
Abstract
Introduction
Nasoalveolar molding (NAM) is a well-established pre-operative adjunct for correcting bilateral cleft lip and palate (BCLP) deformity.1,2 NAM involves an orthopedic device with an intra-oral molding plate and an external nasal molding device. NAM has been shown to improve the anatomical alignment of lip, alveolus, palate, and nasal segments.3-17
The changes following NAM have improved short- and long-term outcomes following surgical correction.18-27 NAM narrowing of the cleft enhances the ability of the infant to create a seal during breastfeeding, which may improve early weight gain. 28 Nasopharyngeal, oropharyngeal, and total airway size have also been shown to increase following NAM in patients with BCLP. 29
Regardless of the known benefit in BCLP patients following NAM therapy, there is little understanding of the changes throughout the treatment period. Additionally, there are significant costs associated with travel due to frequent clinical visits during the treatment period. 30 Thus, it is vital to elucidate the rate of change that occur during therapy to determine the ideal treatment duration. The purpose of this study is to utilize three-dimensional (3D) weekly images to assess the progressive changes in lips and nose during NAM therapy in patients with BCLP.
Methods
A retrospective review of pre-NAM and 10 weekly 3D craniofacial images of patients diagnosed with BCLP who underwent NAM therapy was performed following institutional review board approval by the University of Texas Southwestern Medical Center. Medical records were reviewed to collect demographic and operative interventions. Three-dimensional craniofacial images were acquired pre-NAM and each of the 11 weeks during NAM therapy with 3dMD imaging system (3dMD, Atlanta, GA). Virtual 3D-derived models were analyzed using 3dMD Vultus (3dMD, Atlanta, GA).
NAM therapy was started around 20 days after birth, and the appliance was adjusted weekly with an orthodontist in the orthodontic clinic of Children’s Health Children’s Medical Center Dallas. A new appliance with nasal stents was delivered about 6 weeks after the initiation of the treatment. Six measurements were made at each weekly time point for all patients (Figure 1). They included nostril height (base ala to top ala), nostril width (medial ala to lateral ala), lip gap (base prolabium to lateral segment cupid’s peak), columella height (base columella to top columella), prolabium height (base prolabium to base columella), and nasion–prolabium–chin angle. Statistical analysis was performed to calculate totals and averages with standard deviation.
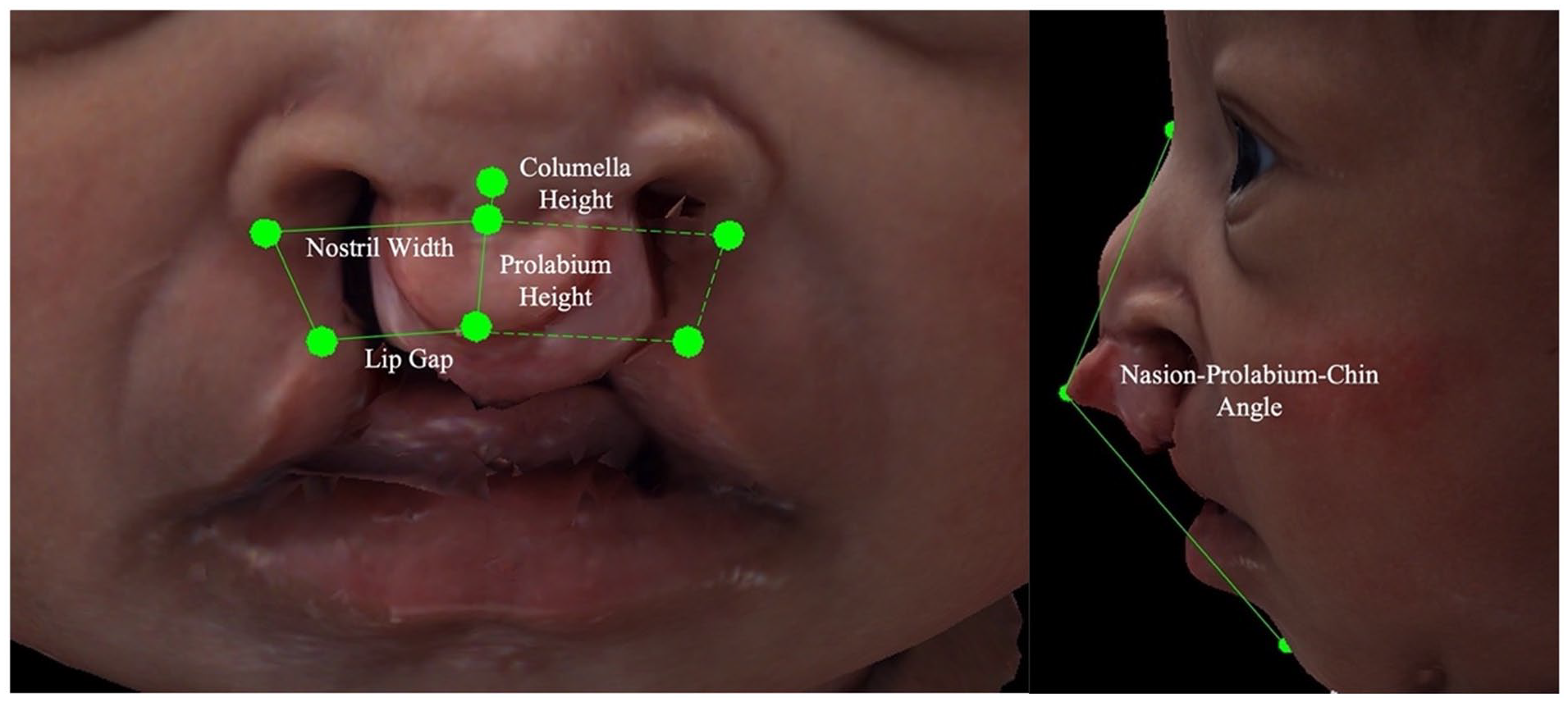
Bilateral cleft lip and palate nasolabial measurements: nostril width, lip gap, columella height, prolabium height, and nasion-prolabium-chin angle.
Results
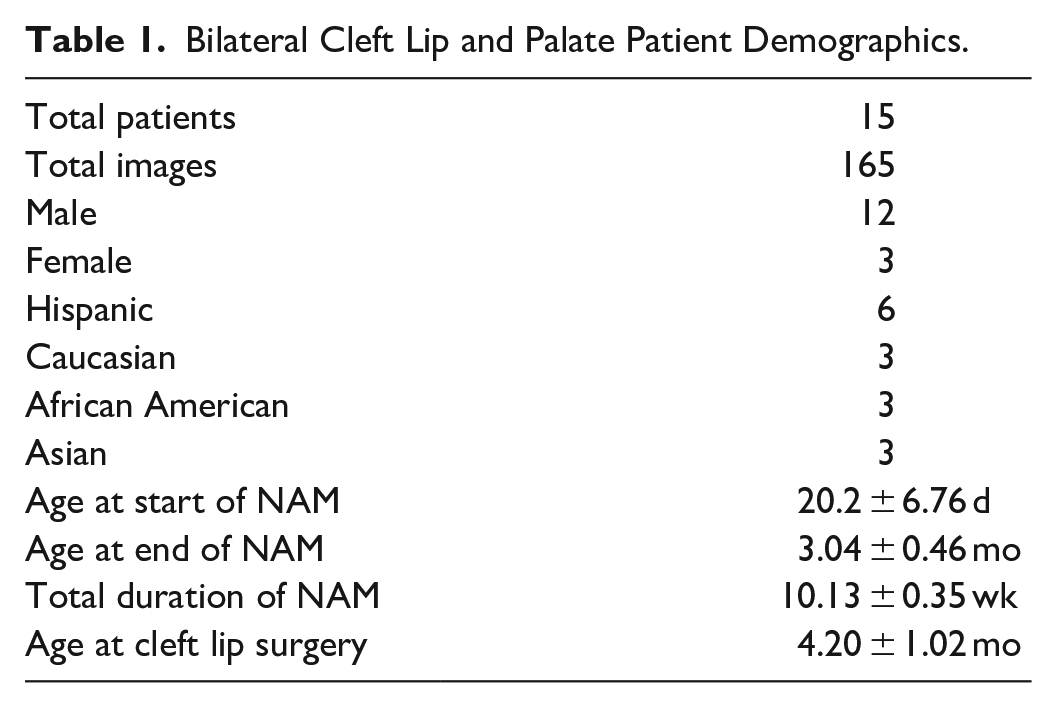
A total of 15 patients who underwent 11 weeks of NAM with 165 images pre-NAM and over 10 weeks following were reviewed (Table 1). The cohort was 80% male and 20% female. The patients were 40% Hispanic, 20% Caucasian, 20% African American, and 20% Asian. The average age at the start of NAM was 20.2 ± 6.76 days. No patients experienced complications while undergoing NAM therapy.
Bilateral Cleft Lip and Palate Patient Demographics.
The nostril height has a positive correlation with R2 equal to .792 (Figure 2 A). The increase in height showed a consistent elevation rate over the time of NAM therapy from 6.16 ± 1.55 mm to 7.38 ± 1.21 mm. Nostril width had a weak negative correlation with R2 equal to .559 (Figure 2 B). The width started at 18.08 ± 2.35 mm pre-NAM and ended therapy at 17.02 ± 2.21 mm. The lip gap had a strong negative correlation of R2 equal to .858 with a decreased lip gap change over time (Figure 2 C). The gap decreased from 17.44 ± 4.09 mm to 13.40 ± 2.82 mm at the end of NAM therapy. Columella height had a strong positive correlation of R2 of .866 (Figure 2 D). The height of the columella increased consistently over time from 1.36 ± 1.11 mm to 2.94 ± 1.24 mm. The prolabium height had a weak positive correlation with R2 equal to .301 (Figure 2 E). The height increased from 5.55 ± 1.88 mm to 7.37 ± 1.51 mm. The angle of the nasion–prolabium–chin positively increased over time with R2 equal to .664 (Figure 2 F). The angle increased from 121.64° ± 10.27° to 133.62° ± 9.22°.
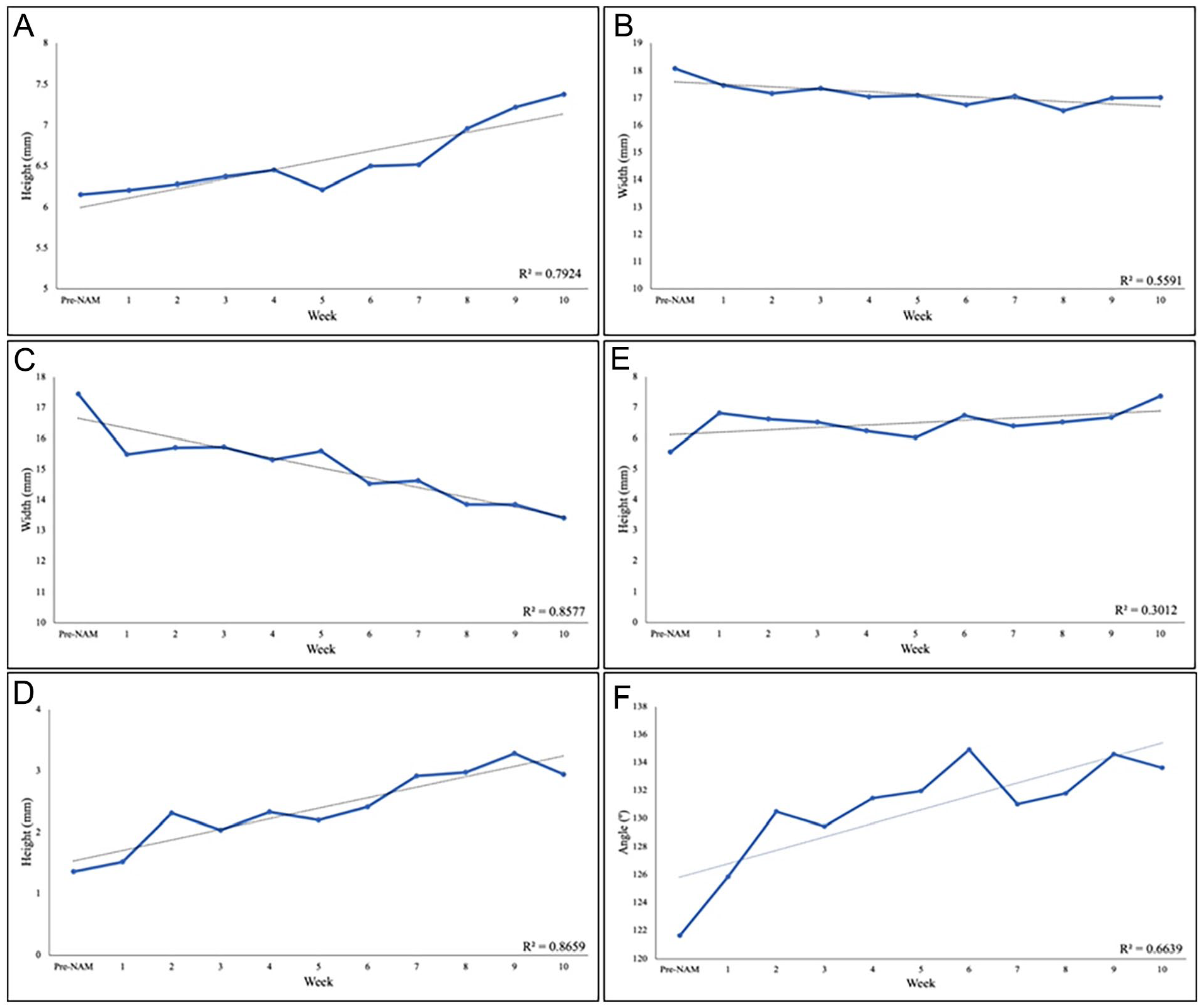
Three-dimensional measurements of bilateral cleft lip and palate patients undergoing nasoalveolar molding. A) Nostril height. B) Nostril width. C) Lip gap. D) Columella height. E) Prolabium height. F) nasion – prolabium – chin angle.
Discussion
NAM includes an intraoral plate to mold the alveolar segments and nasal stent extension for nasal shaping. NAM has been shown to provide a more favorable anatomical alignment for primary cleft lip and nasal repair.3-17 These are potential benefits demonstrated in both the short- and long-term outcomes following surgical correction18-27 The temporal changes throughout the treatment period have yet to be elucidated. An increased length of therapy has an additional cost burden on patient families due to travel for frequent clinical encounters. 30 Our study reports the progressive growth changes that occur across the NAM treatment period in BCLP patients.
NAM has been shown to reduce the cleft gap in BCLP patients.1,4,8-18 The lip gap demonstrated a consistent and linear decrease over the treatment period. This contrasts with our group’s previous findings in unilateral cleft lip and palate (UCLP) patients, where a rapid decrease was observed at the beginning of NAM therapy, followed by a plateau. 3 However, Nazarian Mobin et al showed equivalent improvements in gap width between UCLP and BCLP patients by the end of NAM therapy. 7 A decrease in cleft width has multiple benefits, including a decreased rate of complications and the need for secondary surgeries.31,32 These results indicate that the longer the treatment period, the greater the decrease in cleft lip gap.
The length of the prolabium remained stable across the treatment period, showing little effect of NAM. Meanwhile, the angle of the nasion to the prolabium to the chin angle increased over time, indicating that while the prolabium remained the same height, there was a posterior movement of the prolabium into a more anatomical position. Posterior movement of the prolabium was shown by El-Ashmawi et al, who found a significant increase in nasolabial angle following NAM therapy. 11
The nasal stent extensions in NAM therapy are utilized to increase the nasal protrusion, which is deficient in the BCLP nasal deformity.33,34 The benefits of NAM therapy have been previously shown to increase the height of both the nostrils and columella.1,7,10,11,13-15,22-24 The nostril height was found to have consistently increased change throughout the treatment period. A similar trend was seen with columella height, indicating that both the nostril and columella height consistently increase with increased length of NAM. The nostril width, as expected, had minimal change over time. These findings in the nostril height and width are consistent with our previous NAM findings in UCLP. 3
Our current protocol included 10 weeks of NAM therapy ending around 3 months of age. Patients become more active at this age and develop the motor skills to disrupt the appliance. An additional consideration is the potential for delay in primary surgical repair. The ideal timing of cleft lip repair remains debated, with the most common age range being within 4 to 6 months.35-38 In our cohort, the average age at repair was around 4 months, leaving the potential for lengthening our treatment protocol. The findings of our study would indicate the benefit of increased length of NAM therapy protocol as a plateau has not been reached in the improvement of the lip gap, posterior movement of the prolabium, and nostril and columella height. The current study’s power is limited by the size of the patient cohort. Future studies should include subgroup analysis of treatment lengths and cleft severity to elucidate further which patients may benefit from longer treatment lengths.
Conclusions
The 3D weekly craniofacial images demonstrated a consistent rate of progressive changes in BCLP during NAM therapy. A consistent decrease in lip gap exists while the prolabium remains a consistent length but with progressive correction of the protrusive prolabium with posterior movement. The nostril and columella height consistently increased across the treatment period with little change in nostril width. These findings indicate that an increased treatment period would continue to have consistent change and result in a decreased lip gap with the posterior movement of the prolabium and an increase in the nostril and columella height. The benefits of an increased treatment period with NAM must be weighed against the hindrance of delaying primary surgical repair and the cost burden to patients’ families.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Institutional Review Board approval was not required.
Informed Consent
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of the University of Texas Southwestern Medical Center, with the need for written informed consent waived.