
Abstract
A traumatic arteriovenous fistula (AVF) is a type of acquired vascular malformation, caused by blunt or penetrating trauma. Traumatic AVFs result in a pathologic connection between arterial and venous vasculature, bypassing the corresponding capillaries. When an intra-operative insult to vasculature within a surgical site is implicated in the subsequent formation of a traumatic AVF, the suspected etiology is iatrogenic. Although the most common etiology of traumatic AVFs of the entire body is iatrogenic trauma, intraoperative vascular insults (ie, ligation and cauterization) are routinely delivered within maxillofacial surgical sites, without formation of an acquired vascular malformation. A traumatic AVF in the pre-auricular region is exceedingly rare and has infrequently been described as a complication following minimally invasive temporomandibular joint (TMJ) surgery, managed with endovascular surgery. We describe a rare case of bilateral TMJ arthroscopies complicated by the formation of a pulsatile, traumatic AVF between the right superficial temporal artery and right retromandibular vein, treated with minimally invasive endovascular embolization by the interventional radiology team. This case report highlights the diagnosis of a traumatic AVF in the pre-auricular region and multi-specialty management of an early complication of minimally invasive maxillofacial surgery.
Introduction
An arteriovenous fistula (AVF) is an abnormal vascular connection between an artery and a vein, bypassing the corresponding capillaries. There are 2 types of AVFs depending on etiology of the malformation: congenital or acquired. Acquired AVFs are the result of pathologic wound healing after trauma to vasculature. Traumatic events to vasculature result from physical injury with a blunt or penetrating foreign object. Traumatic AVFs (TAVF) are considered iatrogenic when they occur as a result of an intra-operative blunt or penetrating traumatic insult to vasculature within the surgical site. Generally speaking, iatrogenic vascular injuries (ie, transection, ligation) are not uncommon occurrences during open temporomandibular joint (TMJ) surgery and are managed with conservative local hemostatic measures. These transient iatrogenic vascular injuries are expected intra-operative occurrences of open surgery due to the extensive vascularity of the maxillofacial complex. However, a vascular injury that progresses to become an aberrant vascular anomaly like a TAVF is considered rare.1,2 The complication of an iatrogenic TAVF has previously been described as a complication following open surgical approaches to the maxilla and mandible; but development of iatrogenic TAVF as a complication of minimally invasive TMJ surgery has fewer than 10 published reports.1-5
In this article, we report an uncommon case of a 23-year-old female who acquired a unilateral TAVF of the right pre-auricular region, within her first post-operative week following bilateral minimally-invasive TMJ arthroscopies. This case report highlights the work-up and management of the uncommon complication of iatrogenic TAVF between the superficial temporal artery and retromandibular vein. This patient’s symptomatic TAVF was successfully treated via endovascular approach by our Interventional Radiology colleagues. This case report is written in accordance with the CARE guidelines.
Case Report
A 23-year-old female, with history of autoimmune-mediated TMJ arthritis, presented to our clinic on post-operative day 8 status post repeat bilateral TMJ arthroscopies, with complaint of progressive right pre-auricular pain (out of proportion compared to left) and pulsatile tinnitus of 8 days duration. Patient reports throbbing with audible rhythm of her heartbeat beginning on her first night post-operatively, mere hours after arthroscopic surgery. The patient endorsed a noticeable increase in right-sided discomfort with continued pulsatile tinnitus on post-operative days 4 and 5. The patient was compelled to seek emergency assistance for pain control at an outside hospital on post-operative day seven. The patient reported that at the outside hospital, no pain medication was given and advanced imaging of CT Face with contrast was obtained. The study was read as “vessel abnormality right surgical site.” The patient reported discovering that applying manual pressure inferior to surgical site alleviated her pulsatile tinnitus. Upon physical examination, the patient had mild asymmetry of bilateral pre-auricular edema, with right larger than left, without overlying erythema, ecchymosis, nor calor. The right pre-auricular region was exquisitely tender, though exam was negative for pulsatile mass, fluctuance, nor crepitus on palpation. Furthermore, the exam was significant for a loud bruit on auscultation of the right pre-auricular region, using a stethoscope. The bruit was heard loudest over the posterior puncture wound, where the arthroscopic cannula had been blindly inserted, at the posterior aspect of the surgical site (Figure 1). This was the location of the previous glenoid fossa-portal through which the 1.9 mm arthroscope was utilized within a 2.0 mm cannula. A single 5-0 fast gut suture was intact at the posterior fossa-portal puncture site; suture was present but not intact at the anterior operative-portal puncture site, where a 2.0 mm working cannula had been utilized intra-operatively. The bilateral external auditory canals were clear with tympanic membranes intact. The range of motion was >30 mm with guarding, and there was no significant deviation on opening. The remainder of the physical examination was unremarkable.
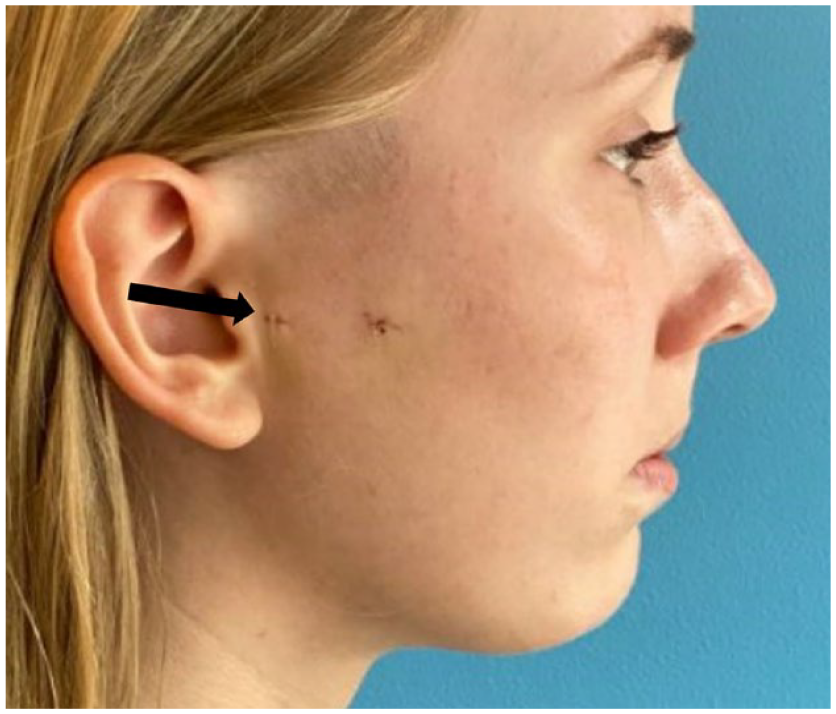
Post-operative day 8, bruit best auscultated over trocar puncture site for arthroscopic cannula (black arrow).
A CT Face with contrast obtained at an outside hospital was uploaded to system the following day. It significant for contrast-enhancement of right superficial temporal vessels with an aberrant vessel coursing lateral to the right TMJ capsule, to the subcuticular skin layer of the right pre-auricular region. The vessel traced proximally from the posterior aspect of the mandibular condyle and laterally to the soft tissue overlying the temporomandibular joint. The CT was self-read as a suspected arteriovenous fistula of the superficial temporal vessels versus deep auricular vessels. An informal Neuroradiology consultation for imaging interpretation confirmed our self-read of AVF on CT. Consultation request was made to Interventional Radiology (IR), requesting evaluation and management of suspected TAVF. During consultation with IR, definitive treatment of the AVF via endovascular embolization was offered. The alternative of non-surgical treatment was offered, with 2 months of observation and repeat imaging, to assess for spontaneous resolution. Risks of endovascular embolization are rare but include: infection, hemorrhage, vessel injury, Onyx embolus migration, vision loss if an ophthalmic artery collateral is involved, cranial nerve or other new neurologic deficit, other non-target embolization or catheter-related thrombus formation that can result in stroke, kidney injury, and allergic reaction. The patient elected for a diagnostic angiogram and consented for possible embolic maneuvers by Interventional Neuroradiology, in hopes of resolving the pulsatile tinnitus.
Procedure Details:
The right common femoral artery was accessed using a micropuncture kit. A 6 Fr Pinnacle sheath was placed over a 3J wire, flushed, and connected to a regulated pressurized heparinized saline infusion. A 5 Fr Envoy MPD catheter was introduced into the descending thoracic aorta over the 3J wire, double flushed, and connected to a heparinized saline flush. The right common carotid artery was then selectively catheterized using the MPD catheter and a Terumo guide wire. Digital subtraction angiography was performed which showed AV shunting from the right superficial temporal artery to the right retromandibular vein (Figure 2). The right external carotid artery was then selectively catheterized and additional digital subtraction angiography was performed (Figure 3). A decision was made to embolize the fistula with both a Concerto coil and Onyx-34, using the coil as a scaffolding to prevent Onyx migration into the venous system. An Echelon 10 microcatheter and a Synchro 2 microwire were advanced into the MPD. Using roadmap guidance, the Echelon 10 was navigated into the superficial temporal artery at the site of the fistula. Digital subtraction angiography was performed. A Concerto coil was carefully deployed partially in the retromandibular vein. The microcatheter was then withdrawn into the superficial temporal artery, where the remainder of the coil was deployed (Figure 4). The Echelon 10 dead space was flushed with DMSO. Onyx-34 was then slowly injected using a blank mask to monitor reflux. In total, 0.3 mL Onyx-34 was set within the coil as a scaffold over 5 minutes. Final digital subtraction angiography was performed which showed there was good Onyx placement within the coil at the site of fistula. There was no evidence of residual AV shunting from the right superficial temporal artery to the right retromandibular vein (Figure 5). The procedure was concluded, patient was admitted for overnight observation. Course complicated by a right groin hematoma, which resolved with conservative measures. After one yar of follow up, there has been no further complications, nor recurrence of the AVF. The patient’s initial temporomandibular joint arthropathy remains asymptomatic and well-managed medically with existing anti-rheumatic medication and non-surgical treatment strategies.
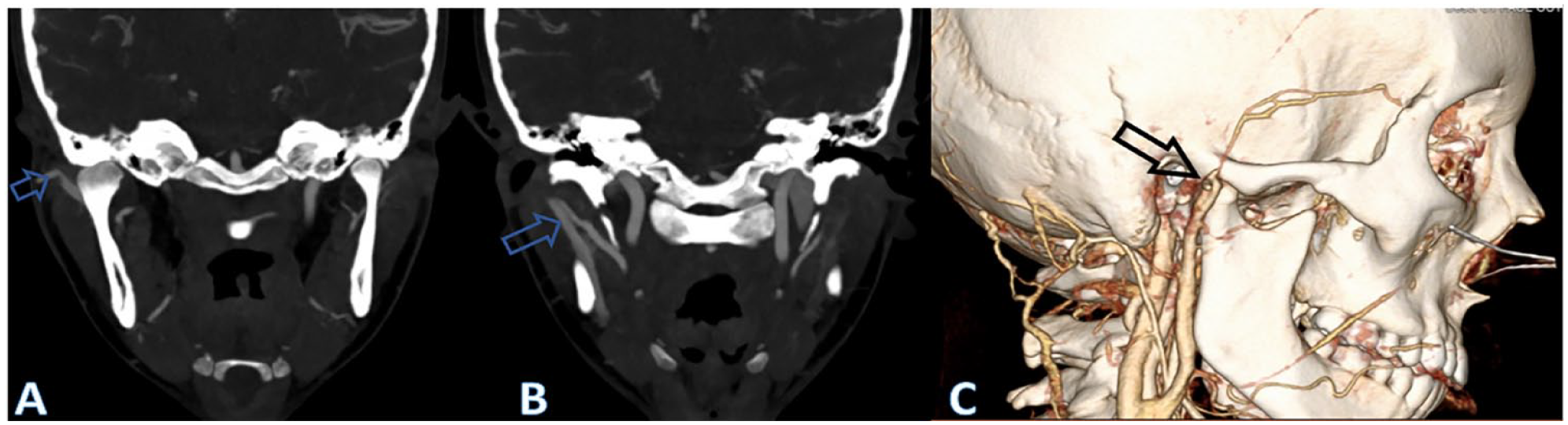
Asymmetric density consistent comparing the right and left retromandibular veins consistent with arteriovenous shunting to the right retromandibular vein (A and B). Three-dimensional reconstruction showing relationship of craniofacial anatomy (C).
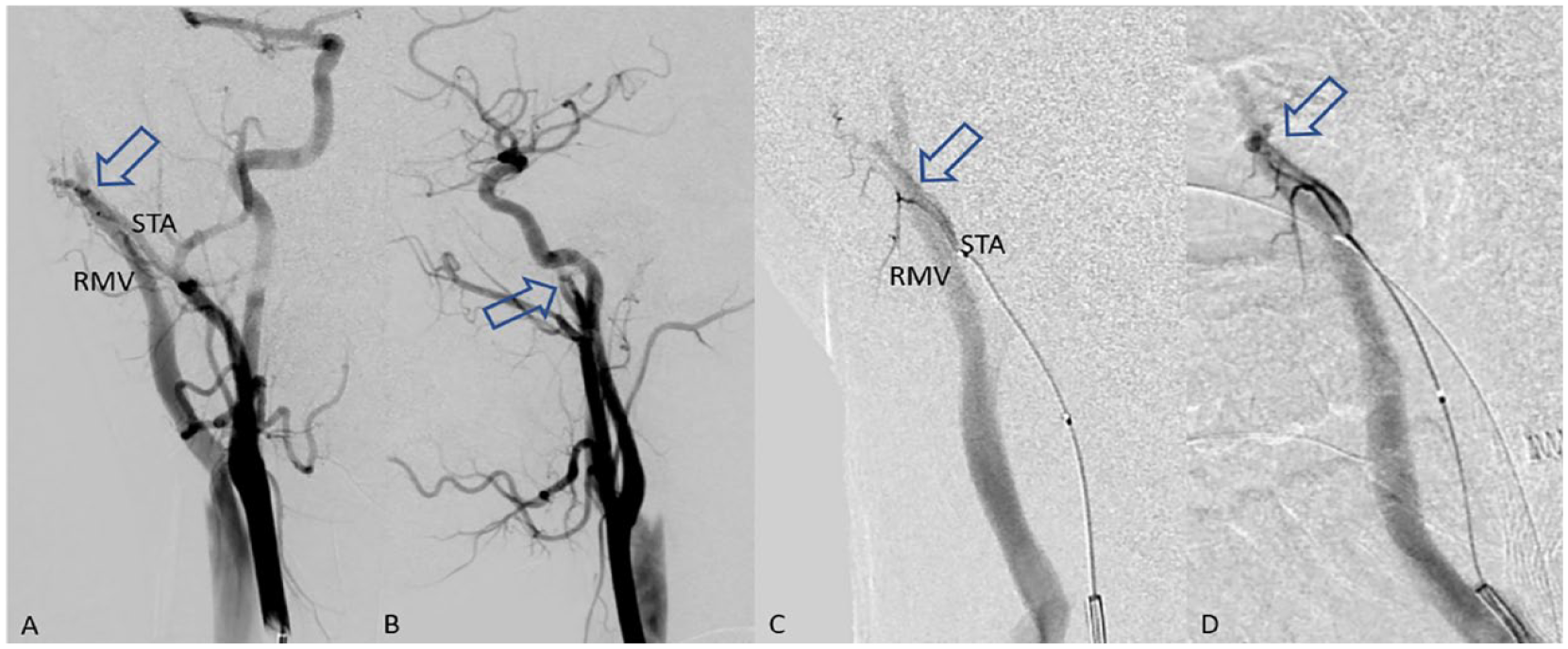
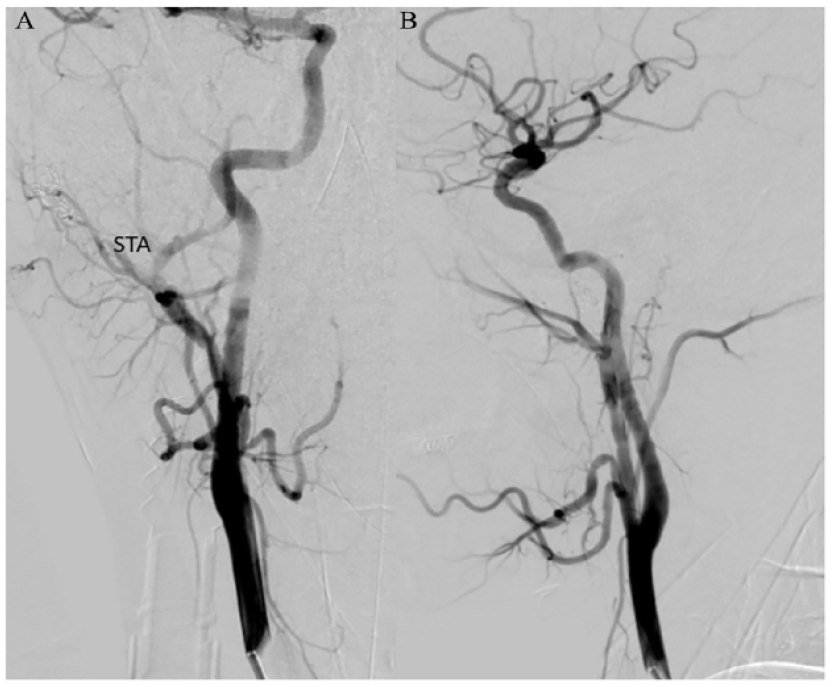
Right common carotid digital subtraction angiography showed AV shunting from the right superficial temporal artery to the right retromandibular vein (arrows at the shunt). Anteroposterior (A) and lateral (B) projections. Right superficial temporal digital subtraction angiography showed AV shunting from the right superficial temporal artery to the right retromandibular vein. Anteroposterior (C) and lateral (D) projections.
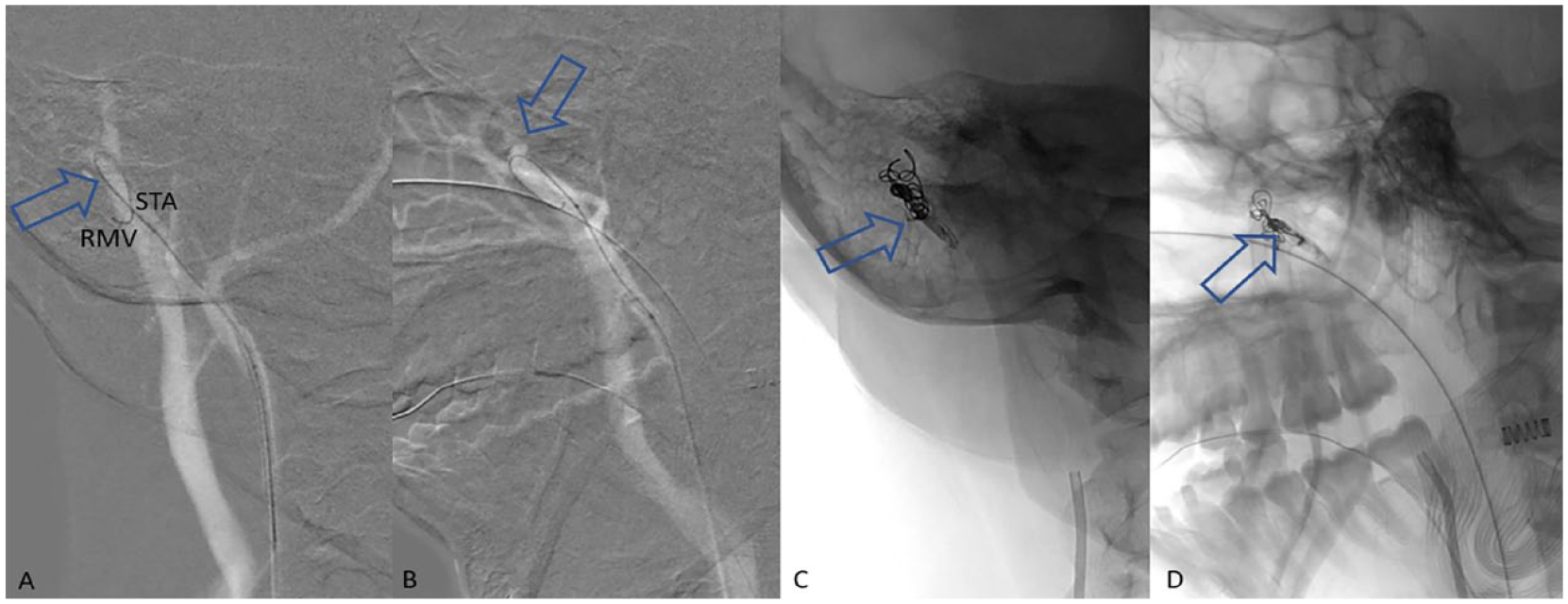
A microcatheter was easily navigated from the right superficial temporal artery into the right retromandibular vein. Anteroposterior (A) and lateral (B) projections. Then, a single coil was carefully deployed partially in the retromandibular vein and partially in the superficial temporal artery to serve as a scaffolding for Onyx. Onyx was injected on the scaffolding, preventing it from migrating into the venous system. Anteroposterior (C) and lateral (D) projections.
After successful embolization, right common carotid digital subtraction angiography showed no residual AV shunting from the right superficial temporal artery to the right retromandibular vein. Anteroposterior and lateral projections seen in figures (A) and (B), respectively.
Discussion
TMJ Arthroscopy is a minimally invasive procedure that involves blind puncture of sharp trocars into the pre-auricular region, to establish arthroscopic and operative portals within the superior joint space of the TMJ 6 . While the development of a traumatic arteriovenous fistula (AVF) is an exceptionally rare complication, it is a complication of TMJ arthroscopy that was successful treated with a minimally-invasive endovascular intervention. There are fewer than 10 published case reports of AVF formation after TMJ arthroscopies, the majority of which were treated with open surgery.3,4,6-8
Patients who develop traumatic AVFs as a rare and early complication of minimally invasive maxillofacial surgery can be managed with vascular interventions via open surgical or endovascular approaches.1,2,9-11 For this type of maxillofacial AVF, endovascular approaches are preferred given low procedural risk.12,13 In this patient’s case, given this complication of a traumatic AVF developed a minimally-invasive endoscopic TMJ surgery, pursuing open surgery for wound exploration and possible AVF ligation of the right pre-auricular region was considered to be a less ideal management option. We report a case of a traumatic AVF successfully treated with minimally invasive endovascular interventions. Traumatic AVFs may or may not present with symptoms. Symptoms vary based on size of vascular lesion, involved vessels, proximity to the middle ear ossicles, and depth relative to superficial skin. The most common symptoms of traumatic AVF include: tenderness to palpation, pulsatile tinnitus, and distortion of superficial skin with or without visualization of distended veins. In this case, the patient presented with exquisite tenderness to palpation and positive findings of an obvious bruit on auscultation. However, venous distension or gross facial edema were no present.
Establishing an accurate diagnosis is the first step in management, accomplished by: obtaining a thorough history of presenting illness; meticulous physical examination that includes auscultation of the area; advanced imaging, and consultation to colleagues from Interventional Neuroradiology or Vascular Surgery. In patients presenting with the aforementioned common symptoms, a history of recent blunt facial trauma or head and neck surgery should raise suspicions for the presence of a traumatic AVF. Upon initial review of outside hospital imaging, we suspected that the patient’s post-operative course had been complicated by AVF formation in the right pre-auricular region. Given the absence of a vascular outpouching or obvious vessel enlargement, a pseudoaneurysm was determined to be less likely. Of note, our initial preference was to obtain advanced imaging for better characterization of circulatory structures, such as a CT-angiogram (CTA). A CTA of the head and neck would allow for a more detailed characterization of suspected traumatic vascular lesion, suspected to be of iatrogenic etiology, due to post-operative onset and localize to the surgical site.
Indications for treatment include: bothersome symptoms and patient preference for treatment. Other indications (not present in this case) include: cerebral venous reflux with intracerebral hemorrhage risk, heart failure, or other cardiovascular risks that may be present with a large vascular shunt. Typically, medical management of a traumatic AVF involves symptom monitoring and repeat imaging. If surgical treatment via endovascular surgical intervention is deferred after initial evaluation, patient symptoms should be followed closely and serial imaging studies are recommended to rule out fistula progression. Special considerations and indications for treatment of a traumatic AVF include patient-specific symptoms such as onset of significant pain, development of pulsatile tinnitus, or other bothersome symptoms that interfere with daily living. There is a slightly elevated procedural risk of unplanned embolic event, compared to embolization of the knee but embolization of a pre-auricular AVF is still considered a relatively low risk procedure. This slightly increased risk of unplanned embolic event is due to proximity to the intra-cranial vasculature and great vessels of the neck. 10 The recurrence rate of traumatic AVFs treated with endovascular embolization is not known. For recurrence, a similar trans-arterial or trans-venous embolization could be performed. Other treatment options include: open surgery for wound exploration and possible fistulectomy with vessel ligation, or radiosurgery, to treat dural AVF and cerebral AVMs.
Post-operatively, patients are kept with the head of bed flat for 3 hours to prevent flexion at the hip, neuro checks and pulse checks with close monitoring for 1 night post-operatively. In as little as 3 hours post-operatively, the patients are allowed stand and walk as tolerated, although no vigorous exercise for 1 week. Submersion of groin in water is deferred for 24 hours, post-operatively. In our case, the embolization was complicated by a groin hematoma that self-resolved over a week. Given the commonality of groin hematomas following endovascular intervention, the Interventional Radiology team deferred further work up of a unifying vasculopathy as the cause of both the AVF and groin hematoma.
Conclusion
Our case presented above illustrates the successful identification and endovascular treatment of an infrequent complication of iatrogenic traumatic AVF formation, following arthroscopic surgery of the TMJ. A multidisciplinary approach to diagnosis and treatment of the complication was utilized to achieve endovascular embolization and complete resolution of symptoms.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The Massachusetts General Hospital IRB protocol number is 2022P000762.