
Abstract
Frailty has emerged as an important predictor of postoperative complications across surgical fields, but its role in traumatic spinal fractures remains underexplored. This study evaluated the relationship between frailty, measured with the 5-item Modified Frailty Index (mFI), and in-hospital complications in a national cohort of patients with spinal fracture. A retrospective cohort study was conducted using the National Trauma Databank from 2017 to 2021, identifying adult patients with spinal fractures. Patients were classified as nonfrail (NF, mFI = 0), mildly frail (MF, mFI = 0.2), and severely frail (SF, mFI ≥ 0.4) according to the 5-item mFI. Multivariable logistic regression analysis was performed to assess the association between frailty and complications during the primary hospitalization for spinal trauma while adjusting for key covariates, including Glasgow Coma Scale (GCS), Injury Severity Score (ISS), spine region, spinal cord injury, concomitant head injury, surgical intervention, and hospital characteristics. The final cohort included 356,583 patients. 53.0% were classified as NF, 25.5% as MF, and 21.5% as SF. SF patients had higher odds of developing complications compared with NF patients (OR = 1.86, 95% CI: 1.77–1.96, p < 0.001). Complications such as cardiac events (1.3%), thromboembolism (1.1%), and pressure ulcers (0.6%) were more prevalent in frail patients. Lower GCS scores (GCS 3–8: OR = 3.19, 95% CI: 3.03–3.36, p < 0.001) and higher ISS scores (ISS 16–24: OR = 5.27, 95% CI: 5.02–5.53, p < 0.001) were associated with increased complication risk. Additionally, surgical intervention (OR = 2.84, 95% CI: 2.73–2.94, p < 0.001), the presence of spinal cord injury (OR = 2.73, 95% CI: 2.60–2.87, p < 0.001), and head injury (OR = 1.57, 95% CI: 1.52–1.63, p < 0.001) increased the likelihood of complications. Alongside the GCS and ISS, the 5-item mFI is an effective tool for identifying patients who may be at increased risk of in-hospital complications following traumatic spinal fractures. These findings highlight the importance of frailty assessment in spine trauma management and optimized patient care.
Keywords
Introduction
As the United States population becomes older and increasingly medically complex, frailty scores have been proposed as a method to quantify morbidity and mortality risk. Frailty, defined in the early 2000s as weight loss, weakness, exhaustion, slowness in movements such as walking, and low activity, increases risk for falls, disability, hospitalization, and death. 1 The modified Frailty Index (mFI) is a widely accepted measure in medical research to predict outcomes; it has been found to correlate with postoperative morbidity and mortality in several surgical subspecialties.2,3 Following elective spine surgery, more frail patients tend to experience longer lengths of stay (LOS), higher rates of nonhome discharge, and greater 30-day hospital readmission rates.4–8 While the mFI has been studied extensively in predicting outcomes of elective spine surgery, the 5-item mFI has not been as thoroughly investigated in operative or nonoperative spine trauma.5,6,8 In trauma, though patients cannot always be optimized before surgery, frailty assessments may inform management and recovery likelihood after invasive interventions.
As the incidence of trauma in older and more frail patients continues to increase, it will be necessary for health care workers in time-critical situations to have quick and reliable tools to triage patients for complication likelihood and to guide treatment decisions. This study aims to determine whether the 5-item mFI is a reliable predictor of complications in patients with traumatic spinal fractures. We hypothesize that more severe 5-item mFI scores will be associated with an increased frequency of complications after correcting for patient, injury, and treating facility characteristics.
Materials and Methods
Cohort selection
A retrospective analysis of the National Trauma Databank (NTDB) was performed including years 2017–2021. The NTDB, the largest United States trauma registry, is maintained by the American College of Surgeons. 9 The NTDB is a deidentified repository of trauma incidents tabulated from over 900 North American hospitals, which choose to participate. The present study was exempt from Institutional Review Board review as the NTDB is a publicly available deidentified dataset.
The NTDB contains patient diagnoses for the hospital admission in the form of International Classification of Diseases, Tenth Revision (ICD-10) codes. 10 Patients were screened for a vertebral fracture using diagnosis codes including stems S12.-, S22.0-, and S32.0-. Additional inclusion criteria were age > 18, blunt injury, and treatment at a level I or II trauma center. Exclusion criteria included penetrating or other mechanisms of injury, hospital arrival without signs of life, Injury Severity Score (ISS) classified as very severe (greater than or equal to a score of 25, due to an inherently high complication rate rather than frailty), and missing data for variables included in multivariate regression. 11
mFI calculation
The 5-item mFI is composed of hypertension, diabetes mellitus, congestive heart failure, chronic obstructive pulmonary disease, and dependency on others for completing activities of daily living (functionally dependent status). 12 Patients receive one point for a history of any of the five comorbidities, and the total score is divided by 5. Patients were designated as being nonfrail (NF) if their mFI was 0, as mildly frail (MF) if their mFI was 0.2, and severely frail (SF) if their mFI was > 0.4.
Covariates
Patients were determined to have a cervical injury if they had a diagnosis code of S12.-, a thoracic injury if they had a diagnosis code of S22.0-, or a lumbar injury if they had a diagnosis code of S32.0- (Table 1). Concomitant spinal cord injury was determined using codes S14.0, S14.1, S24.0, S24.1, S34.0, or S34.1. Patients were categorized into those with initial Glasgow Coma Scale scores (GCS) of 3–8, of GCS 9–11, and of GCS 12–15 at hospital presentation to determine the severity of altered consciousness. 13 Patients with an ISS of 1–8 were considered minor, a score of 9–15 were considered moderate, and a score of 16–24 were considered severely injured. 14 ICD-10 procedure codes were used to determine whether patients underwent surgery during the primary hospitalization (Table 1). The presence of a concomitant head injury was screened using ICD-10 diagnosis codes S02- or S09-. Hospital teaching status was recorded as nonteaching, community, or academic, which included academic and university medical centers. Hospital type (for-profit, not for-profit, or government) and trauma center level (I or II) were also determined.
ICD-10 Diagnosis Codes Used to Screen Patients for a Spinal Fracture, as Well as ICD-10 Codes Used to Screen Patients with Spinal Cord Injury, Head Injury, and Spinal Surgery
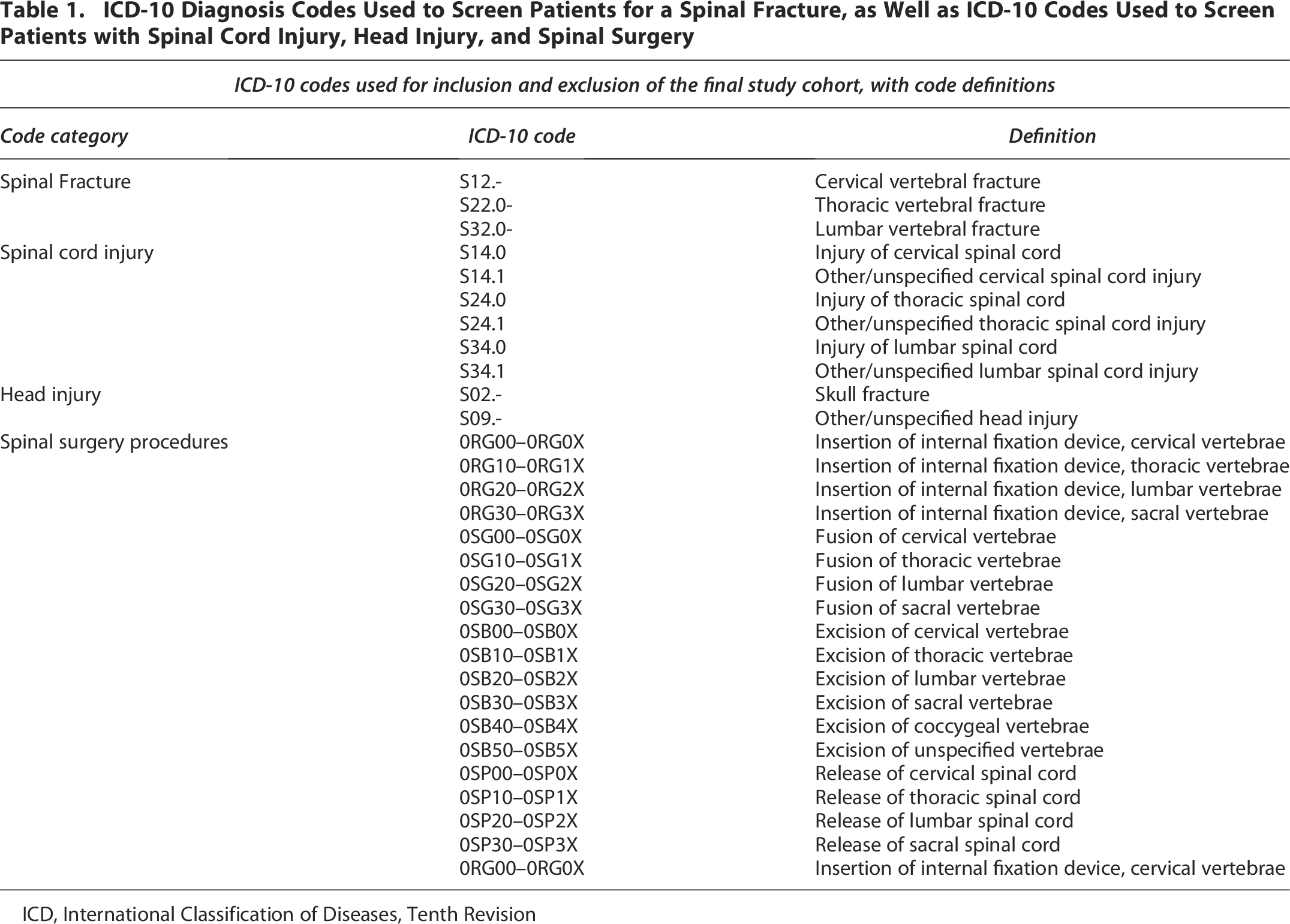
ICD, International Classification of Diseases, Tenth Revision
The NTDB records binary data regarding in-hospital complications during the primary hospitalization. Complications included pressure ulcer development, renal injury, unplanned return to the operating room, respiratory complication, catheter-associated urinary tract infection (CAUTI), deep surgical site infection (SSI), superficial SSI, organ space SSI, extremity compartment syndrome, central line-associated bloodstream infection, and osteomyelitis. Two additional composite complication variables were created: cardiovascular complications, including cardiac arrest, myocardial infarction (MI), and/or cerebrovascular accident (CVA), and venous thromboembolism (VTE) complications, including deep vein thrombosis and/or pulmonary embolism.
Various covariates were analyzed for their correlation with complication development. Patient demographics included age and sex. The presence of a spinal cord injury (SCI) and concomitant head injury were selected as complications may be more likely in polytrauma patients. GCS and ISS were selected as patients with more severe injuries may be more likely to develop a complication. The spine region, mechanism, and intent of the injury were selected as these different modalities of injury may confer different recovery patterns. Hospital characteristics, including the hospital type, teaching status, and verification level, were selected as they may affect the availability of specialized care and resources. Lastly, evaluating the impact of surgical versus non-surgical management assessed potential risks and benefits associated with different treatment approaches.
Outcomes
Our primary outcome variable was the presence or absence of in-hospital complications following spine fracture. We additionally determined whether other injury-associated factors, such as lower initial GCS, higher ISS, or hospital characteristics, were predictive of complications following spine fracture.
Statistical analysis
Descriptive statistics were calculated for the entire cohort and for patients stratified by mFI group. Continuous variables were presented as means with standard deviation, ordinal variables were presented as medians with first and third interquartile ranges (IQR), and categorical variables were presented as frequencies and percentages. Differences among mFI groups for continuous variables were analyzed using one-way analysis of variance with Tukey’s HSD post hoc testing. Differences in categorical variables were assessed using Chi-square testing with Bonferroni corrections for multiple comparisons. A standard alpha of 0.05 was used as a threshold for significant correlation.
mFI category as a predictor of the development of any complication was determined through calculation of an odds ratio (OR) and a 95% confidence interval (CI). Similar analyses were also conducted for GCS and ISS categories, respectively. A multivariable logistic regression was then conducted, including patient- and hospital-level factors, which were hypothesized to predict complication development. These variables included patient age, sex, mFI category, spine region of injury, presence of a SCI, concomitant head injury, surgical intervention, GCS category, ISS category, mechanism of injury, and intent of the injury, as well as hospital type, teaching status, and trauma center verification level. The model’s goodness of fit was assessed through the Akaike information criterion (AIC). All statistical analyses were conducted in R (R version 4.4.0; R Foundation for Statistical Computing, Vienna, Austria).
Results
Cohort descriptive statistics
Among 5,481,046 patients in the NTDB from years 2017 to 2021, 356,583 (6.5%) patients had a traumatic spinal vertebral fracture and met all inclusion criteria (Fig. 1). The median age was 58 (IQR: 38–73) years and 219,749 (61.6%) were males. Most (277,047, 77.7%) patients identified their race as white and did not identify their ethnicity as Hispanic or Latino (320,317, 89.8%). 189,005 (53.0%) patients were classified as NF, 90,835 (25.5%) patients were MF, and 76,743 (21.5%) patients were SF. Lumbar injuries were most common (151,443, 42.5%), followed by thoracic (104,583, 29.3%) and cervical injuries (100,557, 28.2%). The median initial GCS was 15 (IQR: 15–15) and the median ISS was 8 (IQR: 5–13). 191,259 (53.6%) patients had minor injuries, 104,466 (29.3%) patients had moderate injuries, and 60,858 (17.1%) patients had severe injuries. The median hospital LOS was 5 (IQR: 3–9) days, and 45,849 (12.8%) patients underwent surgical intervention. The most common complications included cardiac complications (4,507, 1.3%), VTE (4,055, 1.1%), and pressure ulcers (2,294, 0.6%; Fig. 2).
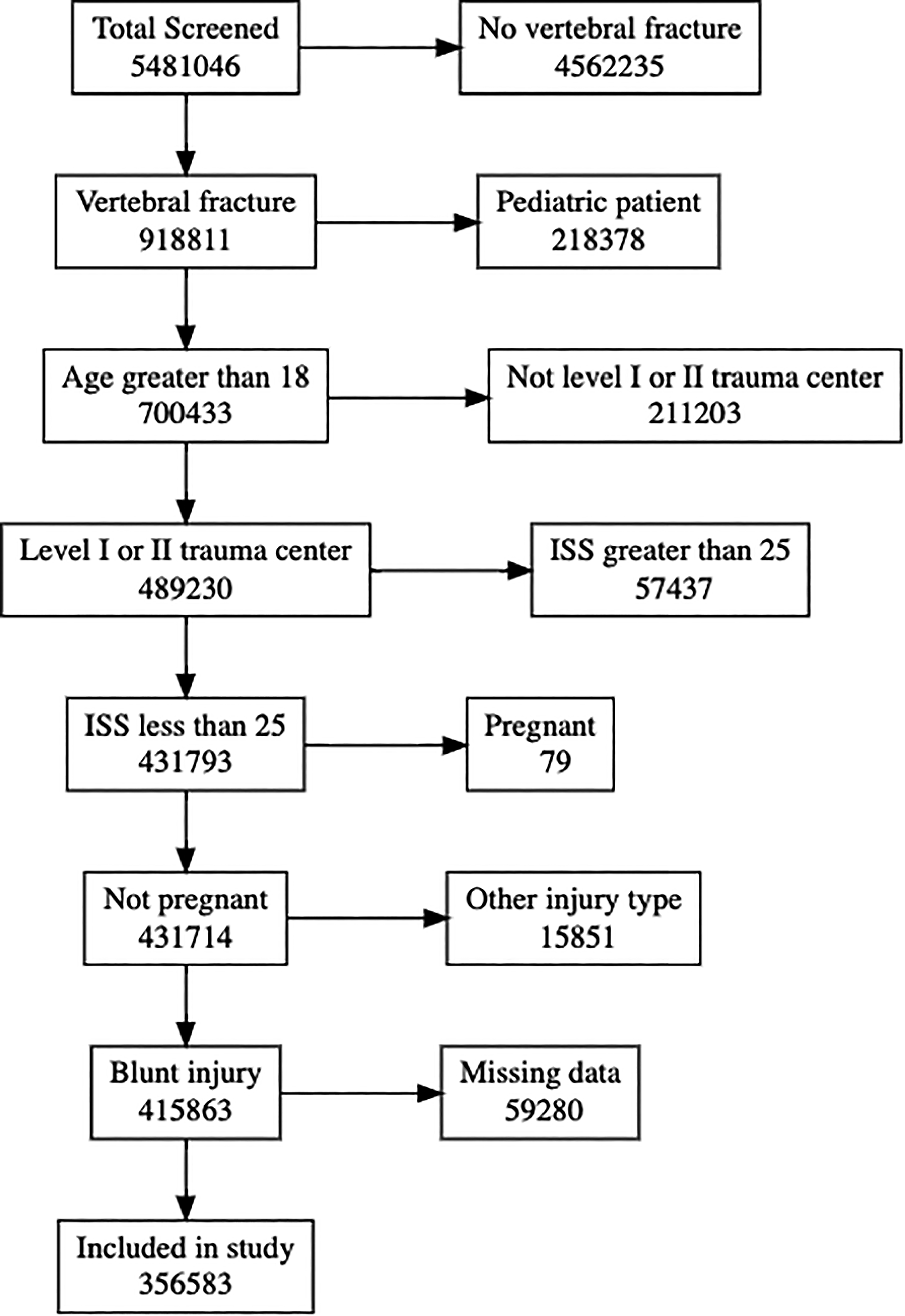
Flow diagram demonstrating the final cohort selection and how many patients were excluded for each inclusion and exclusion criterion. The number of patients in each box on the left represents the number of patients included, and the number of patients in each box on the right represents the number of patients excluded for each exclusion criterion. ISS, Injury Severity Score.

The frequency of each complication during the primary hospitalization for spine trauma stratified by level of frailty as determined by the mFI. Cardiac complications include stroke, myocardial infarction, and cardiac arrest. CAUTI, catheter-associated urinary tract infection; CLABSI, central line-associated blood stream infection; DVT, deep vein thrombosis; OR, operating room; PE, pulmonary embolus; SSI, surgical site infection.
Patient demographics
The mean age was significantly different among mFI groups (F [2, 356,580] = 101,592, p < 0.001; Table 2) with SF patients having the highest mean age (SF: 72.1 ± 12.0 vs. MF: 66.0 ± 15.3 vs. NF: 44.5 ± 18.2 years). There was a greater proportion of males (χ2 [2,N = 356,583] = 4,003.8, p < 0.001; SF: 54.4% vs. MF: 57.9% vs. NF: 66.3%) and non-white patients (χ2 [10,N = 356,583] = 4,838.1, p < 0.001; SF: 17.2% vs. MF: 18.0% vs. NF: 26.5%) in the NF group. More NF patients had lumbar injuries compared with MF and SF patients (χ2 [4,N = 356,583] = 1,197.4, p < 0.001; SF: 38.9% vs. MF: 40.2% vs. NF: 44.9%). NF patients had a higher rate of SCI compared with MF and SF patients (χ2 [2,N = 356,583] = 263.4, p < 0.001; SF: 5.1% vs. MF: 5.9% vs. NF: 6.7%). There was a significantly greater proportion of SF patients with GCS 12–15 when compared with MF and NF patients (χ2 [4,N = 356,583] = 1,938.1, p < 0.001; SF: 96.2% vs. MF: 95.6% vs. NF: 92.6%), and there was a greater proportion of SF patients with minor injuries on the ISS (χ2 [4,N = 356,583] = 9,729.9, p < 0.001; SF: 66.0% vs. MF: 57.2% vs. NF: 46.9%).
Patient Demographics and Baseline Characteristics Stratified by mFI Category

GCS, Glasgow Coma Scale; ISS, Injury Severity Score; mFI, modified Frailty Index.
Treating hospital characteristics
A significantly lower proportion of SF patients were treated at an academic hospital (χ2 [4,N = 356,583] = 104.7, p < 0.001; SF: 50.1% vs. MF: 51.3% vs. NF: 52.2%) and at a level I trauma center (χ2 [2,N = 356,583] = 9.1, p = 0.011; SF: 63.3% vs. MF: 63.4% vs. NF: 63.8%) compared with MF and NF patients. A higher proportion of SF patients were treated at a nonprofit hospital (χ2 [4,N = 356,583] = 71.4, p < 0.001; SF: 89.2% vs. MF: 88.5% vs. NF: 88.5%).
Univariate predictors of complication development
When compared to NF patients, MF patients (OR = 1.30, 95% CI: 1.25–1.35, p < 0.001) and SF patients (OR = 1.67, 95% CI: 1.61–1.74, p < 0.001) had greater likelihood of developing a complication (Fig. 3). A significantly greater proportion of SF patients developed any complication during the primary hospitalization when compared with MF and NF patients (χ2 [4,N = 356,583] = 678.0, p < 0.001; SF: 5.7% vs. MF: 4.5% vs. NF: 3.5%). SF patients had higher rates of complications, including CAUTI, renal injury, respiratory complications, sepsis, pressure ulcer, and cardiac complications (Table 3). Conversely, a smaller proportion of SF patients developed extremity compartment syndrome or had to return to the operating room when compared with MF or NF patients.

The percentage of patients with and without any complication during the primary hospitalization for spinal trauma, stratified by modified Frailty Index (mFI) category. Odds ratios represent the development of any complication. MF, mildly frail; NF, not frail; SF, severely frail.
Complications Developed during Primary Hospitalization Stratified by mFI Category

CLABSI, central line-associated bloodstream infection; CAUTI, catheter-associated urinary tract infection; DVT, deep vein thrombosis; OR, odds ratio; PE, pulmonary embolism; SSI, surgical site infection.
Male patients were more likely to develop a complication when compared to females (OR = 1.57, 95% CI: 1.51–1.62, p < 0.001). When compared with patients with initial GCS 12–15, patients with GCS 9–11 (OR = 3.47, 95% CI: 3.19–3.79, p < 0.001) and with GCS 3–8 (OR = 5.09, 95% CI: 4.85–5.33, p < 0.001) were more likely to develop a complication. Similarly, when compared to patients with minor injuries, patients with moderate (OR = 2.51, 95% CI: 2.40–2.62, p < 0.001) or severe injuries (OR = 5.98, 95% CI: 5.73–6.23, p < 0.001) were more likely to have a complication. The presence of a head injury (OR = 1.57, 95% CI: 1.52–1.63, p < 0.001) or a SCI (OR = 3.60, 95% CI: 3.44–3.76, p < 0.001) increased the likelihood of complications. Patients who underwent surgery were also more likely to have a complication compared with those who did not (OR = 2.84, 95% CI: 2.73–2.94, p < 0.001).
Treatment at a nonteaching (OR = 0.80, 95% CI: 0.76–0.84, p < 0.001) or a community hospital (OR = 0.93, 95% CI: 0.89–0.96, p < 0.001) reduced the likelihood of complications when compared to treatment at an academic hospital. Treatment at a level II trauma center also reduced the likelihood of complication development compared with treatment at a level I center (OR = 0.82, 95% CI: 0.79–0.85, p < 0.001). Hospital type was not a significant predictor of complications.
Multivariable regression analysis
Multivariate logistic regression was performed for the likelihood of complication development. The overall model was significantly predictive (p < 0.001) with an AIC of 108,678. For every additional year of age, the odds of complications increased by 1.7% (OR = 1.017; 95% CI: 1.016–1.018; p < 0.001). Males had 40% higher odds of complications compared to females (OR = 1.40; 95% CI: 1.35–1.45; p < 0.001). MF (OR = 1.29; 95% CI: 1.23–1.35; p < 0.001) and SF (OR = 1.86; 95% CI: 1.77–1.96; p < 0.001) patients were significantly more likely to develop a complication when compared with NF patients. Thoracic spine injuries were associated with slightly lower odds of complications compared with cervical spine injuries (OR = 0.95; 95% CI: 0.90–0.99; p = 0.013), with no difference in complication risk for patients with lumbar injuries. A concomitant SCI was associated with complications, increasing the odds by 69% (OR = 1.69; 95% CI: 1.60–1.78; p < 0.001). Surgical intervention was associated with more than doubled odds of complications (OR = 2.36; 95% CI: 2.26–2.47; p < 0.001). Presence of concomitant head trauma was protective, reducing odds by 18% (OR = 0.82; 95% CI: 0.79–0.85; p < 0.001).
Patients who sustained self-inflicted injuries (OR = 1.28; 95% CI: 1.04–1.58; p = 0.021) or injuries with intent classified as “other” (OR = 2.54; 95% CI: 1.78–3.63; p < 0.001) were more likely to develop a complication when compared with patients with unintentional injuries. Patients in motor vehicle traumas were more likely to develop a complication than patients who fell (OR = 1.22; 95% CI: 1.17–1.27; p < 0.001). Hospital arrival with GCS 9–12 (OR = 2.66; 95% CI: 2.43–2.92; p < 0.001) or GCS 3–8 (OR = 3.63; 95% CI: 3.45–3.83; p < 0.001) increased the likelihood of developing a complication when compared with patients with GCS 12–15. Similarly, patients with moderate (OR = 2.49; 95% CI: 2.38–2.61; p < 0.001) or severe (OR = 5.70; 95% CI: 5.42–5.99; p < 0.001) injuries on the ISS were more likely to develop a complication compared with patients with minor injuries.
Treatment at a community hospital was associated with increased risk of complication development when compared with academic hospitals (OR = 1.12; 95% CI: 1.07–1.16; p < 0.001), though there was no difference when compared with nonteaching hospitals. Treatment at a level II trauma center was associated with decreased odds of developing a complication when compared with treatment at a level I center (OR = 0.90; 95% CI: 0.86–0.95; p < 0.001). Hospital type was not a significant predictor.
Discussion
Using NTDB data from 2017 to 2021, this study found that higher 5-item mFI scores, lower GCS, and greater injury severity were all associated with an increased likelihood of in-hospital complications after traumatic spinal fracture. These results show the 5-item mFI, quickly calculated from commonly data, stratifies complication risk after traumatic vertebral fracture alongside injury severity. While the use of national de-identified data carries inherent limitations, this study benefits from a large patient sample size from a diverse geographic distribution with varied practice patterns. As the rates of spinal injury continue to increase among an aging population, the 5-item mFI may be an additional useful tool in devising a treatment plan during patient triage and hospital admission.
Cardiac complications, including MI, CVA, and cardiac arrest, as well as VTE and pressure ulcers were the most common complications. Heart failure correlates with frailty, and spine trauma may worsen pre-existing conditions, leading to in-hospital cardiac complications. 15 Additionally, patients with greater premorbid frailty, who likely have longer hospital LOS and diminished functional recovery, may be more likely to develop VTE and pressure ulcers from prolonged immobilization.16,17 Previous literature has additionally demonstrated an increased risk of mortality in frail patients following elective spine surgery.8,18 While predictions of complication development must be tailored to individual patients, these results provide insights into the complications that frail patients are most likely to develop, which may guide providers in their management. mFI risk stratification may also guide the use of invasive interventions that could help recovery without unduly increasing complication risk.
Prior studies of the mFI as a predictor of outcomes following traumatic spine injury have been published. One study investigated patients operatively managed for traumatic SCI in the NTDB and found that higher 11-point mFI scores correlated with increased risk of complication development and non-routine discharge. 19 Another study found that adult SCI patients with increasing frailty on the 5-item mFI were more likely to experience an adverse event and in-hospital mortality. 20 The current study builds upon these prior works by using a contemporary cohort and generalizing to all patients with a vertebral fracture, not only those who sustained SCI or underwent surgery. We also correct for injury level, the presence of an SCI, and concomitant head injuries, among other covariates, which influence recovery from spine injuries.21–23 Further validation of the 5-item mFI is required in prospective cohorts, particularly those aimed at implementation of this tool to aid patient triage; nevertheless, these results may motivate the use of the 5-item mFI in patients with both acute and nonacute spinal pathology.
The cohort included demonstrated a predominance of patients with lumbar injuries, which aligns with epidemiological data showing that vertebral fractures overall most commonly occur in the lumbar spine, whereas SCI more frequently involves the cervical spine due to its relatively narrow canal.16,24 In contrast, the greater mobility and weight-bearing demands of the thoracolumbar region increase its susceptibility to bony injury. These biomechanical and epidemiological differences highlight the need to distinguish outcomes between patients with and without associated SCI. Additionally, the finding that patients treated at level II trauma centers had lower complication rates than those treated at level I centers, though initially unexpected, may be explained by differences in case severity and patient triage. Level I centers often receive patients with higher injury burden, greater medical complexity, or polytrauma, all of which inherently elevate complication risk. 25 Level II centers may also provide more streamlined care for less complex injuries, which could contribute to the lower complication rates observed. 26
In addition to greater frailty on the mFI, lower GCS and higher ISS scores were strong predictors of complication development. The GCS is commonly used as a risk stratification tool for patients with spinal trauma, given that concurrent brain injuries are likely to affect both injury assessment and functional recovery.22,27 Greater injury severity as measured by the ISS also expectedly increased the likelihood of complication development.28,29 While the 5-item mFI is a quick and effective method of risk stratification, it is not a perfect predictor and may hold less predictive power than the GCS and ISS. However, the benefit of the mFI is that it captures a different dimension of risk than the GCS and ISS, namely premorbid health burden, and its continued significance in the multivariable analysis presented here suggests that it may be used in conjunction with these other easily implemented tools in a trauma triage setting when formulating a treatment plan.
This study has several limitations. First, ICD-10 lacks specific codes for neurosurgical and orthopedic procedures, so some patients may have been inadvertently excluded. Second, coding or data entry errors and inconsistent reporting of variables such as race and insurance reduce reliability, as with all national datasets. Third, unmeasured factors such as provider bias, experience, hospital resources, or treatment quality may have influenced outcomes. Fourth, health issues not captured by the 5-item mFI could affect recovery, and because it uses common comorbidities, the index may overestimate frailty in otherwise healthy patients. 7 Fifth, while all hospital complications recorded in the NTDB were analyzed, relevant complications including the development of gastrointestinal stress ulcers, which is a complication of spinal trauma and treatment in a critical care unit, were not recorded and reflect the limitations of using a national database.30,31 Finally, as a retrospective cohort study, causal relationships between frailty and complications cannot be established. Future work should consider the use of prospective, multicenter data to ensure data completeness and to address the limitation of unrecorded complications. Use of such a dataset may also allow for analysis of long-term outcomes and the delayed development of complications, which is lacking in the NTDB. Lastly, the prospective study of clinical predictive tools which include the mFI in addition to the GCS and the ISS would serve to better understand the utility of considering frailty in real-time decision making.
Conclusions
The 5-item mFI is a simple and efficient tool for estimating frailty in trauma settings. In this NTDB analysis, greater frailty was associated with higher complication rates, most commonly cardiac events, VTE, and pressure ulcers. Additional predictors included lower GCS, higher ISS, head trauma, SCI, and surgical intervention, though the mFI remained significant after adjustment. The 5-item mFI can easily be incorporated into practice to identify high-risk patients and guide targeted care. Prospective studies are needed to validate its implementation in trauma settings.
Transparency, Rigor, and Reproducibility Summary
This study was not pre-registered with any organization as it is a retrospective review of a national de-identified database. An analysis was not pre-registered prior to data collection. A total of 5,481,046 patients were screened in the NTDB with the final sample being comprised of 356,583 patients after all inclusion and exclusion criteria were applied. This final cohort was used for all analyses. Blinding was not applicable as this is a retrospective review of a de-identified database. Data were acquired through the American College of Surgeons and is not publicly available. Analyses were conducted using R (R version 4.4.0). The key inclusion criteria are established standards in the field. Correction for multiple comparisons was performed using multivariate regression.
Authors’ Contributions
C.P.: Formal analysis, investigation, methodology, software, visualization, writing—original draft, and writing—reviewing and editing. M.J.H.: Conceptualization, investigation, and writing—reviewing and editing. R.S.: Conceptualization, investigation, and writing—reviewing and editing. O.Y.T.: Conceptualization and writing—reviewing and editing. O.P.L.: Conceptualization and writing—reviewing and editing. J.S.F.: Conceptualization, supervision, validation, and writing—reviewing and editing.
Footnotes
Author Disclosure Statement
The authors have no competing interest to disclose.
Funding Information
There was no funding provided for this research.