
Abstract
Background:
Cancer-related distress is a multifactorial experience affecting patients’ quality of life and treatment outcomes. Despite global efforts to promote distress screening, data from low-resource settings remain limited.
Objectives:
To assess the prevalence, severity, and contributors to distress among cancer patients in a tertiary oncology center in Lebanon and identify palliative care (PC) referral gaps.
Design:
Cross-sectional secondary analysis of a quality improvement initiative.
Setting/Subjects:
Adult cancer patients receiving treatment at the infusion unit of the Naef K. Basile Cancer Institute, American University of Beirut Medical Center.
Measurements:
Distress was evaluated using the National Comprehensive Cancer Network Distress Thermometer (NCCN DT). Patients with DT scores ≥ 4 completed the NCCN Problem List. Sociodemographic and clinical data were extracted from institutional records.
Results:
Among 670 patients (mean age: 56 ± 15 years; 56% female), 76% reported moderate-to-severe distress (score ≥ 4), and 37% experienced severe distress (score > 7). Distress was significantly higher in females (p < 0.001) and patients with solid tumors (p = 0.015). Key distress domains included physical (93%), emotional (83%), and practical problems (70%). Only 1% of distressed patients had prior PC referrals.
Conclusions:
Distress is highly prevalent among cancer patients in Lebanon, particularly among women and those with solid tumors. Despite strong evidence for the benefits of early PC, referral rates remain alarmingly low. Routine distress screening and integration of PC services are urgently needed to address this gap and improve holistic cancer care in low-resource settings.
Introduction
The global burden of cancer continues to rise, with the World Health Organization reporting approximately 20 million new cases in 2022. 1 Current estimates suggest that one in five individuals will develop cancer in their lifetime. 2 Advances in diagnosis and treatment have improved early detection and survival rates, with 53.5 million people surviving at least five years post-diagnosis as of 2022. 3 However, a cancer diagnosis and its multimodal treatments often heighten the risk of distress for both patients and their families. 4
Distress in cancer patients, as defined by the National Comprehensive Cancer Network (NCCN), is a multifaceted emotional experience encompassing psychological, social, and spiritual dimensions that can hinder effective coping with the disease and its treatment. 5 Contributing factors include advanced or recurrent disease, younger age, female gender, lack of social support, and prior psychiatric conditions. 6 Such distress is associated with reduced quality of life, poorer treatment adherence, and increased mortality risk, 7 prompting some experts to advocate for its recognition as the sixth vital sign in cancer care. 8 Additionally, patients experiencing depression alongside cancer often report heightened anxiety, pain, fatigue, and functional impairment, increasing their vulnerability to suicidal ideation. 7 Despite its profound impact, distress remains frequently underrecognized and undertreated, underscoring the need for timely intervention to improve both patient well-being and clinical outcomes. 9
Globally, psychosocial distress affects 15% of patients at initial diagnosis, rising to nearly 60% in palliative care (PC) settings. 10 In the Middle East and North Africa (MENA) region, reported distress prevalence ranges between 60% and 70%.5,11,12 In Lebanon, a country in the MENA, the burden of cancer has grown significantly, with new cases increasing from 7200 in 2004 to 11589 in 2020. 13 While early integration of PC has been shown to improve treatment outcomes and reduce distress, 14 access remains limited. Lebanon, being also a low-middle-income country (LMIC) according to the World Bank, faces systemic challenges in health care accessibility, making PC services a luxury many patients cannot afford.
This study aimed to assess the prevalence and causes of distress among cancer patients receiving treatment at the Naef K. Basile Cancer Institute (NKBCI) infusion unit at the American University of Beirut Medical Center (AUBMC). Ultimately our goal was to identify distress-related challenges, adapt existing services to the needs of patients and promote their utilization to improve patient support and outcomes.
Methods
Study design and patient population
This was a cross-sectional hospital-based study conducted at the NKBCI infusion unit, an outpatient chemotherapy unit at AUBMC. Patients receiving active treatment or follow-up were eligible for enrollment in the study. PC services were available on a consultative basis during working hours, 8 am–5 pm, from Monday to Friday. Referral was done through treating oncologists to the PC team. Data were collected from eligible patients selected from daily infusion schedules between September 2018 and June 2019.
This is a secondary analysis of de-identified data from a quality improvement initiative conducted at the NKBCI at AUBMC. No changes were made to the data after initial collection, and no patient-level interventions were performed as part of this study. The study was approved by the institution’s Quality Council. The patient population consisted of cancer patients undergoing treatment at the NKBCI infusion center, with participants randomly selected to ensure a heterogeneous representation of cancer types and disease stages.
Data collection and measures
Demographic and clinical data were collected, including age, gender, cancer diagnosis, treating physician, cancer stage, and prior PC referrals. Distress levels were assessed using the National Comprehensive Cancer Network’s Distress Thermometer (NCCN DT), a validated, single-item 11-point Likert scale (0 = no distress, 10 = extreme distress) measuring distress experienced in the preceding week (Supplementary Appendix S1).13–15
We used a cutoff score of ≥ 4 on the DT to define moderate-to-severe distress in order to maximize sensitivity in detecting patients who may require support and those that should be evaluated using the NCCN Problem List (PL) based on NCCN clinical recommendations.
16
The PL is a 40-item tool categorizing distress-related concerns into five domains:
Practical (e.g., financial, transportation, work/school) Familial (e.g., partner/child-related concerns, fertility) Emotional (e.g., depression, anxiety, sadness) Physical (e.g., pain, fatigue, nausea, sleep disturbances) Spiritual/Religious (e.g., existential concerns, loss of faith)
The NCCN DT has been previously translated to and validated in Arabic (Supplementary Appendix S2). 6
Data collection was carried out by the program’s research assistant (RA), who had received training supervised by the principal investigator. The training covered standardized administration of the DT and PL, sensitive communication with patients, and importance of maintaining confidentiality. The RA reviewed the daily infusion schedule to monitor the total number of patients and identify eligible individuals for inclusion. In order to minimize selection bias related to timing, symptom severity, or staff preference and avoid convenience selection, the RA assigned each eligible patient a unique number using a random-number table to determine the recruitment order. The process was supported and facilitated by the primary care physicians, the clinical nurse specialist in oncology, and the infusion unit’s nurse manager.
Sample size calculation
A formal sample size calculation was not conducted prior to the start of the study due to the absence of previous research assessing the prevalence of distress among Lebanese adults using the NCCN DT. As such, there was no baseline prevalence estimate available to inform a precise calculation. In light of this, the study adopted an exploratory, cross-sectional design and included all eligible participants accessible during the data collection period. The relatively large final sample size (n = 670) allows for meaningful subgroup analyses and provides valuable preliminary data to inform future research and formal sample size estimations.
Statistical analysis
Descriptive statistics were used to summarize patients’ demographic and clinical characteristics. Continuous variables were presented as means and standard deviations, while categorical variables were reported as frequencies and percentages. Group comparisons between distress levels (no to mild vs. moderate to severe) were conducted using independent t-tests for continuous variables and chi-square tests for categorical variables. For categorical variables with small cell counts, for example, PC referral status, chi-square tests with Fisher’s exact correction were applied. Analysis of variance was used to compare distress scores across age groups and cancer stages. We also performed a multivariable linear regression in order to explore independent predictors of distress severity with distress score (0–10 scale) as the dependent variable. Based on clinical relevance, the following variables were entered simultaneously into the model: age categories, gender, cancer stage (combined), cancer type (solid vs. liquid), prior PC referral, and the presence of practical/familial, emotional/spiritual, and physical problems from the NCCN PL. A significance level of p < 0.05 was considered statistically significant. All analyses were conducted using SPSS version 29.
Results
Data collection was performed from September 2018 to June 2019, with a total of 670 cancer patients included in the analysis. The mean age of participants was 56 ± 15 years (range: 22–89 years), with a higher proportion of females (56%) than males (44%).
The mean distress score on the NCCN DT was 6 ± 3. Females had significantly higher mean distress levels than males (6.74 vs. 5.75, mean difference 0.99, p < 0.001). A high proportion of patients (76%) reported moderate-to-severe distress (score ≥ 4), with 37% experiencing severe distress (score > 7). Notably, 99% of patients had no prior referral to PC services (Table 1). The majority of patients (97%) had malignant diagnoses, while 3% were nonmalignant. Among these patients, 88% had solid tumors, and 12% had liquid cancers. The most common malignancies were breast cancer (29%), followed by lung (11%), colon (9%), and pancreatic cancer (7%). In addition, there was a statistically significant association between diagnosis type and distress category (p = 0.035). In particular, patients with breast cancer had a higher proportion of moderate-to-severe distress; while those with colon cancer had a significantly lower proportion of moderate-to-severe distress. Those with lung, pancreatic, and other cancers did not differ significantly among the distress categories (Table 1).
Patient Characteristics by Distress Level
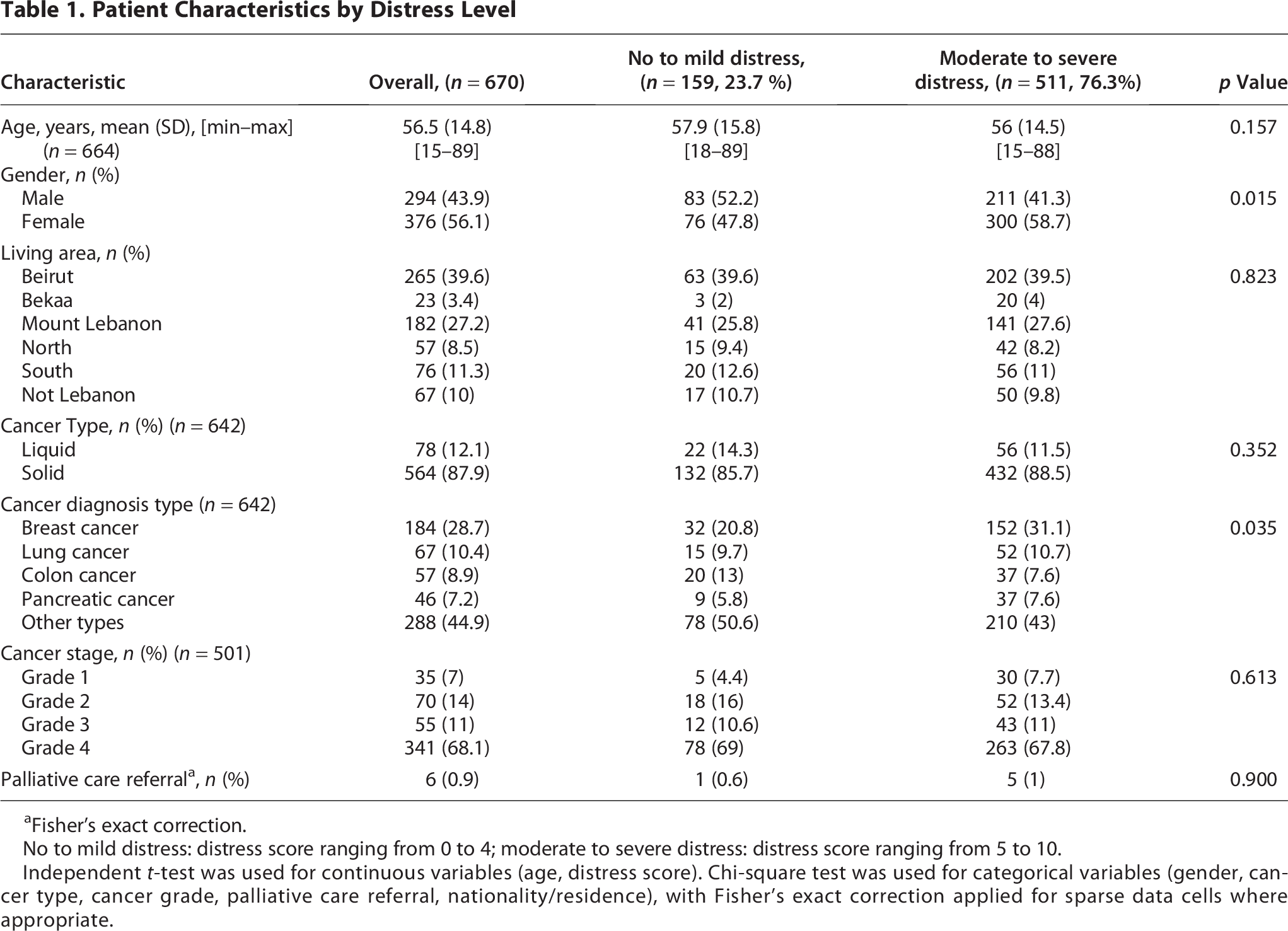
Fisher’s exact correction.
No to mild distress: distress score ranging from 0 to 4; moderate to severe distress: distress score ranging from 5 to 10.
Independent t-test was used for continuous variables (age, distress score). Chi-square test was used for categorical variables (gender, cancer type, cancer grade, palliative care referral, nationality/residence), with Fisher’s exact correction applied for sparse data cells where appropriate.
Patients with solid tumors had significantly higher distress scores (6.4 ± 2.6) compared to those with liquid cancers (5.6 ± 2.6; p = 0.015).
Analysis of distress contributors using the NCCN PL revealed distinct patterns among participants. Physical problems emerged as the most prevalent source of distress, affecting 93% of patients, with common complaints including pain, fatigue, and nausea. Emotional difficulties followed closely, reported by 83% of participants, encompassing issues such as anxiety, depression, and persistent sadness. Practical challenges represented another significant category, affecting 70% of the sample, particularly regarding financial strain, work/school disruptions, and transportation difficulties. Familial concerns were reported less frequently, present in 40% of cases, typically involving childcare responsibilities or partner conflicts. Notably, spiritual or religious concerns were the least common source of distress, affecting only 3% of the patient population (Fig. 1). The problems did not significantly differ between solid and liquid cancer groups (Table 2).

Prevalence of Sources of Distress. Bar charts show the percentage of participants reporting problems across three domains: emotional/spiritual, practical/familial, and physical. Each bar represents the proportion of respondents endorsing the problem using the NCCN Problem List, with sample sizes (n) indicated below each label.
Distress Problems by Type of Cancer

Patients with solid tumors had significantly higher distress scores compared to those with liquid tumors (mean = 6.4 vs. 5.6, p = 0.015). No significant differences in distress scores were observed across cancer stages (p = 0.475) (Table 3).
Distress Score by Age, Gender, Cancer Type, and Cancer Stage

ANOVA test performed for age, and cancer stage.
Independent t test performed for gender and cancer type.
Cancer stage available for 501 participants.
The multivariable regression analysis showed that several factors were associated with high distress scores in the adjusted model. Females reported significantly higher distress than males (B = 0.70, 95% CI: 0.33–1.08; p < 0.001). Practical or familial concerns (B = 0.69, 95% CI: 0.22–1.15; p = 0.004), emotional or spiritual concerns (B = 2.30, 95% CI: 1.78–2.81; p < 0.001), and physical concerns (B = 1.27, 95% CI: 0.55–1.99; p < 0.001) were also strong independent predictors of greater distress. Age, cancer stage, cancer type, and palliative-care referral status were not statistically significant in the adjusted model (all p > 0.05).
Discussion
Our study provides critical insights into distress proportions and characteristics among cancer patients in Lebanon, revealing three key findings: exceptionally high rates of moderate-to-severe distress physical and emotional problems as predominant distress contributors, and significantly greater mean distress in solid versus liquid tumor patients. Although both groups exhibited distress scores above the clinical intervention threshold, patients with solid tumors had higher mean scores. This could be partially explained by the burden of solid tumors that often entail more extensive treatment modalities (e.g., surgery, radiation, multi-agent chemotherapy), visible physical changes, and symptom burden compared with liquid tumors.
There was a significant association between cancer type diagnosis and distress severity, suggesting diagnosis-specific psychological needs. Breast cancer patients had significantly high levels of moderate-to-severe distress, consistent with evidence that women with breast cancer commonly experience increased fears and psychological burdens.
The distress proportion in our cohort substantially exceeds global reports, including Indian (53%), 17 Mexican (56%), 18 and American (46%) 19 populations. This disparity may reflect Lebanon’s unique health care challenges as a LMIC, where limited psychosocial support services and economic instability likely exacerbate cancer-related distress. The predominance of physical (93%) and emotional (83%) distress sources mirrors international patterns,15,17 underscoring the universal nature of these cancer burdens. Particularly concerning is our finding that 99% of distressed patients lacked PC referrals, despite strong evidence that early PC intervention improves symptom control and quality of life. 19 This represents a critical care gap in our setting.
The predominance of physical and emotional problems as key contributors to distress in our study population aligns with international findings and reinforces the multidimensional nature of cancer-related suffering. Nearly all patients (93%) reported physical symptoms—pain, fatigue, and nausea—highlighting the ongoing challenge of symptom management in active oncology care. These findings are consistent with prior studies from India and Mexico, where similar symptom burdens were reported as principal sources of distress.17,18 Emotional issues, reported by 83% of participants, including anxiety, depression, and sadness, also mirror global prevalence trends, where psychological morbidity in cancer patients has been extensively documented.4,7 Emotional suffering often coexists with somatic symptoms and can amplify their severity, creating a feedback loop that exacerbates distress and impairs quality of life.9,20 The high frequency of these concerns underscores the importance of integrated psycho-oncology services and proactive symptom control strategies. Despite this, our findings reveal a critical gap: only 1% of patients had prior PC referrals, which are known to alleviate both physical and emotional symptoms through holistic and multidisciplinary approaches.10,21 In Lebanon, access to PC services remains limited and is often introduced late in the disease trajectory, highlighting a gap between needs and service utilization. At the time of our study, PC services at AUBMC were still in the early stages of structured development, leading to low referral rates despite significant need. However, the PC program has expanded with increased staff, higher referral volumes, and more defined clinical pathways. Failure to address the dual burden of this issue not only diminishes patient well-being but also risks poorer adherence to treatment and worse clinical outcomes.9,19
Moreover, our results reveal higher mean distress in solid versus liquid tumors. This distress level disparity (6.4 vs. 5.6, p = 0.015) offers novel clinical insights. Although the mean difference in distress scores between patients with solid and liquid cancers was modest (0.8), both averages exceeded the NCCN intervention threshold, indicating that this difference is clinically relevant. Minor increases in DT score levels are associated with elevated psychosocial burden, risk of anxiety and depression, and greater health care utilization, underscoring that both groups warrant systematic screening and timely supportive intervention. 22 While direct comparisons are scarce in literature, we hypothesize that this difference stems from more frequent pain syndromes, visible physical changes, and complex treatment regimens in solid malignancies. This finding warrants particular attention in oncology practice, as solid tumors constitute 88% of our cases. Our findings reinforce the multidimensional nature of cancer-related distress, showing that emotional/spiritual, physical, and practical stressors are the most influential causes of patient distress. The magnitude of effect for emotional concerns (B = 2.30) highlights the substantial psychosocial burden experienced by cancer patients. Additionally, consistent with the literature, females reported significantly higher distress scores even when adjusting for other variables, which suggests that females may be more susceptible to high emotional impact due to cancer.
The study limitations include single-center design and unanalyzed stage-specific distress variations. However, there are several strengths including: robust sample size (n = 670) with sex-balanced representation, inclusion of both solid and liquid tumors, and pioneering data from Lebanon’s understudied context. These factors enhance the validity and regional relevance of our findings.
Conclusion
This study highlights the substantial burden of distress among cancer patients at our center, with 76% experiencing moderate-to-severe distress, predominantly driven by physical and emotional challenges. Given the alarmingly low referral rates to PC (only 1%), our findings underscore the urgent need for routine distress screening and timely integration of PC services in oncology care. Addressing these gaps could significantly enhance patient well-being, treatment adherence, and overall health care outcomes.
Future research should explore barriers to PC utilization and evaluate targeted interventions to improve distress management in low-resource settings. Such efforts will better equip health care providers, policymakers, and hospital administrators to meet international standards of comprehensive cancer care while optimizing health care resource allocation. By prioritizing psychosocial support and early PC, Lebanon can take critical steps toward alleviating suffering and improving quality of life for cancer patients.
Authors’ Contributions
R.Y. and H.O. conceived the idea and design of the study and wrote the article. L.H. recruited the subjects and collected their data. R.E.H. conducted the data analyses and generated results. All authors have read and approved the article.
Footnotes
Acknowledgments
The authors would like to thank Ms Sara Ajjour (AUB) for her assistance in the review and editing of the article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study did not receive any funding.
Supplemental Material
Abbreviations
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.