
Abstract
The nasal columella presents one of the most intricate challenges in facial reconstruction due to its unique contours and limited availability of adjacent tissue. Several surgical techniques exist for successful columellar reconstruction, and the choice of approach depends on factors such as the size of the defect, surgical expertise, and overall esthetic goals. In cases involving substantial columellar defects, or deformities affecting multiple nasal subunits, local or regional flaps are often necessary to achieve optimal reconstruction. In this report, the authors present a case of pediatric columellar reconstruction utilizing a modified local flap technique derived from the upper lip lift used in esthetic surgery for facial rejuvenation and lip enhancement. This method distinguishes itself from previous adaptations by remaining entirely subnasal, without extending beyond the width of the alar base, disrupting the philtrum, or disturbing the orbicularis oris muscle. This technique offers notable advantages for pediatric patients, such as its ability to minimize scarring, prevent additional deformities, and be performed in a single stage.
Level of Evidence:
Level IV, case study.
Introduction
The nasal columella is widely recognized as one of the more challenging facial structures to successfully reconstruct due to its distinctive contour and the limited availability of adjacent tissue for reconstruction.1-3 Additionally, the columella is a critical esthetic subunit of the nose, influencing both nasal tip projection and definition of the nasolabial angle. 4 During the reconstructive process, additional esthetic considerations include skin tone, subcutaneous bulk, and areas of transition between the base of the columella, nasal tip, and nasal floor. 5 The ideal columella begins at the apex of symmetric nostrils and has a width equal to the distance between the defining points of the nasal tip. 6 The base of the columella exhibits a slightly broader width than the apex, with an overall height that measures approximately two-thirds the length of the base (Figure 1). 6
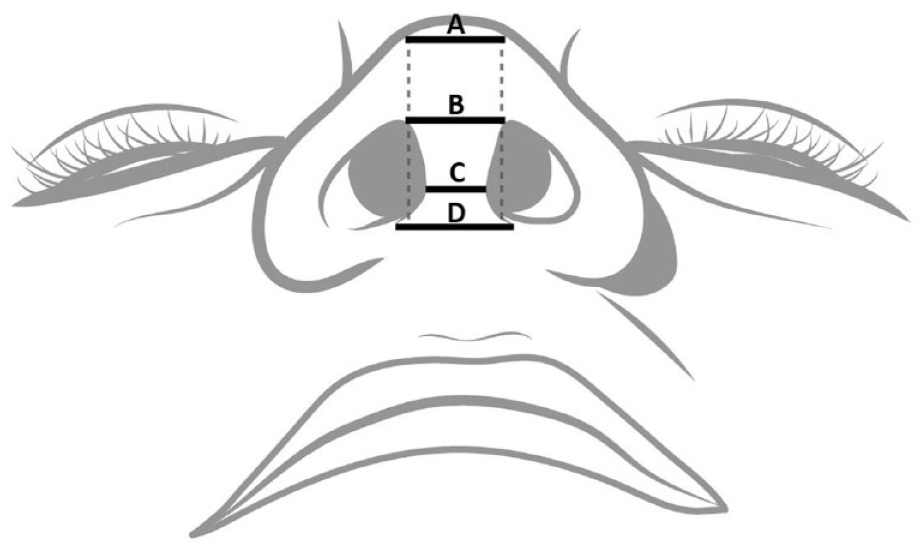
The ideal columella begins at the apex of the nostrils (B) with a width equal to the distance between the tip defining points (A). It tapers down to reach its narrowest point where the lower and middle thirds of the columella meet (C) and gently broadens toward the base, which exhibits a slightly greater width than the apex (D).
The etiology of columellar defects is extensive and includes traumatic injury, ischemia, cutaneous malignancy, vascular malformation, congenital absence of the columella, and nasal dysgenesis. 3 Numerous surgical techniques exist in the literature for successful columellar reconstruction, however, there is no single “best” method. Rather, the most appropriate surgical approach depends on the extent of the defect, surgical expertise, and esthetic goals of reconstruction. 3
Full thickness skin grafts and composite grafts are typically used for smaller columella defects. For small superficial defects limited to skin and subcutaneous tissue, full thickness skin grafts are preferred due to minimal scarring and multiple donor site options. 7 Composite grafts are more often utilized for small full thickness defects requiring additional soft tissue support. For larger isolated columellar defects or deformities involving multiple nasal subunits, local or regional flaps are often required for successful reconstruction. 3
Local flap sites include the nasolabial, nasofacial, nasal vestibule, alar, and upper lip regions (Figure 2). 3 Among the choices for local lip flaps, the philtrum and medially based upper lip flaps are the most prevalent, offering favorable esthetic outcomes with minimal donor site morbidity. 3 Additionally, pedicled and prelaminated labial mucosal flaps have been successfully used for reconstruction.8,9
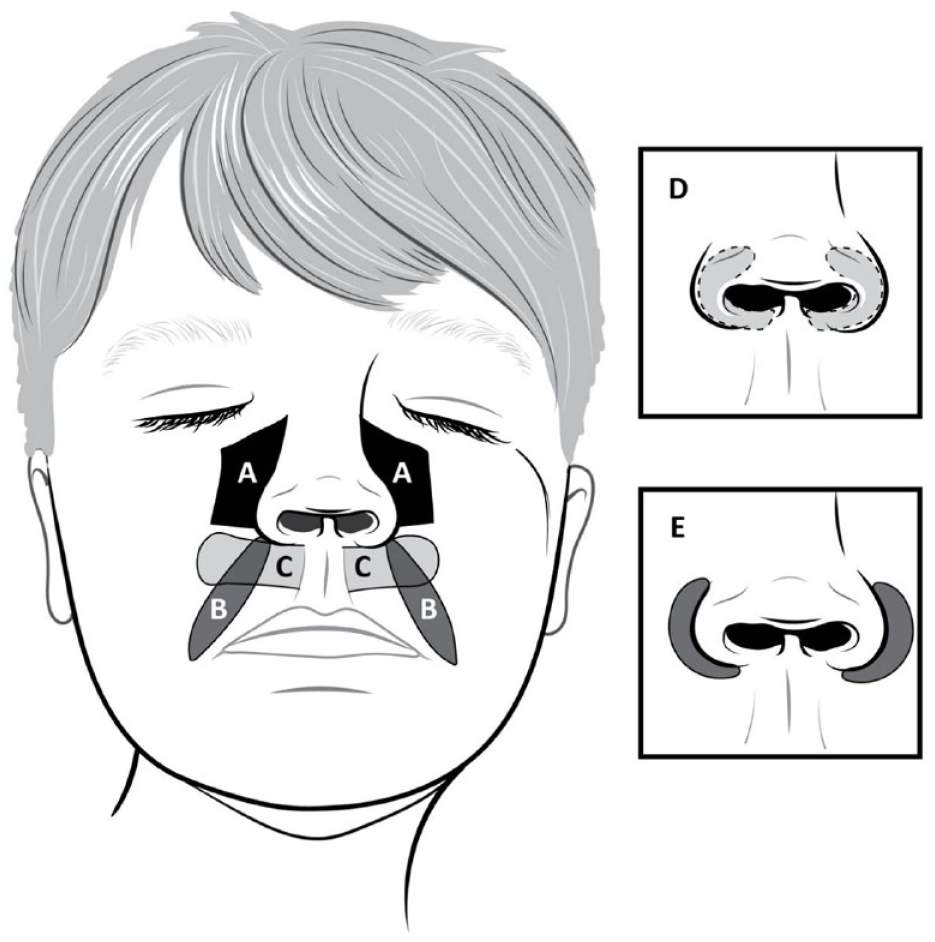
Local flaps are often used for reconstruction of larger columellar defects; common sites include (A) nasofacial, (B) nasolabial, (C) upper lip, (D) nasal vestibule, and (E) nasal ala.
Traditionally used for improvement in esthetic appearance, the upper lip lift employs similar techniques to local lip flaps and was initially adapted for columellar reconstruction by Pincus and Bukachevsky in 1990, later modified by Brunetti et al in 2020.10,11 To the best of our knowledge, this paper reports the first pediatric case of columellar reconstruction utilizing a modified lip lift approach.
Case Presentation
A 4-year-old female presented for evaluation of a columellar defect. Prenatal history was notable for delivery at 26 weeks via cesarean section, followed by an extended stay in the neonatal intensive care unit (NICU). Shortly after birth, the patient required intubation due to neonatal respiratory distress syndrome and was subsequently transitioned to nasal continuous positive airway pressure (nCPAP) on hospital day (HD) 5. Due to significant breakdown of the columella, she was weaned to nasal cannula on HD 17, at which time plastic surgery was consulted. Physical examination revealed complete columellar skin loss with an open wound; the caudal septum was not visualized due to overlying subcutaneous tissue. She did not receive plastic surgery intervention during this hospitalization and was recommended for reconstruction in 4 to 5 years.
The patient presented for follow-up at 4-years-old with complaints of loud breathing while sleeping and frequent epistaxis. On examination she had minimal columellar skin and very little septal cartilage (Figure 3). Reconstructive options were discussed with her parents, and shortly after the patient’s initial clinic visit, she underwent columellar reconstruction using a composite graft from the auricular helix.

Pre-operative photos taken during the patient’s initial evaluation for her columellar defect at 4 years old.
Unfortunately, the composite graft did not yield the desired result, so a second reconstructive procedure was offered to the patient. A lip lift for columellar reconstruction was performed approximately 7 years following the initial surgery (Figure 4). Bilateral incisions were marked inferior to the nasal ala, extending laterally to the alar crease without exceeding the width of the alar base or disrupting the philtrum. The skin graft from the initial surgery had significantly scarred and was removed from the previous columella cartilage graft. Bilateral subalar flaps were dissected along a subcutaneous plane directly adjacent to the underlying musculature, and the orbicularis oris was left undisturbed. Each flap measured 12 mm long and 7 mm wide. The flaps were then elevated from their medial pedicle and transposed perpendicularly to approximate the midline and cover the previous cartilage graft. The flaps were sutured together and anchored inferiorly to the nasal tip with 4-0 Vicryl to form the apex of the columella. The lateral edges of the flaps were secured to the septal mucosa with 5-0 Monocryl and closed superficially with 5-0 plain gut suture. The donor site defects were then repaired with deep dermal sutures using 4-0 Vicryl followed by 5-0 plain gut for reinforcement of the skin (Figure 5).

Pre-operative photos taken at 11 years old, prior to lip lift reconstruction, demonstrate significant scarring of the previous columella composite graft.

Photos on the top row show bilateral medially based subalar flaps marked prior to lip lift reconstruction. Photos on the bottom row show the newly reconstructed columella with bilateral flaps approximated along the midline.
Written informed consent for utilization of patient information, imaging, and pictures was provided by the patient’s legal guardians.
Outcome
Postoperative courses for both procedures were uneventful with no complications. However, the initial reconstruction with the composite graft did not heal as hoped and became scarred due to insufficient subcutaneous tissue. Consequently, the patient underwent a second procedure at 11 years old using a more robust reconstructive method. The patient was discharged home 2 hours after the lip lift for columella reconstruction. She was unable to present for follow-up as she lived out-of-state, therefore, the patient was evaluated via telemedicine; no concerns related to postoperative healing, nasal airway obstruction, or uncontrolled pain were reported. The patient sent photographs at 2 weeks postoperatively, which demonstrated appropriate healing with minimal scarring. Subsequent photographs sent at approximately 3 months postoperatively showed completely healed columella reconstruction (Figure 6).

Patient photos taken 2 weeks (top row) and 3 months (bottom row) following columella reconstruction.
Discussion
The nasal columella is a challenging subunit to reconstruct with high quality esthetic results. As such, numerous surgical techniques exist to address variations in deformity, donor site, and surgical expertise. 3 Local flaps are often used for larger full thickness defects and are optimal for isolated columella deformities that do not involve other nasal subunits. 3 In this report, we present a case of pediatric columellar reconstruction utilizing a local flap technique modified from the esthetic surgical upper lip enhancement procedure.
Lip lift techniques initially emerged to address the esthetic effects of upper lip soft tissue lengthening seen with aging in men and women. 12 In 1971, Cardosa and Sperli published the first subnasal lip lift, which was subsequently adapted by many surgeons. 13 One of the most popular modifications was Austin’s wavy ellipse, later modified by Spiegel as a bull’s horn excision, which is now the most commonly utilized technique for upper lip enhancement.12,14,15 Additional modifications to the upper lip lift include Jung et al ’s short scar technique that spares the columella and philtrum. 16
A case series by Pincus and Bukachevsky was the first to borrow techniques from esthetic lip lifts for columellar reconstruction. 10 Bilateral medially based horizontal flaps were created along the nasal sill and extended laterally to the nasolabial creases. Both flaps were then rotated medially, sutured together, and anchored to the nasal tip with good cosmetic results. 10 In 2020, this technique was modified by Brunetti et al for columellar reconstruction in an elderly woman with a defect from excision of desmoplastic basal cell carcinoma. 11 Similar to Spiegel’s lip lift, they created an incision within bilateral alar grooves that extended laterally and included a portion of the philtrum. The flaps were then transposed, as described by Pincus, and sutured together to reconstruct the caudal portion of the columella. 11 Although the flaps were harvested along the subcutaneous plane, the dissection proceeded deeper medially to include a portion of the orbicularis oris for adequate flap perfusion. 11
Our adaptation of the upper lip lift for columellar reconstruction differs from previous reports in that it is purely subnasal and does not exceed the width of the alar base or disrupt the philtrum. This is especially useful in pediatric patients who have full thickness columellar defects too large for composite graft reconstruction, as many local flaps result in donor site scarring that may be as prominent as the deformity itself.9,17,18 Of note, labial and nasofacial incisions are particularly difficult to camouflage in children.17-20 Our modified lip lift approach is well-suited for pediatric patients as it can be performed at a young age with low potential for discernible scarring.
Another advantage of our modified lip lift technique, in comparison to previous reports, is its shallow dissection and preservation of the orbicularis oris muscle. The orbicularis oris is a complex structure that serves multiple functions, including sphincteric activity of the mouth and facial expression. 21 Severe loss of muscle tone can result in noticeable drooping of the commissure, as well as difficulties with drooling or eating. 22 Complications such as nostril show, philtrum scarring, and animation deformity have been associated with surgical upper lip enhancement involving resection of the orbicularis oris. 12 In our modified lip lift technique for columellar reconstruction, we avoid any form of excision of the orbicularis oris, thus avoiding the potential for such complications.
Although our modification of esthetic upper lip enhancement offers numerous advantages over other techniques for columellar reconstruction, it is important to consider the possible pitfalls to keep in mind with this patient population. In young children without upper lip soft tissue lengthening, there is a risk of causing excessive tooth show with larger subalar flaps. Additionally, the apical redundancy caused by the medial rotation of the flaps may introduce small dog ear deformities. In cases with significant columellar defects that may not be fully addressed by the modified lip lift, this technique can be performed in a single stage with a cartilage graft or augmented with future fat grafting.
Conclusion
We present the first pediatric case to employ a modified upper lip lift approach for minimally invasive columellar reconstruction. While traditionally used in the elderly to address upper lip soft tissue lengthening, the surgical techniques designed for esthetic upper lip enhancement can be effectively adapted for reconstructive purposes. This adaptation holds tremendous potential for pediatric patients as it can be performed in a single stage and offers the advantages of minimal scarring and the prevention of complications that could otherwise lead to further deformity.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Disclosures
No disclosure.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Institutional Review Board approval was not required.