
Abstract
This multicenter retrospective study evaluated the impact of social determinants of health (SDoHs) on presentation, management, and outcomes of basilar skull fractures (BSFs) across three Level 1 trauma centers in Arizona (2017–2022). A total of 502 adult patients with International Classification of Diseases, 10th Revision (ICD-10) defined BSF were included. Demographic and clinical variables—including age, sex, race, insurance status, housing status, and psychiatric or substance use history—were analyzed as proxies for SDoH. Multivariable regression models adjusted for comorbidity burden and extent of bone involvement. Motor vehicle collisions (45.0%) and falls (29.9%) were the most common mechanisms of injury. Most patients required Intensive Care Unit (ICU) admission (71.5%) and mechanical ventilation (45.0%), while 24.7% underwent surgical intervention. Complications occurred in 73.5% of patients, and in-hospital mortality was 13.1%. SDoHs were associated with differences in injury patterns and hospital course. Older patients were more likely to sustain fall-related injuries and had longer hospital stays, while younger patients more frequently sustained motor-vehicle-related injuries. Female patients were less likely to sustain assault-related injuries and less likely to require ICU admission. Non-White patients presented with more severe neurological injury and experienced longer ICU stays. Patients with private insurance had less severe presentations and shorter hospital and ICU stays compared with those with government insurance. No SDoH variables were associated with mortality. SDoHs significantly influence injury patterns and health care utilization in BSF. These findings highlight opportunities for targeted prevention and resource allocation to address disparities in neurotrauma care.
Introduction
Basilar skull fractures (BSFs), defined as fractures involving one or more bones that form the base of the skull, account for approximately 20% of all skull fractures. 1 The temporal bones are most commonly affected, although fractures may also involve the occipital, sphenoid, ethmoid, and the orbital plate of the frontal bone. Because BSFs typically result from substantial blunt force trauma and are strongly associated with traumatic brain injury (TBI), most existing literature examines BSFs within broader studies of TBI rather than as a distinct clinical entity.2,3
Prior studies of BSFs have largely focused on clinical signs or radiological findings as predictors of outcome or etiology of specific complications from BSF.4,5 However, the current literature provides limited characterization of demographic factors or comorbidities that may influence BSF incidence, presentation, or severity.
In studies of other traumatic injuries, social determinants of health (SDoHs) have increasingly been recognized as contributors to differences in treatment and outcomes. 6 Despite growing recognition of these disparities, the influence of SDoH on BSF incidence, characteristics, and outcomes remains poorly understood.
The objective of this retrospective study was to evaluate the relationship between selected SDoH and the etiology, characteristics, and outcomes of BSF among patients treated at Level 1 trauma centers in Arizona.
Methods
Patients
All trauma patients with an International Classification of Diseases, 10th Revision (ICD-10) diagnosis of BSF between January 2017 and December 2022 at three Level 1 trauma centers in Arizona were included. The full list of ICD-10 codes is provided in Supplementary Figure S1. Patients under 18 years of age and those deceased prior to hospital arrival or in the emergency department (ED) were excluded.
Primary and secondary outcomes
The aim of this study was to examine the relationship between SDoH and BSF at Level 1 trauma centers in Arizona.
Primary outcomes included mechanism of injury (MOI) and hospital course. Hospital course was defined by ED disposition, surgical versus nonsurgical treatment, and type of operative procedure performed. Additional outcomes included total length of stay, ventilator days, Intensive Care Unit (ICU) admission and ICU length of stay, in-hospital complications, and mortality.
Secondary outcomes characterized injury severity and included extent of bone involvement, specific bones affected, presence of concomitant TBI (e.g., cerebral contusion, subarachnoid hemorrhage, subdural hematoma, epidural hematoma, intraventricular hemorrhage, pneumocephalus, diffuse axonal injury, spinal cord injury, neck fracture, or facial fracture), and admission Glasgow Coma Scale (GCS), which was stratified into severe (≤8), moderate (9–12), and mild (13–15).
Data collection
Collected variables included age, gender, ethnicity, race, insurance status, housing status, and comorbidities. Psychiatric history and substance use were also recorded. Race/ethnicity, insurance status, and psychiatric/substance use history were used as proxies for SDoH.
Comorbidity burden was quantified using the Simple Disease Count method and grouped as 0 versus ≥1. Alcohol and drug screens on admission were categorized as positive, negative, or not tested.
Statistical analysis: Confounding variables
Comorbidity burden and total bone involvement were used as proxies for baseline health and injury severity.
Pearson chi-square testing assessed associations with outcomes. Variables significant across multiple outcomes were included as confounders in regression models. Certain SDoH variables were recoded to improve model stability (e.g., age groups, race dichotomized as White vs. non-White).
Both comorbidity burden and bone involvement were included as confounders due to their plausible relationships with injury severity and outcomes.
Statistical analysis: Main analysis
Logistic regression was used for dichotomous outcomes, with coefficients reported as odds ratios (ORs). Negative binomial regression was used for length of stay and ventilator days due to right-skewed distributions. Statistical significance was defined as p ≤ 0.05.
Some outcomes demonstrated perfect prediction. In these cases, small categories were excluded to allow model convergence. While penalized regression methods were considered, small sample sizes limited interpretability.
Ethics committee
This study received ethical approval from the University of Arizona Institutional Review Board (IRB), with the IRB number (approval #00002077) on November 2, 2023.
Results
Patient characteristics
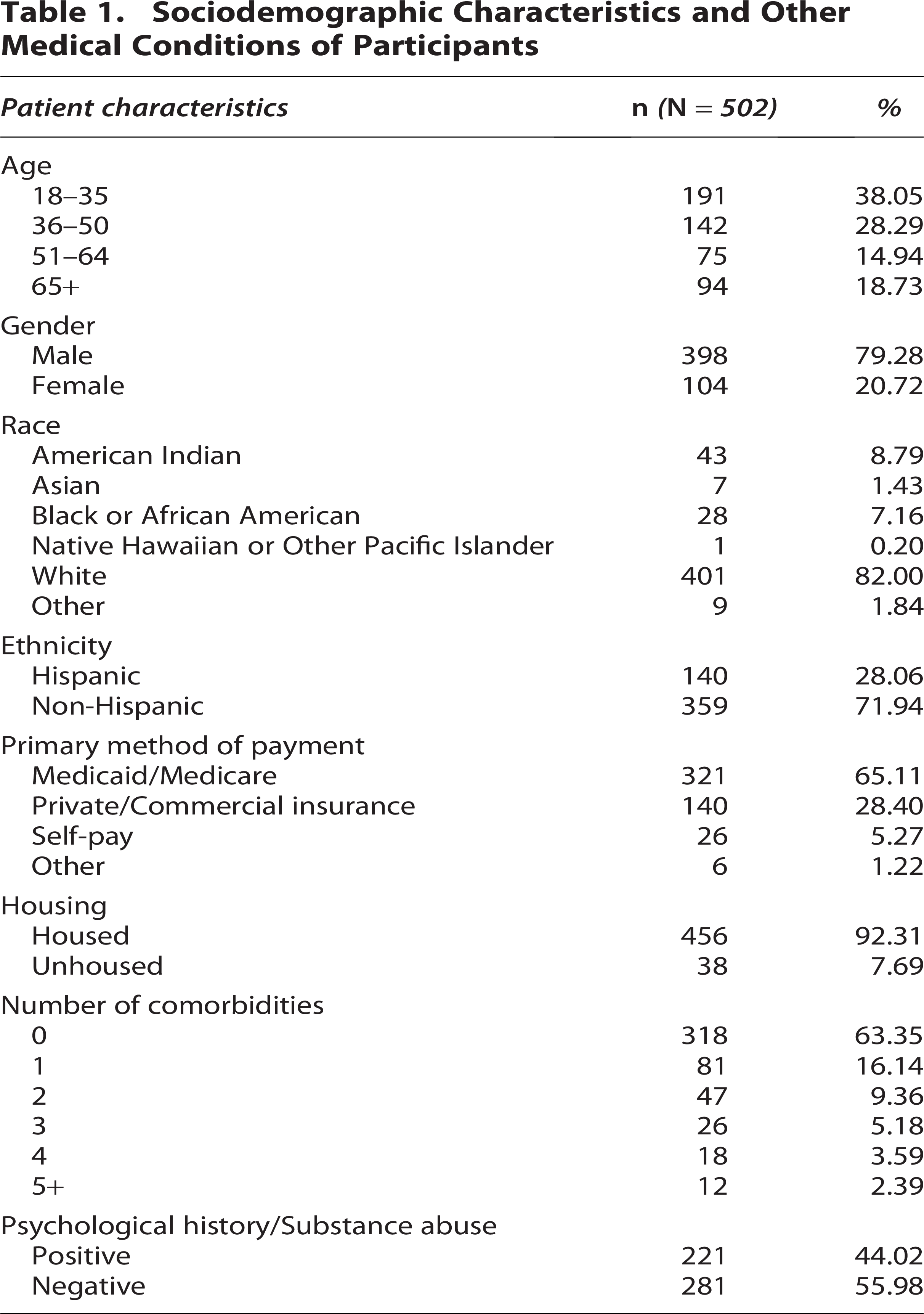
A total of 502 patients were included. Patients were predominantly aged 18–35 and 36–50 (38.05% and 28.29%) and male (79.28%). Most were White (82.00%) and non-Hispanic (71.94%), with American Indian patients representing the second largest group (8.79%).
Government insurance was most common (65.11%), followed by private insurance (28.40%). Most patients were housed (92.31%), with 38 experiencing homelessness.
The cohort was relatively healthy, with most patients having no chronic conditions (63.35%), although 44.02% had a history of psychiatric illness or substance use. Patient characteristics are summarized in Table 1.
Confounding variables
Comorbidity burden differed significantly for surgery, ED disposition, and ventilator days. Total bone involvement was associated with multiple outcomes, including management approach, procedures, length of stay (LOS), ICU metrics, and mortality. Given these findings, comorbidities and total bone involvement were treated as confounding variables in subsequent analyses.
Injury characteristics
Injury characteristics are summarized in Table 2.
Descriptive Statistics of Patient Upon Hospital Arrival, Emergency Department Disposition, Treatment, Length of Stays, Complications, and Mortality
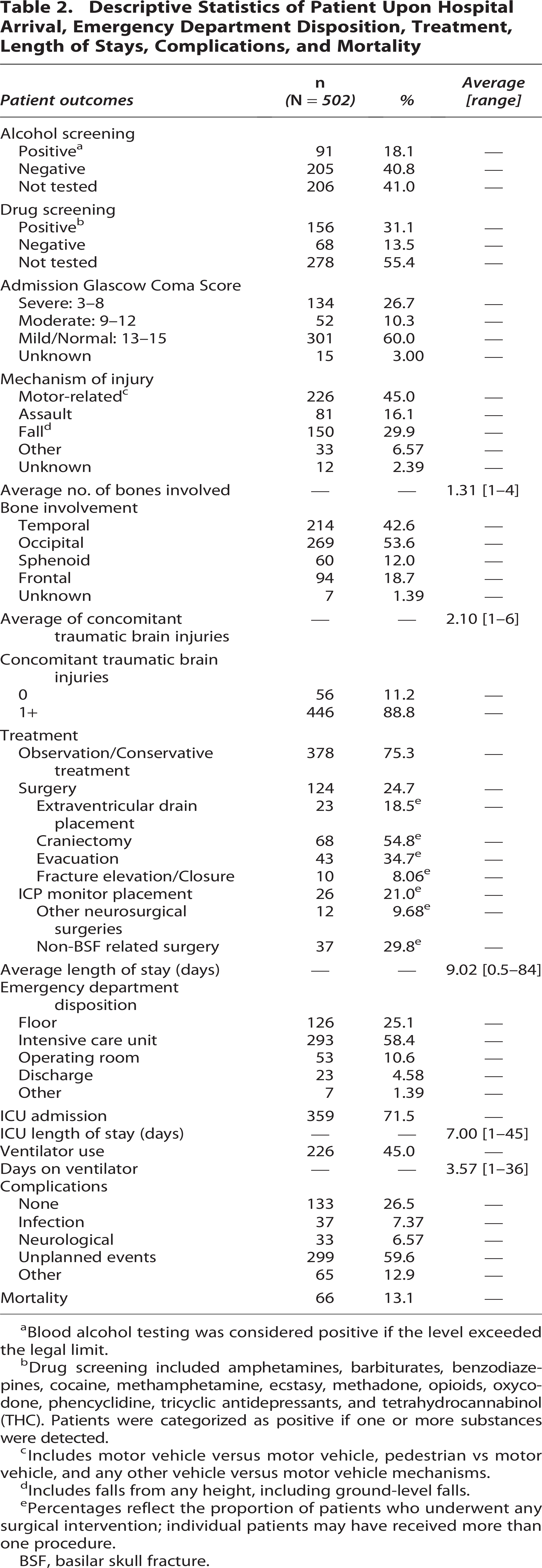
Blood alcohol testing was considered positive if the level exceeded the legal limit.
Drug screening included amphetamines, barbiturates, benzodiazepines, cocaine, methamphetamine, ecstasy, methadone, opioids, oxycodone, phencyclidine, tricyclic antidepressants, and tetrahydrocannabinol (THC). Patients were categorized as positive if one or more substances were detected.
Includes motor vehicle versus motor vehicle, pedestrian vs motor vehicle, and any other vehicle versus motor vehicle mechanisms.
Includes falls from any height, including ground-level falls.
Percentages reflect the proportion of patients who underwent any surgical intervention; individual patients may have received more than one procedure.
BSF, basilar skull fracture.
A substantial proportion of patients were not tested for substances (alcohol: 41.0%, n = 206; drugs: 55.4%, n = 278). Among those tested, positivity rates were higher for drugs than alcohol (31.1%, n = 156 vs. 18.1%, n = 91).
Motor vehicle–related incidents were the most common MOI (45.0%, n = 226), followed by falls (29.9%, n = 150) and assaults (16.1%, n = 81). Other mechanisms, including self-inflicted injuries, accounted for 6.6% (n = 33).
Most patients presented with mild or normal GCS scores (60.0%, n = 301), with severe cases more common than moderate (26.7%, n = 134 vs. 10.3%, n = 52).
Occipital and temporal bones were most frequently involved (53.6%, n = 269 and 42.6%, n = 214), while frontal and sphenoid fractures were less common (18.7%, n = 94 and 12.0%, n = 60). The majority of patients (88.8%, n = 446) had at least one concomitant TBI.
Hospital course statistics
Hospital course data are summarized in Table 2.
Following initial evaluation, most patients remained hospitalized, with 4.6% (n = 23) discharged home and 1.4% (n = 7) transferred. Over half were admitted directly to the ICU (58.4%, n = 293), while 25.1% (n = 126) were admitted to the general floor. The remaining 10.6% (n = 53) were taken to the operating room from the ED.
Mean hospital length of stay was 9.0 days (range 0.5–84). Overall, 71.5% (n = 359) required ICU admission at some point, with a mean ICU stay of 7.0 days. Management was primarily conservative, with 75.3% (n = 378) receiving noninvasive treatment (excluding intubation). Nearly half of patients (45.0%, n = 226) required mechanical ventilation, with a mean duration of 3.6 days.
Approximately one-quarter (24.7%, n = 124) underwent surgery. Common procedures included craniectomy (54.8%, n = 68), hematoma evacuation (34.7%, n = 43), Intracranial Pressure (ICP) monitoring (21.0%, n = 26), and Extraventricular Drain (EVD) placement (18.5%, n = 23). Other neurosurgical procedures were less frequent (9.7%, n = 12), while 29.8% (n = 37) underwent at least one non-BSF-related operation, most commonly fracture fixation or exploratory laparotomy in polytrauma.
Complications occurred in 73.5% (n = 369) of patients, most commonly unplanned events (58.8%, n = 295), primarily return to the OR (93.6%, n = 276). Less frequent events included unplanned intubation (4.4%, n = 13) and ICU readmission (2.0%, n = 6). Neurological complications occurred in 7.4% (n = 33), infections in 6.6% (n = 37), and other complications in 12.9% (n = 66). Overall in-hospital mortality was 13.1% (n = 66).
Age analysis
Across age groups, logistic regression demonstrated significant differences in MOI, ED disposition, hospital length of stay, ICU length of stay, and complications, while other characteristics and outcomes were similar (Table 3).
Logistic-Regression-Based Odds Ratios of Injury Characteristics and Patient Outcomes by Age Group and Gender
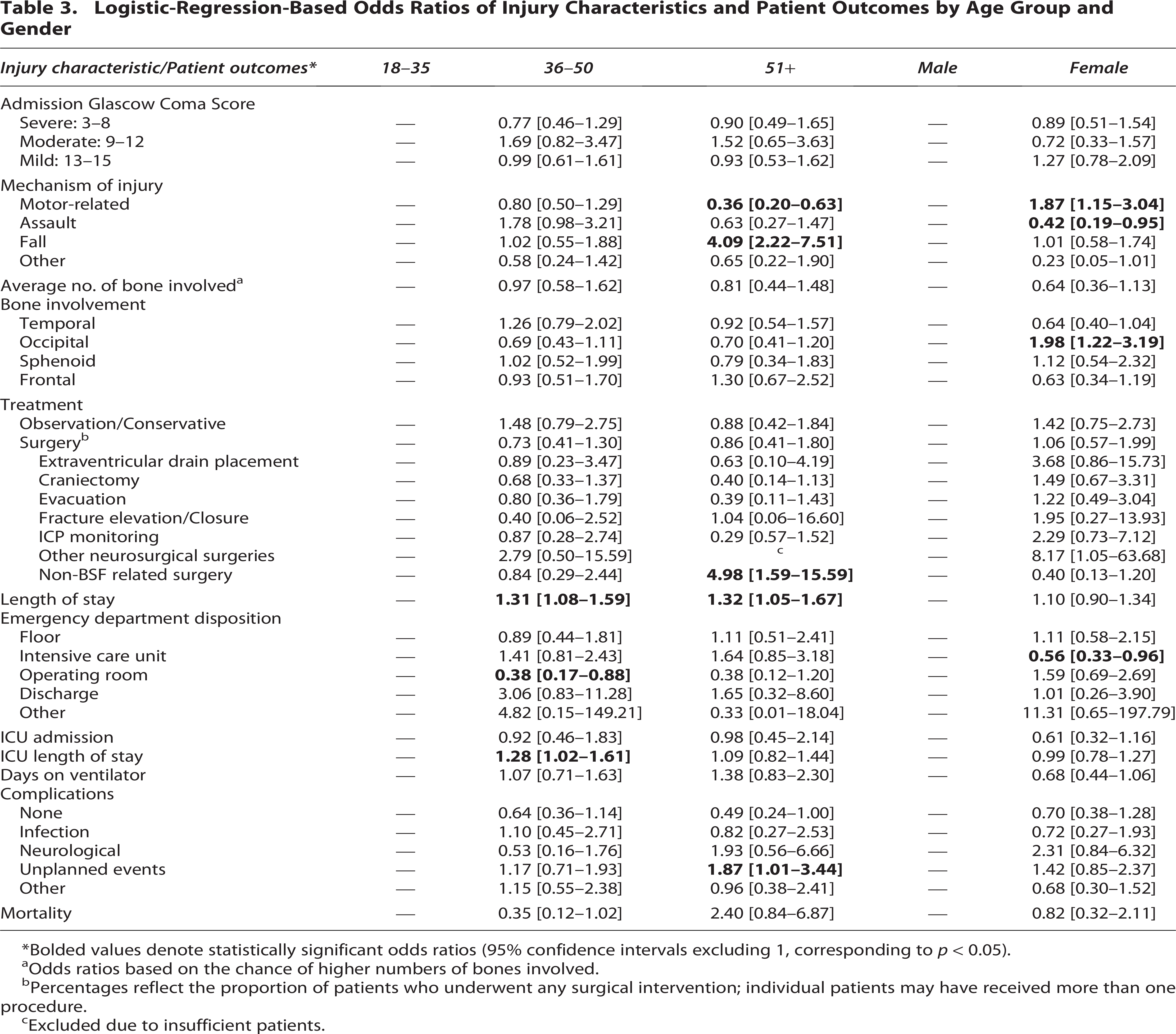
Bolded values denote statistically significant odds ratios (95% confidence intervals excluding 1, corresponding to p < 0.05).
Odds ratios based on the chance of higher numbers of bones involved.
Percentages reflect the proportion of patients who underwent any surgical intervention; individual patients may have received more than one procedure.
Excluded due to insufficient patients.
Patients aged ≥51 years were approximately four times more likely to sustain a fall (OR = 4.09; 95% CI: 2.22–7.51) and less likely to experience motor-vehicle-related injury (OR = 0.36; 95% CI: 0.20–0.63).
Patients aged 36–50 years were less likely to be taken directly to the operating room from the ED (OR = 0.38; 95% CI: 0.17–0.88) and had longer ICU stays (OR = 1.28; 95% CI: 1.02–1.61). Overall surgical rates did not differ significantly across age groups.
Hospital length of stay increased with age, with ORs of 1.31 (95% CI: 1.08–1.59) for patients aged 36–50 years and 1.32 (95% CI: 1.05–1.67) for those aged ≥51 years.
Gender analysis
Female patients were less likely to experience assault-related injury (OR = 0.42; 95% CI: 0.19–0.95) and more likely to sustain motor-vehicle-related injury (OR = 1.87; 95% CI: 1.15–3.04) compared with male patients.
Female patients were also less likely to be admitted to the ICU directly from the ED (OR = 0.56; 95% CI: 0.33–0.96) and had higher odds of occipital bone involvement (OR = 1.98; 95% CI: 1.22–3.19).
Otherwise, injury characteristics, management, and outcomes were comparable between genders (Table 3).
Race and ethnicity analysis
The main difference in race was GCS, with non-White patients twice as likely to present with severe scores (OR = 2.06; 95% CI: 1.19–3.57) and less likely to present with mild scores (OR = 0.58; 95% CI: 0.34–0.97).
Non-White patients were also less likely to be taken directly to the operating room from the ED (OR = 0.24; 95% CI: 0.08–0.74) and had longer ICU stays (OR = 1.33; 95% CI: 1.04–1.72), while surgical rates and overall ICU admission were similar between groups.
The only significant difference in ethnicity was in bone involvement, with Hispanic patients showing higher rates of temporal fractures (OR = 1.80; 95% CI: 1.16–2.80) and lower rates of occipital fractures (OR = 0.63; 95% CI: 0.41–0.99). Results are summarized in Table 4.
Logistic-Regression-Based Odds Ratios of Injury Characteristics and Patient Outcomes Based on Race and Ethnicity
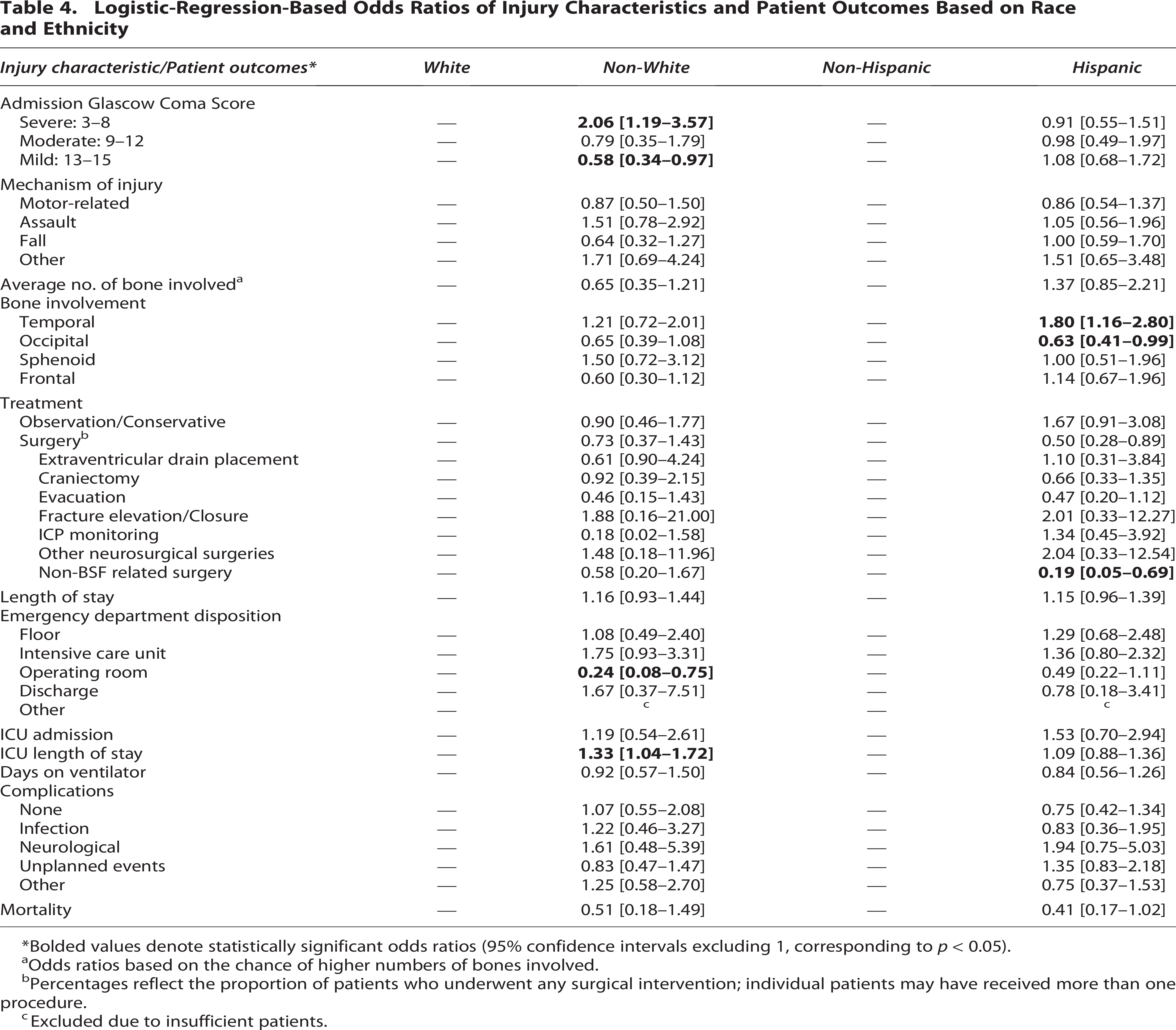
Bolded values denote statistically significant odds ratios (95% confidence intervals excluding 1, corresponding to p < 0.05).
Odds ratios based on the chance of higher numbers of bones involved.
Percentages reflect the proportion of patients who underwent any surgical intervention; individual patients may have received more than one procedure.
Excluded due to insufficient patients.
Socioeconomic analysis
Several differences were identified between patients with government-sponsored insurance and those with private insurance (Table 5). Privately insured patients were more likely to present with mild GCS (OR = 1.75; 95% CI: 1.12–2.73). They also had lower rates of assault (OR = 0.51; 95% CI: 0.27–0.97) and higher rates of falls (OR = 2.04; 95% CI: 1.25–3.33).
Logistic-Regression-Based Odds Ratios of Injury Characteristics and Patient Outcomes Based on Primary Payment Method and Housing Status
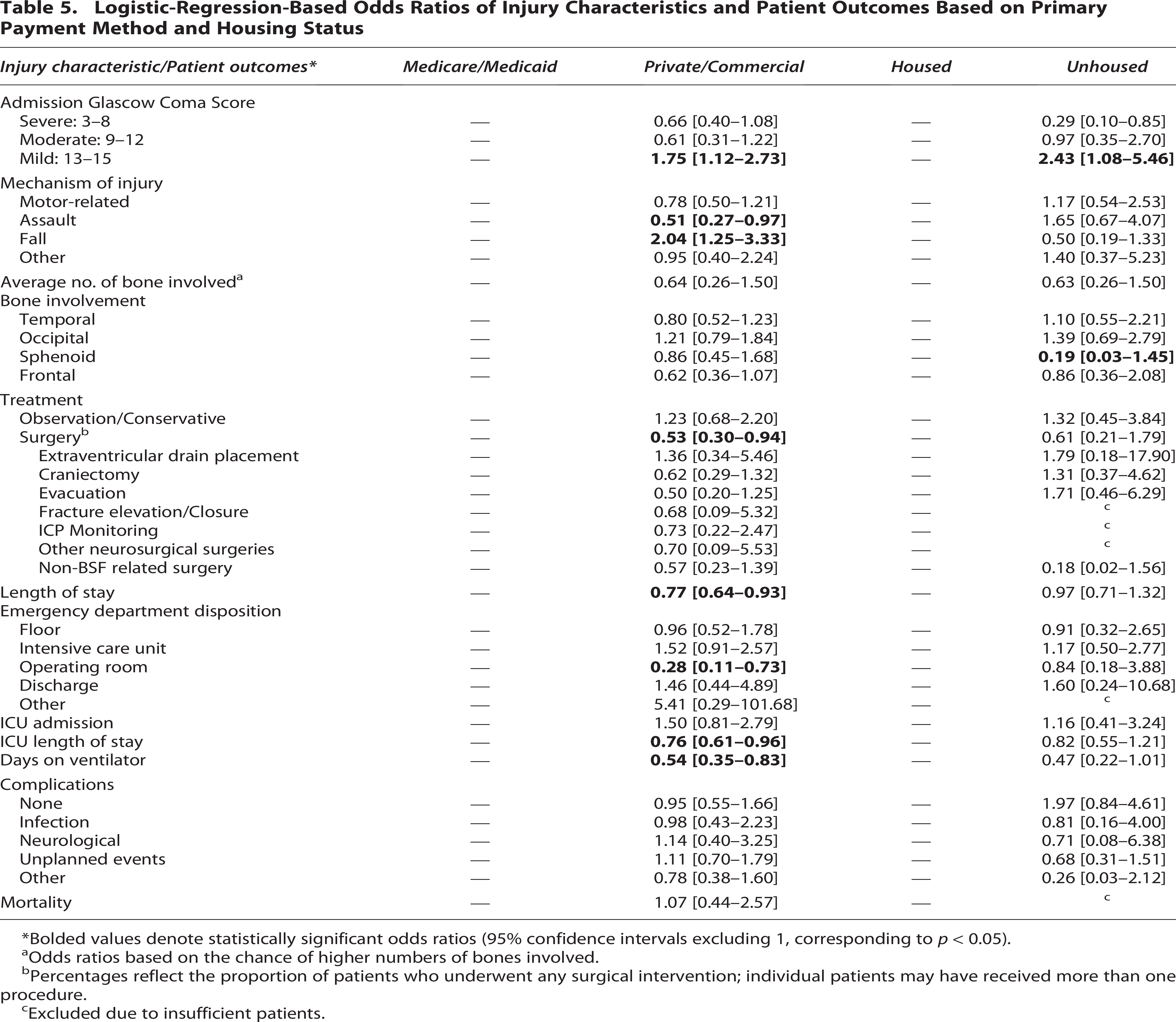
Bolded values denote statistically significant odds ratios (95% confidence intervals excluding 1, corresponding to p < 0.05).
Odds ratios based on the chance of higher numbers of bones involved.
Percentages reflect the proportion of patients who underwent any surgical intervention; individual patients may have received more than one procedure.
Excluded due to insufficient patients.
Privately insured patients demonstrated less complex hospital courses, including lower likelihood of surgery (OR = 0.53; 95% CI: 0.30–0.94), fewer operative ED dispositions (OR = 0.28; 95% CI: 0.11–0.73), shorter hospital stays (OR = 0.77; 95% CI: 0.64–0.93), shorter ICU stays (OR = 0.76; 95% CI: 0.61–0.96), and fewer ventilator days (OR = 0.54; 95% CI: 0.35–0.83), likely reflecting less severe initial presentation.
In housing analyses, several variables were excluded due to insufficient data (Table 5). However, unhoused patients were more likely to present with mild GCS (OR = 2.43; 95% CI: 1.08–5.46) and had lower rates of sphenoid bone involvement (OR = 0.19; 95% CI: 0.03–1.45).
Underlying medical condition analysis
Underlying medical conditions findings are summarized in Table 6.
Logistic-Regression-Based Odds Ratios of Injury Characteristics and Patient Outcomes Based on Comorbidities and History of Psychiatric or Substance Use Disorders
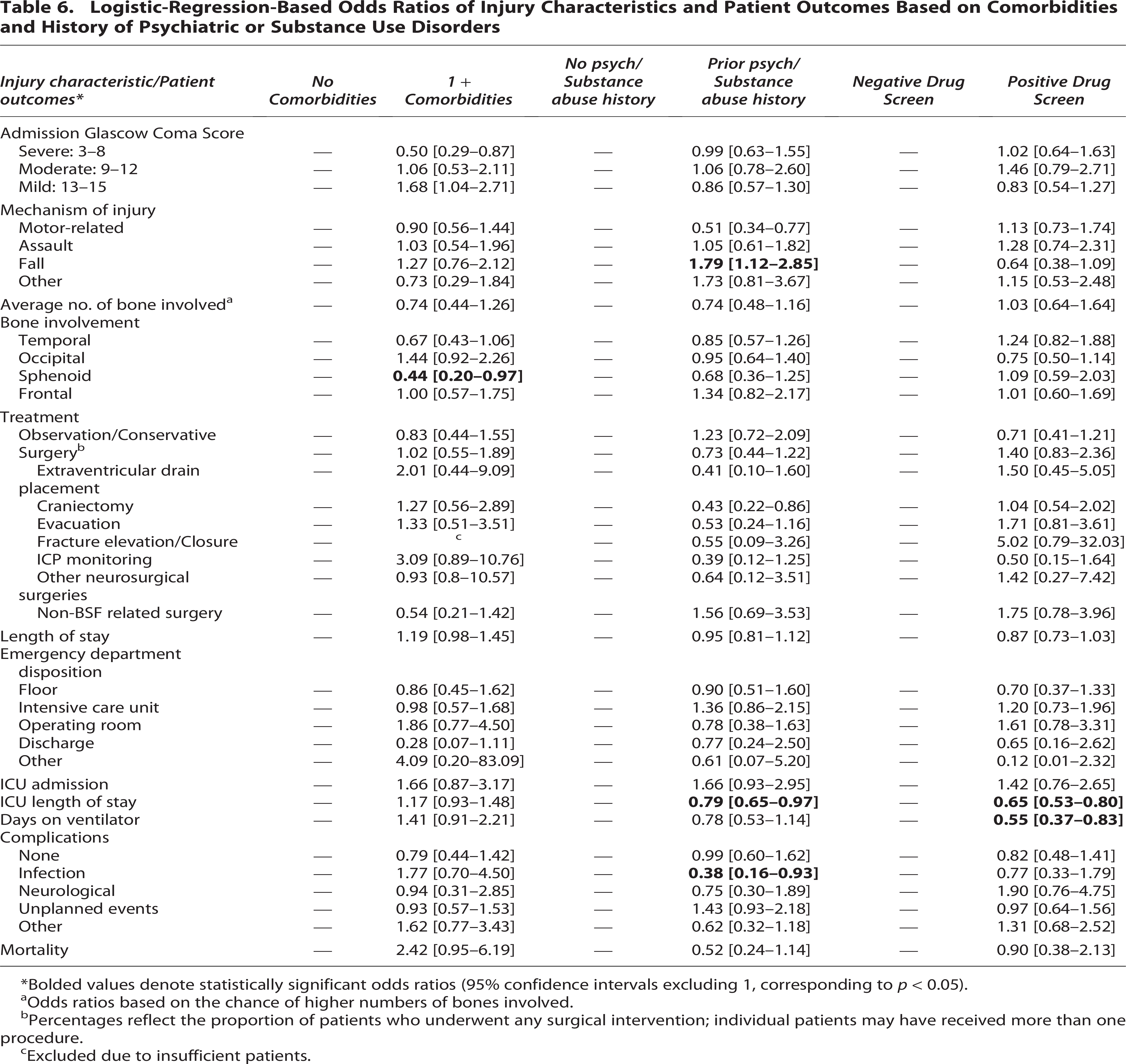
Bolded values denote statistically significant odds ratios (95% confidence intervals excluding 1, corresponding to p < 0.05).
Odds ratios based on the chance of higher numbers of bones involved.
Percentages reflect the proportion of patients who underwent any surgical intervention; individual patients may have received more than one procedure.
Excluded due to insufficient patients.
Sphenoid bone involvement was the only outcome significantly associated with comorbidity status, with patients having ≥1 comorbidity less likely to demonstrate sphenoid involvement (OR = 0.44; 95% CI: 0.20–0.97).
Patients with psychiatric or substance use history were more likely to sustain fall-related injuries (OR = 1.79; 95% CI: 1.12–2.85). This group also had shorter ICU stays (OR = 0.79; 95% CI: 0.65–0.97) and lower infection rates (OR = 0.38; 95% CI: 0.16–0.93), while ICU admission and other complication rates were similar.
Patients with a positive drug screen had shorter ICU stays (OR = 0.65; 95% CI: 0.53–0.80) and fewer ventilator days (OR = 0.55; 95% CI: 0.37–0.83), with no differences in ICU admission or other outcomes.
Mortality
There were no significant findings for mortality across all comparison groups.
Discussion
While prior studies have focused on epidemiology and outcomes of TBI, fewer have specifically evaluated BSF.7–16 By characterizing demographic, clinical, and socioeconomic predictors, our findings provide additional insight into BSF patterns and outcomes.
Age
Prior literature demonstrates a bimodal distribution, with younger men more affected by high-risk behaviors and older women more vulnerable due to falls and bone fragility.5,8,17 Our findings are consistent with this pattern, with younger patients more likely to sustain motor-vehicle-related injuries, while patients 51 and older more likely to sustain falls.
Older adults also demonstrated longer LOS and higher rates of unplanned events, consistent with prior TBI literature showing increased morbidity and worse outcomes in this population. 9 These disparities are likely influenced by comorbidities, frailty, and polypharmacy. 18
These findings highlight opportunities for targeted prevention strategies, including motor vehicle safety interventions in younger populations19,20 and fall-prevention efforts in older adults. 21
Gender
Consistent with prior studies reporting that 75–85% of cases occur in males, our cohort demonstrated a male predominance (79.3%).5,22 While females were less likely to sustain assault-related injuries, they were more likely to sustain motor-vehicle-related injuries.
This pattern may reflect biomechanical differences or limitations in current safety models, which are often based on male anthropomorphic data. Prior studies suggest that females may be more susceptible to certain injury patterns, including concussion, following motor vehicle collisions. 23
Several studies report higher mortality in men following TBI, including BSF, even among geriatric patients.16,24 In contrast, women experience more persistent postconcussive symptoms and worse functional outcomes despite lower injury severity.16,25 This was reflected in our cohort, where females were less likely to require ICU admission, suggesting less severe injury.
The biological basis of these differences remains unclear. Early studies suggested that estrogen and progesterone may have neuroprotective effects.26–31 Further research is needed to clarify these mechanisms.
Race and ethnicity
In our study, non-White patients were more likely to present with severe GCS scores on arrival and were less likely to undergo operative intervention, despite longer ICU stays and similar ICU admission rates.
Black patients have been reported to sustain TBI at higher rates than White patients, although findings on in-hospital mortality are mixed.13,15,32–34 Beyond the acute setting, both Black and Hispanic patients are less likely to be discharged to inpatient rehabilitation, a disparity associated with worse long-term functional outcomes.35,36 These differences are likely multifactorial, reflecting socioeconomic factors, access to postacute care, quality of care delivery, and structural inequities.
Housing status
Compared with housed patients, they were more likely to present with mild GCS scores. The higher likelihood of mild GCS despite similar mechanisms of injury is unclear but may reflect unmeasured factors such as delayed presentation, differences in prehospital triage, or underestimation of injury severity.
Housing status may influence both causes and outcomes of BSF. A temporal relationship has been described, with TBI increasing the risk of subsequent homelessness.14,37,38 Mechanisms of injury in unhoused populations also differ, with higher rates of assault and pedestrian–vehicle incidents.39,40 In addition, these patients often have a higher burden of comorbidities, including elevated rates of alcohol and substance use disorders, which complicate both acute management and recovery. 41
Outcome disparities in unhoused patients with TBI are well documented. These individuals experience longer hospital stays, higher rates of unplanned 30-day readmissions, increased risk of reinjury, and more frequent discharge to unstable housing, all contributing to poorer recovery and increased health care costs.42,43 These findings underscore the broader impact of SDoH on neurotrauma outcomes. Targeted interventions addressing housing instability show promise. A randomized trial found that providing stable housing to homeless adults with mental illness reduced violence-related TBIs. 44
Psychiatric comorbidities and substance use disorders
In our cohort, patients with a prior psychiatric or substance use history were more likely to sustain BSF following a fall and were more likely to require ICU admission. Infection rates were lower in this group despite higher ICU utilization. Patients with a positive toxicology screen had shorter ICU stays and fewer ventilator days, despite similar ICU admission rates and mechanisms of injury compared with those testing negative.
The relationship between substance use and TBI is well established as bidirectional, reflecting both increased risk of injury and higher rates of substance use following TBI. 45 Substance use is associated with increased TBI incidence, although rates may decline after injury, potentially due to provider counseling and prolonged hospitalization. 46
Given the higher incidence of fall-related injuries in this population, substance use represents a key target for intervention. Strategies such as counseling on injury risk, psychiatric referral, and fall-prevention measures have been described in prior studies and may help reduce recurrent injury.47,48
Insurance type
In our cohort, private insurance was one of the strongest predictors of both BSF presentation and outcomes. Privately insured patients were more likely to present with mild GCS, sustain injuries from falls rather than assaults, and experience shorter hospital and ICU stays with fewer ventilator days compared with those with government-based insurance.
These findings suggest that privately insured patients may have less severe neurological injury and less complex hospital courses. This likely reflects underlying socioeconomic differences, including access to preventive care, comorbidity burden, and postinjury rehabilitation resources.
Addressing these disparities will require policies that expand access to postacute care and promote equitable discharge planning. Understanding how financial and systemic factors influence neurotrauma care is essential to improving both efficiency and patient-centered outcomes.
Limitations
Its retrospective, observational design limits causal inference and is subject to incomplete or inaccurate documentation. Variables such as housing status, psychiatric history, and substance use may have been underreported or inconsistently recorded.
Although data were collected from multiple Level 1 trauma centers in Arizona, findings may not be generalizable to regions with different demographics or injury patterns. Some variables required category consolidation due to small sample sizes (e.g., race, comorbidity burden), which may have reduced analytic granularity.
Finally, this study was limited to in-hospital outcomes, and long-term neurological and functional outcomes were not assessed.
Given the number of statistical comparisons, the likelihood of false-positive findings is increased when using a threshold of p ≤ 0.05. Results should therefore be interpreted with caution, and future studies may benefit from methods that account for multiple testing, such as false discovery rate adjustment.
Conclusion
Overall, this study identifies several demographic and social associations with BSF incidence and outcomes. Age, gender, race, housing status, psychiatric history, substance use, and insurance type each appear to shape the presentation and course of BSF in distinct ways. Many of these are risk factors that represent targets for prevention and system-level reform. Future research should aim to validate these findings in multicenter cohorts and explore interventions that address not only the biological but also the structural drivers of neurotrauma disparities.
Transparency, Rigor, and Reproducibility Statement
This retrospective multicenter study was conducted at three Level 1 trauma centers and approved by the IRB (STUDY 00002077). The study was not preregistered. All adult patients with ICD-10 diagnoses of BSF from 2017–2022 meeting inclusion criteria were analyzed (n = 502), with predefined exclusion criteria applied.
Data were extracted from trauma registries using standardized methods. SDoH variables were defined a priori, and select variables were recoded to improve statistical stability. Analyses included chi-squared testing, nonparametric comparisons, logistic regression, and negative binomial regression, with comorbidity burden and injury severity included as confounders based on clinical relevance and statistical screening.
Due to the observational design, no randomization or blinding was performed. Missing data were handled by case-wise exclusion without imputation. Potential type I error from multiple comparisons is acknowledged.
Deidentified data are not publicly available but may be shared upon reasonable request and regulatory approval.
Authors’ Contributions
E.P.: Conceptualization, data curation, investigation, methodology, and writing—original draft. J.S.: Investigation, methodology, and writing—original draft. A.P.: Investigation, methodology, and writing—review and editing. J.B.: Investigation, visualization, and writing—original draft and review and editing. R.U., H.K., C.B., E.A., W.C., D.W., A.H., and K.W.: Investigation. K.J.: Formal analysis and software. P.N.: Conceptualization, supervision, and writing—review and editing.
Footnotes
Ethical Considerations
This is an IRB-approved retrospective study; all patient information was deidentified, and patient consent was not required. Patient data will not be shared with third parties.
Consent to Participate
The Ethics Committee of the University of Arizona IRB waived the need for ethics approval and patient consent for the collection, analysis, and publication of the retrospectively obtained and anonymized data for this noninterventional study.
Author Disclosure Statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding Information
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.