
Abstract
Purpose:
Present a novel technique for fabrication of nasoalveolar molding (NAM) appliances for neonates with cleft lip and palate (CLP) using magnetic resonance imaging (MRI).
Study design:
Proof-of-concept study.
Setting/Participants:
One patient with unilateral CLP was recruited for participation in this study at our institution.
Interventions:
This study employed 2 different methods for creating a NAM appliance, which is used in patients with CLP to improve anatomic positioning of the orofacial cleft in preparation for primary cheiloplasty. The patient underwent intraoral impression for traditional fabrication of a NAM appliance (PMMA-NAM) and also MRI of the face for digital fabrication of a NAM appliance (CAD-NAM). The 2 appliances were then compared using landmarks for measurements.
Primary Outcome:
Landmark measurements on NAM appliances; Clinical interchangeability of NAM appliances.
Results:
There was a statistically significant difference in the external arch width between the CAD-NAM and the PMMA-NAM. All other NAM measurements were statistically similar. Additionally, there was clinical success in the interchangeable fit of both appliances on both models.
Conclusions:
This technique could potentially eliminate the need for creation of an intraoral impression, as well as the adverse events associated with this, in the fabrication of NAM appliances. Larger studies are necessary to further define the efficacy of this novel approach and generalizability to other patients with CLP.
Keywords
Introduction
In the past 5 years, literature has become available which explores the idea of using computer-aided-design/computer-aided-manufacturing (CAD/CAM) and three-dimensional (3D) printing technology for the fabrication of pre-surgical infant orthopedic appliances for patients with cleft lip and palate (CLP). Pre-surgical infant orthopedics (PSIO) were introduced as early as the 1950s with the primary objective of repositioning the nasolabial and maxillary segments closer together to reduce the severity of the cleft in preparation for primary cheiloplasty.1,2 Other objectives include facilitating feeding, improving maxillary growth and the projection of the nasal tip, and reducing nasal deformity.2,3 PSIO appliances have since been modified and reconstructed to improve esthetic and functional results for patients with CLP. 4 McNeil is credited with describing the first PSIO appliance, which consisted of an acrylic molding plate that could be selectively modified to re-approximate the alveolar segments and narrow the cleft gap. 1 Over a decade later, Georgiade and Latham designed the Latham Appliance, a pin-retained active appliance used to approximate the alveolar segments. 5 This appliance is controversial due to the requirement of general anesthesia to place it. 5 Almost 20 years later, Grayson et al developed the nasoalveolar molding (NAM) appliance, which imitated McNeil’s device, but added a nasal stent to address concerns with nasal deformities. 6 Drawbacks of these PSIO appliances include difficulty in obtaining an intraoral impression in an infant, as well as the specialized training required by the provider to construct and apply the devices. Qualified providers are generally located in large metropolitan areas and academic centers, leaving many remote and rural areas of the country and world without access to PSIO devices.
The field of dentistry is moving to a more digital experience for patients as dental professionals expand on using digital imaging technology, CAD/CAM, and 3D printing technologies. Currently, efforts are focused on utilization of these advancements in the field of general dentistry, prosthodontics, and orthodontics to implement same-day dentistry for adult and adolescent patients. With advances in computer-aided design (CAD), it is worth exploring whether this technology could be used to create a safer and more widely available pre-surgical molding experience for patients born with CLP. Contributions from Ghivizzani, 2 Kasper et al, 3 and El-Ashmawi et al 7 have shown that a NAM appliance can be 3D printed with great accuracy from a scanned stone model obtained from a traditional intraoral impression. 3D printed materials can also be constructed using computed tomography (CT) or magnetic resonance imaging (MRI) data; this has been done for many other craniofacial surgeries. However, the use of image-guided, 3D-printed materials has not been previously explored in PSIO device fabrication. The purpose of our study is to eliminate the intraoral impression step of device fabrication and instead use images obtained from an MRI face to create 3D-printed devices. Thus, we hope to completely digitize the experience of fabricating a PSIO appliance.
We hypothesize that a NAM appliance can be digitally rendered from an MRI face scan, and that digital design can be used for fabrication of a functional NAM appliance.
Methods
This study was approved by the Committee for the Protection of Human Subjects at our institution (HSC-DB-20-0268). Inclusion criteria for this study was for newborns with cleft lip with or without cleft palate who were born at our institution with plans to undergo treatment with our cleft palate-craniofacial team. Infants that could not tolerate an intraoral appliance were to be excluded. The legal guardian of the infant was approached to participate in the research study.
Ultimately, one patient with a unilateral CLP was recruited for this proof-of-concept study. This patient was seen by the team at our institution. After obtaining informed consent, the 36-day old infant was sent for a non-sedated MRI of the face. During the MRI scan, a feed-and-swaddle method was utilized to induce sleep and obtain imaging. 8 The patient fasted for 4 hours prior to the scan and then was fed via a nasogastric feeding tube 10 minutes prior to entering the MRI suite. The patient was tightly swaddled with all appropriate monitoring devices and ear protection in place. An acrylic splint and subsequently a metal-free pacifier were used during the scan to promote sleep, separate the tongue from the hard palate, and make the soft tissue structures more distinguishable on the MRI. The pacifier was a commercially available brand provided by our children’s hospital, and the acrylic splint was a 3D-printed, non-commercial flat plate intended to separate the tongue from the palate.
The face MRI was obtained with an Ingenia Elition 3.0T MRI scanner (Philips, Cambridge, Massachusetts) using the following parameters: (1) 2 sets of isotropic 3D T2-weighted images (T2WI) acquired in the sagittal plane with a repetition time (TR) of 2500 milliseconds (ms), echo time (TE) of 255 ms, slice thickness 1, slice spacing 1, field-of-view (FOV) of 24 centimeters (cm), flip angle of 90° and (2) 2D axial T1-weighted images (T1WI) with TR of 725 ms, TE of 10 ms, slice thickness 2, slice spacing 2.2, FOV of 12 cm, and flip angle of 90°.
Two sets of T2WI sequences, one with an oral acrylic splint and one with a pacifier, were acquired. The acrylic splint caused the patient to move and reject the object from their mouth, prompting the team to reinitiate the T2WI sequence. The initial incomplete T2WI sequence obtained using the acrylic splint was inadequate and had no role in the remainder of the study. With the pacifier, the infant remained still. Thus, the image quality for the T2WI sequence obtained using the pacifier was adequate and diagnostic on the axial, coronal, and sagittal planes with no motion artifact. Acquisition time for each of the 2 sets of T2WI sequences was 3 minutes. During the T1WI acquisition, the infant began to move, and only axial 2D sequences with mild motion artifact could be acquired; these were ultimately adequate. Acquisition time for the T1WI was 4 minutes. Total scan time was approximately 25 minutes.
The MRI Digital Imaging and Communications in Medicine (DICOM) data was converted to a stereolithographic (STL) format using 3D Slicer, an open source image computing platform. 9 Once uploaded into 3D Slicer, the MRI images could be viewed and manipulated to build a 3D model of the arch. The alveolar segment was selected from each slice using a paint feature in the software, and a 3D model was digitally created within 3D Slicer from these selections. It was determined that the T1WI series was superior to the T2WI series for distinguishing between soft tissues. The computer file containing the T1WI-based digital 3D model was saved in STL format and transferred to 3Shape Appliance Designer (3Shape; Copenhagen, Denmark), a CAD software, where a NAM appliance could be digitally fabricated (CAD-NAM) using the model. Both the model (CAD-MODEL) and the digitally designed CAD-NAM appliance were 3D printed using a Formlabs Form 2 SLA 3D Printer (Formlabs, Inc.; Somerville, Massachusetts). The CAD-NAM was printed using Formlabs Dental LT Clear Resin (Formlabs, Inc.; Somerville, Massachusetts) with 2 millimeter (mm) uniform thickness, and the CAD-MODEL was printed in Grey V4 Resin (Formlabs, Inc.; Somerville, Massachusetts).
Two days after the MRI, the same patient was seen at our institution for collection of an intraoral impression with Aluwax (Aluwax Dental Products Company; Allendale, Michigan) heated in hot water and creation of a custom unilateral cleft-sized impression tray made from polymethyl methacrylate (PMMA) hard acrylic (Dentsply; Milford, Delaware). The impression was taken in a hospital setting with appropriate monitors and rescue equipment available with the patient in the supine position. The impression was poured in yellow stone and a traditionally fabricated Grayson NAM appliance was made using Caulk Orthodontic Resin PMMA hard acrylic (Dentsply; Milford, Delaware) and GC COE-SOFT soft acrylic (GC America; Alsip, Illinois) at an estimated 2 mm thickness. 4 This appliance (PMMA-NAM) and model (IMP-MODEL) were considered the gold standard for this study to which all measurements from the CAD-NAM and CAD-MODEL were compared.
Specific landmarks were chosen to compare the IMP-MODEL to the CAD-MODEL and the PMMA-NAM to the CAD-NAM. Using these points, measurements were taken by a single investigator on 4 separate days. Each model and appliance were measured at separate times of the day and recorded on a blank document, and the resulting data were sent to a second member of the team for statistical analysis. All measurements were made using a caliper and recorded to the nearest tenth of a millimeter. For the models, the following measurements were compared: arch length, external arch width, internal arch width, arch circumference, and cleft space. For the appliances, the following measurements were compared: length, external width, and internal width. A Student’s t-test was performed with P value <.05 considered statistically significant.
Results
Clinical analysis yielded successful results, defined by confirming adequate fit of the PMMA-NAM on the CAD-MODEL and adequate fit of the CAD-NAM on the IMP-MODEL (Figure 1). The CAD-NAM required no adjustments to the edges and printed with smooth, rounded internal surfaces. The external surface was removed from the support structures and polished using a diamond lab bur. The PMMA-NAM required some adjustments using the diamond lab bur to create smooth rounded edges and remove irregularities in the hard acrylic.
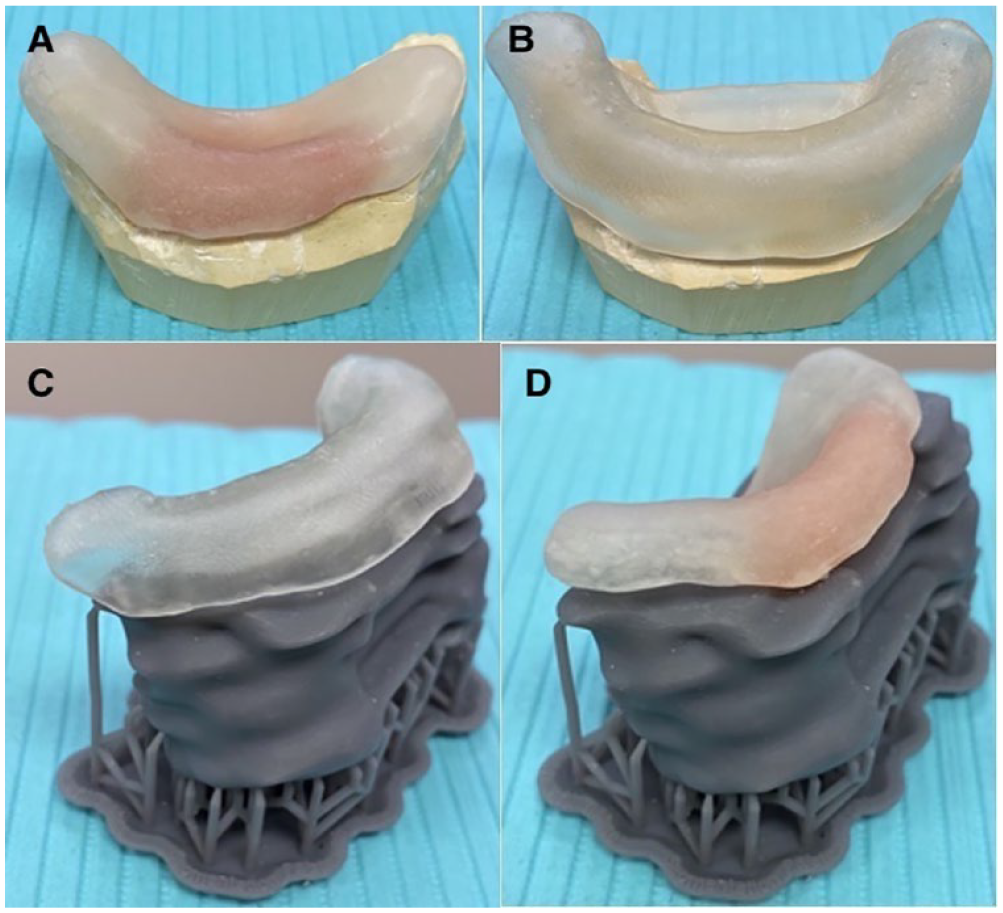
(A) PMMA-NAM fit on IMP-MODEL, (B) CAD-NAM fit on IMP-MODEL, (C) CAD-NAM fit on CAD-MODEL immediately following 3D printing, and (D) PMMA-NAM fit on CAD-MODEL immediately following 3D printing.
Statistical analysis showed some variation between the 2 methods. When comparing the IMP-MODEL to the CAD-MODEL (Table 1), there was a statistical difference in the external arch width by a mean difference of +2.25 mm (P = .0001). There was also a significant difference in the arch circumference by a mean difference of +1.625 mm (P = .0049). Additionally, the cleft space width was considered statistically different with a mean difference of −0.675 mm (P = .0005). There were no significant differences in the arch length or the internal arch width (P > .05).
Statistical Analysis Comparing IMP-MODEL to CAD-MODEL (All Measurements in Millimeters).
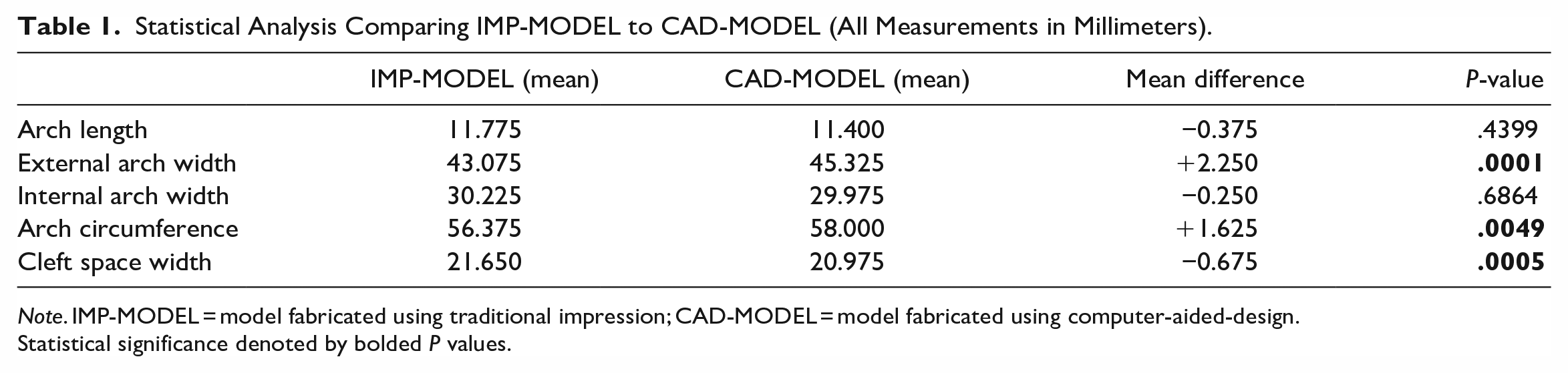
Note. IMP-MODEL = model fabricated using traditional impression; CAD-MODEL = model fabricated using computer-aided-design.
Statistical significance denoted by bolded P values.
When comparing the PMMA-NAM to the CAD-NAM (Table 2), statistical analysis showed a significant difference in the external arch width with a mean difference of +1.15 mm (P = .0031). There were no significant differences in the internal arch width or the arch length (P > .05).
Statistical Analysis Comparing PMMA-NAM to CAD-NAM (All Measurements in Millimeters).
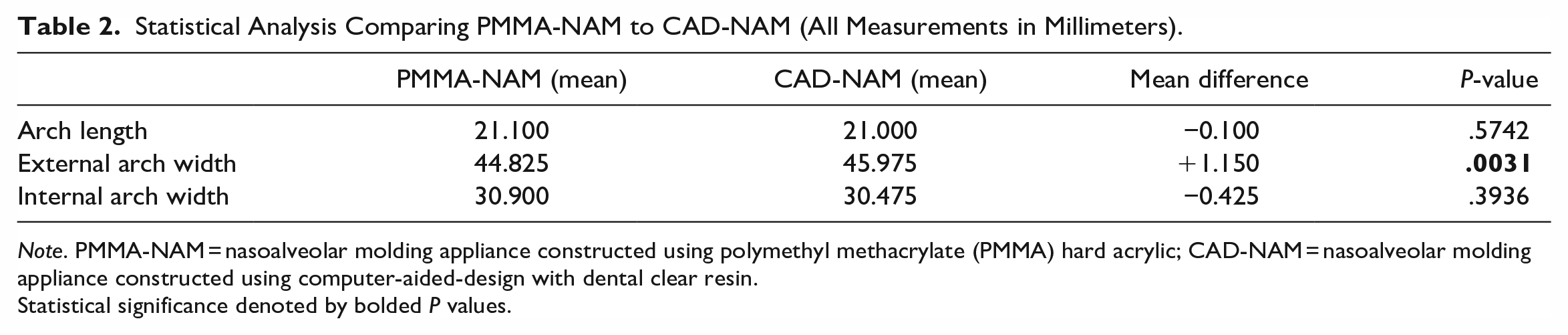
Note. PMMA-NAM = nasoalveolar molding appliance constructed using polymethyl methacrylate (PMMA) hard acrylic; CAD-NAM = nasoalveolar molding appliance constructed using computer-aided-design with dental clear resin.
Statistical significance denoted by bolded P values.
Discussion
This proof-of-concept study demonstrates the feasibility of fabricating functional 3D-printed NAM devices using images obtained by MRI. In current clinical practice, there are many barriers to providing effective PSIO therapy for infants with CLP. For many providers, it has not been feasible to treat children with CLP using PSIO devices, such as NAM, due to lack of training, increased chair and lab time, fear of adverse events during intraoral impression collection, and lack of appropriate materials and resources. Nonetheless, the American Board of Pediatric Dentistry College of Diplomats recommended in their 2012 conference paper that intraoral impressions for neonates should be taken in a clinical setting where infant airway emergencies can be managed. 6 This type of environment is not always accessible to providers, especially those in rural areas. Consequently, providers who lack the experience or resources to manage airway-related emergencies in infants could be less comfortable collecting intraoral impressions needed for traditional fabrication of NAM appliances. Image-based anatomical acquisition, as we have shown here with MRI, may be useful for creating these devices in remote clinical practices, thus allowing more children to benefit from this care.
Patients born with CLP face a lifetime of surgeries and medical interventions. 10 Minimizing exposure to general anesthesia should be a priority when exploring new methods of treatment for this patient population. Using the feed-and-swaddle protocol, the radiology team in this study was able to obtain adequate MRI imaging without using medically-induced sedation or general anesthesia. An acrylic splint was initially fabricated to promote separation of the palate from the tongue; however, the infant rejected this device, which prompted them to move. Subsequently, the pacifier was better tolerated by the patient and provided sufficient separation of the soft tissues without causing artifact on the images. Larger studies are needed to confirm the efficacy of the feed-and-swaddle technique during acquisition of MRIs for 3D printing of NAM appliances.
Both CT and MRI have been used by other authors to create 3D models of patients with cleft palate. 11 CT scans can be acquired with very thin images, ranging from 0.15 to 0.5 mm, but would unnecessarily expose the infant to ionizing radiation. 11 The American Academy of Pediatric Dentistry recommends that practitioners follow the “As little as reasonably achievable” (ALARA) principle to minimize a patient’s exposure to radiation. 12 Our study proposes the use of MRI, which causes no radiation exposure, rather than CT in the creation of a model and design of a properly fitting NAM appliance. Furthermore, MRI is known to be superior to CT in terms of differentiating soft tissue structures, which may be more useful for fabricating NAM appliances. Future studies should compare the clinical efficacy of 3D-printed NAM devices based on MRI images to those obtained from CT.
3D MRI acquisition is preferable for reconstruction of images needed for 3D printing. However, the image acquisition time for MRI is high compared to other imaging modalities, like CT. 13 The initial acquisitions of our patient were done using 3D T2WI. After these acquisitions, as the patient was becoming less cooperative, it was decided to acquire the T1WI using a 2D technique to reduce imaging time. In retrospect, we found that the 2D T1-weighted images, in spite of not being isotropic, proved more useful for identifying soft tissue structures. Arens et al described similar findings when obtaining MRI imaging of the upper airway. 14 In the future, our group intends to start the image acquisition with 3D T1WI to optimize imaging quality, thus combining the tissue resolution provided by the T1WI and the spatial resolution provided by isotropic 3D acquisition.
Although there were several measurements that were considered statistically different, it is important to take note of the clinical significance and the lack of a true “perfect” model in this study. The absolute differences in all of these measurements remained very small. Most importantly, the 2 NAM appliances were shown to be interchangeable on the 2 models, representing a clinically acceptable result. In future studies, a patient try-in would yield more useful information, as this is the only “model” which can truly be considered the gold standard. True adequate fit can then be measured by the number of required adjustments and reports of irritation or ulceration on the soft tissue, as demonstrated in the study by El-Ashmawi et al. 7
Although the difference in external arch width in the NAM group was considered statistically significant, there may have been inaccuracies in the thickness of the appliance. The CAD-NAM was printed with uniform 2 mm thickness throughout, whereas the PMMA-NAM was hand-fabricated and may have had varying levels of thickness throughout. Fortunately, chairside adjustments can easily be made for both appliances, which could have eliminated any minor discrepancies while preserving the integrity of the appliances. There were statistical differences between the IMP-MODEL and the CAD-MODEL for the measurements of external arch width, arch circumference, and cleft space width. While these measurements are worth considering, analysis of the NAM appliance is considered more valuable than analysis of the models as the appliance is ultimately used by the patient. In real-world application, a 3D model generally would not be printed or utilized for analysis because it is an intermediate step in fabrication of the NAM appliance.
One concern for the CAD-NAM appliance is the necessity to add soft acrylic in the cleft space. Once the appliance is printed, there is no indication of where the cleft is or where to add the soft acrylic. This could be addressed by creating small notches in the digitally fabricated NAM appliance to indicate where the cleft space is located. Additionally, with further research and funding, a software designed specifically for this purpose may allow for further customization prior to 3D printing.
This study was limited by the number of participants as it was a proof-of-concept study. Without data from larger, multi-institutional studies, the results observed may not be generalizable to other patient populations. While this proof-of-concept study provides interesting insights into the digital workflow of NAM appliance fabrication using MRI and offers evidence that this technique is worth investigating further, expansion of the study to include additional patients is warranted. In addition, future studies should incorporate more investigators to perform the measurements of the models and appliances rather than a single investigator performing measurements on separate days. Thus, further studies on the efficacy of this approach will be driven by the inclusion of more participants and investigators. In addition, the age of the child in this study at intraoral impression was 38 days postnatal. The Grayson et al method recommends impression and initiation of treatment as soon after birth as possible. 6 Georgiade and Latham also noted the importance of early intervention to avoid maxillary collapse while manipulating the maxillary segments. 5 In future studies of 3D printed NAM appliances, treatment should begin at 1 to 2 weeks postnatal. Lastly, the feed-and-swaddle method utilized to encourage sedation in this study may not be effective for all infants during an MRI.
Conclusions
Using a feed-and-swaddle technique, a non-sedated MRI of the face was feasibly obtained and converted to a digital format to build a 3D-modeled rendering of the alveolar segments in a neonate with CLP. The 3D-modeled rendering of the alveolar segments was then used to digitally design a functional NAM appliance. Larger, multi-institutional studies are necessary to improve accuracy and efficacy of the workflow as well as to increase generalizability of these results.
Footnotes
Acknowledgements
Our group would like to acknowledge Seferino Romo, ARRT MR, MRI Clinical Educator, Memorial Hermann Hospital TMC, for his contribution with the acquisition of the MRI images.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the Committee for the Protection of Human Subjects at UT Health Houston (HSC-DB-20-0268).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.