
Abstract
Kinetic impact projectiles (KIPs), also known as non-lethal projectiles, are crowd-control methods considered to be less harmful than traditional ammunition. KIPs have been used worldwide by law enforcement in crowd-control settings, and most recently used during the social justice protests that ensued following the death of George Floyd during the summer of 2020. Possible injuries from KIPs are broad, ranging from minor to severe and life-threatening injuries, and include both blunt and penetrative trauma throughout the body. Past reports on KIP trauma have not included detailed references to the craniofacial region. We present 4 patients who suffered craniofacial trauma secondary to KIP injury with both acute and chronic sequelae. While KIPs are considered non-lethal weapons, this limited series demonstrates the range of severe, and even life-threatening, injuries due to KIPs that craniofacial surgeons may encounter.
Introduction
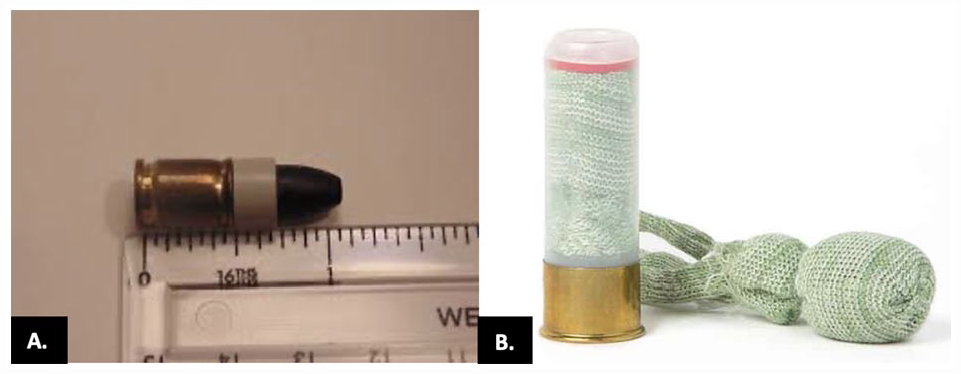
Kinetic impact projectiles (KIPs), also known as non-lethal projectiles, are increasingly being used as crowd-control methods during public protests or situations involving civil disorder. As the name implies, the weapons transfer kinetic energy from a weapon to a person, with the goal of temporarily incapacitating an individual without significant injury or death. 1 Examples of KIPs include rubber bullets, plastic bullets, bean bag rounds, rubber-coated metal bullets, and sponge bullets (Figure 1). Rubber and plastic bullets can be cylindrical or spherical and can be shot as single or grouped projectiles. Bean bag rounds, on the other hand, are cloth bags filled with small metal pellets which expand when fired for a wide surface area of impact. There are several types of launchers available for KIP weapons, but one of the most common is the riot shotgun. These weapons are often 12-gauge shotguns, which can be dual-purposed to switch between traditional ammunition and less-lethal ammunition. 2
Wounding potential of a weapon is partially determined by the efficiency of which its kinetic energy can be transferred to its target. Kinetic energy of a missile is the product of the mass of the projectile multiplied by its velocity squared. Projectile velocity is influenced by the ballistic coefficient, which is the quotient of a bullet’s sectional density (SD) and the form factor for bullet shape (I). The ballistic coefficient essentially describes a projectile’s ability to overcome air resistance; a lower value indicates a greater loss of speed per distance.3,4 External ballistics and ballistics of wounding are complex phenomena that require additional considerations including, but not limited to, drag, energy release rate, retardation effects, and bullet tumbling. KIPs are designed so that low amounts of kinetic energy impact the victim due to a low ballistic coefficient. However, the weapon’s properties can cause unstable flight, leading to inaccuracy and impact on unintended targets or anatomical parts. 1 A comparison of kinetic energy between common weapons can be seen in Table 1.
Approximate Velocity and Kinetic Energy of Common Projectile Weapons.
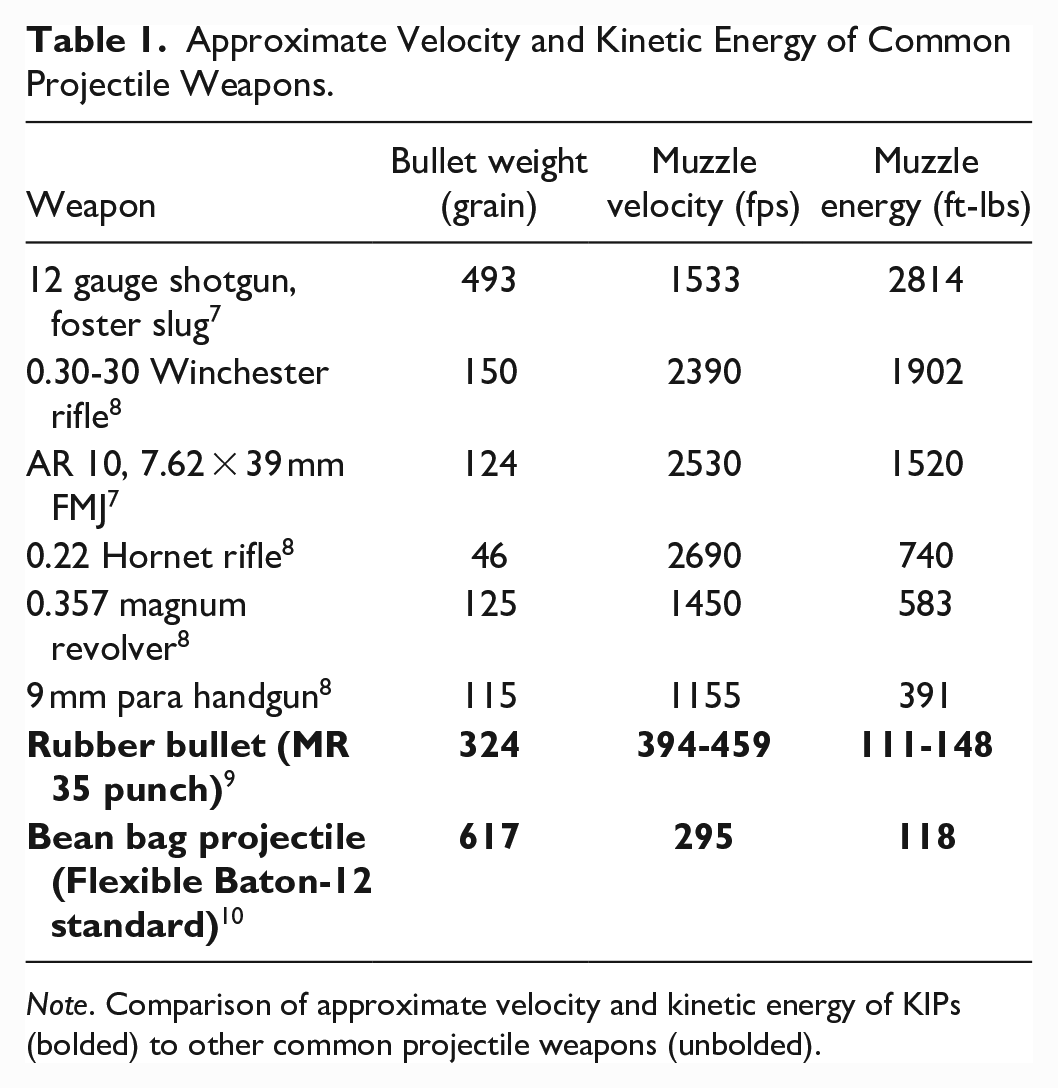
Note. Comparison of approximate velocity and kinetic energy of KIPs (bolded) to other common projectile weapons (unbolded).
While KIPs have a significantly lower muzzle velocity and thereby may be expected to decrease risk of serious injury, recent reports of injuries from KIPs include neurosurgical emergencies, blunt trauma to the chest, penetrating ocular trauma, and testicular rupture.11-14 However, there is a paucity of reports detailing craniofacial-specific injuries due to KIPs. The aim of this study is to report the acute and chronic impact of KIPs in the context of craniofacial trauma during the 2020 social justice protests in Austin, TX. The authors hypothesize that while KIP are considered less lethal weapons, they can cause severe craniofacial trauma.
Methods
The authors conducted a retrospective review of craniofacial injuries caused by non-lethal projectiles during the social justice protest in the summer of 2020 at a level 1 trauma center in Austin, TX. IRB approval was obtained, and due to the public nature of these cases, the research team worked diligently hospital legal team to obtain participant consent. Data was reviewed from the medical record. Additionally, one patient requested an interview with our research team almost 3-years following the incident to further explain the long-term sequelae he experienced; qualitative data from this interview is included.
Results
Five patients were identified who experienced craniofacial trauma due to KIPs. Four of these patients provided consent for publication in this case series. These patients ranged in age from 20 to 29 years, 3 were male, and one patient was female. KIP weapons used included 2 rubber bullets and 2 beanbag projectiles. Acute injuries included a comminuted NOE fracture, mandibular parasymphyseal and body fracture, cheek laceration with facial nerve injury, and subarachnoid and subdural hemorrhage. Chronic sequelae included vision loss, post-concussive symptoms, mandibular osteomyelitis and hardware failure, and post-traumatic stress disorder. Detailed clinical reports are described below.
Clinical Reports
Patient #1
A 25-year-old male presented to the emergency department after being struck by a rubber bullet causing a 6 cm infraorbital laceration extending to the left medial canthus with periorbital ecchymosis and conjunctival injection (Figure 2). The patient was also noted to have asymmetric pupils with the left pupil being 5 to 6 mm and non-reactive. Visual acuity was subjectively unchanged with patient reporting baseline blurriness in vision prior to injury. Maxillofacial CT imaging showed a comminuted left nasoorbitoethmoid (NOE) fracture (Figure 3).

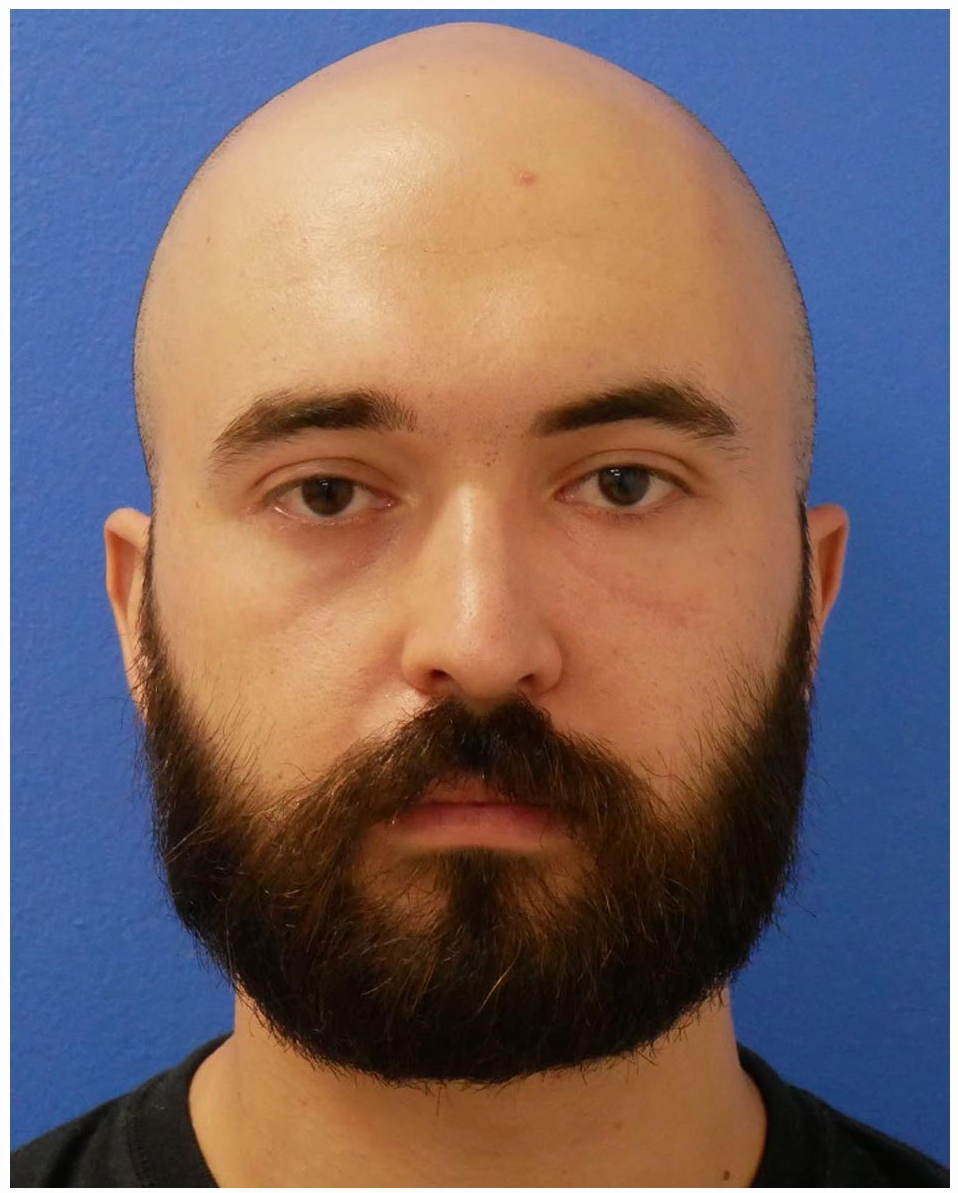
Left orbital injury immediately after penetrating trauma with a bean-bag.
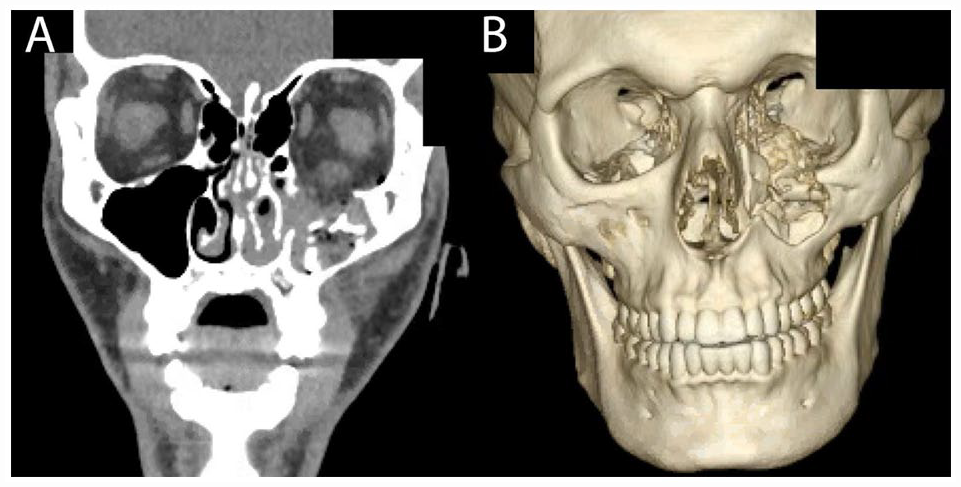
CT (A) and 3D reconstruction (B) of left comminuted maxillary and orbital floor fractures due to a bean-bag projectile
The patient underwent debridement of the left cheek, facial laceration repair and a closed reduction with stabilization of the nasal fracture. One week later, underwent ORIF of maxillary fracture which included bone grafting to the area and orbital floor reconstruction with a titanium reinforced porous polyethylene implant (Medpor Titan®) and further closed nasal septal reduction.
At 5 months follow-up, he experienced worsening vision loss of the central visual field and underwent retinal repair with ophthalmology. At this time, he also complained of persistent post-concussive symptoms of daily headaches, cognitive fatigue, word-finding difficulty, neuropathic pain in the orbital region, and mild memory loss. These symptoms limited his ability to work as a political activist and chef. At the 14-month follow-up, he continued to have orbital pain, for which he was referred to pain management and physical medicine and rehabilitation for further management (Figure 4). Patient most recently underwent resection of a left infraorbital neuroma with nerve graft reconstruction.
Follow-up at 14 months after bean-bag injury to the left eye.
Patient #2
A healthy 26-year-old man was struck by a rubber bullet during Texas State Capitol protests and suffered severe lower facial soft tissue and bony trauma. He was taken to an outside hospital and underwent an open mandibular parasymphyseal and body fracture with an open-reduction internal fixation (ORIF) and maxillomandibular fixation (MMF).
Two months after his initial surgery, he presented to the lead author’s craniofacial clinic with new onset jaw pain exacerbated while chewing. Physical exam revealed a left lower facial wound with exposed mandible, hardware, purulence, and granulation tissue, all concerning for mandibular osteomyelitis and hardware failure (Figure 5). Cultures were positive for infection with oral flora species.
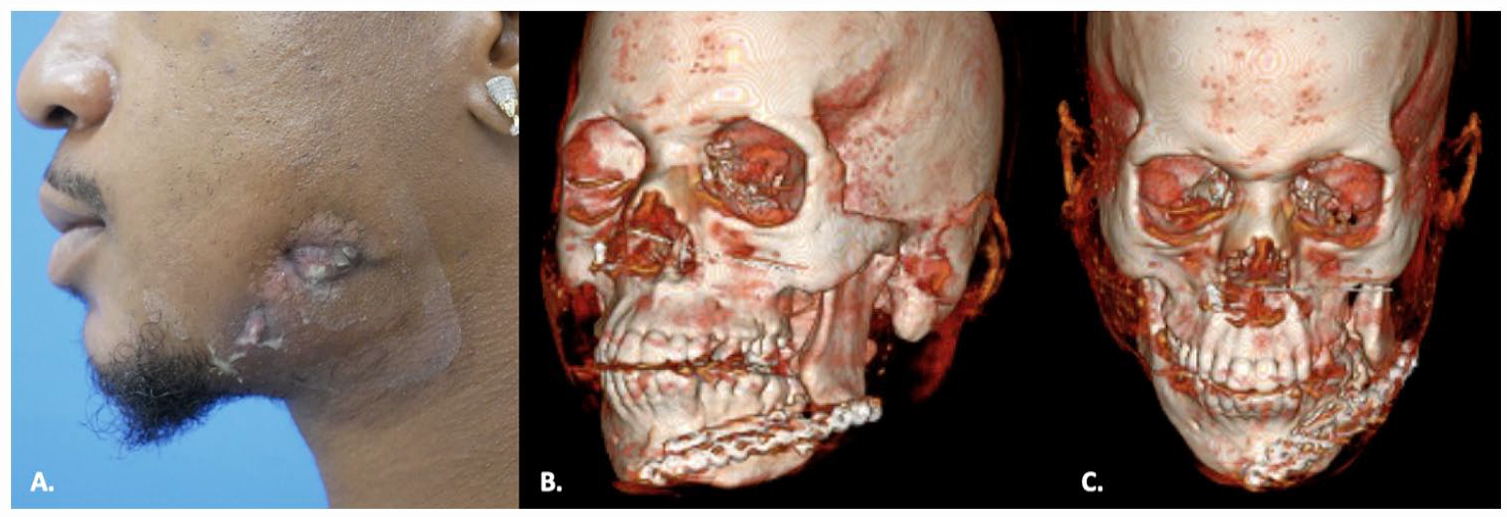
Picture (A) and 3D reconstruction (B and C) of patient one at initial presentation to the plastic surgery clinic 2-months after mandibular fracture repair.
Maxillofacial computed tomography (CT) demonstrated mandibular osteomyelitis, hardware malposition, mandibular nonunion proximally, and mandibular malunion distally with lingual rotation of the lateral segment of teeth. Because of the multifaceted nature of this patient’s condition including both soft tissue infection and significant bony malunion and nonunion, a staged treatment approach for reconstruction was selected.
First, to address the osteomyelitis, the patient was admitted to the hospital to initiate intravenous antibiotics, followed by wound and mandibular debridement, hardware removal, and placement of an mandibular external fixator. One month later, the second stage of reconstruction aimed to achieve mandibular union. This consisted of internal fixation and corticocancellous bone grafting. Five months later, the patient underwent segmental mandibular osteotomies, maxilla-mandibular fixation (MMF), and osteosynthesis of the left mandibular body with augmentation to achieve improved dental alignment. At 16 months following initial injury, the patient had stable healed soft tissue and a reproducible occlusion without pain (Figure 6).

Sixteen-month follow-up pictures (A and B) after mandible fracture repair and subsequent infection.
Patient #3
A healthy 29-year-old female presented to the emergency department with an open wound to the right cheek after sustaining a bean bag projectile injury to the face. Physical exam showed a 3 × 3 cm wound with a bean bag retained in the right cheek inferior to the zygoma in the preauricular region (Figure 7). Buccal contusions were seen on intraoral inspection and neuromuscular examination of the face suggested injury to the marginal mandibular and buccal branch of the facial nerve.
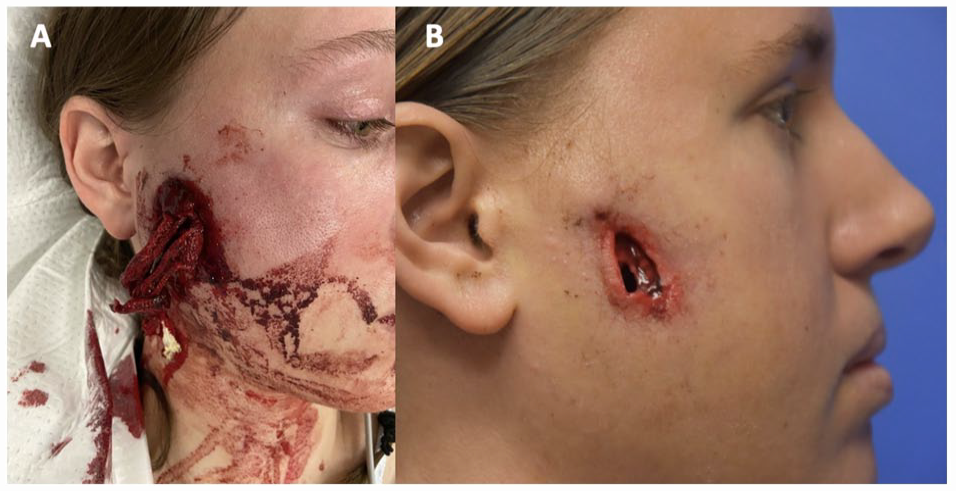
Retained bean bag projectile to the right cheek at initial presentation (A) and following foreign body removal (B).
Maxillofacial CT showed facial fractures of the right orbital floor and the right posterior mandibular body and ramus deemed structurally insignificant and managed without fixation. She underwent foreign body removal with debridement of the skin, subcutaneous tissue, muscle, fascia, and small pieces of comminuted bones.
Six months later the patient underwent scar excision to reduce contraction and fat grafting to restore soft tissue contour and volume. At 8 months post-op, her facial nerve function had returned to normal (Figure 8).

Eight-month follow-up after retained right cheek bean bag projectile.
Patient #4
A previously healthy 20-year-old male was brought into the emergency department after sustaining a beanbag projectile injury to the right parietal cranium. On presentation, the patient had a GCS of 4 with CT demonstrating a comminuted and depressed right parietal skull fracture with accompanying subarachnoid and subdural hemorrhage (Figure 9). The patient was then taken immediately to the operating room by the neurosurgery service for a craniectomy with hematoma evacuation, debridement of dura and necrotic brain tissue, duraplasty, and cranioplasty with titanium mesh. In the subsequent weeks, the patient was noted to be intermittently agitated secondary to ICU psychosis and was seen by inpatient psychiatry and palliative care services. Patient was eventually discharged to a neurology rehabilitation with long-term neurosurgery follow-up in his hometown of San Antonio. Seven months after initial admission, patient returned to our hospital reporting of intermittent suicidal ideation and self harming behavior but was discharged home with outpatient follow-up. In order to better understand the long term impacts of this trauma, the research team conducted a video interview to understand the long term physical and psychological ramifications of suffering trauma secondary to KIPs and surgery.
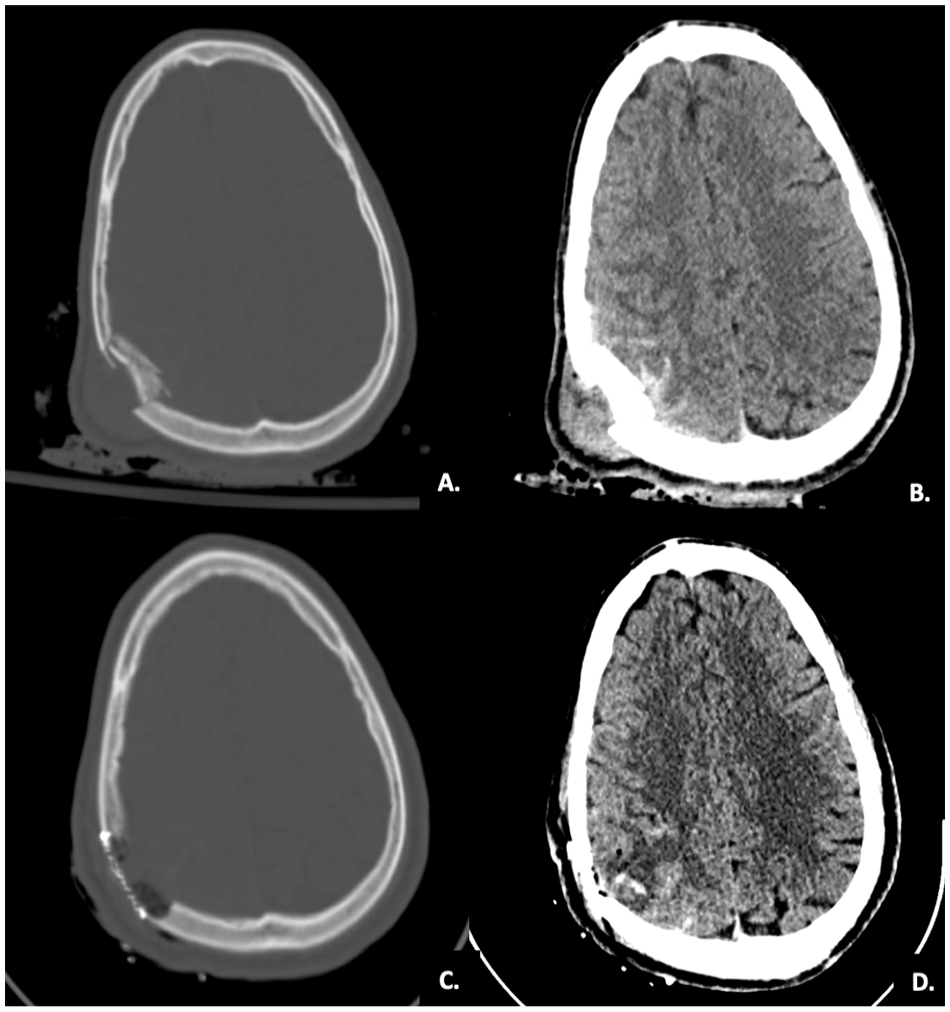
CT at initial presentation (A and B). CT after the craniectomy, duraplasty, and cranioplasty with neurosurgery (C and D).
Two years following the KIP incident, the patient reports having PTSD from ICU psychosis. He noted that immediately after the injury, he faced significant cyberbullying, had suicidal ideations, an exacerbation of preexisting BPD, and reduced self esteem secondary to his surgical scars. Currently, he sees a therapist and describes a long recovery journey since the 2020 event. Additionally, he recently began his undergraduate studies but still reports difficulties concentrating, forgetfulness, anxiety, and obsessive-compulsive behaviors. When asked about his future, he states he is going forward “armed with a mixture of baby steps and hope.”
Discussion
The first KIPs were constructed with sawed-off pieces of wooden broom handles and used in the 1880s during protests in Singapore. British colonialists further refined the wooden projectiles in the 1960s to use against protesters in Hong Kong, Malaysia, and Singapore. Britain later developed the first plastic polyvinyl chloride (PVC) and rubber bullets for use in Northern Ireland. In the United States rubber and plastic bullets were first utilized during the Vietnam War protests, but authorities halted their use in 1971 following a fatality. 1 However, KIPs were reintroduced in the United States during the 1980s as a form of crowd control management and have remained in continuous use to the present. The protest following the death of George Floyd is the most recent episode of significant use and resulted in at least 89 injuries in Minnesota and an estimated 115 head injuries across the United States. 15 , 16
Given the continued use of KIPs as crowd control measures, it is important physicians be well versed in the triaging of patients based on injury extent into minor, moderate, severe, and life-threatening categories to determine appropriate medical and surgical management. In a review of 1984 individuals with injuries secondary to KIP use, 15% of individuals faced permanent disability while the mortality rate was 3%. Of the mortality cases, penetrative injuries caused 56% of death, blunt trauma to the head and neck accounted for 23% of cases, and chest and abdominal trauma accounted for 27% of mortality cases. 17
Of the cases described here during the 2020 George Floyd protests in Austin, Texas, injuries were primarily caused by rubber bullet and bean bag projectiles. Acute injuries ranged from soft tissue loss to bony trauma with contusion, comminuted fractures, and a subarachnoid hemorrhage (Figure 10). Two of the 4 patients discussed above required multistage procedures in the acute setting, reflecting the complex nature of injury sustained. Injuries requiring acute craniofacial surgical management are summarized in Table 2. This demonstrates the variety of injuries from KIPs that we found, and the importance of highly trained surgeons in the multidisciplinary care of these patients.
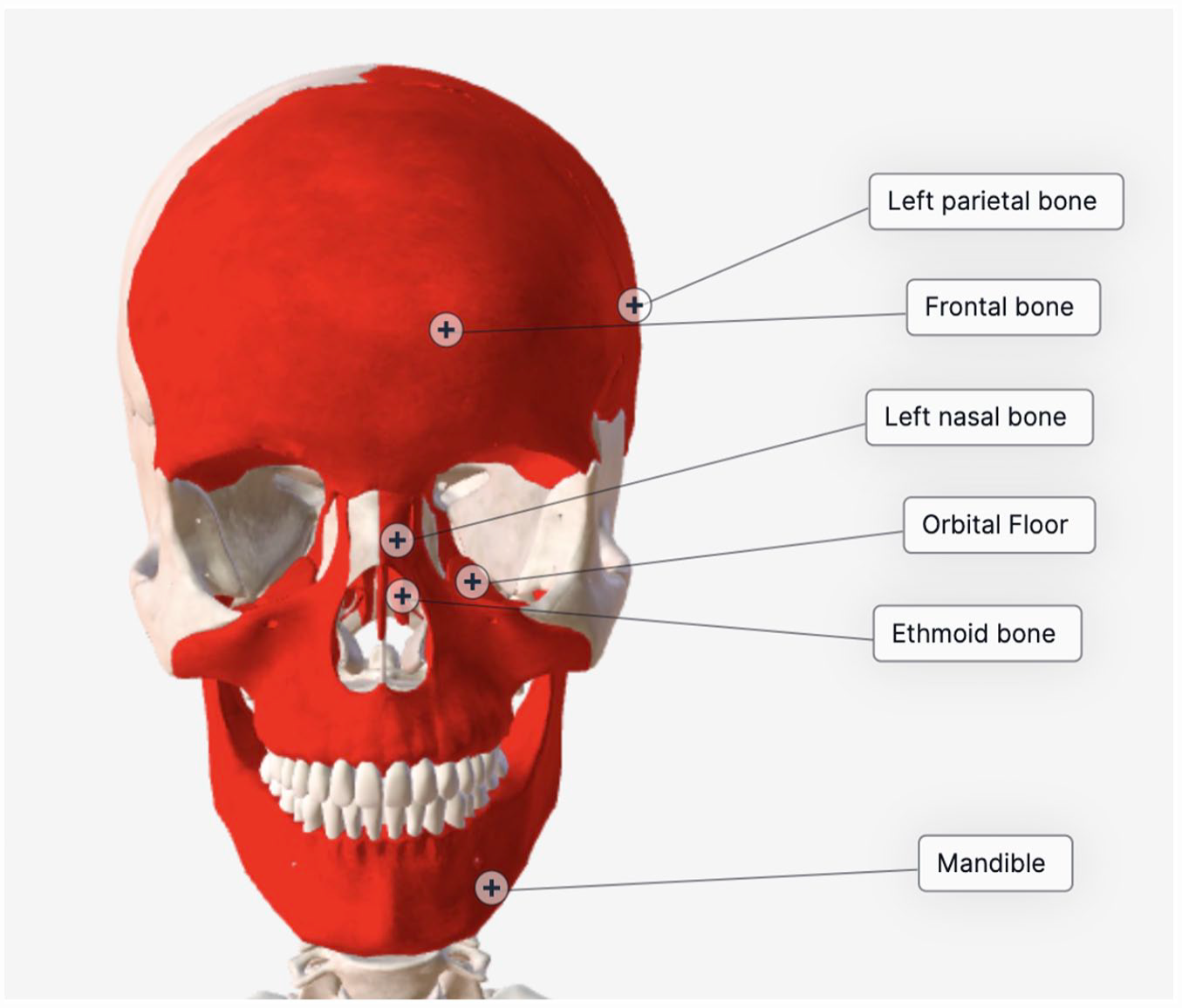
Diagram summarizing regions of craniofacial fractures seen in our patient cohort.
Summary of Acute Injuries Caused by Rubber and Bean-Bag Bullets in 4 Patients.

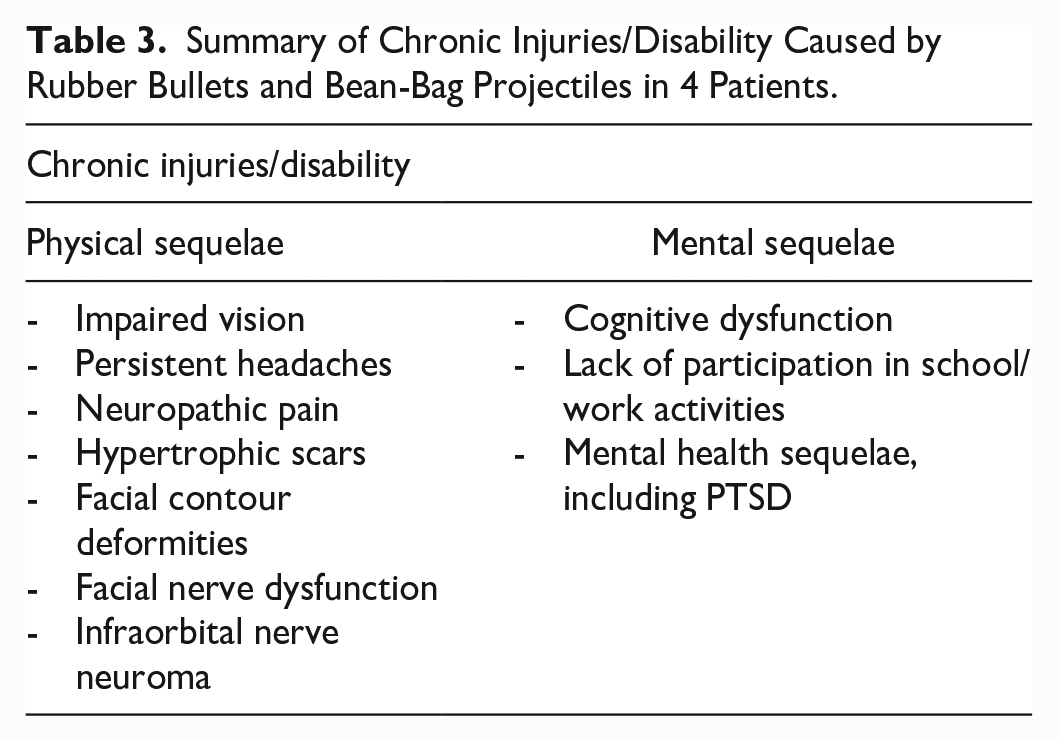
In addition to acute injuries, the patients presented in this series also suffered from chronic conditions due to KIPs (Table 3). Further, the majority of our patients (3 of 4) required multidisciplinary care including ophthalmology, neurosurgery, pain management, physical medicine and rehabilitation, and neuropsychiatry. Long-term impacts of KIPs have not been extensively documented or studied. One report from Los Angeles demonstrated that bean bag injuries were associated with the need for psychiatric consultation for 69.2% (27/39) of patients. 8 Two of 4 patients in this series had documented long-term psychological sequelae including persistent post-concussive symptoms and persistent neuropsychiatric findings (ie, anxiety). PTSD was also seen in this cohort of patients. The long-term psychological and physical impacts of KIP injuries, especially in the context of social unrest, must be further investigated.
Summary of Chronic Injuries/Disability Caused by Rubber Bullets and Bean-Bag Projectiles in 4 Patients.
While several retrospective studies describe the range of full-body injuries KIPs may cause, there are few reports specific to the craniofacial region and even less data regarding long-term health outcomes. As demonstrated in this series, the craniofacial plastic surgeon may be called upon to care for patients after a KIP injury to the face. However, only one case report was found focusing on craniofacial trauma due to a KIP, describing sustained zygomaticomaxillary complex fracture and significant facial nerve injury. 17 Limitations of this study include a small sample size of 4 patients and relatively short follow-up of 1 year for most patients.
Future work includes creating a database of KIP-associated injuries and monitoring the health status of affected individuals longitudinally to identify the unique needs of this population and to identify potential treatments targeting these issues. A database would allow for a global, centralized cohort of patient data for both research and advocacy purposes. Comparisons between craniofacial injuries with KIPs and traditional ammunition rounds could be made to better understand the differences between high and low impact projectiles. In our small series of KIP craniofacial trauma seen in Austin, TX following the George Floyd protests, we have discovered complex, composite (bone and soft tissue) trauma generally requiring multistage repair with notable rate of chronic sequelae. Given this documentation of acute and chronic impacts of KIP use, providers and patients should continue to advocate for safe crowd control practices in their communities.
Conclusion
KIPs have been considered less lethal methods of crowd control. However, injuries from KIPs can be severe and even life threatening. In the acute setting, patients may require multiple surgical interventions and complex multidisciplinary care. There are also notable long-term physical and mental health issues that require treatment. This short series describes 4 patients with craniofacial trauma due to bean bag projectiles and rubber bullets during public protests, demonstrating the potential dangers of these weapons. Given the nature of craniofacial injury from KIPs, law enforcement should consider restricting the use of this form of crowd control or additional training to prevent craniofacial trauma.
Footnotes
Authors’ Note
This work has not been previously presented.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by The University of Texas at Austin Institutional Review Board (STUDY00002358).