
Abstract
Keywords
Introduction
Early integration of palliative care and excellent symptom management have been shown to produce significant benefits for quality of life at the end of life. 1 As a result, there has been a push towards better community palliative care that enables patients to remain at home and avoid crisis admissions and interventions that are not within their goals of care. However, little research has examined whether these benefits hold true regardless of sex or gender. 2 By sex we mean the biology of being a man or woman whereas gender is used in a social sense, to describe the opportunities and constraints arising from sex roles. We differentiate gender from individually defined gender identity. A shift towards more care in the home may disproportionately burden women, who traditionally are society's informal care-providers. Supports women and men have available to them at the end of life may differ.3–5 Some of these differences arise from deeply rooted gender norms and roles that society has traditionally deemed acceptable despite their embedded inequities, creating disparities between women and men in terms of place of death, amount and type of support offered, likelihood of accepting palliative care, or experiences of symptoms such as fatigue, and caregiver burnout.3–9
Although there is extensive documentation that sex/gender has a large influence on experiences, preferences, and care received at the end of life,4–17 and one review of women as care-givers, 3 much of the research on palliative care has inadvertently neglected to study the effect of gender, particularly on care receiving. 5 This remains a largely unrecognized obstacle to providing palliative care that is universally beneficial. Healthcare providers are not able to cater care to the needs of each patient and family unit without applying a lens that reveals deeply rooted gendered constructs and expectations.4,5,8,18 This lack of insight fails men and women in different ways, as they struggle and grapple with the impact of very different ingrained beliefs. For example, men are often implicitly taught that they must be stoic, strong, and not express any emotion or ask for help, and instead, ‘fight’ for a cure until the very end.12,19–21 Traditional socialization of women, in contrast, is to be caring, sensitive, and willing to put others first despite any burden to themselves.4,22–24 These ingrained beliefs significantly colour what either group thinks is expected of them at the end of life and shape the types of supports, treatments, and communication they seek or need from healthcare providers.
Since ideal end of life care is holistic, patients cannot be separated from their family or caregivers. It is therefore not only the sex/gender of the patient that can affect disparity, but that of caregivers as well. Women, as the traditional carers in most societies, often have spent a lifetime providing informal care, without being recognized for such efforts.3–5,24 Their work is hence rendered largely invisible and often undervalued, which may unintentionally deplete their emotional reserve. This can affect the choices they make for themselves at the end of life. Having experienced the effort required to be a caregiver, they may feel guilty about, and choose not to burden family members with that same weight and responsibility.5,8,15,18
Despite increasing recognition of gender as a determinant of health, research on the extent and complexity of gender disparities in end of life care is limited, and evaluations of the strength of existing evidence are lacking. This study aims to fill that gap by identifying and mapping out relevant concepts creating gendered disparities in end of life care, evaluating the quality of the evidence backing these concepts, and identifying gaps in existing research to inform future research direction. A scoping review was chosen as the research design due to the expected heterogeneity of the concepts being mapped and the lack of precision in the clinical research question being asked, making it the best design for exploring a wide array of themes while retaining a systematic methodology for combing through the literature. 25
Methods
Table summarizing critical appraisal and descriptive analyses from each of the 15 studies included in review. Table includes article title and year of publication, strength rating, checklist used, context of study (where relevant), reasons for rating, and key findings and themes.

Results
A systematic search of the databases in August 2021, returned a total of 624 articles, of which 335 were duplicates and 274 were excluded, leaving 15 articles that met inclusion criteria for the scoping review (See Figure 1 for details regarding exclusions).
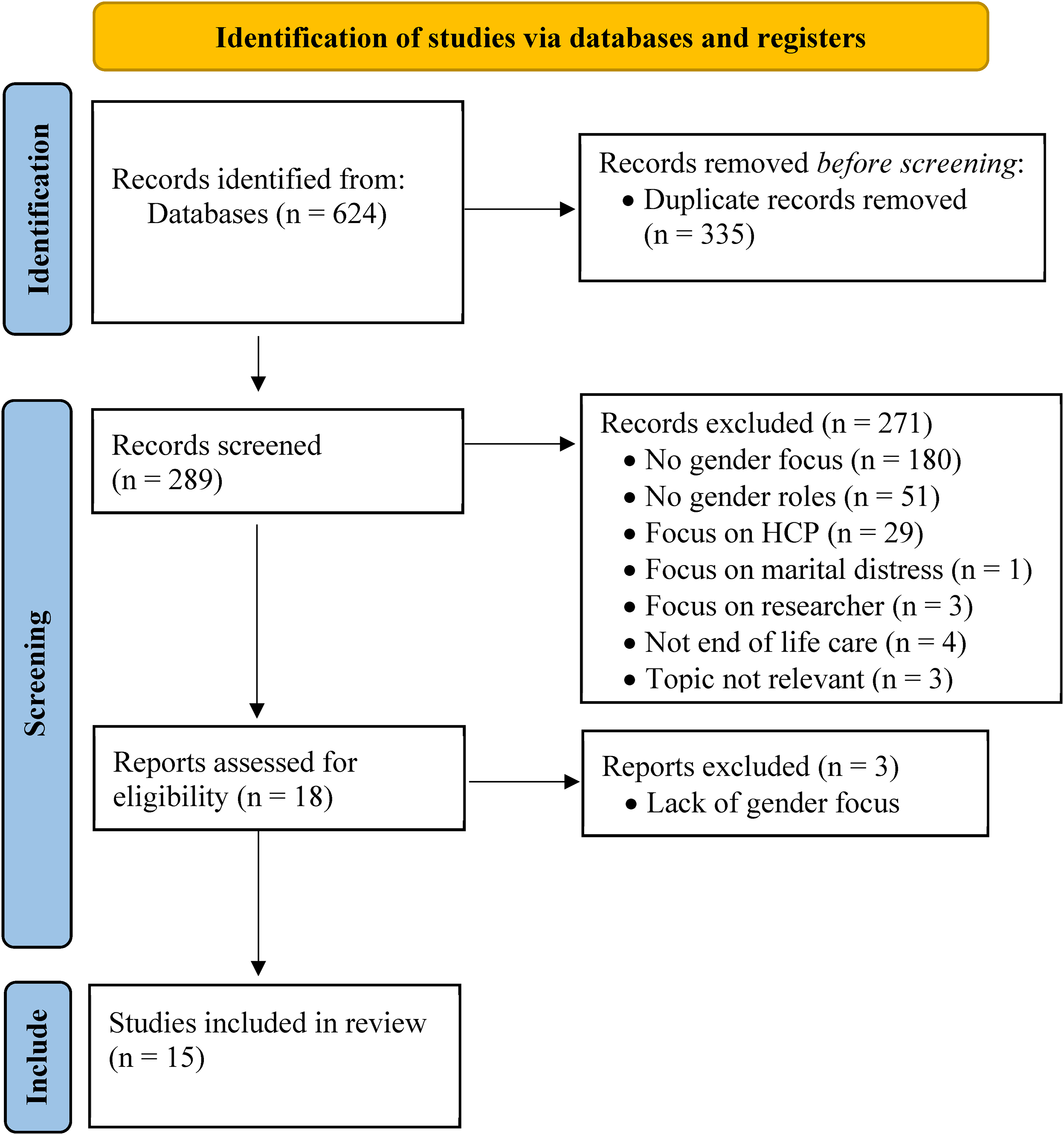
PRISMA 2020 flow diagram for identification of studies, which included searches of databases and registers only.
Critical Appraisal of Studies
The 15 articles that were critically appraised included one systematic review, six quantitative studies, six qualitative studies, one letter to the editor, and one critical essay. These studies were published between 2011 and 2020, and were conducted in Canada, USA, England, Sweden, Germany, Portugal, and New Zealand. The AMSTAR checklist and NICE guidelines were used to appraise papers based on study format.28,29 The letter to the editor and the critical essay were read for additional perspective and used to confirm consistency, but since neither reported a study, critical review options were limited. Overall, most studies were of poor to moderate quality. Eight were classified as weak, five as moderate, and two as strong, using the rating described in the methods section (Table 1).
Thematic Analysis
Descriptive analyses were carried out for each of the studies included in the review and their findings were included in the critical appraisal table (Table 1). Thematic analysis was then conducted to synthesize heterogeneous data into themes that could be presented in an organized fashion. Findings from each study were coded by the primary author into 6 general themes: living situation, symptom experience, care context, care preferences, caregiving, and coping strategies.
Healthcare providers’ approaches were not exempt from gender bias. At times, they delegated physical care tasks to female, and decision making to male caregivers.
24
They also provided more support to male caregivers, who were seen as “heroic” in providing care outside their gender role, while women were not offered the same support.5,24 Women were assumed to inherently be more compassionate, sensitive to others, and willing to put others before themselves regardless of the woman's health. They were expected to care about and for a loved one, whereas men were not held to the same standard.4,24 Healthcare providers were unaware of their unequal expectations of males and females and essentially rendered women's work invisible and undervalued.5,24 In terms of formal supports, female caregivers were less likely to qualify for various government financial support benefits offered to caregivers, as these were generally linked to employment and women were more often unemployed or involved in part-time work. When they did qualify, they often received less money, again related to women's lower incomes across occupation and location. Men, however, applied for and, therefore, received such benefits less frequently, suggesting that they underutilized this formal support, perhaps because they were less likely to provide care to their partners.
37
Discussion
Overall, gender bias appeared to permeate many aspects of end of life care. Although research on such sex/gender disparities has been conducted in the past ten years, most studies had small sample sizes and lacked enough detail on selection, methods, and data collection to achieve internal validity. External validity was also limited, as most involved only one or two centres with patients from specific cultural contexts or locations (eg, inpatient or hospice populations), or with specific medical conditions. Despite these gaps, the literature identifies significant sex/gender disparities for care giving and receiving and in multiple domains of end of life care. The push for more end of life care in the community may unfairly burden women who shoulder most caring duties but receive less care support.3–7,24,34 Six domains or themes were specifically identified, under which gender disparities fell: living situation, symptom experience, care context, care preferences, caregiving, and coping strategies. All of these were clearly linked to deeply ingrained social constructs of sex/gender with each creating inequitable expectations at end of life.
By the end of their lives lifelong inequities in pay and working conditions leave women with limited financial resources compared to men.3,5 Women's greater life expectancy brings with it the harm of widowhood and of living alone when death approaches.31,32,34 Unfortunately, a longer lifespan also brings greater burden of symptoms and suffering, perhaps somewhat linked to being society's natural ‘caregivers’ throughout life.4,7,30 By outliving their spouses, women are disadvantaged at the end of life when there are fewer caregivers and resources left to provide for them. 32 They are more likely to accept formal care and dying in an institution rather than at home to avoid being a burden, one they may know well having often provided home care to their spouses.3,6 That caregiving work can be rendered invisible by healthcare providers, who subconsciously put in place more support for male caregivers since they are seen as ‘unnatural’ in this role. 24 Perhaps this lifelong toll of continuing to dutifully care even after receiving multiple medical diagnoses or nearing the end of life is offsetting some of the benefit women should receive with earlier palliative care, and resulting in a disparity in benefit.5,34 Women, but not men, emphasize appearance as an important coping mechanism. This is likely related to the social currency of a woman's appearance, which has been linked to value and identity in a way that does not hold true for men. Appearing old and losing hair is much more stigmatized for women and acceptable for men, so women are more likely to dye their hair, paint their nails or wear wigs, attempting to retain status and value in society. 35
Ignoring the effect of gender constructs also disadvantages men who are taught that they must be strong and tough, that expressing emotion is “unmanly”, and that vulnerability is a weakness.4,21 This can discourage seeking end of life support or communicating feelings and symptoms to healthcare providers. Men then rely more on themselves rather than an extended network for support, and after a lifetime of suppressing feelings, have more difficulty communicating needs, fears, or perceived weaknesses.6,14,36 Men could, instead, be encouraged to express their emotions and symptoms and approach others for support, rather than succumbing to social pressure to remain silent and strong. Boys need to be encouraged to talk about physical and psychological pain earlier in life so it becomes more natural and they develop a wider vocabulary for describing how they feel later on. 36 Experiencing vulnerability often equates to a loss of manhood, a core tenet of male identity; thus, acknowledging and/or revealing increasing dependence often precipitates struggles with depression. 33 Finally, men who do wish to assume the role of caregiver may be pushed aside as the unnatural choice, with a female caregiver being favoured. 5
Implications for Research and Practice
We are cautious in making recommendations about palliative care practice given that this was a scoping review and papers identified did not demonstrate exceptional methodologic quality. Some conclusions do, however, seem reasonable and provide guidance for future research. Gender disparities in end of life care giving and receiving disadvantage both men and women, but in different ways. Subsequent research might consider whether and how social constructs of gender affect the type of communication, care, and support that patients and families need. Reflexivity is required to challenge gender assumptions, bring gendered processes to the forefront instead of allowing them to be rendered invisible in everyday practice, and to increase awareness of how physicians’ own socioeconomic status creates power imbalances that can influence interactions with patients and their families. The impact of discussing gender roles, relations, and biases in professional health care education is an area for potential research. The focus of such education and research on it might go beyond sex differences, to examine gender as a social process that interacts with and affects sociopolitical structures and other life circumstances. 36 How might patients and families become partners in challenging gender biased expectations? Finally, research that reveals whether systemic and gendered assumptions about caring determine both men's and women's roles in providing informal palliative care might be a first step in breaking down these stereotypes. 24
Limitations
Some might consider our focus on disparities between men and women to be a binary view that ignores the more fluid construct of gender identity, and therefore a limitation in scope. Our aim was to examine whether and how the expectations and constraints tied to sex/gender, affect end of life care. Gender identity, while not the same as the social construct of gender, likely does play a role in end of life care, but one that has already been studied and reviewed. This became evident when we undertook a secondary Medline search of ‘palliative care’ and ‘gender identity’ which yielded 13 papers. A title review limited this to two papers, ‘Gendered Processes in Hospice Palliative Home Care for Seniors With Cancer and Their Family Caregivers’, 24 and ‘Expanding the Palliative Care Domains to Meet the Needs of a Community-Based Supportive Care Model (qualitative research)’, 38 one of which was already included in our study, and neither of which addressed gender identity. However, when we searched ‘palliative care and transgender (subject or keyword)’ eight relevant papers were found, five of which were reviews done over a three year timespan.39–43 This seemed adequate and also surprising given the dearth of reviews about sex/gender bias in palliative care.
Another limitation is the omission of intersectionality in the scoping review. By this we mean that sex, alone, is only one of many social circumstances that might influence end of life expectations and care, and that its influence is not independent of other factors such as race, socioeconomic status, or geographic region.44,45 It would be important to study the intersecting impact of these factors on end of life care and the interconnected disparities that might result. This scoping review has only scratched the surface in examining intersectionality. Two articles demonstrated differential effects of gender in different cultures: the value attached to women's appearance in Portuguese culture 35 and cultural perspectives from Gambia and Kerala where there is an increased prevalence of HIV affecting gender dynamics. 32 Finally, the review of the literature was primarily conducted by one author, whose social location - physician, Chinese cultural background, and female sex - also subconsciously provide a lens through which the research was analyzed and presented. This bias was minimized as much as possible by using objective checklists for appraising the evidence and having the second author review and verify the findings.
Conclusion
Overall, more comprehensive and generalizable research of greater validity is needed to paint a better picture of sex/gender effects in end of life care. Nonetheless, research is still consistent in demonstrating that significant gender disparities exist in end of life care. Palliative care professionals can play a pivotal role in working to upend these disparities by building awareness of personal biases and using that awareness to provide support to patients and families, educate future medical professionals and patients/families, and initiate important care discussions that can overturn unequal gendered expectations.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.