
Abstract
Introduction:
Plastic surgeons frequently take facial trauma calls, and their responsibilities may include infection care. The head and neck is a site of presentation for necrotizing fasciitis which requires a high level of suspicion and prompt acti2on for diagnosis and treatment. We performed a meta-analysis of the literature on necrotizing fasciitis of the head and neck (HNnf) to summarize clinical factors, causative organisms, and treatment, and included 2 cases presenting to our institution.
Methods:
A meta-analysis of the literature from 1990 to 2021 was completed on HNnf. After institutional review board approval, medical records of 2 patients presenting with a diagnosis of HNnf to an academic plastic surgery center between July and September 2021 were retrospectively reviewed. Systematic reviews and articles without comprehensive individualized patient data were excluded.
Results:
A systematic review was performed including 2 cases presenting to our institution. A total of 149 individual cases of HNnf spanning a 30-year period were included. The most common associated comorbidity was diabetes mellitus. The most frequent source of infection was odontogenic. Most patients required serial debridements in addition to IV antibiotics. Streptococcus pyogenes was the most frequent pathogen; however, most infections were polymicrobial. Infections in the periorbital region were significantly monomicrobial (P = .011). Acute reconstructive surgery requirements: 27 patients had skin grafting, 9 had flap reconstruction. Mortality rate was 12.3%. Increasing age was a significant predictor of mortality (P = .01). Patients with diabetes were significantly more likely to die from HNnf (52.6%, P = .039) and require multiple debridements (P = .001) for HNnf as compared to patients without diabetes. Infections initially arising from the submandibular region were found to be an independent negative predictor of mortality (P = .029).
Conclusion:
Our experience with HNnf along with meta-analysis of the literature revealed trends in demographics, presentation, organisms, and outcomes, increasing the collective knowledge of this rare entity.
Background
Necrotizing fasciitis is a life-threatening soft tissue infection caused by a virulent single organism or, more commonly, a polymicrobial infection, involving a wide variety of aerobic and anaerobic, gram-positive, and gram-negative bacteria.1,2 Typically, necrotizing fasciitis occurs on the abdomen, perineum, or lower limbs after trauma or surgery. However, it occurs rarely in the head and neck region, particularly when the patient’s health is already compromised. 3 The true worldwide incidence of necrotizing fasciitis of the head and neck (HNnf) remains unknown, but multiple case reports and case series have been published. Bayetto et al. 4 reported 48 per 100 000 infections per year in South Australia, and others estimate 1% to 10% of necrotizing fasciitis cases involve the head and neck.1,2
Delayed diagnosis of HNnf is a common event because the condition can arise unexpectedly out of a seemingly trivial infection or injury. Moreover, patients with HNnf may present with systemic effects and subtle physical examination findings.1,5,6 Initially, symptoms can include erythema in the head and neck, fever, crepitus, tachycardia, diaphoresis, pain, swelling, and tenderness on palpation out of proportion to the physical examination findings. HNnf can then progress to include skin changes, local pain replaced by paresthesia and anesthesia, necrosis, sepsis, and death, if untreated.1,5,6 Diagnosis is suspected based on patient history and physical examination, lab tests, imaging, and confirmed with surgical exploration.1,5,6,7 A multi-disciplinary approach with early diagnosis and prompt aggressive treatment is vital to improved prognosis, encompassing aggressive resuscitation, early and frequent assessment for surgical debridement, appropriate broad spectrum antimicrobial therapy, supportive critical care, reconstruction, and rehabilitation.1,6,8
To better understand these lesser described infections, we retrospectively reviewed 2 patients who had been treated with a diagnosis of HNnf presenting to a large academic plastic surgery group practice, and performed a meta-analysis of the literature to summarize and determine trends in clinical factors, causative organisms, treatment options, and patient outcomes.
Methods
Case Series
The authors designed a retrospective case series of 2 patients that presented to an academic plastic surgery center (The University of Texas at Austin Dell/Seton Medical Center; Austin, Texas) with a diagnosis of HNnf. The patients were treated with plastic surgery consultation for reconstruction by the senior authors (PC and RH). After institutional review board approval, inpatient and outpatient plastic surgery patient information was reviewed from July to September 2021. The retrospective review of the medical record was conducted utilizing basic demographics (age and gender), comorbid conditions, location of defect(s), empiric antibiotic regimen, causative organism(s), surgical procedure(s) performed, length of stay, and complications.
Search Strategy
A literature review was conducted in accordance with methodology conducted by Gunaratne et al. using PubMed, Medline, and EMBASE databases (1990 to present) with the search algorithm “(head and neck) AND necrotizing fasciitis” 6 was performed before September 2021 without language or geographic location limitations. The bibliographies of the relevant studies were additionally reviewed to identify additional citations. Care was taken to avoid duplication of patient data from repeated publications of series from a single institution or database, with only the most recent reports considered. Additionally, the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines were cross-referenced to ensure proper reporting. 9
Inclusion and Exclusion Criteria
HNnf was defined as clinical or histological evidence of necrotizing fasciitis involving any anatomic region above the clavicle. Infections spreading to sites beyond the clavicle, such as the superior mediastinum, were also included. For the purposes of the statistical analysis, published articles with comprehensive individualized data, including age, gender, comorbidities, location of defect(s), antibiotic treatment, causative organism(s), surgical procedure(s) performed, adjunct therapy, reconstruction of defect(s), and patient outcomes (morbidity and mortality), were sought. Non-English articles, systematic reviews, articles lacking demographic data, patient outcomes, or a majority of the individualized data, and cases in which patient age was <18 years were excluded.
Statistical Analysis and Outcomes
Pertinent data, figures, and averages were collected and analyzed using Microsoft Excel and Stata 13.0 (StataCorp, College Station, TX, USA). Outcomes were statistically determined with bivariate analysis. For 2-categorical variables, we used Chi-Squared or Fisher Exact Tests, where appropriate. Factors with a P-value below .1 were moved into the multivariable analysis. Logistic regression analysis was run since the outcome variable was dichotomous. P-values less than .05 were considered a statistically significant level.
Results
Case series
The results of our case series of 2 patients are summarized below. Both patients had comorbid diabetes. Additionally, they both had submandibular infections and favorable outcomes following serial debridements. There were a variety of gram-positive, gram-negative, and anaerobic organisms that were isolated from cultures. One patient received a skin graft for acute reconstruction (Table 1). Images obtained from maxillofacial CT for each case are shown in Supplemental Figure 1.
Summary of Case Series.
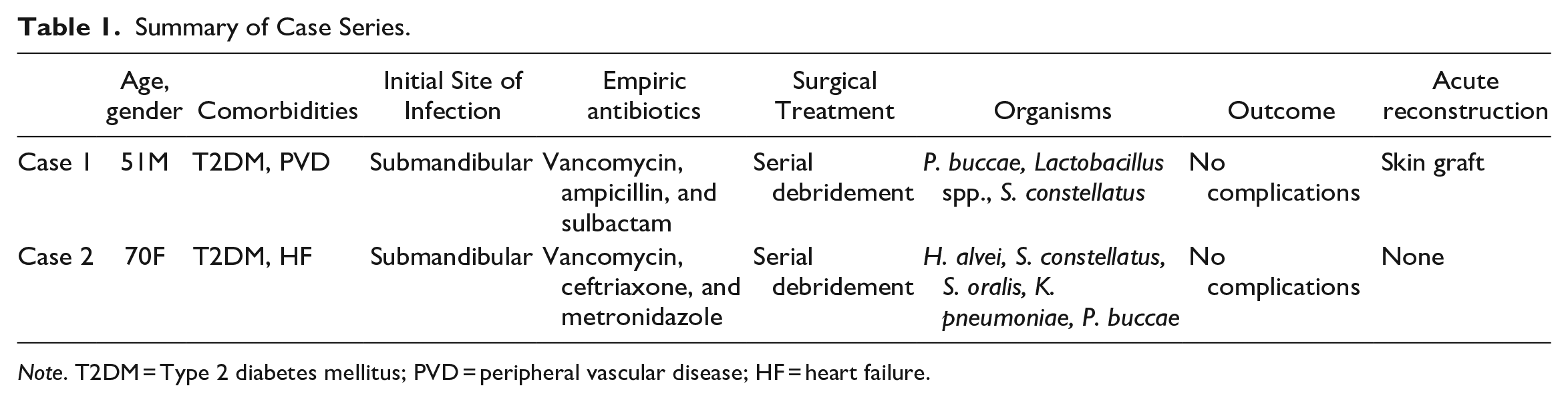
Note. T2DM = Type 2 diabetes mellitus; PVD = peripheral vascular disease; HF = heart failure.
Article Selection
A total of 244 publications were retrieved from the literature search. Titles and abstracts were reviewed, removing duplicate results across databases, systematic reviews, non-English articles, and articles not relevant to HNnf. The remaining 144 primary source data articles were appraised in full, and 56 were further removed due to exclusion criteria. The bibliographies of the appraised articles were reviewed, and 5 further publications were included. The cumulative review comprised 93 studies spanning from 1990 to 2021 that documented 147 eligible cases. A summary of the search strategy and its results is outlined in Supplemental Figure 2.
Patient Characteristics
Combining our case series of 2 patients with the cases in review, 149 patients with comprehensive individualized data over a 30-year time period were incorporated into the meta-analysis. In this sample, HNnf cases were most commonly reported from Asia (53 [35.6%]), followed by Europe (39 [26.2%]) and the United States (38 [25.5%]; Table 2). The median and average ages were 57 and 54.5 years respectively, with a range of 19 to 85 (SD; 15.9). There were slightly more male patients (55.7%). The most common associated comorbidity was diabetes mellitus (28.2%), followed by hypertension, alcohol use disorder, and immunosuppression, which were equally present in 8.7% of patients. Nearly half (45.6%) of all patients did not have any reported comorbidities. The most common source of HNnf was odontogenic (40.3%).
Patient Demographics.
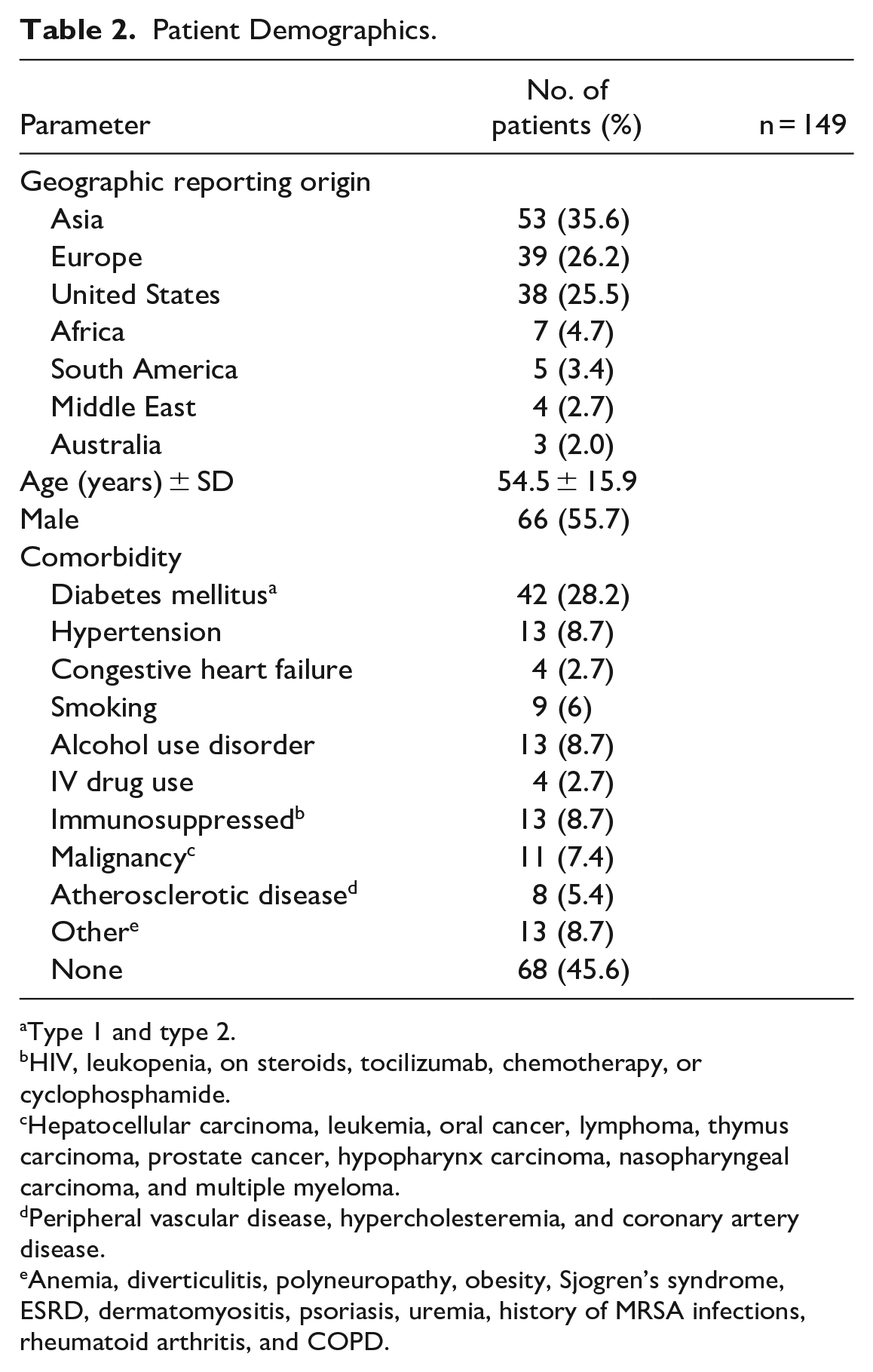
Type 1 and type 2.
HIV, leukopenia, on steroids, tocilizumab, chemotherapy, or cyclophosphamide.
Hepatocellular carcinoma, leukemia, oral cancer, lymphoma, thymus carcinoma, prostate cancer, hypopharynx carcinoma, nasopharyngeal carcinoma, and multiple myeloma.
Peripheral vascular disease, hypercholesteremia, and coronary artery disease.
Anemia, diverticulitis, polyneuropathy, obesity, Sjogren’s syndrome, ESRD, dermatomyositis, psoriasis, uremia, history of MRSA infections, rheumatoid arthritis, and COPD.
Necrotizing Fasciitis Features
For the 149 patients under review, there were a variety of initial infection sites, determined during full text review as the first site with evidence of infection before involvement of other head and neck regions. Submandibular infections were most common (66 [44.3%]), consistent with the most common source of infection being odontogenic (Figure 1). A 19.5% of patients initially had periorbital infections, 15.4% had parapharyngeal infections, 8.7% had infections involving the malar and submalar areas of the face, and 5.4% had infections of the superficial layer of the neck. The laryngeal, scalp, and preauricular regions were less common sites of initial infection. One patient with periorbital necrotizing fasciitis developed an ascending infection into the brain causing fulminant cerebral infarction. 10 Throughout the clinical course of 56 (37.6%) patients, necrotizing fasciitis developed in multiple regions of the head and neck.
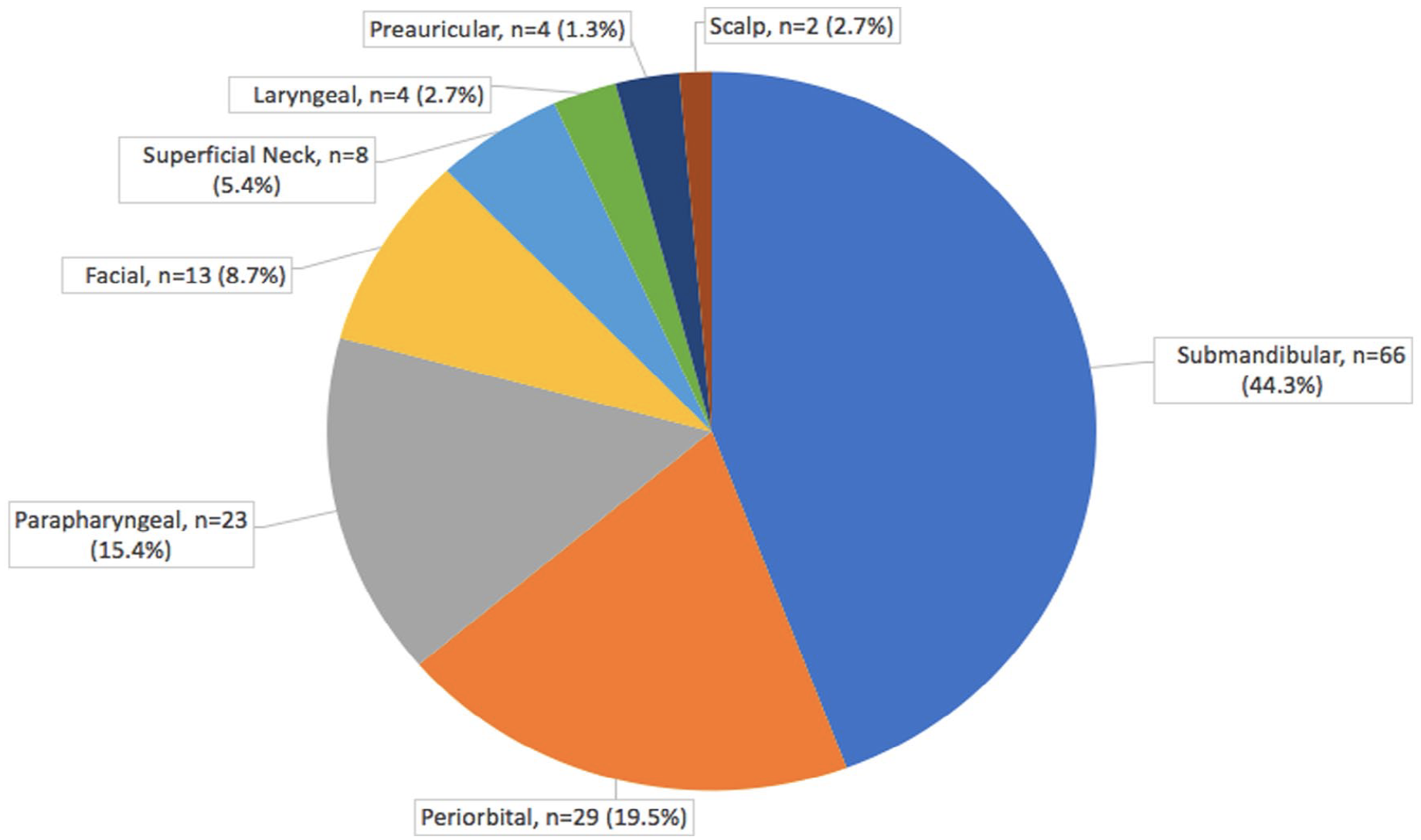
Sites of initial infection.
Microbiology
In 20 cases, either no organism was isolated from wound culture or no organism was reported. Of the remaining 129 cases with a reported organism, 54 (41.9%) had a monomicrobial infection isolated from wound or surgical culture whereas 75 cases (58.1%) were polymicrobial (Table 3). Streptococcus pyogenes was the most commonly isolated organism in both monomicrobial and polymicrobial infections. Among the 21 monomicrobial infections in which S. pyogenes was isolated, most cases (13 [61.9%]) were reported in the U.S., and the most common infection site origin was the periorbital region (10 [47.6%]). Infections originating in the periorbital region were significantly monomicrobial (P = .011) on Chi-square analysis.
Causative Organisms.
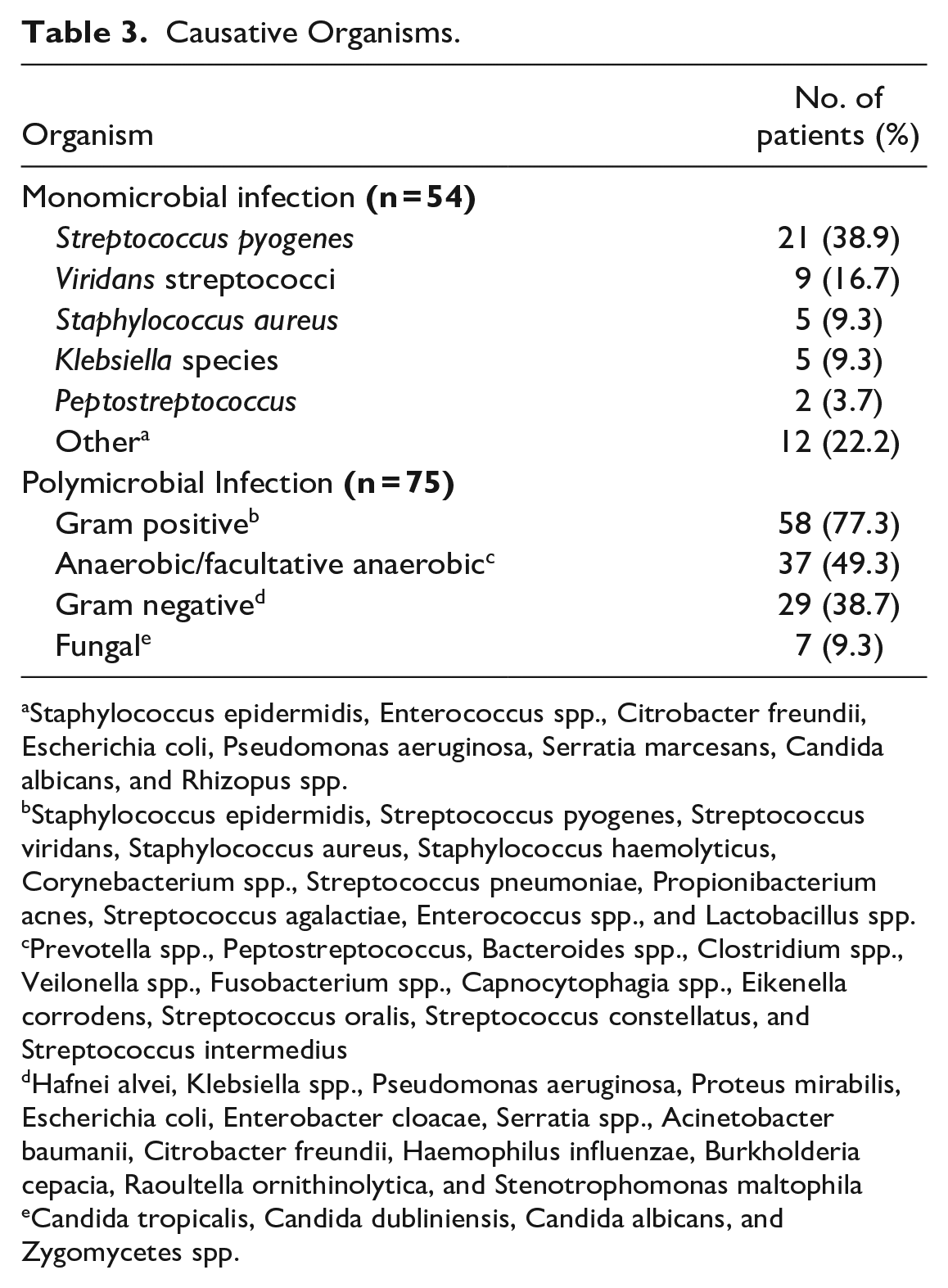
Staphylococcus epidermidis, Enterococcus spp., Citrobacter freundii, Escherichia coli, Pseudomonas aeruginosa, Serratia marcesans, Candida albicans, and Rhizopus spp.
Staphylococcus epidermidis, Streptococcus pyogenes, Streptococcus viridans, Staphylococcus aureus, Staphylococcus haemolyticus, Corynebacterium spp., Streptococcus pneumoniae, Propionibacterium acnes, Streptococcus agalactiae, Enterococcus spp., and Lactobacillus spp.
Prevotella spp., Peptostreptococcus, Bacteroides spp., Clostridium spp., Veilonella spp., Fusobacterium spp., Capnocytophagia spp., Eikenella corrodens, Streptococcus oralis, Streptococcus constellatus, and Streptococcus intermedius
Hafnei alvei, Klebsiella spp., Pseudomonas aeruginosa, Proteus mirabilis, Escherichia coli, Enterobacter cloacae, Serratia spp., Acinetobacter baumanii, Citrobacter freundii, Haemophilus influenzae, Burkholderia cepacia, Raoultella ornithinolytica, and Stenotrophomonas maltophila
Candida tropicalis, Candida dubliniensis, Candida albicans, and Zygomycetes spp.
There were a wide variety of organisms isolated from the 75 cases with polymicrobial infection, categorized broadly in Table 3 as gram positive organisms, anaerobic/facultative anaerobic organisms commonly found in the oral cavity, gram negative organisms, and fungi. Among these cases, 2.7 organisms were isolated on average. Gram positive organisms were isolated in most cases (57 [77.3%]), followed by anaerobic/facultative anaerobic organisms (37 [49.3%]) and gram negative organisms (29 [38.7%]). Forty-seven cases were caused by a mixed polymicrobial infection in which organisms from multiple categories were isolated.
On logistic regression among the patients with reported organisms, the odds of finding S. pyogenes as an isolated organism in HNnf wound cultures slightly decreased over time during the 30-year study period (OR = 0.96; 95% CI, 0.92-0.99). This finding was shared by S. viridans (OR = 0.92; 95% CI, 0.87-0.97). However, K. pneumoniae was found to have slightly higher odds over time (OR = 1.09; 95% CI, 1.02-1.16).
Treatment and Patient Outcomes
There were 112 cases (75.2%) that reported empiric antibiotics, defined as antibiotics given to patients before culture results were obtained. Thirty-nine patients had an odontogenic source of infection and received a variety of empiric antibiotics. However, 19 of these patients (48.7%) were not provided with adequate anaerobic coverage. These patients typically received monotherapy with clindamycin or beta lactams such as penicillin and cephalosporins, and some patients were given empiric antibiotic therapy involving a combination of these agents that were still considered inadequate by review of the author (RT) with infectious disease expertise.
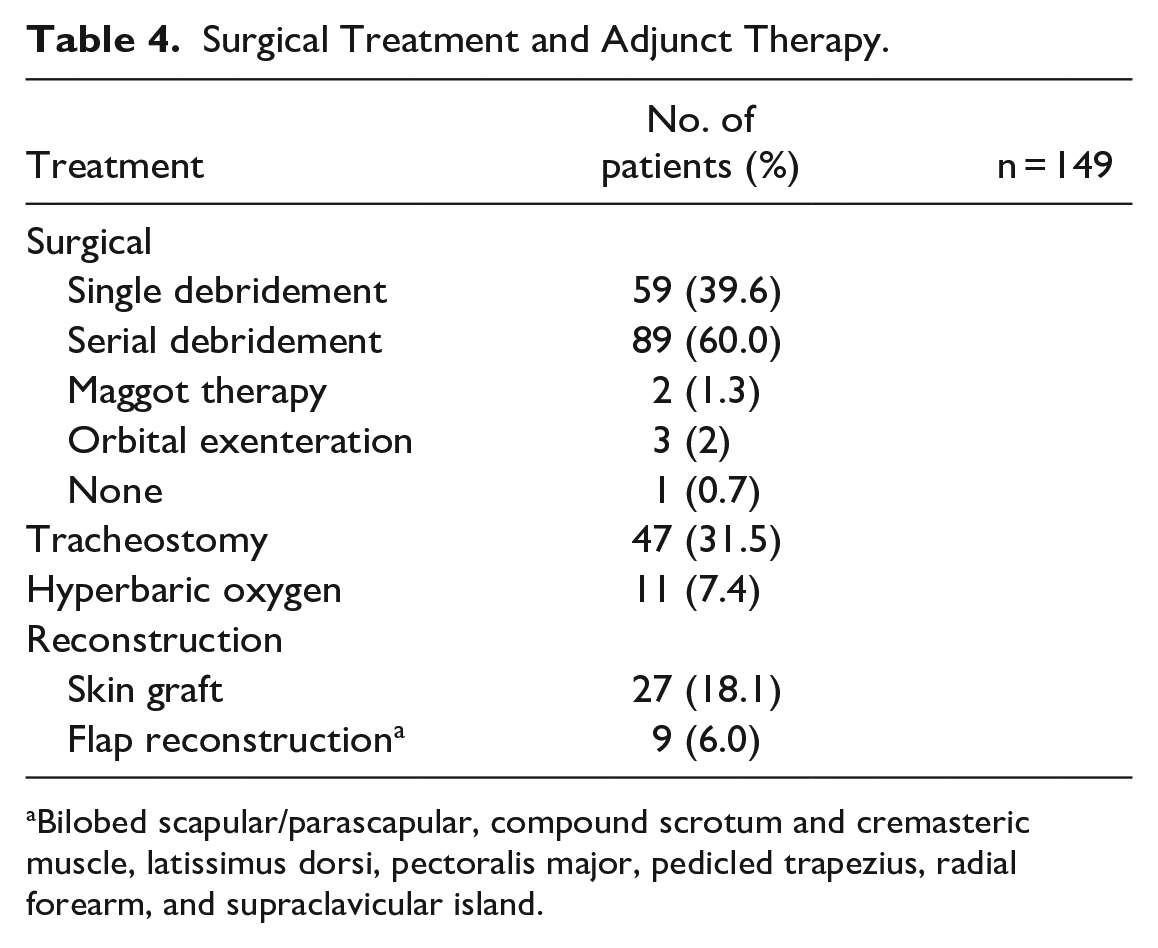
The majority of patients (89 [60%]) ultimately required serial debridements until clinical improvement (Table 4). Reconstructive requirements varied widely depending on the size and location of the defect, although most patients (116 [77.9%]) did not receive any acute reconstruction. 27 (18.1%) patients received a skin graft (Table 4), of which 3 were grafted with biosynthetic mesh. Nine patients received flap reconstruction with various types of tissue flaps, which were not limited to muscle flaps. The authors of 1 case of periorbital necrotizing fasciitis utilized a compound graft from the scrotum, incorporating skin and cremasteric muscle that was reinnervated with a sural nerve graft coapted onto the frontal nerve in order to restore dynamic eyelid animation. 11 Three patients received a skin graft in addition to flap reconstruction.
Surgical Treatment and Adjunct Therapy.
Bilobed scapular/parascapular, compound scrotum and cremasteric muscle, latissimus dorsi, pectoralis major, pedicled trapezius, radial forearm, and supraclavicular island.
Hyperbaric oxygen therapy (HBOT) was used as adjunct therapy in 11 (7.4%) patients (Table 4). Tracheostomy was performed in nearly one-third of patients (31.5%) who typically had pharyngeal, submandibular, and/or mediastinal involvement for protection of the airway.
Mediastinitis (necrotizing and non-necrotizing) was the most common complication of HNnf, occurring in 20 (13.4%) patients. Sepsis was reported as the next most common complication, occurring in 15 (10.1%) patients. More than two-thirds of patients (67.8%) clinically resolved without complications following treatment. There were no comorbidities independently associated with complications on Chi-square analysis. Mortality rate among our 149 patients in review was 12.3% (n = 19), and increasing age was a significant predictor of mortality (P = .01) on Chi-squared analysis.
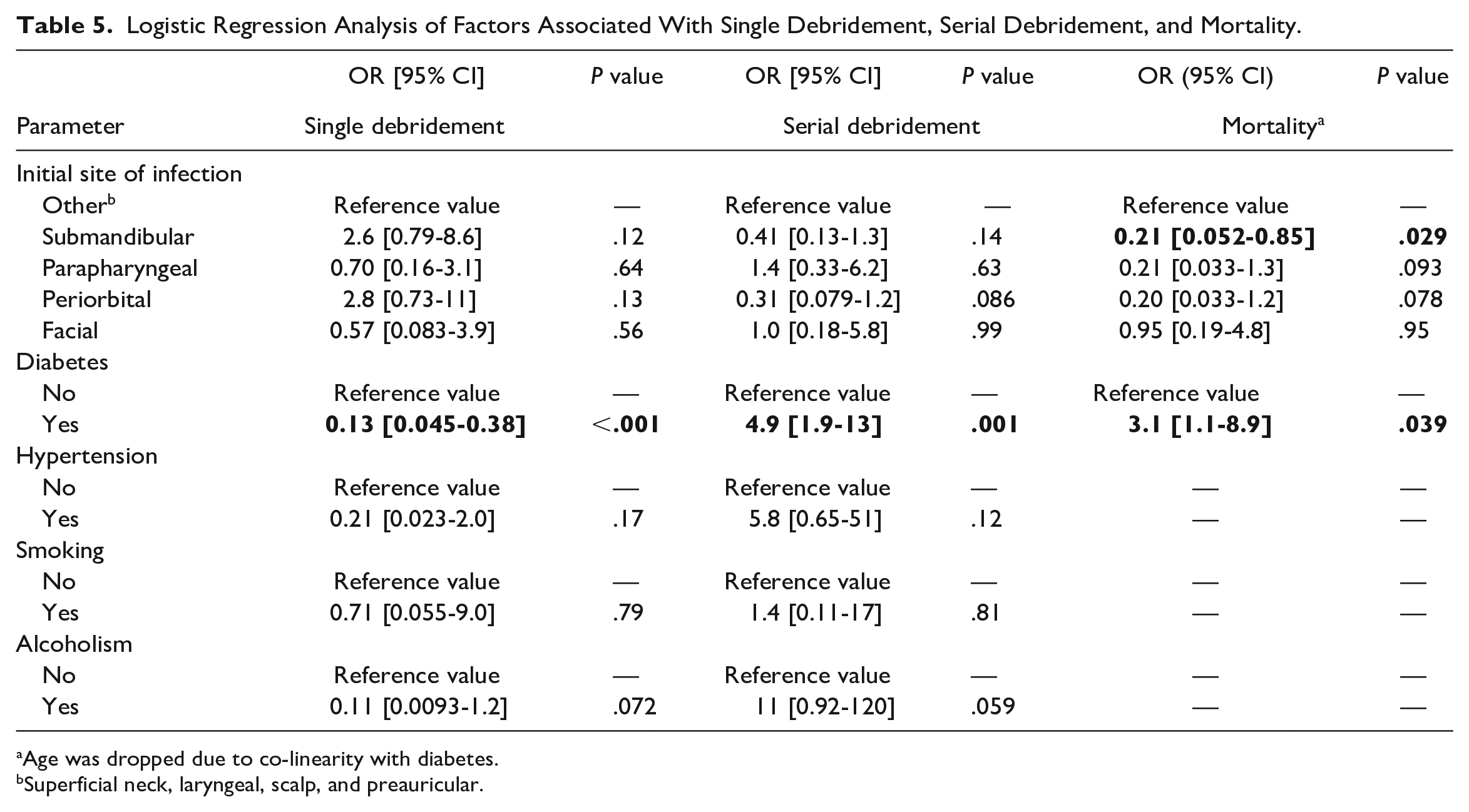
To determine patient factors associated with surgical burden and mortality in HNnf, the geographic origin of report, initial site of infection, gender, age, and comorbidities were included in the analysis. Initial Chi-squared analyses led to gender and the geographic origin of report to be excluded from the multivariate analysis completely as P > .1 for these parameters. Hypertension, smoking, and alcoholism were excluded following Chi-squared analyses with mortality.
On multivariate logistic regression analysis, an initial site of infection in the submandibular area was an independent negative predictor of mortality (OR = 0.21; 95% CI, 0.025-0.85; Table 5). Parapharyngeal, periorbital, and facial sites of initial infection were not significant predictors of surgical requirements or mortality. Diabetic patients had significantly higher mortality compared to non-diabetic patients (OR = 3.1; 95% CI, 1.1-8.9) and were significantly more likely to require serial debridements compared to non-diabetic patients (OR = 4.9, 95% CI, 1.9-13). Similarly, diabetic patients were significantly less likely to achieve clinical resolution following a single debridement compared to patients without diabetes (OR = 0.13, 95% CI, 0.045-0.38). There were no significant differences between patients with hypertension, smoking, or alcohol use disorder compared with respective patients without each of these respective comorbidities. Hypertension and alcoholism trended with increased numbers of serial debridement, but this was not statistically significant.
Logistic Regression Analysis of Factors Associated With Single Debridement, Serial Debridement, and Mortality.
Age was dropped due to co-linearity with diabetes.
Superficial neck, laryngeal, scalp, and preauricular.
Discussion
Global Reporting
Among our sample of patients, most cases were reported in Asia (53 [35.6%]), followed by Europe (39 [26.2%]) and the United States (38 [25.5%]). Taiwan was the country to most frequently report cases of HNnf following our exclusion criteria (14 [10.6%]). However, there are no studies on global reporting of HNnf, making comparisons to the literature difficult to conclude. Moreover, our exclusion process may have skewed representation of HNnf cases toward certain locations, and not all cases of HNnf will be reported in the literature. Therefore, in the present study, the geographic reporting of HNnf cases should not be interpreted to be completely representative of HNnf occurrences.
Comorbidities and Infection Source
Gunaratne et al., in a large-scale retrospective review of cervical necrotizing fasciitis, found diabetes mellitus (18.3%), and alcohol use disorder (9.1%) as the most prevalent risk factors. 6 Of note, their large sample size was the result of the complication of primary and secondary source data, including multiple systematic reviews over a 60-year study period. While our review is the first to perform a meta-analysis on primary source data. Our sample of primary data including 149 patients more commonly had diabetes mellitus (28.2%), and alcohol use disorder was similarly present in 8.7% of patients. Other risk factors commonly reported in the literature include cirrhosis, arteriosclerosis, atherosclerosis, HIV, corticosteroid therapy, chronic renal failure, cancer, drug abuse, obesity, malnutrition/malnourishment, old age, and organ transplants.1,2,6 In our review, 8.7% of patients were categorized as immunosuppressed, including etiologies such as HIV, leukopenia, or taking immunosuppressants. A 8.7% of patients had hypertension. A 7.4% patients had an underlying malignancy of various types, with about half of these occurring in the head and neck. Patients with these malignancies often developed HNnf as a postoperative complication of tumor resection, especially in those who had received resection of primary tumor followed by bilateral neck dissection.8,11,12 HNnf developed as a postoperative complication of other surgeries as well, including thyroidectomy and sebaceous cyst removal.13,14 Nearly half (45.6%) of all patients did not have any reported comorbidities, showing that there should be concern for HNnf in the presence of suggestive physical exam findings even in patients without significant medical history.
The most common source of HNnf was odontogenic (40.3%), which is consistent with many cases of HNnf involving the submandibular and parapharyngeal regions in our review. Gunaratne et al. found a similar rate of odontogenic infections (47.0%). Additionally, there were some unusual causes of HNnf including an infected occipital psoriatic plaque and bathing in a public hot tub.15,16 Some patients developed HNnf following lacerations from a rusty nail, razor blade, or glass window.17 –19 One patient even developed HNnf as a result of buccal mucosa injury with a toothbrush, illustrating the potential to develop HNnf from trivial injury. 20
Microbiology
Multiple reviews have classically proposed at least 2 distinct microbial entities for necrotizing fasciitis, including polymicrobial with aerobic and anaerobic bacteria (type 1) or Streptococcus pyogenes alone or in combination with Staphylococcus species (type 2).3,21 In HNnf, the more common organisms include, in descending order, Streptococcus, Staphylococcus, Prevotella, Peptostreptococcus, Bacteroides, Fusobacterium, Enterobacter, Klebsiella, Escherichia coli, Pseudomonas, and Candida.1,6 Of cases with reported organisms in our analysis, most HNnf infections were polymicrobial with a wide variety of anaerobic, gram-positive, and gram-negative causative organisms. S. pyogenes was the most commonly isolated organism among monomicrobial and polymicrobial infections, showing that HNnf shares the established microbial paradigm in necrotizing fasciitis. Periorbital necrotizing fasciitis was found to be significantly monomicrobial (P = .011), and S. pyogenes was the causative organism in 76.9% of these cases, suggesting that type 2 necrotizing fasciitis occurs frequently in this area.
Interestingly, the odds of S. pyogenes and S. viridans to be isolated from HNnf wound cultures slightly decreased over time (OR = 0.96 and 0.92, respectively), while K. pneumoniae isolation was found to have slightly increased odds over time (OR = 1.09) in our thirty-year study period. While the magnitudes of these trends are not strong enough to indicate clinical significance, they certainly suggest that HNnf microbiology is slowly evolving. As more literature on HNnf becomes available, additional studies are needed to study changes in HNnf microbiology.
Empiric Antibiotic Therapy
For patients with necrotizing skin infections, blood, purulent wound drainage, and operative cultures must be collected promptly to tailor antibiotic therapy. Early and aggressive use of antibiotic therapy is essential for improving patient outcomes and should be performed concomitantly with prompt surgical evaluation and treatment. 22 Given the serious nature of HNnf infections, broad spectrum intravenous antibiotics like ampicillin-sulbactam, amoxicillin-clavulanate, piperacillin-tazobactam, or carbapenems in combination of vancomycin to cover gram positive organisms like methicillin resistant staphylococcus aureus (MRSA) should be initiated. Once MRSA is ruled out, vancomycin can be discontinued and antibiotics de-escalated to address cultured organisms. Furthermore, the proper regimen is guided by the source of infection if known or highly suspected. For odontogenic infections, the addition of an agent that provides anaerobic antimicrobial activity, such as metronidazole, is vital. Clindamycin has been used as an agent for anaerobic coverage and the reduction of bacterial toxins but is likely to be inadequate, as studies have shown oral pathogens to have high rates of resistance to clindamycin.23,24 We found that nearly half of patients with an odontogenic source of HNnf were not provided with proper empiric antibiotic coverage for anaerobic organisms. Varying guidelines among countries and limited access to resources may contribute to this finding.
Equally important as selecting the proper empiric antibiotics, de-escalating the antibiotic regimen after obtaining culture results must be performed to prevent secondary bacterial infections with drug-resistant pathogens. No clinical trials have evaluated the duration of therapy in necrotizing fasciitis, but guidelines recommend that antimicrobial therapy be administered until further debridement is no longer necessary, the patient has improved clinically, and fever has been absent for 48 to 72 hours. 25
Surgical Management
In our review, most patients (89 [60%]) received serial debridements until clinical resolution. In 58 patients (39%), a single operation was performed as surgical treatment; however, in some cases this debridement was extensive. One patient with HNnf affecting the submandibular and parapharyngeal regions required wide exposure of the neck with resection of necrotic bands extending to the anterior mediastinum, and was subsequently treated with targeted antibiotic therapy and hyperbaric oxygen. 26 Three patients required orbital exenteration in addition to debridement due to an unsalvageable globe or to prevent spread of infection into the brain.17,27,28 Two patients were initially debrided, but due to their poor clinical status and surgical candidacy, maggot therapy was provided as an alternative to further debridement.11,29 Of note, these 2 patients had their cases published in 2002 and 2004, with no subsequent cases utilizing maggots in our review. However, both patients had favorable outcomes without morbidity or mortality, and achieved acceptable cosmetic results. The 1 patient exempt from debridement was found to have extensive cerebral infarction from ascending infection to the brain and was too unstable to undergo surgery, expiring 5 days after presenting. 10
Acute reconstructive surgery following debridement was not reported in the majority of cases; only a small subset of patients—18.1% receiving skin graft and 6% receiving flap reconstruction had reconstructive surgery performed. The decision to perform reconstructive surgery depended on a variety of factors including surgeon and institution preference, access to resources, and the extent of the surgical defect. HNnf was therefore shown to be a condition typically treated with primary debridement in the acute setting. However, due to the lack of long-term follow-up, the quality of functional outcomes and rates of secondary reconstructive surgery cannot be adequately assessed in this review.
Compared to the aggressive surgical treatment of necrotizing fasciitis in the extremities and trunk, surgical treatment in the face, head, and neck requires more finesse due to it being a compact area housing vital structures, so that only the necrosed tissue is excised and, where possible, the muscles, nerves, arteries, and skin are preserved.1,6,30 In 1 case illustrating these complexities, the patient’s common carotid artery had been inadvertently clamped together with the internal jugular vein during debridement, resulting in loss of cardiac output and ultimately death. 31 Additionally, the head and neck is an anatomical region that contains several fascial planes that promote spread of infection. Any delay in the treatment of necrotizing fasciitis will therefore expedite the spread of infection to dangerous spaces and subsequently to the mediastinum inferiorly. We found mediastinitis to be the most common complication of HNnf in our review, occurring in 13.4% of patients.
Mortality
The mortality rate among our sample of patients was 12.3%, which is comparable to the 13.4% mortality rate found among a global systematic review by Gunaratne et al. 6
To the authors’ knowledge, this is the first study to analyze HNnf mortality from published primary source data only. Age is a statistically significant risk factor for mortality from HNnf, which is an association shared among analyses of patient outcomes in other types of necrotizing fasciitis.32,33 Accounting for potential confounding in multivariable analysis, a decreased likelihood of mortality was independently associated with initial submandibular infections. It is unclear why this was found, but possible explanations may include that submandibular necrotizing fasciitis is diagnosed more promptly, or perhaps the area is treated more comprehensively with aggressive surgical debridement.
An increased likelihood of receiving serial debridements and an increased likelihood of mortality were independently associated with diabetes. The former finding is expected, given that patients with diabetes have poorer surgical outcomes in necrotizing fasciitis, with significantly higher rates of amputation following necrotizing fasciitis in the limbs. 34 In the head and neck, we show this association to manifest itself as an increased likelihood to require serial debridements for clinical resolution. However, multiple recent analyses of necrotizing fasciitis have shown diabetes to be independently associated with poorer patient outcomes but not mortality.33 –37 Perhaps the extensive network of fascial planes and abundance of vital structures contained within the head and neck compound dangerously with the impaired cutaneous wound healing and increased susceptibility to infection in patients with diabetes, leading to significantly higher rates of mortality. Therefore, aggressive medical and surgical therapy is needed for all, but especially in diabetic and elderly populations suspicious of HNnf presentation. Additional prospective studies may be designed in the future to further assess these associations.
Limitations
The limitations of this study are attributable to the retrospective study design. Medical records, which are not designed or standardized for research purposes, may not include all variables of research interest and therefore information in the articles we reviewed may have been lacking. In addition, there may be considerable variation between the data points that the authors of each case report or case series choose to report, further reducing the ability to perform a comprehensive analysis. To reduce the effects of these issues, we excluded articles that were missing key demographic information. Of the remaining articles, statistical analyses were performed according to the availability of data, censoring articles as appropriate. However, this does not account for possible reporting bias in the literature, which likely underreports cases of HNnf that occur worldwide. With regards to the microbial analysis that was performed, no articles provided how cultures were obtained and did not mention culturing techniques, limiting the validity of our results.
Conclusion
A meta-analysis of the literature was performed along with our retrospective case series of 2 patients to determine clinical factors, causative organisms, and treatment considerations. Our review consisted of 149 patients with individualized data from global reports spanning 3 decades with an average age of 54.5 and diabetes as the most common comorbidity. Streptococcus pyogenes was the most causative organism in both monomicrobial and polymicrobial infections. Most infections were polymicrobial. However, periorbital infections leading to necrotizing fasciitis tended to be monomicrobial. All patients were treated with empiric antibiotic therapy, but nearly half of patients with an odontogenic source of infection did not have proper coverage for anaerobes. Most patients required serial debridements for surgical treatment. Acute reconstructive surgery was not commonly reported. Further studies could be performed to elucidate possible rates of secondary reconstructive surgery after this potentially deforming head and neck infection. Mortality rate was 12.3%. Relative to nondiabetic patients, diabetic patients with HNnf had greater surgical requirements and increased mortality, showing the need for greater suspicion and prompt diagnosis and treatment in these patients.
Supplemental Material
sj-docx-1-fac-10.1177_27325016231166134 – Supplemental material for Head and Neck Manifestations of Necrotizing Fasciitis: A Case Series and Meta-Analysis
Supplemental material, sj-docx-1-fac-10.1177_27325016231166134 for Head and Neck Manifestations of Necrotizing Fasciitis: A Case Series and Meta-Analysis by Derek Yan, Cole Holan, Pablo L. Padilla, Sina Ramtin, Darsh Shah, Ellen Hancock, Rama Thyagarajan, Patrick Combs and Raymond Harshbarger in FACE
Supplemental Material
sj-docx-2-fac-10.1177_27325016231166134 – Supplemental material for Head and Neck Manifestations of Necrotizing Fasciitis: A Case Series and Meta-Analysis
Supplemental material, sj-docx-2-fac-10.1177_27325016231166134 for Head and Neck Manifestations of Necrotizing Fasciitis: A Case Series and Meta-Analysis by Derek Yan, Cole Holan, Pablo L. Padilla, Sina Ramtin, Darsh Shah, Ellen Hancock, Rama Thyagarajan, Patrick Combs and Raymond Harshbarger in FACE
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Institutional Review Board approval was not required.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.