
Abstract
Introduction
Craniofacial Trauma and Anomalies affect a substantial proportion of the global community, especially those within the low-and middle-income countries (LMICs). In LMICs, the difficulties with access and the cost of rehabilitation put treatment beyond the reach of vast numbers of affected individuals.1,2
The scope of craniofacial conditions may include anomalies like cleft lip and palate, craniofacial clefts (Tessier), craniosynostosis, encephaloceles, craniofacial trauma, and orthognathic pathologies.
Cleft lip and/or palate occurs in approximately 1 per 500 to 700 births. Thus, there are about 220 000 new cases each year globally, and the prevalence varies considerably across geographic areas or ethnic groupings. 2 The incidence of craniosynostosis is as high as 1 in 2000 but varies by the type of fusion,3,4 with the non-syndromic subtype present in 0.4 to 1 in 1000 births. 5
Anterior encephaloceles are seen more commonly in Asia, Africa, and Russia, with 1 case in 3500 to 6000 live births. However, they are much less frequent in North America and Europe (1 case in 35 000 live births). 6
The vast majority (90%) of trauma-related deaths occur in resource-limited settings, The global disease burden for CMF trauma largely occurs within LMICs. Over 7.5 million new facial fractures occurred in 2017.7,8
Most of the literature stresses the concept of a team approach for craniofacial surgery and, therefore, the need for the cooperation of different specialists to provide optimal care for the patient.9 -13 Complex craniofacial surgery, other than for cleft lip and palate, is practised mainly in the advanced countries of Europe and America. South Africa has the only well-established craniofacial surgery service in Africa.
In low-resource environments, patients often experience delays in care after sustaining craniofacial trauma, which increases the risk of complications and poorer outcomes, while others remain untreated and live with defects. 14
Many LMICs depend on foreign missions, visiting surgical teams and benevolent organizations for the treatment of such complex craniofacial anomalies. However, the recent COVID-19 pandemic has highlighted the need for local capacity development.
This study describes the gains in developing local capacity for complex craniofacial surgery in Kumasi, Ghana, through international collaboration.
Methods
Evolution of Partnership
The Komfo Anokye Teaching Hospital (KATH) established a multidisciplinary cleft clinic in 2003. The clinic collaborated with partners from Seattle, USA, Nigeria, and Ethiopia to advance team cleft care throughout Africa. Over the years, several other partnerships have been developed for capacity development and training.
In 2005, with support from colleagues in Seattle, the American Cleft Palate/Craniofacial Association (ACPA) elected Dr Peter Donkor, as a Visiting Scholar when he visited established cleft/craniofacial centers in Seattle, Washington, Rochester, New York, and Birmingham, Alabama. The visit to Birmingham brought him in contact with Dr John H Grant, the craniofacial team lead. In 2011, Dr John H. Grant visited OUR CENTER to explore the potential for establishing a collaboration with KATH to enhance craniofacial surgical capacity. In 2013, Dr John H. Grant III received an endowed chair with funding that enabled him to support the training of surgeons from developing countries in craniofacial surgery. An important condition for the award was that trainees had to return to their home countries to practice and teach others.
Based on consultations between Dr J.H.Grant and Dr Peter Donkor, Dr Solomon. Obiri-Yeboah, then a senior resident of Dr Donkor, was selected as the first international fellow to train in craniofacial surgery in Birmingham.
During Solomon’s training, the need to train a neurosurgeon from OUR CENTER to partner with him became evident, and Dr James Johnston, a neurosurgeon colleague of DrGrant on the Alabama Craniofacial team, sourced for funding to support the training of Dr Frank Nketia Boakye, a Kumasi based neurosurgeon alongside Solomon. The 2 surgeons returned to THEIR HOME COUNTRY in 2016 and started to jointly perform complex craniofacial surgeries for patients requiring them. From 2017 until the outbreak of the COVID-19 pandemic in 2020, the Alabama craniofacial team visited the team yearly for joint surgeries, further training, building and strengthening the collaboration (see Figures 1–3). The success, the challenges and the prospects of this initiative are described.

From left to right; Drs Peter Donkor, John H Grant, Solomon Obiri-Yeboah, James Johnston, and Frank Nketia Boakye.

With Dr. Grant in clinic and OR.

Alabama children’s craniofacial team’s yearly visit to KATH.
Formation of the Multidisciplinary Craniofacial Team
A multidisciplinary cleft team has existed at our center since 2003 and has grown steadily. In 2015, while the first author was in training realized the need for a neurosurgeon on the team and hence, initial meetings to identify a suitable one were made. The Second author, who was then also in training was made to join the first author to be trained by the same team. On Return, a pediatric intensivist, then the only one in the hospital was approached and gracefully agreed to join the team. The team has since been growing steadily through dialogs and training.
Review of Cases Done
A retrospective review of patients seen by the Multidisciplinary Cleft and Craniofacial team from January 2016 to December 2022 at Komfo Anokye Teaching Hospital was conducted. Six hundred forty-six cases of orofacial clefts, craniofacial traumas, and other complex craniofacial conditions were reviewed (Figure 4). The diagnoses were confirmed by clinical examinations and radiographic imaging.
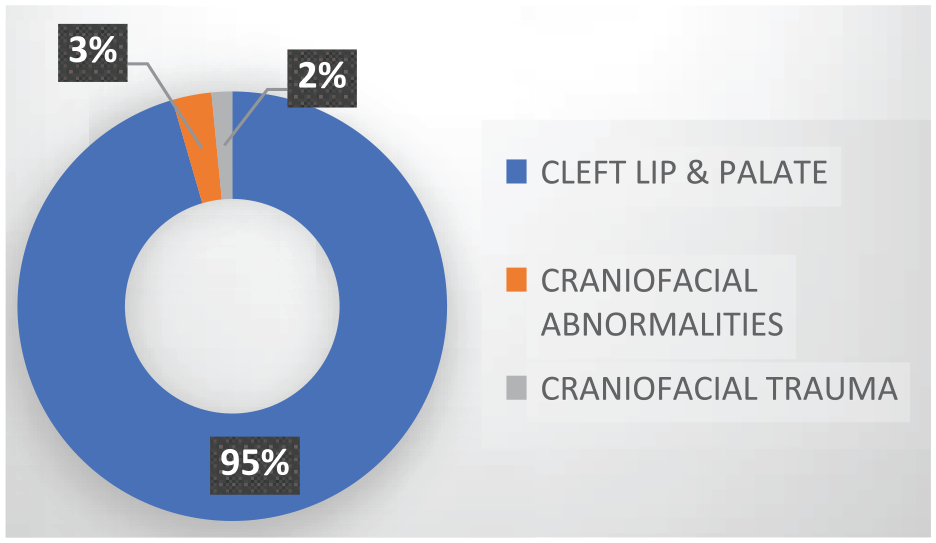
Distribution of craniofacial conditions.
The diagnoses of the Cleft cases were basically clinical, and the other craniofacial cases confirmed by clinical examinations and radiographic imaging such as CT scans and MRIs. All these images are readily available in our center. Cases done under the period of review include various forms of cleft lip and palate. (Figure 5), Tessier facial clefts, syndromic and non-syndromic craniosynostosis, Frontonasal/Frontoethmoidal encephaloceles. and others (Tables 1 and 2).
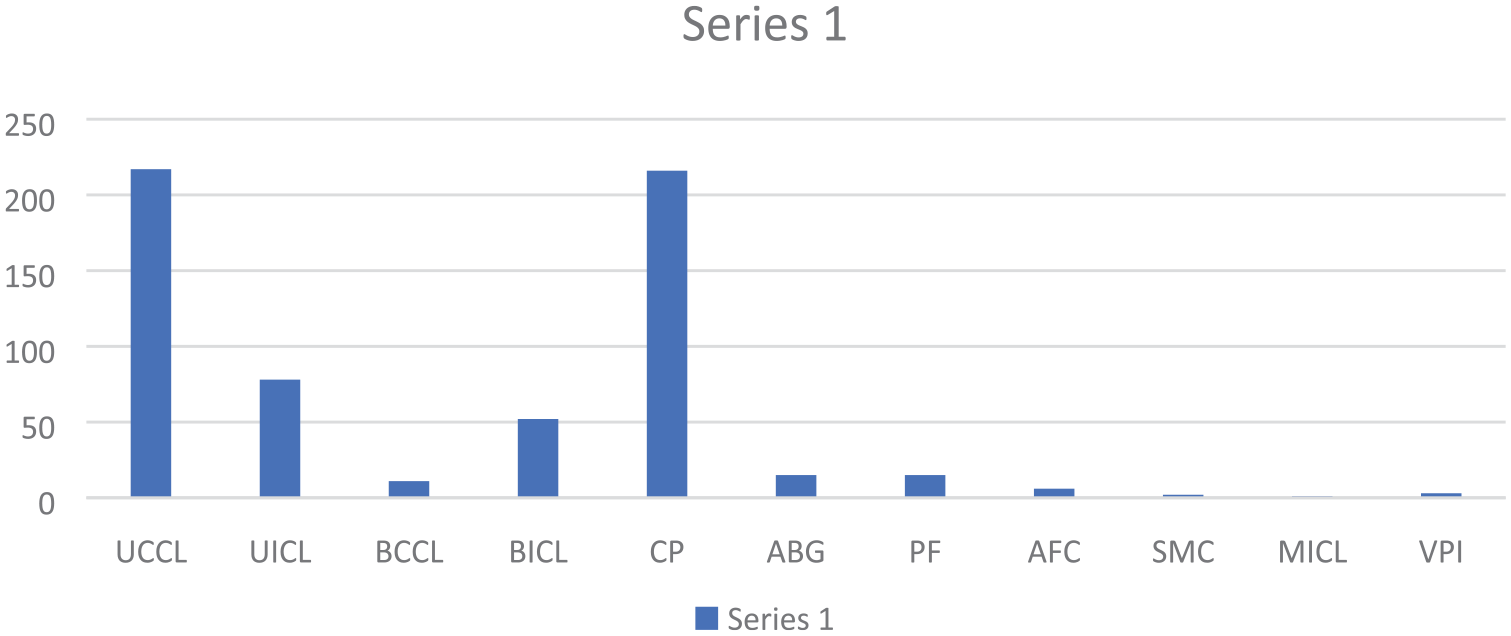
Distribution of orofacial cleft.
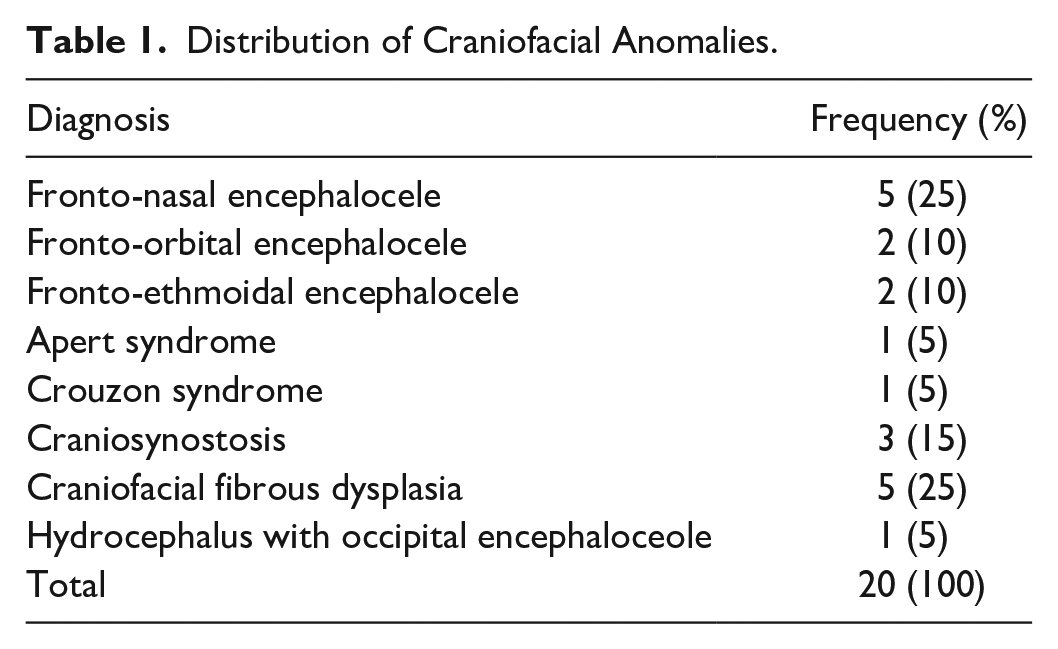
Distribution of Craniofacial Anomalies.
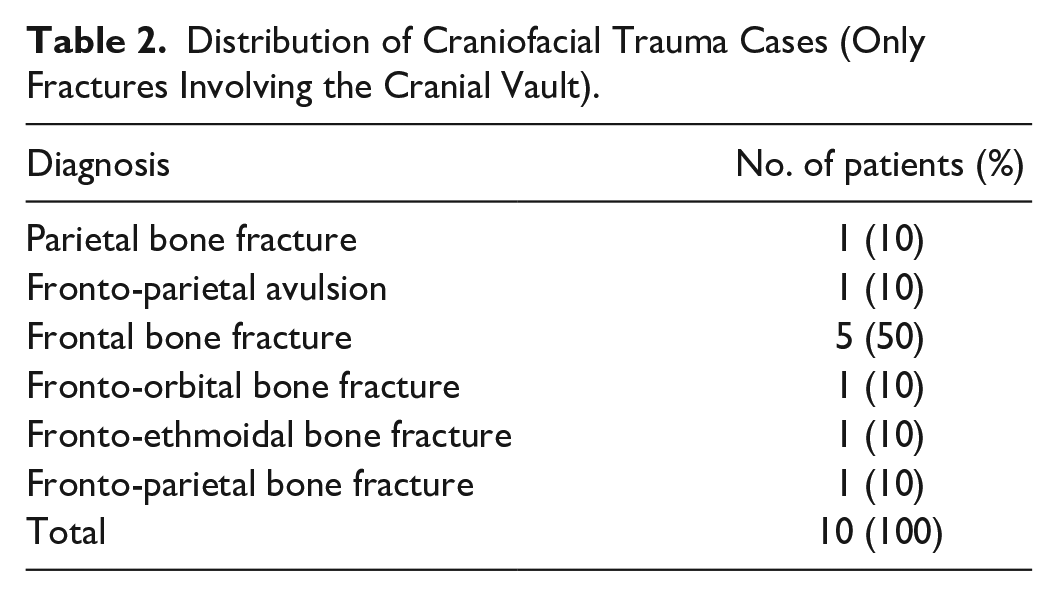
Distribution of Craniofacial Trauma Cases (Only Fractures Involving the Cranial Vault).
Modified Milard’s technique was used for the unilateral cleft lips, modified Manchester technique was used for the bilateral cleft lips, Langenburg, 2 flap palatoplasty, and Furlow double opposing Z palatoplasty were used for our palate repairs depending on the presentation (Figures 6 and 7). Frontoorbital advancement with cranioplasty of various forms was used in syndromic and non-syndromic craniosynostosis (Figure 8). For the encephaloceles, frontal orbital bandeau rearrangement was performed (Figure 9) with autologous calvarial bone graft, while a cranioplasty utilizing autologous split calvarial graft was performed on comminuted skull fractures, open reduction, and internal fixation was performed for depressed skull fractures, and alloplastic bone cement was used for large calvarial defects following trauma or Pott puffy tumor treatment (Figure 10).
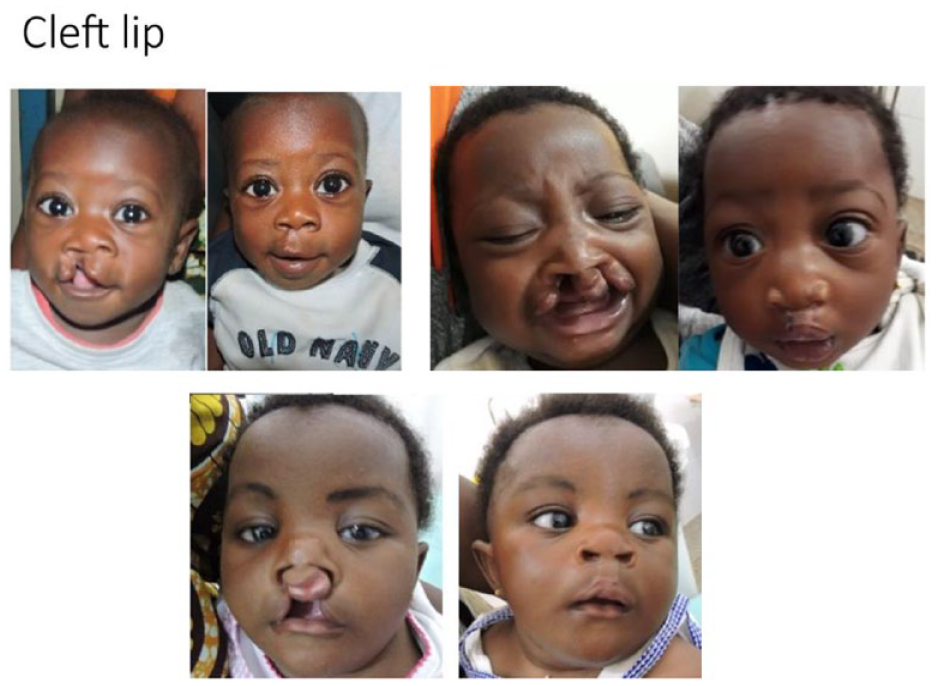
Cleft lip.
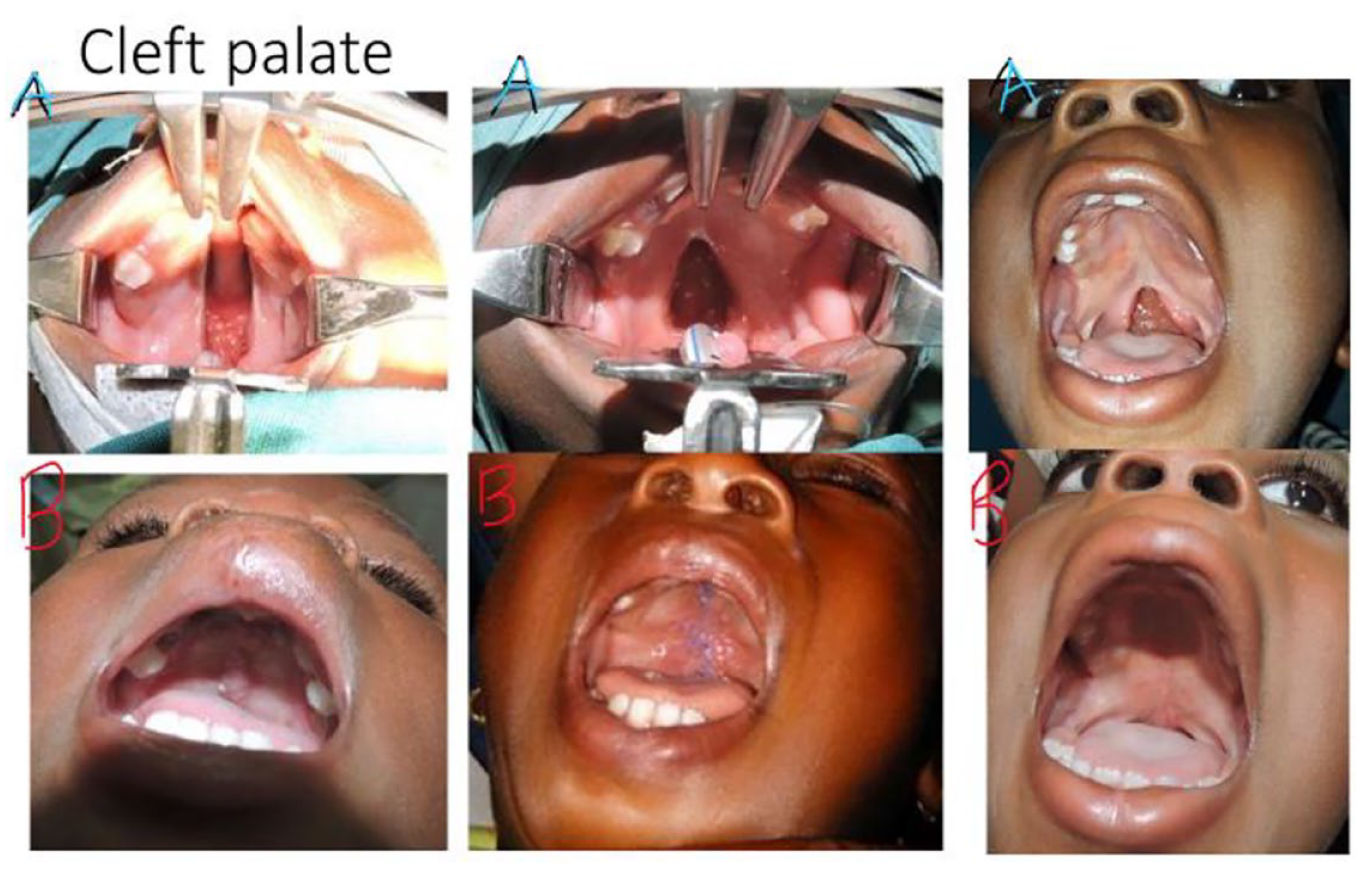
Cleft palate.

Craniosynostosis, fronto-orbital advancement, cranioplasty.
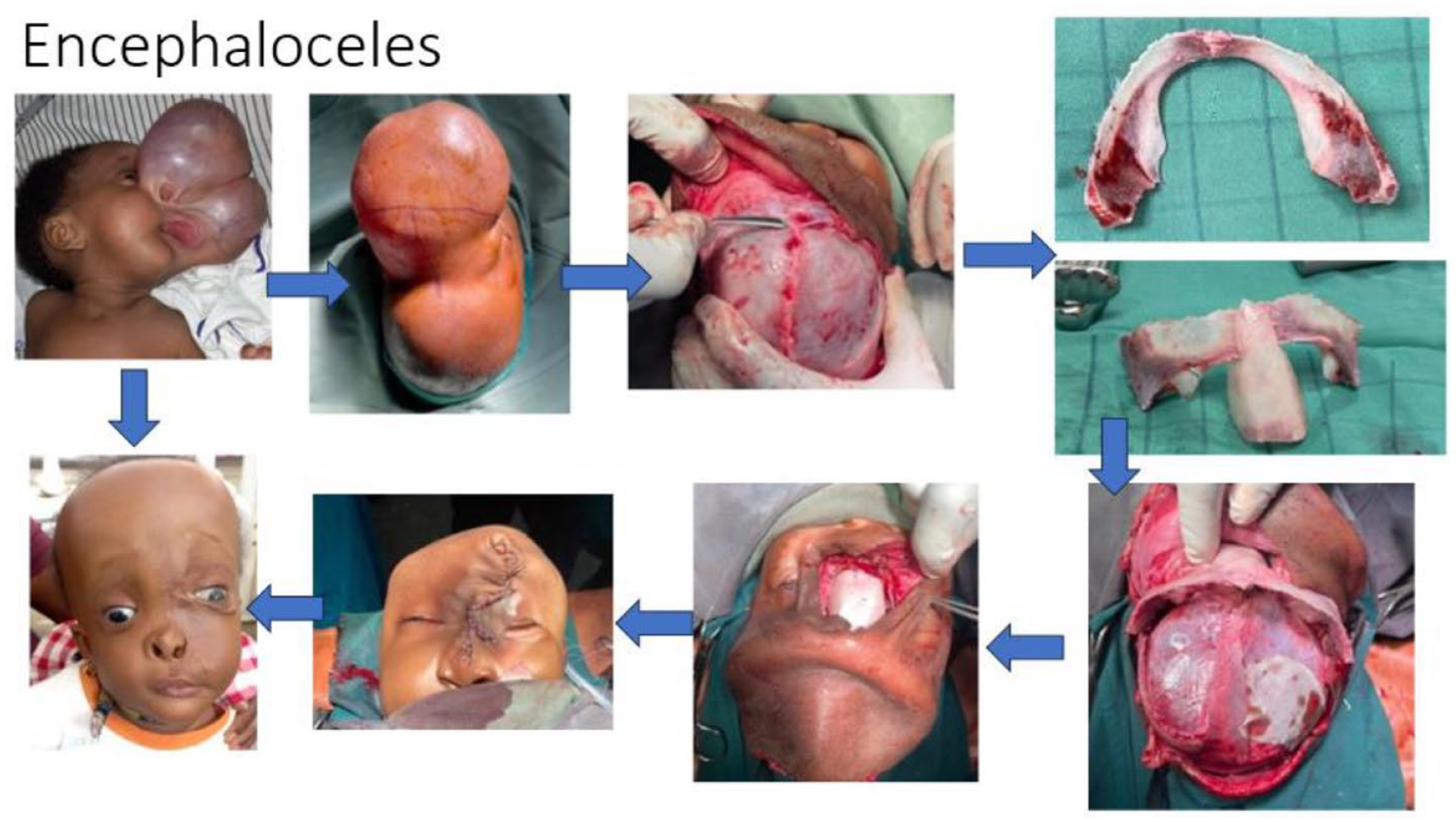
Encephalocele.
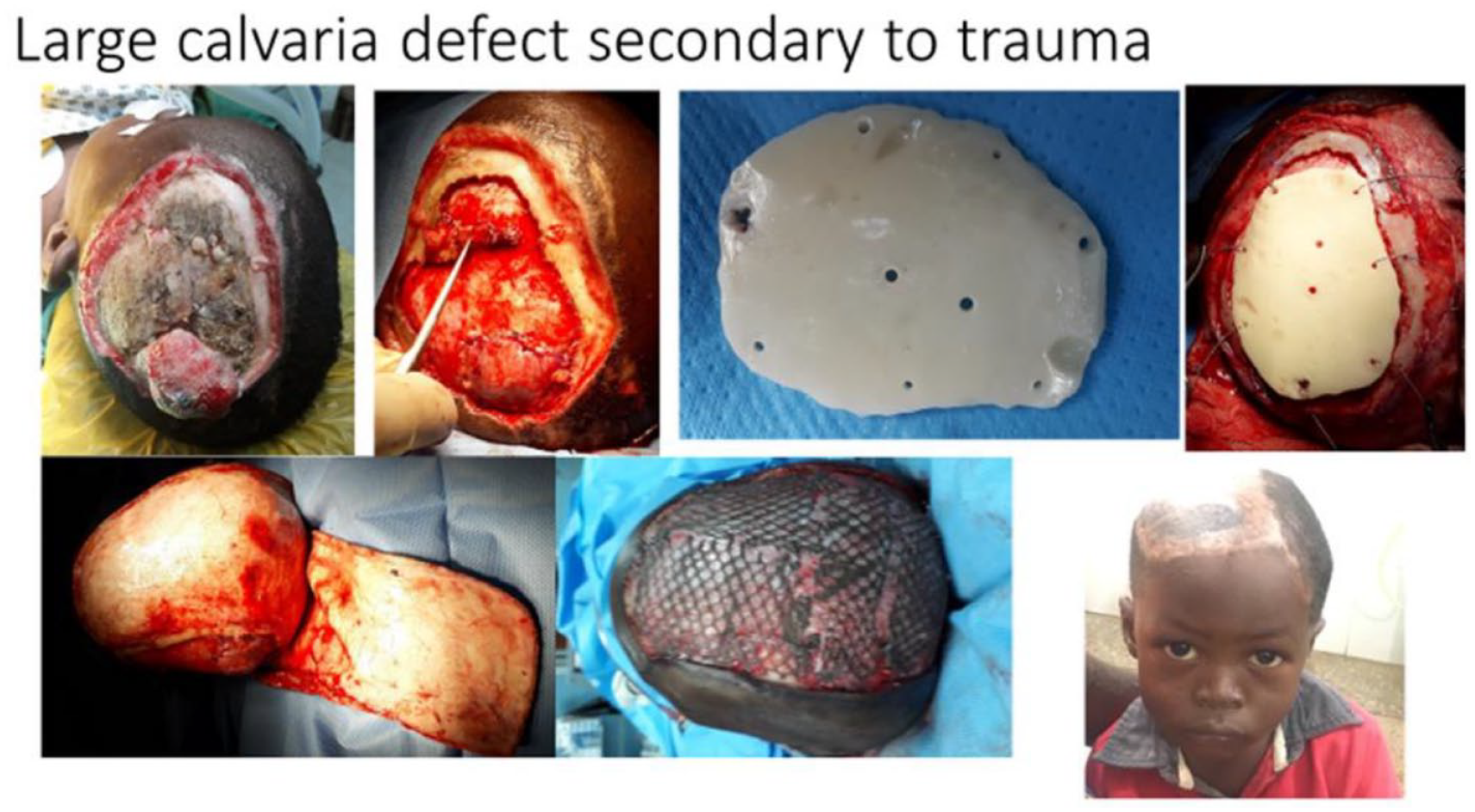
Large defect, the use of alloplastic bone cement.
All patients were reviewed by the cleft palate and craniofacial multidisciplinary team before surgery, and all specialties were involved in the post-operative management as well. Informed consent was obtained from all patients.
Results
A total of 646 patients were operated over the period under review, out of which 616 (95.4%) cases were orofacial cleft, 20 (3.1%) cases of other craniofacial anomalies, and 10 (1.6%) cases of craniofacial trauma affecting the face and cranial vault or base of the skull. There were 304 males and 342 females, with their ages ranging between 3 months and 53 years. The majority (90.9%) were in the age group of 0 to 10 years, followed by 11 to 20 years (5.9%); 21 to 30 years (2.0%), and the rest above 30 years.
Discussion
A long-term collaboration between Komfo Anokye Teaching Hospital, Kumasi, Ghana and the University of Alabama, Birmingham and Children’s of Alabama, created the opportunity for two Ghanaian surgeons to undergo fellowship training in craniofacial surgery in the US. Since their return, they have developed a service for complex craniofacial surgery that incorporates the combined efforts of multiple specialties, including anesthesia, pediatrics, maxillofacial surgery, neurosurgery, nursing, nutrition, and social work.
During the 6-year period under review, 646 patients were treated surgically. with 95% of cases being orofacial cleft.
Significantly, 30 patients were operated on for a variety of craniofacial conditions which were not previously treated at our center. Though the numbers are low compared with more established craniofacial centers elsewhere,9,15 -17 these are expected to increase with increased awareness of the service over time. Multidisciplinary cleft care has been in existence in our hospital since 2003, and hence, awareness of cleft lip and palate is higher than that of the other craniofacial anomalies. Hence, it will require further exposure to inform the Ghanaian public about the availability of expertise for managing complex craniofacial anomalies in the country.
Craniofacial anomalies and trauma represented 3% and 2%, respectively, of total cases seen. The variety of conditions seen, including encephaloceles, craniofacial syndromes with craniosynostosis, and fibrous dysplasia, highlighted the burden of craniofacial conditions among the population that go untreated even after successful diagnosis.
Craniofacial trauma represents an area requiring unique expertise and multidisciplinary care when confronted with complex injuries involving the face and cranial vault.
Challenges
Establishing a craniofacial practice in deprived countries such as Ghana is not without challenges. Some of the challenges faced within the period under review include;
Multidisciplinary Team approach
Developing and maintaining cleft and craniofacial teams in LMICs is challenging due to a lack of expertise and the fact that the few are overburdened. The challenge with creating teams in places like Ghana is that the multidisciplinary clinic is “Voluntary” and extra duty for the providers. Hence, they don’t make it to the multidisciplinary clinic when they are busy with their primary responsibility.
Diagnosis of Craniofacial Cases
In addition to the classical clinical signs of encephaloceles, non-syndromic craniosynostosis, and syndromic craniosynostosis like Cruzons and Apertz syndromes, the diagnosis is based on conventional X-rays, computed tomography scan (CTS), 3D CT, magnetic resonance imaging (MRI), and ultrasonography.
For complex craniofacial cases, CT scan with 3D reconstruction and MRI are performed at our center. The biggest challenge here is Cost. None of these diagnostic imaging are covered by national health insurance, so patients have to pay out of pocket. Unfortunately, many patients cannot afford and thus delay treatment.
Treatment
In advanced countries, virtual surgical planning is used to simulate osteotomies and repositioning of bone segments during cranial vault remodeling for correction of craniosynostosis and orthognathic surgeries.18,19 Others use endoscopic approaches, especially in sagittal synostosis. Most centers in advanced countries are moving toward the use of resolvable plating systems, especially in pediatric cases. The technologies are not available in our center and hence make use of the traditional way of managing these cases. Stainless steel wires 26/28 gauges are used most often due to the patient’s inability to afford titanium microplates.
Another challenge with managing complex craniofacial cases in LMICs like Ghana is the need for a Pediatric Intensive Care Unit (PICU) with a pediatric intensivist. In our center, there are limited PICU rooms and cases are delayed or rescheduled severally due to the limited availability of PICU space.
Complications
The most common complication recorded has been post-operative infections and extrusion of the tips of stainless-steel wires. All infections were treated with antibiotics after culture and sensitivity, extruded wires and those under the skin that causes discomfort were removed.
The Prospects
The West African sub-region is still a virgin land for craniofacial practice, and there is a huge deficit of surgical skills, anesthesia, and intensive care resources. Hence, there is a need to train more professionals to replicate ourselves within the countries in the sub-region. There is a huge gap in skill training, human resources, equipment, and materials that international collaborators can help fill.
With the help of Smile Train a national cleft and craniofacial center is being built in Kumasi, and with this, many more children born with cleft palate and craniofacial anomalies will receive care. The Komfo Anokye Teaching Hospital craniofacial center is poised to become a center of excellence in cleft and craniofacial care, capacity building and research in the sub-Saharan African subregion.
Conclusion
Through successful international collaboration, a service for treating patients with complex craniofacial conditions is being developed at the Komfo Anokye Tteaching Hospital in Ghana. In the midst of all the numerous challenges, success has been chopped, and solutions are being made every day to surmount the challenges. This expertise will hopefully be extended to other countries in the African region to reduce dependency on external expertise.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The study was approved by the Institutional Review Board at Komfo Anokye Teaching Hospital (KATHIRB), with approval number “KATH-IRB/AP/032/20.”