoalveolar molding (NAM) have heterogeneous protocols across institutions. As a result of the heterogeneity follow-up protocols for adjustments are highly variable, but most typically follow-up with weekly to biweekly clinic visits. One study found that NAM patients required an average of 11 dental visits, which accounted for $2312 in indirect lost income per family. 36 Expenses increase with more frequent clinic visits, time off of work for parents and guardians, and travel to cleft lip centers can require some families in the USA to travel over 65 miles. This physical and psychological strain of such financial burdens from cleft lip repair is known as a “form of treatment-related toxicity.” Studies have shown that financial toxicity increases the risk of lower quality of life, survival, and increased psychological stress. 37 These findings highlight that approaching each patient through a patient and family-centered decision treatment plan can improve outcomes. Although cost burdens and financial toxicity are not care metrics that are well understood in CLR, some of these findings suggest that an intervention that decreases the need for frequent clinic visits may positively impact families. The interventions we compared in our study are unique in their application. Dermabond is applied intraoperatively during wound closure and does not need to be reapplied. Botox can be injected pre-operatively or intra-operatively and its effects last 3 to 4 months. Botox and Dermabond would not replace NAM but serve as one-time adjuvants that may help decrease the overall need for clinic visits.
Our systematic review and meta-analysis have several limitations. The heterogeneity of the studies examining Botox did not have defined protocols for the timing of injections, follow-up, and post-operative care. The Dermabond studies were compared to sutures and due to this, our meta-analysis was skewed. Lastly, there is a paucity of literature on both Botox and Dermabond use in CLR. Future studies would benefit from uniform protocols when evaluating scar quality, post-operative care, and a minimum of 1-year follow-up. However, we believe that even with the limited literature available and the evidence we have gathered it is worthwhile to investigate these findings further.
Conclusion
Overall, the current literature supports the use of Botox for cosmetic improvement of the lip following cleft lip primary repair or revision as a result of decreased tension on the closure due to its induction of temporary paralysis. Dermabond has the advantage of not requiring suture removal and has comparable cosmetic outcomes with regard to traditional suture closure, but in these studies was only used as a replacement or adjuvant for sutures rather than as an immobilizing cast and thus more research is needed to solidify its role in these cases. Overall there is a benefit to the utilization of both techniques during cleft lip repair for both improved esthetic outcome and patient convenience. However, the data in support of Dermabond’s utility in improving scars for CLR is more limited which highlights the need for further studies to determine its role in these cases.
Footnotes
Appendix
Search Terms.
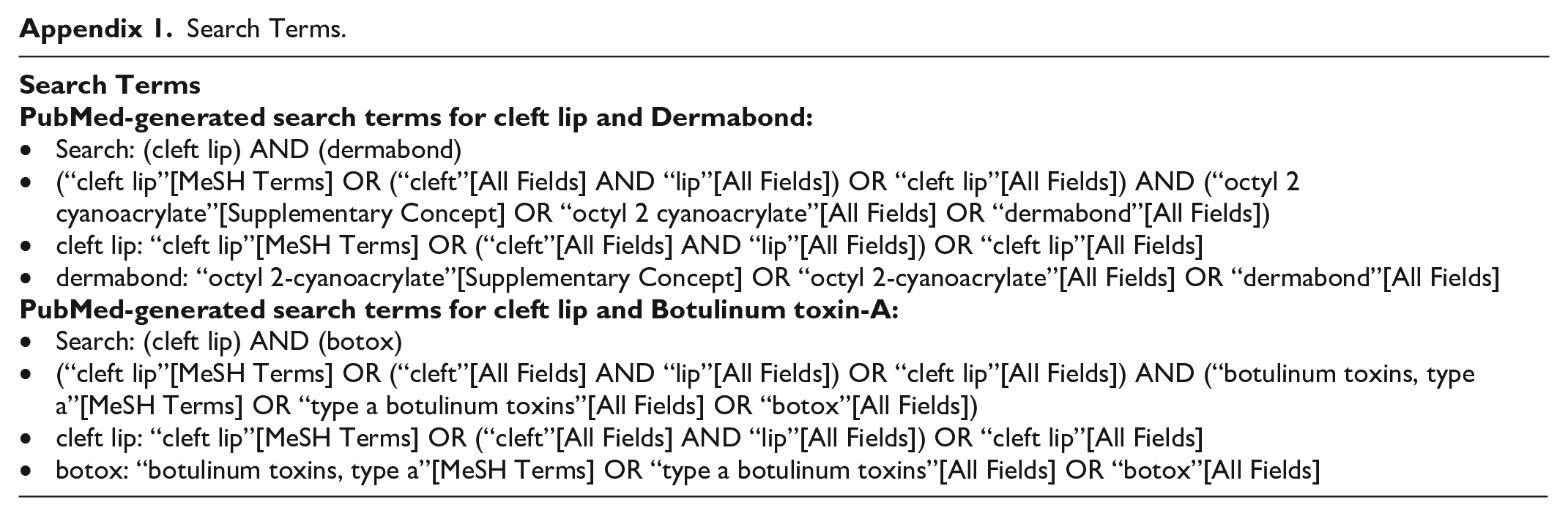
• Search: (cleft lip) AND (dermabond) • (“cleft lip”[MeSH Terms] OR (“cleft”[All Fields] AND “lip”[All Fields]) OR “cleft lip”[All Fields]) AND (“octyl 2 cyanoacrylate”[Supplementary Concept] OR “octyl 2 cyanoacrylate”[All Fields] OR “dermabond”[All Fields]) • cleft lip: “cleft lip”[MeSH Terms] OR (“cleft”[All Fields] AND “lip”[All Fields]) OR “cleft lip”[All Fields] • dermabond: “octyl 2-cyanoacrylate”[Supplementary Concept] OR “octyl 2-cyanoacrylate”[All Fields] OR “dermabond”[All Fields] • Search: (cleft lip) AND (botox) • (“cleft lip”[MeSH Terms] OR (“cleft”[All Fields] AND “lip”[All Fields]) OR “cleft lip”[All Fields]) AND (“botulinum toxins, type a”[MeSH Terms] OR “type a botulinum toxins”[All Fields] OR “botox”[All Fields]) • cleft lip: “cleft lip”[MeSH Terms] OR (“cleft”[All Fields] AND “lip”[All Fields]) OR “cleft lip”[All Fields] • botox: “botulinum toxins, type a”[MeSH Terms] OR “type a botulinum toxins”[All Fields] OR “botox”[All Fields] |
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Institutional Review Board approval was not required.