
Abstract
Background:
While sex differences are known to influence end-of-life preferences and experiences, the impact of sex on medical assistance in dying (MAiD) is not well understood. This study aims to examine sex differences in those who request MAiD.
Methods:
This retrospective cohort study included all adult patients in Nova Scotia, Canada who requested MAiD between June 17, 2016, and December 31, 2018, and were deceased at time of analysis on June 10, 2020 (n = 383). Descriptive statistics and logistic regression were used for analysis.
Results:
Completion of the MAiD assessment process or provision did not differ by sex. Compared with females, more males had a Charleson comorbidity Index (CCI) greater than six (38.2% vs. 26.3%, p = 0.019) and were married or common law (65.1% vs. 49.1%, p = 0.002). Females had decreased odds of completing MAiD assessment if they were cohabitating (OR: 0.45, 95% CI: 0.2–0.97, p = 0.046). Males had decreased odds of completing MAiD assessment with a CCI > 6 (OR: 0.51, 95% CI: 0.27–0.95, p = 0.035), or with specialist palliative care consultation (OR: 0.41, 95% CI: 0.17–0.91, p = 0.037).
Conclusion:
Males with a higher degree of comorbidity and specialist palliative care involvement—likely indicators of poorer prognosis at time of MAiD request—were less likely to complete MAiD assessment. Males may be having end-of-life planning conversations later in their disease course, which may impact their ability to have their preferred mode of death. Future research considering sex and preferences at end-of-life, including palliative care involvement, is needed.
Key Message
Males with higher degree of comorbidity and specialist palliative care involvement—likely indicators of poorer prognosis at the time of MAiD request—were less likely to complete MAiD assessment process. End-of-life planning conversations should occur early and often, to facilitate individual’s preferences at end of life.
Introduction
In 2015, the Carter v. Canada supreme court judgment abolished the criminal code prohibition of physician assisted death. 1 On June 17, 2016, the Canadian Parliament passed Bill C-14, legalizing medical assistance in dying (MAiD) in Canada for competent adults who meet certain eligibility criteria. Specifically, they must be 18 years of age or older and have decision-making capacity, be eligible for publicly funded health care services, make a voluntary request that is not the result of external pressure, give informed consent to receive MAID (meaning that the person has consented to receiving MAID after they have received all information needed to make this decision), have a serious and incurable illness, disease, or disability (excluding a mental illness until March 17, 2027), be in an advanced state of irreversible decline in capability, and have enduring and intolerable physical or psychological suffering that cannot be alleviated under conditions the person considers acceptable. 2 An individual requesting MAiD must undergo two independent medical assessments to ensure they meet eligibility criteria, and make a written request for MAiD. 3 In 2021, MAiD was allowed for those whose natural death was not reasonably foreseeable. 4 Further, those who may lose capacity because of their illness are able to make an advanced request for MAiD by signing a waiver of consent. 5 Between 2016 and 2023, there were 60,301 MAiD provisions in Canada. 6 From the first annual report in 2019 until 2022, the cohort was on average 48.4% female, with average age from 75.2 to 76.3 years, and the most common condition reported was cancer.6–10
Differences in end-of-life care between sexes needs to be considered to support equitable access, especially as the landscape of MAiD changes. 11 The Canadian Institutes of Health Research defines sex as “biological and physiological characteristics that distinguish females from males.” 12 There are known sex differences in response to environment stressors, physiological distress, and biological stress responses. 12 More broadly, suffering has been described as a combination of physical, emotional, existential, and spiritual distress. 13 In a study of advanced cancer patients admitted to hospice and palliative care patients, males were more likely to have symptom distress. 14 In a study of patients with heart failure, females tended to live longer with higher symptom burden, undertreatment of pain, and were more likely to become a widow or experience loneliness. 13 Females with heart failure may have higher symptom burden, and less improvement in quality of life following palliative care intervention. 15 Discussions about goals of care are key to ensuring that care concordant with patient values is provided, especially in situations with poor prognoses. Several studies have shown that females may tend to prefer and receive more palliative care, while males may be more likely to receive aggressive life sustaining at end of life, even if death was imminent.16–21 Conversations about prognosis and expectations may play a role, as in a study of patients with metastatic cancer, males who had an end-of-life discussion were less likely to have an ICU stay in the last week of their life. 16 Sex and relationship status may influence social support networks, and in turn, end-of-life decision making. In a study of hospice patients in England, social support through the hospice day program led to reductions in loneliness. 22 In a study of patients from Japan with advanced lung cancer, isolated patients were more likely to die at home, potentially suggesting less access to supports. 23 Overall, socially isolated older adults are less likely to engage in advance care planning. 24
The aim of this study is to identify differences by sex in MAiD outcomes (completion of MAiD assessment and MAiD provision) in Nova Scotia in a cohort of eligible MAiD patients between 2016 and 2018, i.e., before MAiD could be accessed by those without a reasonably foreseeable natural death. This was done to focus on individuals close to end of life, where our variables of interest were more applicable. These variables of Charlson Comorbidity Index (CCI) to predict 10 year mortality, 25 specialist palliative care consultation, and living situation were evaluated as they were previously found to be statistically significant predictors of completing MAiD assessment. 26
Methods
This retrospective cohort study is a secondary analysis of data published by Lees et al. (2021), stratified by patient sex, which was approved by the Research Ethics Board at the Nova Scotia Health Authority (protocol no. 1023925). 26 It was developed in accordance with the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) statement for observational studies, 27 and the SAGER (Sex and Gender Equity in Research) guidelines for a systematic approach to reporting sex and gender in research. 28 Patients were identified through the Nova Scotia Health Authority MAiD care coordination office which maintains a provincial registry for all MAiD requests. The study cohort includes all adult patients (18 years or older) in Nova Scotia who requested MAiD from the first date of legal access on June 17, 2016, until December 31, 2018, to allow for a follow up period for analysis of patient outcomes. This period was before MAiD eligibility had expanded to include those without a naturally foreseeable death or allowed a waiver of final consent. Patients were excluded if they were not deceased by the time of initial analysis on June 10, 2020. Data were extracted from the medical health record, and individual health care providers in the community were contacted if needed for completeness.
MAiD outcomes included both noncompletion (chose not to proceed with MAiD, natural death for any reason, ineligible, or incomplete assessment), and MAiD provision completion. Patient characteristics included age, sex, access to a primary care provider, CCI at the time of request, location (rural or urban), declared religion, living children, marital status, primary diagnosis, and palliative care specialist involvement. CCI is used to predict 10-year survival in patients with multiple comorbidities. 25 Points are assigned based on age, myocardial infarction, congestive heart failure, peripheral vascular disease, stroke, dementia, chronic pulmonary disease, connective tissues disease, peptic ulcer disease, liver disease, diabetes, hemiplegia, kidney disease, malignancy, and AIDS. Those with a CCI over 6 have a 0% estimated chance of 10 years survival. 25 We stratified the study cohort by sex, which was recorded as documented on provincial health cards. Individual’s gender was not documented.
All statistical analyses were performed using statistical packages from R and R Studio. 29 Statistical significance was determined by a p-value of ≤0.05. Descriptive statistics were used to compare patient characteristics and MAiD outcomes between sexes. There was nonnormal distribution of continuous variables on Shapiro–Wilk test, so the Wilcoxon rank sum test was used to analyze these variables. Logistic regression was used to compare completion of MAiD assessment and completion of MAiD provision once eligible between sexes, by specialist palliative care (SPC) consult, CCI, and living situation. The predictor variables of CCI > 6, cohabitation, and SPC consultation were chosen as they were previously associated with decreased odds of MAiD completion. 26 Missing data were indicated in the results and excluded from statistical analysis.
Results
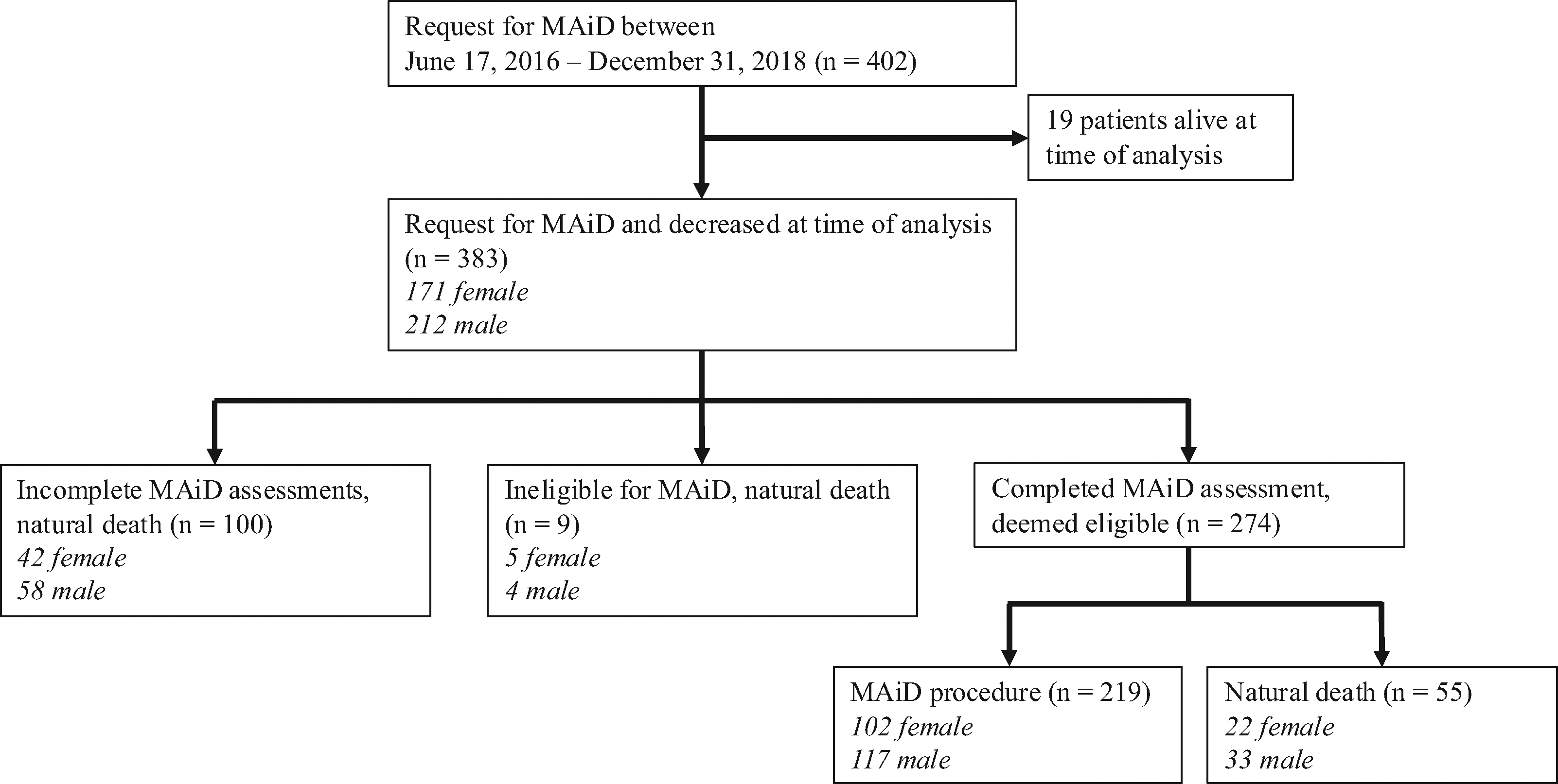
A total of 402 patients requested MAiD between June 17, 2016, and December 31, 2018 (Fig. 1). Nineteen were excluded as they were not deceased at time of analysis, leaving 383 patients included in analysis.
Study population and outcomes.
A greater proportion of patients were male (55.4%). There were no significant differences in age, residence in either a rural or urban area, or having a living child. The composition of primary diagnoses was similar between sexes, with solid malignancy being the most common. Males had a significantly higher burden of comorbidities as measured by CCI > 6 (38.2% vs. 26.3%, p = 0.019). More females had a declared religion (68.4% vs. 57.1%, p = 0.03). More males were married or common law (65.1% vs. 49.1%, p = 0.002). However, there were no significant differences between living status defined as cohabitating, living alone or in long-term care. There was no significant difference in palliative care specialist involvement (Table 1).
Study Population Characteristics

CCI, Charlson comorbidity index; IQR, interquartile range; LTC, long-term care; SPC, specialist palliative care; SD, standard deviation.
Boldface is used to highlight p values <0.05
There were no differences in timeliness to MAiD access once requested, which was recorded as days from MAiD request to death. There were also no significant differences in MAiD assessment completion, or MAiD provision completion between sexes (Table 2).
Maid Outcomes by Sex

Multivariable logistic regression analysis was completed for each sex to identify odds of completion of the MAiD assessment process, adjusted for palliative care consultation, living situation, and CCI (Table 3). Males had a statistically significant decreased odds of completing MAiD assessment with a CCI > 6 (OR: 0.51, 95% CI: 0.27–0.95, p = 0.035). Males also had a decreased odds of completing MAiD assessment if they had palliative care specialist consultation (OR: 0.41, 95% CI: 0.17–0.91, p = 0.037). Females had a decreased odds of completing MAiD assessment when cohabitating (OR: 0.45, 95% CI: 0.2–0.97, p = 0.046).
Logistic Regression Analysis: Completion of Maid Assessment, Adjusted for SPC Consult, CCI, Living Alone

Boldface is used to highlight p values <0.05
We conducted a second multivariable logistic regression analysis by sex for odds of completion of the MAiD provision once eligible, adjusted for the same variables as above (Table 4). Females had statistically significant lower odds of completing MAiD once eligible if they were cohabitating (OR: 0.28, 95% CI: 0.07–0.088, p = 0.046).
Logistic Regression Analysis: Completion of Maid Provision Once Eligible, Adjusted for SPC Consult, CCI, Living Alone

Boldface is used to highlight p values <0.05
Discussion
A greater proportion of those requesting MAiD were male (55%), average age was similar between sexes, and solid malignancy was the most common primary diagnosis. These findings are consistent with Canadian trends.6–10 Between sexes, there were no significant differences in MAiD outcomes including completed assessment or mode of death, nor were there significant differences found in timeliness of access to MAiD. There were also no differences between sexes with respect to having a living child. There was also no difference between sexes and specialist palliative care consultation. This differs from previous literature, which suggested females were more likely to prefer palliative care.16–21,30 Our population included only individuals with a reasonably foreseeable death, and through the MAiD assessment process, all individuals would have had palliative care options offered.
For males, greater comorbidity and palliative care consultation were associated with a decreased odds of completing MAiD assessment. As previously hypothesized, specialist palliative care consultation may be a surrogate marker of more severe disease and/or symptoms at the time of request.26,31 With a poorer prognosis at time of MAiD request, those males may have been less likely to complete assessment before their natural death, or before losing capacity. Delays in timely MAiD assessment for individuals closer to end-of-life could contribute; however, the same was not true for females. Previous studies found men were more likely to have aggressive care at the end of their lives.16–21 This may be related to sex differences in attitudes towards disease. 19 If conversations about approaching end of life were occurring later in the disease course for men, they may not have had time to arrange their preferred mode of death. 31 Having early and ongoing goals of care discussions, along with access to specialist palliative care, is important to ensure patients have realistic expectations about their health and time to make plans in keeping with their wishes.
In our population, more males were married or common law, and more women were widowed (26.3% vs. 15.1%, Table 1). This may be related to general life expectancies being longer for females in Canada (83.8 years for females vs. 79.4 years for males). 32 In the original analysis from Lees et al. (2021), cohabitation was associated with decreased odds of completing MAiD. 26 In this secondary analysis, only females had decreased odds of completing MAiD assessment or provision when cohabitating. A previous study from the United States found that married women were less likely than widowed or divorced women to complete end-of-life care planning. 33 They hypothesized married women may rely more on their partner would make end-of-life choices for them. 33 In our population, women cohabitating may have delayed completing the MAiD process for this reason. Women living alone may be more likely than men to stay connected to their community, providing support for earlier conversations about end-of-life wishes. 34 These are broad generalizations, as every individual has complex factors involved in their decision-making. Therefore, this difference between sexes may be spurious. These findings further highlight the importance of considering sex in end-of-life care, to elucidate clinically meaningful differences.
Our study strengths include a robust and comprehensive provincial dataset. To our knowledge, this is the first study in Canada to evaluate sex differences in MAiD. Our study population only included those who had requested MAiD; therefore, there may be differences in end-of-life preferences between sexes in those who are not interested in MAiD. This data was also collected before MAiD was allowed for those without a naturally foreseeable death, or a waiver of final consent, and our results are not generalizable to these groups. Further evaluation of how sex may impact MAiD outcomes is warranted, considering the expansion of eligibility. 6 As this study only evaluated biological sex, it is not generalizable to gender, and did not consider sexuality. Transgender and nonbinary individuals have been shown to experience discrimination and have less access to health care services. 11 They are also at higher risk of social isolation and precarity at the end of life. 35 Consideration of gender and sexuality is sorely lacking in end-of-life care research, including MAiD, and future research in this area is a pressing need.
Conclusions
While MAiD outcomes did not differ by sex, males were significantly less likely to complete the MAiD assessment process with CCI > 6 and specialist palliative care involvement, which may be crude markers for males MAiD requests’ occurring later in the stage of their illness than females as the primary driver for incomplete assessments. Males may have a greater burden of illness before discussions about end-of-life planning are initiated. Future research should consider the timing of first documented and subsequent goals of care discussions, the timing of MAiD referral, and access to specialist palliative care involvement. This information may be used to help inform knowledge translation into policy and practice, as the landscape of MAiD continues to evolve.
Authors’ Contributions
C.L. completed statistical analysis on the original dataset and conceptualized the article. S.D. wrote the initial draft and revision, and all authors provided feedback.
Footnotes
Author Disclosure Statement
S.D. and A.M.K.N. had no disclosures. C.L. a MAiD Assessor. G.G. is a MAiD Assessor and Provider, the NSH MAiD Clinical Lead, and a Board Member for the Canadian Association of MAiD Assessors and Providers.
Funding Information
Funding for this project was generously provided by the Nova Scotia Health Authority Research Fund grant number RB16300059620. A knowledge translation grant was provided by the Canadian Association of MAiD Assessors and Providers. These funding agencies had no role in data collection, its analysis or interpretation, and has no rights in the approval or disapproval of publication.