
Abstract
Introduction:
Access to specialist care remains a major challenge in rural and remote areas of Canada. Virtual Hallway is a secure digital platform that enables timely, provider-to-provider telephone consultations between primary care providers (PCPs) and specialists. This study evaluates satisfaction and effectiveness of the platform in Prince Edward Island (PEI), a small, rural province, across two time points to assess its sustained impact and usage patterns.
Methods:
A cross-sectional survey was conducted during two periods in 2024. PCPs were invited to complete postconsultation surveys, which assessed user satisfaction, in-person referral avoidance, and motivations for specialist selection. Descriptive statistics and chi-square tests were used for analysis.
Results:
Survey data included 181 postconsultation responses. Referral avoidance remained high (85% and 75% at time points 1 and 2, respectively). User satisfaction was consistently high among both PCPs (98%–100%) and specialists (92%–98%). PCPs reported improved care quality even when referrals were not avoided. Over time, specialist selection shifted from local availability to unmet specialty access within PEI (p = 0.03), suggesting increased use for complex cases.
Conclusion:
The Virtual Hallway platform demonstrated sustained effectiveness in improving access to specialist care and reducing in-person referrals in a rural province. These findings support broader implementation of virtual peer-to-peer consultation platforms to address access disparities across Canada.
Keywords
Introduction
Access to specialty care remains a persistent challenge in the Canadian health care system, with specialists largely concentrated in urban areas, leaving rural and remote regions underserved.1,2 In provinces like Prince Edward Island (PEI), where the population is small and dispersed, accessing specialist care is especially difficult. This creates pronounced geographic disparities, with rural and less populated areas facing the greatest barriers. 1 Patients in these regions often endure both long travel distances and significant delays in care, exacerbating morbidity and mortality due to postponed or inaccessible treatment.2–5 Prolonged wait times for specialist consultations highlight the seriousness of this issue. Additionally, limited specialist access increases pressure on primary care providers (PCPs), who must manage complex cases without specialist input—underscoring the urgent need for solutions that bridge the gap between primary and specialty care.6,7
Virtual consultation platforms have emerged as a promising solution to bridge this gap, enabling PCPs to access specialist expertise more efficiently through technology-enabled communication. Several virtual consultation models have been evaluated internationally, such as eConsult systems in Ontario and Alberta and teleconsultation services within the U.S. Veterans Health Administration and the United Kingdom’s National Health Service.8–10 These programs have consistently demonstrated improved access to specialist input and reductions in unnecessary in-person referrals. However, most prior evaluations focused on asynchronous consultation models and were primarily implemented in urban or regional health networks. Recent evidence indicates that synchronous teleconsultation modalities—such as real-time video or phone consultations—enable richer clinical dialogue and faster decision-making by allowing immediate, bidirectional communication between providers.11,12 This study builds on that body of work by evaluating a synchronous, provider-to-provider model integrated within provincial health care systems and assessing its longitudinal and cross-provincial performance in a rural Canadian context.
The Virtual Hallway (Virtual Hallway Consults Inc., Halifax, Nova Scotia, Canada) platform was created to address these challenges by facilitating provider-to-provider phone consultations between PCPs and specialists, enabling timely communication and reducing reliance on in-person referrals. The platform aims to streamline consultations and improve patient care. A previous Nova Scotia (NS) study showed that it significantly reduced in-person referrals and improved care for patients awaiting specialist input. 13 However, less is known about the platform’s performance across different regions or its long-term effectiveness. To address these gaps, this study evaluates the Virtual Hallway platform’s effectiveness in PEI and examines its sustained impact at a second time point. This longitudinal approach offers insight into trends and the platform’s longer-term utility. We also explored the motivations behind PCPs’ specialist selection to better understand user behavior and how the platform addresses resource gaps. These insights are essential for optimizing the platform’s design and ensuring it meets health care providers’ needs.
Methods
Setting
This study was conducted in PEI over two distinct time periods: the first from January to March, 2024, and the second from October to November, 2024. The two survey periods were selected to evaluate both early implementation and sustained engagement with the platform over time. This approach allowed assessment of evolving usage patterns and satisfaction as adoption matured. Some overlap of respondents likely occurred, but anonymity prevented linking individual responses across time points. Analyses therefore reflect aggregate, unpaired data comparing trends between the two survey periods. PEI is Canada’s smallest province, with a population of ∼160,000 people spread across 5660 km2. The study involved PCPs based in PEI and specialists from both PEI and NS. The Virtual Hallway platform facilitated synchronous provider-to-provider phone consultations, enabling PEI PCPs to access specialist expertise across provincial borders. Both referring and consulting physicians were eligible for compensation through existing provincial health care billing codes, making the service accessible and integrated into the existing health care infrastructure.
Virtual Hallway platform
Virtual Hallway is an online platform that facilitates provider-to-provider, patient-focused virtual consultation via synchronous telephone conversations. To initiate a consult request, a requesting provider logs into the Virtual Hallway system and completes an electronic form detailing a patient-specific question. PCPs submitting a consult request can select and book a phone consultation with a specialist of their choosing. The service is offered at no cost to patients and providers. Fee-for-service specialists and family physicians are reimbursed using existing provincial billing codes, supporting integration into the current health care system. Consultations consist of brief phone calls, typically ∼10 min, followed by a consult report summarizing the advice given. The platform complies with all applicable Canadian health care privacy legislation, including the Personal Information Protection and Electronic Documents Act (PIPEDA) and relevant provincial privacy acts (Personal Health Information Act, Personal Health Information Protection Act, Health Information Act, etc.).
Study design
This was a cross-sectional survey conducted over two time periods to assess the acceptability and feasibility of peer-to-peer phone consultations among health care providers using the Virtual Hallway platform. The first survey period was from January 17 to March 6, 2024, and the second was from October 23 to November 25, 2024. Both surveys were conducted in PEI, Canada, and included participation from PCPs in PEI and specialists from both PEI and NS. The study conforms to the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines for cross-sectional, observational studies. 14
The survey aimed to assess the acceptability of the Virtual Hallway platform, the necessity and quality of subsequent in-person referrals, and the rationale behind selecting a specific specialist. Following each consultation, both the referring and consulting providers were prompted to complete closeout surveys embedded within the Virtual Hallway platform, reflecting their experience with the consultation. The surveys included a 5-point satisfaction rating scale, multiple-choice questions about specialist selection, and yes/no questions addressing referral impact and perceived care quality. The intervention incurred no direct costs to providers or patients due to existing billing codes other than ∼1–2 min reflecting the time required to complete the postconsult survey.
To increase the validity of the survey, face validity was established by incorporating feedback from both study investigators and platform users to ensure the questions were clear and relevant to clinicians and aligned with the local health care system. 15 Content validity was ensured through expert feedback, confirming that the survey comprehensively addressed key aspects of the consultation process. Finally, construct validity was considered in the development of the survey by reflecting on whether the questions reasonably captured key elements of platform use and provider experience, though no formal testing was performed.
Recruitment and respondent characteristics
A convenience sample was used to recruit participants from the entire population of interest. Eligible participants included PCPs in PEI and specialists from both PEI and NS. Inclusion criteria included physicians from applicable regions. Exclusion criteria included other provider groups, such as pharmacists and nurse practitioners. PCPs and specialists based in PEI were invited to participate on a voluntary basis, while NS-based specialists who were already registered on the Virtual Hallway platform were given the option to opt in. Data on individual usage duration outside of these time windows were not collected due to study Research Ethics Board (REB) restrictions. Data on the duration and frequency of platform use prior to survey participation were not captured. However, the two survey periods were designed to represent early and later phases of platform adoption, which likely correspond to varying levels of user experience. A formal sample size calculation was not conducted due to the exploratory nature of the study and the use of convenience sampling. Recruitment efforts included email, fax communications, and general information posted on the platform’s website. Informed consent for participation in the study was assumed through the acceptance of the platform’s terms and conditions and the disclosure introduction. By proceeding with the survey, participants acknowledged their consent to engage in the study. To protect participant privacy, no personally identifiable information was collected. The study was classified as a program evaluation and received an exempt letter from the relevant ethics board, in accordance with Chapter 2 of the Tri-Council Policy Statement guidelines.
Data analysis
Descriptive statistics were used to summarize participant demographics, user satisfaction ratings, referral avoidance rates, and motivations for specialist selection. We assessed data completeness by reviewing survey responses for missing or inconsistent entries and ensured accuracy through built-in survey logic, manual data cleaning, and descriptive checks to identify and address anomalies. Proportions and means with standard deviations (SD) were calculated for key variables. Variation within the data was examined by comparing survey responses across the two distinct time periods using chi-square tests to identify statistically significant differences in referral avoidance rates, specialist perceptions of referral necessity, and motivations for specialist selection over time. A significance threshold of p < 0.05 was applied. All statistical analyses were conducted using standard statistical software, and data were de-identified prior to analysis to maintain participant confidentiality.
Results
This study evaluated the use of the Virtual Hallway consultation platform during two separate periods: January 17 to March 6, 2024, and October 23 to November 25, 2024. Survey respondents included PCPs from PEI and specialists from both PEI and NS. In the first period, 46 PCP and 63 specialist survey responses were collected (N = 109). During this period, 76 unique participants actively used the platform, of whom 23 completed the survey (30% response rate). In the second period, there were 28 PCP and 44 specialist responses (N = 72), and 55 unique participants used the platform, 17 of whom completed the survey (31% response rate), with fewer active users in the second period due to its shorter duration. These numbers represent completed postconsultation surveys, not unique individuals, as some clinicians may have submitted multiple surveys for different consultations. The number of unique respondents in the first period was 23 PCPs and 63 specialists; in the second period, there were 17 unique PCPs and 22 unique specialists. There was no missing data identified. The analysis focused on three primary domains: (1) user satisfaction with the platform, (2) the platform’s influence on the necessity of formal in-person consultations, and (3) the rationale provided by PCPs for selecting specific specialists.
User satisfaction
At the initial time point, nearly all PCPs rated their satisfaction highly, with 98% indicating they were either “very satisfied” or “satisfied” (mean = 4.83, SD = 0.64).
Similarly, 92% of specialists reported being “very satisfied” or “satisfied,” with a mean rating of 4.61 (SD = 0.63).
At the follow-up time point, among PCPs, 100% reported being either “very satisfied” or “satisfied,” with a mean rating of 4.96 (SD = 0.19). Specialists also reported a high level of satisfaction, with 98% reporting “satisfied” or “very satisfied,” and a mean rating of 4.82 (SD = 0.45).
Considering that the user satisfaction was measured with a 5-point Likert scale, using a hypothesis mean value of 3, we performed one-sample t-tests on the data collected at both of the time points. The results showed that the higher than neutral mean in all of the data points was statistically significant (p < 0.05).
Impact on need for formal consultation
At time point 1, PCP survey results indicated that 85% (39/46) of phone consults in PEI resulted in the avoidance of an in-person referral (Table 1). Among the 15% of consults that did not avoid a referral, 29% of PCPs indicated that the consultation was intended to avoid a referral. Additionally, 71% of PCPs reported that the consultation improved the quality of the subsequent in-person referral, and 86% stated it enhanced the patient’s care while they awaited a specialist appointment.
Result of the Closeout Survey of Referring Physicians and Nurse Practitioners on Closing the Phone Consult
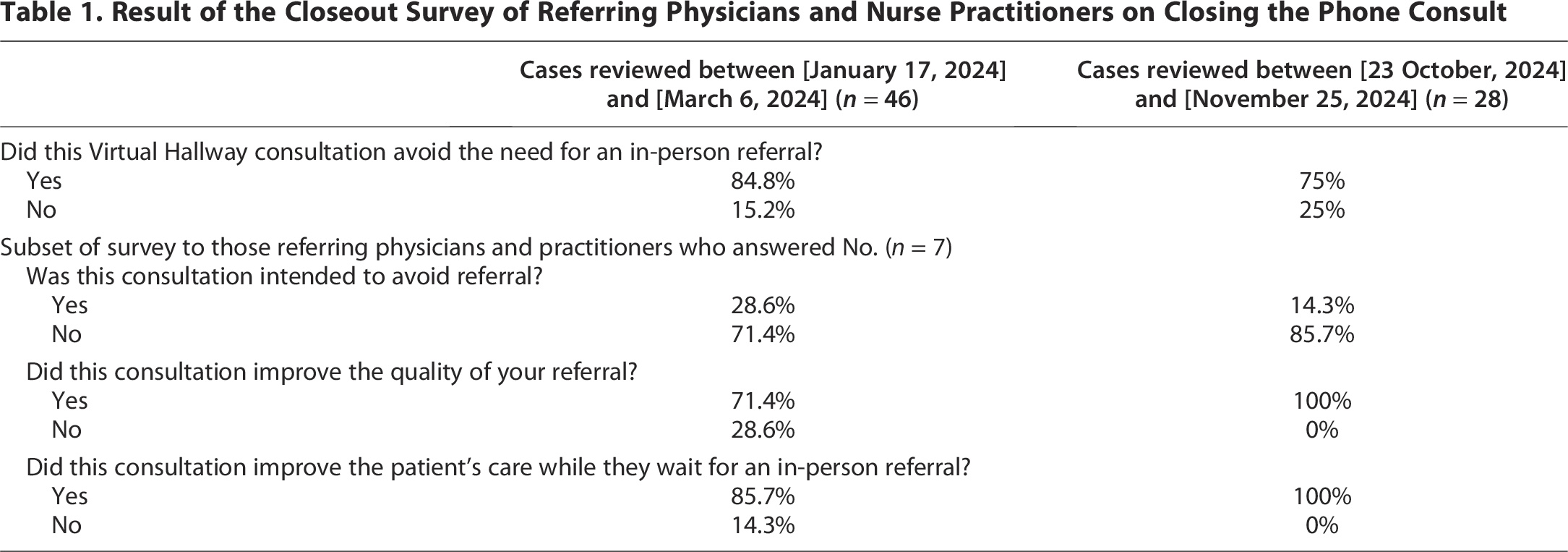
At time point 2, 75% (21/28) of phone consults avoided the need for an in-person referral. While the referral avoidance rate decreased slightly compared with time point 1, the difference was not statistically significant (chi-square test, χ2 = 0.54, p = 0.462). Of the remaining 25%, only 14% of PCPs indicated that the consultation was intended to avoid a referral. Importantly, at time point 2, 100% of PCPs stated that these consultations improved the quality of the subsequent in-person referral and enhanced the patient’s care while they awaited a specialist appointment.
At time point 1, specialists noted that 40% of consults reviewed would have been necessary or somewhat necessary if referred traditionally, while 44% were deemed unnecessary or somewhat unnecessary for in-person consultation (Table 2).
Result of the Closeout Survey of Specialist Consultants on Closing the Phone Consult

At time point 2, 66% of consultations were considered necessary or somewhat necessary for in-person referral, while 16% were deemed somewhat unnecessary or necessary for in-person referral. This reflects a higher perceived necessity for in-person consultations compared with time point 1. This shift was statistically significant (χ2 = 10.75, p = 0.03). The findings suggest an evolving pattern of use, with potentially more complex cases being referred through the platform at time point 2.
Motivations for specialist selection
A survey of PCP motivations for selecting specific specialists revealed notable shifts over time, reflecting an evolution in how the Virtual Hallway platform is utilized (Table 3).
Primary Care Providers’ Motivations for Selecting Specialists at Two Time Points

PEI, Prince Edward Island.
At time point 1, the top reason for selecting a specialist was their local availability within PEI (39%), followed by consultation time availability (33%), an established relationship (15%), and the specialty not being available on PEI (13%).
At time point 2, the specialty not being available on PEI became the most cited reason (39%), followed by consultation time availability (32%), local availability within PEI (18%), an established relationship (7%), and other reasons (4%).
The motivations for selecting a specialist showed significant differences between time points (χ2 = 8.74, p = 0.03).
A descriptive analysis of the specialist types involved during time point 1 (Table 4) and time point 2 (Table 5) shows that a wide range of specialties participated across both periods, with internal medicine, oncology-related specialties, and obstetrics and gynecology among the most frequently represented. The overall distribution shifted somewhat between periods, reflecting natural variation in consultation needs and available specialist capacity.
Specialist Respondent Distribution—First Time Period (January–March 2024)

Specialist Respondent Distribution—Second Time Period (October–November 2024)

Discussion
This study reinforces the sustained effectiveness of the Virtual Hallway platform in facilitating access to timely specialty care. Across two time points, the platform demonstrated consistent outcomes in referral avoidance, high satisfaction among users, and evolving patterns in specialist selection. These findings align closely with prior research in NS, suggesting that the model may have broader applicability.
Several evaluations of virtual consultation models internationally provide important context for interpreting these findings. Studies of Canadian eConsult systems have shown that asynchronous specialist consultation improves timeliness, reduces unnecessary referrals, and enhances communication between PCPs and specialists. 8 Similarly, evaluations from the U.S. Veterans Health Administration and NHS England have demonstrated that virtual specialist advice—whether synchronous or asynchronous—can significantly reduce wait times and improve system efficiency.9,10 Notably, emerging work examining synchronous, real-time teleconsultation models has reported comparable benefits, including rapid clinical clarification and improved decision-making in primary care. 12
While the study demonstrates a positive impact on avoiding in-person referrals and maintaining high levels of satisfaction, it is important to contextualize these findings within the broader landscape of health care in PEI and NS. The reduction in referral needs, particularly at time point 2, suggests that the platform has adapted to address more complex cases. This is further supported by the physicians’ usage pattern of the tool: The primary reason for specialist selection changed from local specialist availability to specialty not being available in their locality between the two time points. Notably, PCPs consistently reported that consultations improved the quality of subsequent in-person referrals when needed and enhanced patient care while awaiting specialist appointments. User satisfaction was another significant finding, with 98% of PCPs and 92% of specialists reporting that they were either “very satisfied” or “satisfied” with their consult experience. These high satisfaction rates underscore the platform’s acceptance and its perceived value among health care providers, further validating the platform’s utility in both PEI and NS.
The findings from this study in PEI align closely with those from the previous NS study, 13 reinforcing the confidence in the findings. Both studies demonstrated significant and similar referral avoidance rates, with PEI achieving an 81% average over both time points and NS having an 84% referral avoidance rate in the previous study. This consistency suggests that the platform is robust across different geographic and demographic contexts. Moreover, the high satisfaction rates among both PCPs and specialists in PEI mirror those observed in NS, indicating that the platform is well-received by health care providers in various settings.
A key new insight from this study is the successful implementation of cross-provincial consultations, allowing PEI PCPs to collaborate with NS specialists. The ability to tap into the broader pool of specialists in NS demonstrated the potential for the model to be used as a tool for bridging gaps in health care access across provincial borders. An analysis of how these in-person referrals compare with previous traditional referral rates in PEI and NS may provide additional context to the findings and help gauge whether the Virtual Hallway platform offers an improvement over the status quo. While specific referral rate data for PEI and NS are not readily available, a study by Liddy et al. 16 suggests that different primary care models impact referral patterns, with those in fee-for-service models tending to have lower referral rates compared with those in capitated models. This comparison could provide valuable insight into the potential advantages of peer-to-peer virtual consultation models in reducing unnecessary in-person referrals and improving health care access.
The impact of this model in PEI demonstrates its potential for broader adoption across Canada, particularly in rural regions. This aligns with recent efforts toward Pan-Canadian licensure, which aim to enhance provider mobility and improve access to care. 17 The model’s ability to significantly reduce the need for in-person referrals and maintain high levels of user satisfaction suggests that it could be a valuable tool in addressing health care access issues in other underserved areas.
To facilitate the expansion of peer-to-peer virtual care platforms like Virtual Hallway, several policy considerations need to be addressed. First, ensuring that adequate reimbursement models are in place is crucial for incentivizing and fairly reimbursing both PCPs and specialists to participate in such programs. Additionally, fostering cross-provincial collaborations, as demonstrated in this study between PEI and NS, should be a priority. Such collaborations can help provinces efficiently tap into the specialist resources of neighboring regions, thereby improving access to care without the need for significant infrastructure changes.
Expanding the use of peer-to-peer consultation platforms could enhance health care equity by ensuring timely specialist access, particularly in rural and remote areas where patients often face long wait times and significant travel burdens to access specialist services. 1 By providing a scalable solution to these challenges, these types of platforms can contribute to a more equitable health care system, where all Canadians have timely access to the care they need, regardless of their location.
More broadly, these findings add to a growing body of evidence supporting virtual consultation models as a means to address long-standing inequities in specialist access. Research across Canada, the United States, and Europe consistently shows that both synchronous and asynchronous virtual consultation systems can shorten wait times, improve communication, and support better care coordination.8–11 By demonstrating similar benefits within small, rural provinces and across interprovincial boundaries, this study contributes unique insight into how synchronous, phone-based consultation models can complement existing eConsult systems and enhance system capacity in geographically dispersed settings.
This study had several limitations. One potential limitation is the use of convenience sampling, which may introduce selection bias. Additionally, the voluntary nature of participation could lead to self-selection bias, where those more familiar with or favorable toward the platform may have been more likely to participate. The study also relied on self-report data, which can introduce response bias, as participants may have provided answers that reflect socially desirable outcomes or personal perceptions rather than objective measures. Another limitation is the small sample size, which may reduce the statistical power and the ability to detect small to moderate effects. Further limitations include the lack of data on participants’ prior platform use and the lack of data on participants’ practice setting. Consequently, differences in user experience between survey periods and practice settings could have influenced satisfaction and referral findings. Also, the study was conducted in specific regions, which may limit the generalizability of the findings. Future research should explore the long-term sustainability, broader applicability across diverse health care settings, and additional benefits of the Virtual Hallway platform—such as cost savings, patient outcomes, reduced wait times, and quality of care for complex cases.
Conclusion
This study contributes to the growing understanding of how synchronous, provider-to-provider virtual consultation models such as Virtual Hallway may help address challenges related to timely access to specialist input, particularly in regions with limited local specialist availability. The findings indicate that such platforms can support reductions in in-person referrals, facilitate timely clinical decision-making, and achieve high levels of provider-reported satisfaction. These outcomes are consistent with broader evidence suggesting that virtual consultation mechanisms can enhance communication between PCPs and specialists and improve overall care coordination.
The ability to enable cross-provincial consultation further illustrates how virtual models may help mitigate gaps in specialist distribution by allowing providers to access a wider range of expertise. Such approaches may therefore complement existing referral pathways and contribute to more flexible and responsive systems of care, especially in geographically dispersed regions where traditional access barriers persist.
As health care systems continue to explore scalable strategies to improve timely access to specialist services, virtual consultation platforms represent a potential component of a broader, multifaceted solution. Future implementation efforts should consider factors such as licensing frameworks, remuneration models, and integration within established clinical and administrative workflows. Ultimately, thoughtfully designed virtual consultation systems may play a meaningful role in supporting more equitable and efficient access to specialist expertise across diverse health care settings.
Authors’ Contributions
D.R.: Contributed to study design, data collection, data analysis, interpretation of results, and drafting of the article. A.A.: Contributed to study design, statistical analysis, data interpretation, and critical revision of the article. A.P.: Contributed to interpretation of findings, contextualization within health systems, and article revision for important intellectual content. K.C.: Provided clinical and health system expertise, facilitated access to PEI data, contributed to interpretation of results, and critically revised the article. J.C.: Conceived and supervised the study, coordinated project administration, contributed to data interpretation, and provided substantial revisions to the article.
Footnotes
Acknowledgments
The authors would like to acknowledge Health PEI for their support and the participating clinicians for their valuable contributions to this research.
Author Disclosure Statement
D.R., A.P., A.A., and J.C. are affiliated with Virtual Hallway, the company that provides the provider-to-provider phone consultation platform evaluated in this study. To mitigate potential bias, data collection and analysis were performed in accordance with STROBE guidelines, and interpretation of results was subject to independent review by a non–Virtual Hallway-affiliated co-author (K.C.). No other potential conflicts of interest are known.
Funding Information
No external funding or grants were received for this study. There was no material support beyond the standard resources of the authors’ respective affiliations.
Ethical Approval and Informed Consent
This study received an REB exemption letter from the Nova Scotia Health Research Ethics Board (REB FILE No. 1031075). It met the requirements outlined in the Tri-Council Policy Statement Chapter 2. Informed consent was deemed unnecessary and was not obtained, as the study involved the use of secondary anonymous data.
Data Availability Statement
Data available upon request.