
Abstract
Background:
The COVID-19 pandemic exacerbated the need for palliative care (PC) and exposed gaps in PC provision in South Africa’s already-strained healthcare system. PC is a neglected yet core component of South Africa’s public healthcare sector.
Aim and objectives:
The study aimed to describe the impact of the COVID-19 pandemic on PC services in one healthcare district of South Africa, the Cape Metro Health District. Specifically, the study objectives were to describe the PC response to the COVID-19 pandemic, and healthcare managers’ perceptions of PC provision during the pandemic.
Methods:
Data for the study were derived from a desktop analysis of documents relating to PC service delivery over the pandemic, and from focus group discussions held with 19 senior healthcare managers.
Results:
The COVID-19 pandemic expedited integration of PC services into the health system and raised awareness of the importance of PC service delivery. It facilitated the allocation of increased resources (financial, infrastructural, and human resources) and enabled the rapid development of training material, in situ support for clinicians and the development of patient referral mechanisms. It was a stimulus for many people to learn about PC and influenced the perspectives of those working in healthcare, including managers, many of whom experienced the loss of family members or friends, foregrounding the importance of PC.
Conclusion:
Planning for future pandemics needs to include recognition of and ongoing care for palliative care patients and factoring in an increased demand.
Plain language summary
This study looked at how the COVID-19 pandemic affected palliative care (PC) services in the Cape Metro District of South Africa. Palliative care helps people with serious illnesses manage symptoms and improve their quality of life, especially near the end of life. Before the pandemic, palliative care was not well integrated into South Africa’s public healthcare system and lacked proper funding and support.
The COVID-19 crisis created an urgent need for better palliative care services. In response, the Cape Metro health system quickly increased resources adding more beds, staff, and equipment. New training materials were developed to help healthcare workers care for patients with COVID-19 who needed palliative care. Support for patients and families, including spiritual and emotional care, also became a focus.
The study used two methods to gather information: reviewing government documents and interviewing healthcare managers. Managers said that the pandemic helped raise awareness about the importance of palliative care and made them more compassionate in their work, especially as many had lost close family, friends and colleagues themselves.
As a result of the crisis, palliative care services, based on participant feedback and documents reviewed, improved and became more integrated into the public health system. The changes included faster referrals, better training, and more structured care plans.
However, there was a concern that these improvements could be lost without continued investment and planning.
The study concludes that palliative care must be included in all future emergency and health system plans. It also highlights the need for sustained funding, staff training, and policy support to ensure people receive the care they need during pandemic, post-pandemic and future health crises.
Introduction
Globally, there are inequities in the provision of palliative care (PC) between developed and developing countries, 1 and deficits in PC access to those eligible were highlighted before the COVID-19 pandemic. 2 PC access is a human right.2,3 The goal for patients with PC needs is freedom from unnecessary suffering, which requires attention to adequate housing, safe food and water, sanitation, and warmth. Early PC helps patients and families manage symptoms, prepare for end of life, and reduces unnecessary hospital admissions and utilisation of health services.4–6
Suffering and death brought on by the pandemic focused attention on the key role of PC and services, and led to calls for the immediate extended provision of PC during and after the pandemic. 7 The crisis exposed the global lack of integration between public health approaches and inequities in PC access. Individuals in impoverished or population-dense settings with weak health systems were less likely to access essential end-of-life care, 22 and the added burden placed on global health systems made the provision of effective PC more vital but difficult. A systematic review conducted by van Langen-Datta et al. 8 during the first 24 months of the pandemic, found that PC services are essential during the pandemic and provided an opportunity for advanced care planning. Furthermore, the integration of specialist PC into primary care and the community is required, along with the need for adequate hospice resourcing, improved access to multi-disciplinary team approach, and visible leadership.
South Africa’s PC services were rooted in the hospice movement, which began in 1979, as a stand-alone PC service. 9 Although PC initially focused on cancer, the HIV pandemic in the 1990s mobilised hospice-focused non-governmental organisations (NGOs) to respond to the end-of-life care needs of those dying at the time. These services occur outside of the public sector health services with the Hospice PC Association providing services through member hospices in communities through home-based care models and specialist inpatient services. 10 This history of PC in SA resulted in PC neglect and lack of integration within the public health services. The 2013 global study, conducted by Lynch et al. 11 that mapped levels of PC development, found that South Africa was one of 20 countries categorised as being in ‘Preliminary Integration’. In 2017, the National Policy and Strategy for PC (NPSFPC) 9 prescribed the integration of PC into the public sector healthcare system and the Western Cape Department of Health and Wellness (WCDHW) initiated a PC service without additional resources prior to the COVID-19 pandemic. However, SA remained at the stage of ‘Preliminary Integration’ along with 21 other countries in the recent Global Atlas for PC second edition (2020). 12
South Africa’s healthcare system was already under strain prior to COVID-19 due to ‘lack of human resources, poor governance and management, and unequal distribution of resources’ 13 . March 2020 marked the start of the global pandemic, challenging global health systems’ response to healthcare needs. The pandemic exacerbated the need for PC since more patients required this care, however, services were at the pre-pandemic state, further highlighting global inequities. 14 The South African healthcare system, like many others globally, sought to respond with agility to address the pandemic. 15 Our aim was to describe the impact of the COVID-19 pandemic on PC service delivery and the perspectives of public sector middle and senior health managers of PC in one district of South Africa during the first 18 months of the pandemic, and identify lessons learnt from their experiences. The research contributes to the body of knowledge on PC services specifically in low- and middle-income countries during times of crisis.
Methodology
Design
A descriptive qualitative study design was used, informed by a post-positivist theoretical assumption. 16 Data derived from a desktop analysis of documents relating to PC during the pandemic, a recognised qualitative analysis method. 17 Focus group discussions with healthcare management teams were conducted to elicit managers’ perspectives.
Study context
The study took place in Cape Town in the Western Cape province of South Africa. Known as the Cape Metro Health District and consisting of eight sub-districts that make up four sub-structures (SS1–SS4), the region is affected by a quadruple burden of disease that includes chronic diseases, communicable diseases such as HIV/AIDS and TB, injuries, and maternal and neonatal diseases due to poverty. 18 The Cape Metro health system forms part of the state-funded provincial health system and comprises tertiary and central, secondary/regional, district and specialised hospitals, and primary healthcare facilities including City Health municipal health services. Established stakeholder relationships exist between the provincial health system and NGOs, Higher Education Institutions, City Health, and the private healthcare sector. The first author is an embedded researcher within the WCDHW and serves as the chairperson of the provincial PC task team
Document selection, review, and analysis
All documents focusing on the keywords PC service provision and COVID-19 that were available in the WCDHW from the start of the pandemic (March 2020) until the start of the third wave (May 2021) were included and reviewed. Relevant documents published prior to March 2020 were also consulted for comparative purposes as well as reports that were published at a later date, but referred to the study period. The relevant documents (Appendix A) included policy documents, clinical guidelines, practice guides, internal memos and plans, working group reports, terms of reference documents and acts, and were accessed on the Western Cape Government website. Those not accessible on the website were requested from WCDHW officials as outlined in the approval letter to conduct the study.
WCDHW policy and other documents were included and systematically reviewed using the READ5F approach. 19 Firstly, materials focusing on PC and COVID-19 were read, followed by data extraction and capture of information along a timeline to paint a picture of PC processes and service provision from the pre-pandemic period until May 2021. Data analysis was iterative: the data were analysed as they were extracted with decision-making about which documents to include until a full picture emerged. The document review concluded once all documents pertaining to PC and COVID-19 within the study period had been identified and reviewed. 19 Content analysis was used to organise information into categories 17 according to the health system characteristics (governance and stewardship, financing, planning, service delivery, capacity planning, and access to essential medicines) of Atun et al.’s 20 conceptual framework for analysing integration of targeted health interventions into health systems.
Focus group discussions and analysis
Nineteen participants from two sub-structure management teams who were approached by email participated in this research. The participants were divided into two groups by sub-structure. They were managers from the senior management team for the sub-structures responsible for governance, stewardship, and strategic policy decision-making. A discussion guide (Appendix B) was used for the focus groups, which took place in 2021 during the third COVID-19 wave via MS Teams. Open-ended questions were asked regarding changes in approaches to PC and the impact of the COVID-19 pandemic on PC. The focus groups formed part of a larger study on PC integration into the health system. 21 For the purposes of this paper, we focus on PC in the context of COVID-19.
The two focus groups were moderated and led by the first author who had existing working relationships with approximately a third of the participants. The discussions lasted approximately 1 hour and were audio-recorded using a digital audio voice recorder and MS Teams. At the outset, participants were reminded that the proceedings were confidential. On completion, the recordings were downloaded from MS Teams and deleted from the online application. All recordings and field notes were transcribed verbatim by a professional transcriber and checked by the researcher before analysis.
The focus group data were analysed using small q, experiential, topic-summary thematic analysis, informed by a post-positivist epistemological stance, 16 prioritising participants’ accounts and focusing on the identification of patterns of meaning, key themes and concepts. 16 The researchers engaged in iterative processes of data immersion, coded the data into meaningful groups using NVivo (Lumivero), and developing thematic maps, followed by interpretive refinement. The reporting of this study conforms to COREQ (Supplemental Material). 22
Results
Increased resources were made available for PC during the COVID-19 pandemic, including financial, infrastructural, and human resource-related resources.23–25 In 2020, funding was allocated to PC as part of the COVID-19 emergency response budget. 25 Prior to the pandemic, the National Department of Health had not allocated a budget for PC despite formal funding requests. To respond to the growing need for PC services, the Western Cape PC task team (PCTT)26,27 and other key stakeholders rapidly responded with a plan that included increased infrastructural and human resources, rapid development of training material for healthcare workers, and formalised referral services for people needing palliative and bereavement care (Table 1) together with budget allocations. The PCTT drafted a position statement and plan for COVID-19 response, emphasising that PC is not only end-of-life care and should include patients and families. 26
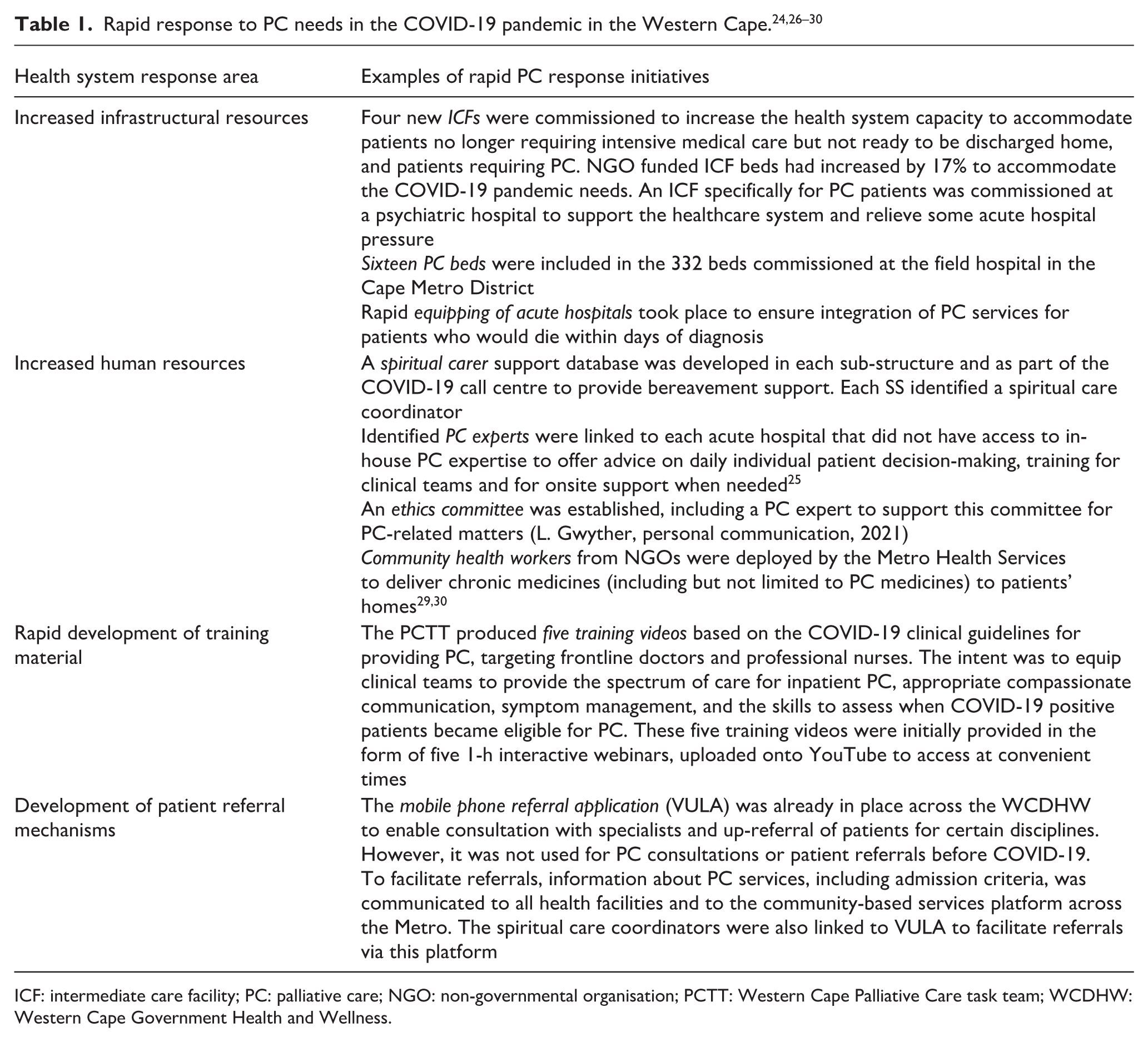
ICF: intermediate care facility; PC: palliative care; NGO: non-governmental organisation; PCTT: Western Cape Palliative Care task team; WCDHW: Western Cape Government Health and Wellness.
Increased infrastructural resources
An initial bed planning exercise was conducted by the provincial health data centre and PCTT members to determine the number of beds required for palliative and end-of-life care at all acute hospitals and stand-alone inpatient PC facilities across the province. The WC provincial health data centre developed a COVID-19 public health dashboard, which was launched just 7 weeks after the first confirmed case, and made accessible to all healthcare workers to facilitate facility-level pandemic planning and response. 31 Each facility was tasked with developing a PC plan to manage the flow of COVID-19 patients to ensure that the referral path for known PC patients differed from that of COVID-19 patients requiring PC. 26 To protect the already-compromised PC patients and preserve the intermediate care facilities (ICFs) for COVID-19 negative patients, alternative facilities were opened for COVID-19 positive patients. Table 2 summarises the facility levels and patient flow.
Western Cape COVID-19 palliative care response plan. 26
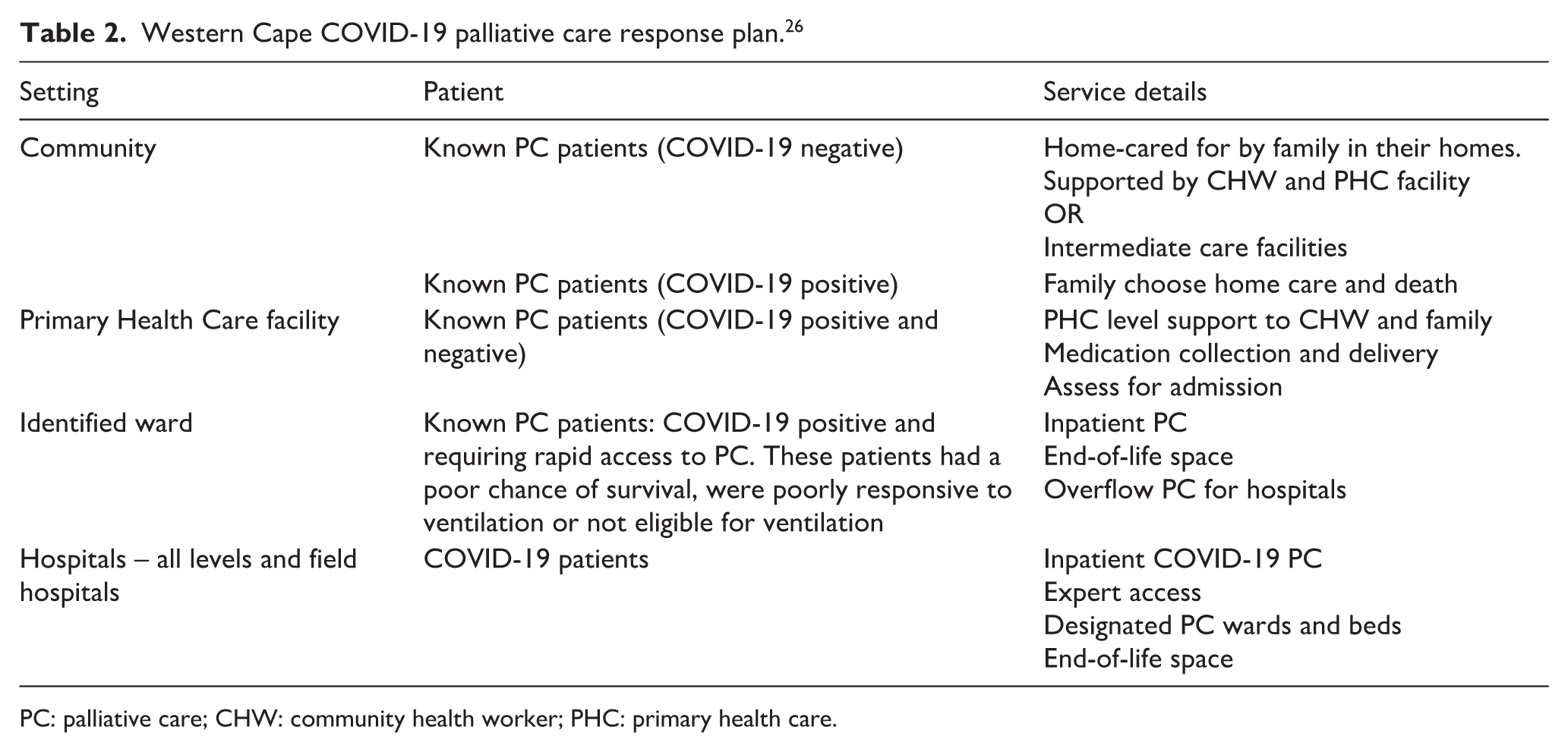
PC: palliative care; CHW: community health worker; PHC: primary health care.
In anticipation of the rapid increased need to accommodate COVID-19 patients, each SS made provision for PC and end-of-life care beds. In SS1, existing ICF beds were preserved for known or newly diagnosed PC patients who were COVID-19 negative and in July 2020, an additional 336-bed transitional care inpatient facility was opened for COVID-19 patients, including 16 beds for palliative and end-of-life care. While it was difficult to anticipate true need, this additional facility provided support to the entire Cape Metro District. In SS2, the ICF beds increased by 30 beds across four NGOs with all beds preserved for COVID-19 negative patients needing PC. In September 2020, SS3 worked with the NGO that provided intermediate care to expand its service and open a stand-alone 50-bed unit for PC of COVID-19 patients from the whole district. In November 2020, a 200-bed transitional care COVID-19 field hospital was opened, and in March 2021, the 50-bed stand-alone PC unit was decommissioned and incorporated into the field hospital (temporary hospital set up to provide emergency care). 23 The ICF beds in SS4 were preserved for known or newly diagnosed PC patients who were COVID-19 negative. An additional 800-bed transitional care field hospital was opened for 5 months and included beds for patients with PC and end-of-life care.
Increasing and reorientating human resources
The increased need for grief and bereavement support to family members brought on by an increase in the number of patients dying before PC could be offered, led to Metro Health Services actively recruiting volunteers from NGOs, faith-based organisations, community structures, and retired staff, to provide spiritual support. This included a nominated coordinator in each SS who established a volunteer database, linking them to training, facilitating referrals, and ensuring access to supervision. Volunteers at the provincial call centre also provided spiritual support to patients and families. 32
PC experts were identified and linked to acute hospitals lacking in-house PC expertise 25 and included in the newly established Provincial Ethics Committee for support (L. Gwyther, personal communication, 2021). At the same time, many NGO services, which included support to PC patients, were reduced to accommodate the pressing need of home delivery of chronic medication parcels for chronic service patients. 34 Decongesting heath facilities reduced infection risk of vulnerable people.30,33,34 Within 6 months, 760,812 chronic medicine parcels were successfully delivered to patients’ homes by community health workers. 24
Rapid development of training material
The need for PC training significantly increased during the pandemic but face-to-face training was not possible. The PCTT rapidly produced five training videos (Table 3) focusing on equipping clinical teams to provide the spectrum of care for inpatient PC, appropriate compassionate communication, symptom management, and skills to assess when COVID-19 positive patients became eligible for PC.
Palliative care training videos.
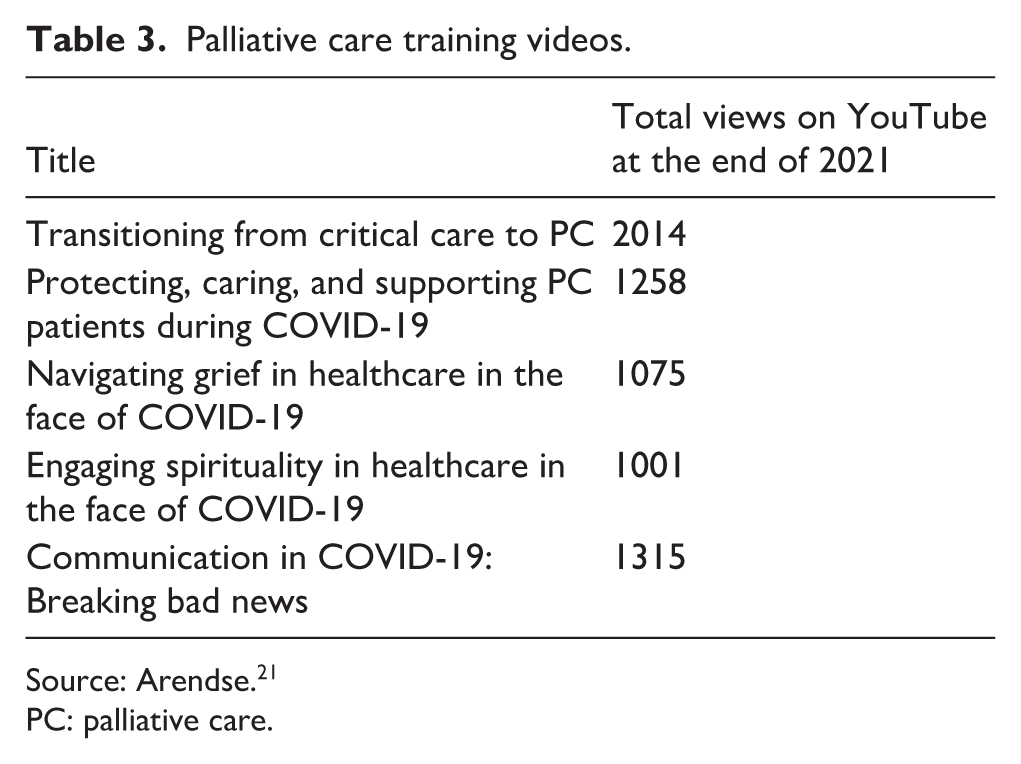
Source: Arendse. 21
PC: palliative care.
Development of patient referral mechanisms
In 2019, the WCDHW lacked one standardised PC referral policy. Patients receiving care in some hospitals were down-referred for further care to primary healthcare services, using the electronic continuity of care discharge summary. 35 The process varied based on whether liaison had been established between the referring health facilities, and relied on the patient presenting at the referral facility. By 2021, the referral pathways for patients in need of PC had improved due to the relationships formed, liaisons established, and need for PC highlighted during the pandemic. 36 The mobile phone referral application (VULA) enabled consultation with specialists and up-referral of patients to specialised services in certain disciplines. To facilitate referrals, information about PC services, including admission criteria, was communicated to all health facilities and to the community-based services platform across the Cape Metro through emails to facility managers and funded NGOs.23,28 The spiritual care coordinators were also linked to VULA to facilitate referrals via this platform. 37
Managers’ perceptions regarding PC provision during the COVID-19 pandemic
The profile of the 19 sub-structure management team members is provided in Table 4 (n = 19).
Profile of the sub-structure management teams (n=19).
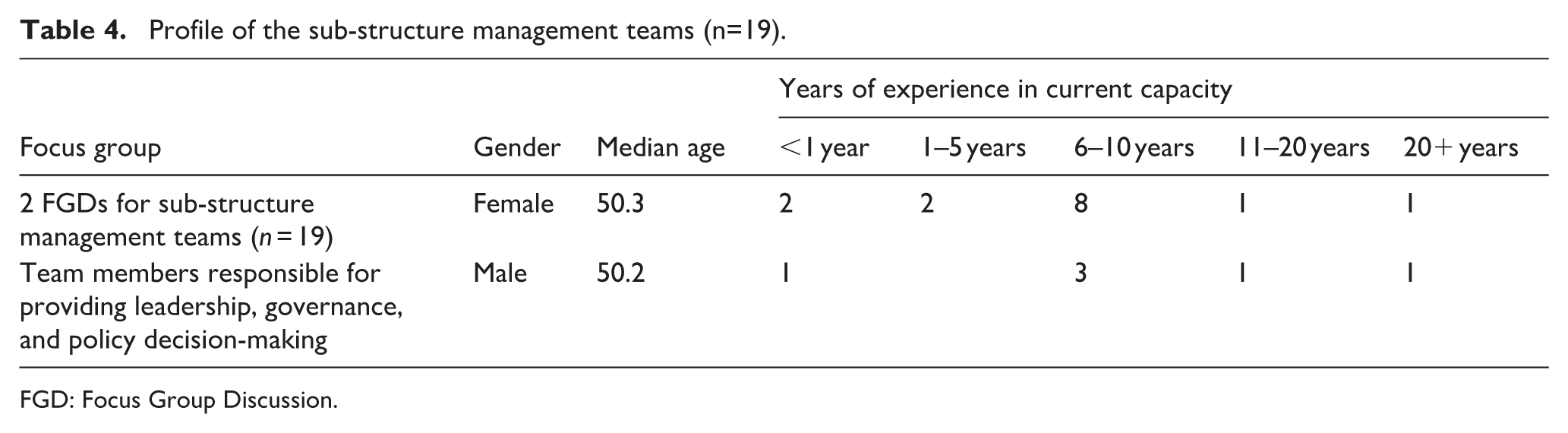
FGD: Focus Group Discussion.
Two subthemes emerged: ‘How the pandemic reshaped the meaning and practice of palliative care’ and ‘Reconfiguring compassion during the COVID-19 pandemic’.
How the pandemic reshaped the meaning and practice of palliative care
Prior to the pandemic, participants were starting to implement the PC policy. With the pandemic onset, the need for rapid integrated PC services dramatically increased. Informants felt vulnerable when the extent of the PC service gap became evident. They felt hopeless and overwhelmed by the number of patients entering the healthcare system. Some had to support the internal medicine teams in making decisions about which patients qualified for intensive care and ventilation. They rallied to support colleagues with the increased burden of updating patients’ families. The ‘no visitors’ policy compromised much-needed support to patients from their family members.
Nobody was ready for COVID. . . most of the patients were classified under the PC radar. From a nursing perspective. . . you couldn’t really deviate your thinking from PC versus any other care. (Focus Group 2, Senior management team member A)
The rapid response and guidance from the Metro Health Services through circulars, clinical guidelines, training videos, and virtual meetings helped managers to support the implementing teams who offer PC services.
There was a palliative care PACK guideline very quickly and that also helped to integrate palliative care in what we do . . . it was very clear. (Focus Group 1, Senior management team member B)
They valued the nationally amended supply chain management delegation that allowed for rapid procurement of equipment for PC. Much of the red tape was removed and the daily petty cash limit was increased. This streamlined procurement time and allowed for purchasing of equipment and consumables at a much lower price.
People in supply chain was willing, we didn’t have to sit for months and motivate why you needed something. It was understood . . . for us to get the phone, to get the airtime to [allow video calls between patients and family] . . . that definitely facilitated [and] enabled that. (Focus Group 1, Senior management team member C)
Reconfiguring compassion during the COVID-19 pandemic
Informants shared personal experiences of losing family, friends, and colleagues, and reflected on the immense pain and sadness they experienced. Some shared that their teams felt valued when they went to the shops after work and were fast-tracked in queues or given tokens of appreciation as frontline staff. Compassion from others influenced their expression of compassion towards colleagues, patients, and family members.
Faced with a pandemic [compassion] kicks in, because . . . you’re not only experiencing that with a patient, you’re experiencing that with your own family, your own friends. . .. (Focus Group 1, Senior management team member D)
Informants emphasised the challenges of providing care during the pandemic, and how this inability to access healthcare violated the patient’s human right to care and dying with dignity with family involvement. Families could not access patients who were admitted, especially when the patients’ conditions suddenly changed and the video call communication with families and identified close contacts 38 was not adequate. These managers shared their feelings of helplessness.
COVID robbed us of the care . . . people [are] supposed to receive . . . It was not easy to convey messages. . . The only voice [families] could relate to was that of the staff in that ward. And tomorrow . . . the [patient’s] condition has changed completely. How does it happen that I speak to the doctor or nurse today, and they tell me my mother is doing well? And then . . . in the evening, . . . the condition has changed or you receive news that they are no longer with us. (Focus Group 2, Senior management team member E)
Informants from both focus groups shared about their journey in caring for and supporting each other, and their teams, irrespective of rank. This is not common within hierarchical structures in a bureaucratic system. They reflected that pulling together as one team was the only way to survive the devastation of this pandemic. They regarded the pandemic as the catalyst for compassion.
I think it was the great teamwork . . . We may not have been fully ready for the impact of COVID. But what happened is we rapidly got together and . . .I think standing together and working as a team, . . . all the role players came together and willingly worked their fingers to the bone to put the systems in place and to reach out and do as we needed to. (Focus Group 2, Senior management team member F)
Discussion
The challenges and devastation of the pandemic cannot be downplayed and as death rates increased, so did the urgent need for access to the rapid provision of PC. 39 Rodin et al. confirm that this was the case globally. 2 Although the delivery of traditional PC services was disrupted and the gaps in PC were exposed, this study found that the COVID-19 pandemic accelerated the integration of PC services into the health system and increased awareness of it’s importance.
The further advantage that the WCDHW had was the already established PCTT and the subsequent rapid development of the Provincial Palliative Care Position Statement & Plan for COVID-19 Response, very early in the pandemic. This plan, amongst others, provided the guidance that the public healthcare sector on the provision of PC beds for COVID-19 positive patients, and the NGO sector on the provision of PC beds for COVID-19 negative PC patients. 26 The need for and provision of additional PC beds was confirmed in the report published by the SA Medical Research Council that found that over the period 1 March 2020 to 8 February 2021, 85%–95% of excess natural deaths in SA was because of COVID-19. 40 According to Janssen and van der Voort, agile governance was necessary, and depends on ‘working practices and methods that facilitate quick responses’, which is further enhanced by access to the software that aids rapid decision-making. 15 This need to respond rapidly to the growing need was met with increased access to resources (financial, infrastructural, and human resources) and devolved financial and supply chain decision-making power to healthcare managers at institutional level. While this worked well in an emergency such as the pandemic for the rapid procurement of necessary equipment, it was not sustained beyond the pandemic due to a risk of corruption.41,42 Mathiba reported on the extensive procurement corruption in SA during the pandemic. 43 This study confirmed that the integration of PC will require ongoing funding, particularly as this relates to the ongoing need for PC-related consumables, equipment, and training.
The study showed that the pandemic’s demand for rapid development of training resources and swift rollout of diverse PC training – supported by in situ PC experts – acted as a catalyst for increasing awareness and understanding of PC. Managers perceived these accelerated initiatives as a demonstration of prompt, tangible support for frontline staff from senior leadership at Metro District and Provincial levels. This environment not only fast-tracked PC capacity but also stimulated widespread learning about PC, reshaping how frontline workers, including managers, understood its role and value. Ultimately, the pandemic created an unprecedented momentum for the embedding of PC knowledge as an essential component of frontline healthcare practice.
Spiritual care is a core component of PC, but it was not fully integrated into practice 44 or prioritised as an essential service within the Metro Health Services, prior to the pandemic. As was found globally, 44 this study showed that the urgent need during the pandemic facilitated the rapid establishment of this service, and that managers should recommit to the ongoing provision of spiritual care.
The District Health System model was implemented in the WCDHW in 2007, positioning middle and senior management intentionally in touch with health facilities. 45 This facilitated their ability to provide support, which included PC decision-making, to clinical teams regarding during the pandemic. Our study showed that crisis does not necessarily lead to disillusionment when management are connected to healthcare workers at the frontline, as this makes for trust and change. 46 This study showed that many managers experienced the loss of family members or friends as a result of the pandemic, meaning that no one was exempted, and foregrounding the importance of PC. The FDG in itself provided a safe space for these managers who share about their vulnerabilities, feelings of hopelessness, and helplessness. Furthermore, the general public displayed compassion to healthcare workers, managers felt compassion to one another and to other colleagues with no regard for hierarchical structure, this was not the local and global reality prior to the pandemic.47,48 Essentially, this study showed that the pandemic was a catalyst that challenged the healthcare system to respond by ensuring rapid access to quality PC for patients and their families and brought compassionate care back into the health system. A multinational study conducted by Matos et al. confirmed an increase in compassion with a decrease in the fear of compassion during the pandemic. 47
This study confirmed that COVID-19 highlighted the need for pandemic preparedness to include the provision of PC at all levels of care, 46 including the home environment, for severely ill and dying patients and their relatives. 49 The pandemic burden surpassed global health systems’ capacity, making integration of PC into COVID-19 pandemic planning essential, 50 although this was done in a reactive way. Pandemic planning included the provision of treatment algorithms to guide decision-making on the rationing of care, rapid training on effective symptom control, PC interventions and principles, and other forms of providing care such as telemedicine 51 and death and bereavement support to surviving family members. 32 Pandemic preparedness must include PC. 8
Conclusion
We found that an enabling culture, senior management buy-in and existing relationships with the PC community and the PCTT, had set the foundation for the increased demand for PC that came with the COVID-19 pandemic. This included ongoing equitable redistribution of existing financial resources for the integration of PC into the public sector health services, in particular for PC-related consumables, equipment, and training. We also identified that while spiritual care, as a core component of PC has gained momentum during the pandemic, to ensure sustainability it will need a compassionate health system with compassionate people to recognise its value to the patients, their families and close friends.
Finally, this study demonstrated that a crisis, such as COVID-19 pandemic, does not mean that the health system will fall apart, as a health system with adequate governance, can pool resources and expertise, to survive it. But to be prepared for future crisis, we found that it is important to invest in emergency and disaster preparedness and response that integrates PC.
Supplemental Material
sj-pdf-1-pcr-10.1177_26323524261435131 – Supplemental material for Impact of the COVID-19 pandemic on palliative care services in the Cape Metro District of South Africa
Supplemental material, sj-pdf-1-pcr-10.1177_26323524261435131 for Impact of the COVID-19 pandemic on palliative care services in the Cape Metro District of South Africa by Juanita O. Arendse, Virginia Zweigenthal and Liz Gwyther in Palliative Care and Social Practice
Footnotes
Appendix A: Documents reviewed for document analysis
Cloete KR. Organisational Redesign Journey MDP Stock-take. In: Wellness WCGHa, editor. Western Cape, 2022.
Disaster Management Act (57/2002): Regulations made in terms of Section 27(2) by the Minister of Cooperative Governance and Traditional Affairs No. 43148, Vol. 657, 2020.
Goliath C. Home deliveries of chronic medication. Chronic Disease Service Coordinating Workgroup, 2020.
Gwyther E. Personal communication regarding palliative care expert access from the Ethics Committee. In: Arendse JO, editor. Unpublished 2021.
Metro Health Services. District Health Plan 2021/22 to 2023/24: Cape Metro Health Service District. In: Health, editor. Cape Metro District: Metro Health Services & City Health, 2021.
Metro Health Services. Internal Memorandum MHS 06 of 2020: De-escalation of Services at Primary Health Care (PHC) facilities in the Cape Metro during National Lockdown – Guidelines for PHC Facility Managers. In: Health, editor. Cape Metro District: Metro Health Services, 2020.
Metro Health Services. Palliative Care Policy Implementation Task Team. Terms of Reference. Cape Town Metro District: Metro Health Services, 2017, p. 3.
Metro Health Services. Internal Memorandum: MHS 09 of 2020 HCBS Programme and Information Management Standard Operating Procedure. In: MHS CD, editor. Cape Town, 2020, p. 22.
Metro Health Services. COVID-19 Risk Reduction Plan, Decongesting current services – Home drop-off of CDU parcels by CHWs. In: MHS CD, editor. Cape Town, 2020.
Morgan J. Report on Palliative Care support during COVID-19. Metro Health Services, 2021.
National Department of Health, South Africa. National Policy Framework and Strategy on Palliative Care 2017–2022. Pretoria: NDoH, 2017, https://www.health.gov.za/wp-content/uploads/2020/11/NationalPolicyFrameworkandStrategyonPalliativeCare20172022.pdf.
Peters F. COVID-19 Palliative Care Ward. Unpublished: Klipfontein Mitchell’s Plain Sub-Structure: Metro Health Services, 2022.
Peters F. Mitchells Plain COVID-19 Intermediate and Palliative Care Admission Criteria. In: Sub-Structure KMP, editor. WCGHW. Cape Town: Metro Health Services, 2020, p. 1.
Western Cape Government. Circular H67 of 2020: Provincial Palliative Care Position Statement and Plan for COVID-19 Response. In: Health, editor. Cape Town: Western Cape Government Health, 2020, p. 137.
Western Cape Government. Circular H79-2020: Clinical guidelines: COVID-19 providing PC. In: Health, editor. Western Cape: Western Cape Government Health, 2020, p. 41.
Western Cape Government. Proposed model for the implementation of the palliative care policy in the Western Cape. In: Health, editor. Cape Town: Western Cape Government Health, 2018.
Western Cape Government. Annual Performance Plan 2018–2019. In: Health, editor. Western Cape: Western Cape Government Health, 2018, p. 197.
Western Cape Government. Annual Performance Plan 2021–2022. In: Health, editor. Cape Town: Western Cape Government Health, 2021, p. 160.
Western Cape Government. Policy Framework on Intermediate Care Circular No. 154 of 2012. In: Health, editor. Cape Town: Western Cape Government Health, 2012, p. 14.
Appendix B: Focus group discussion guide
Acknowledgements
This article is based on research originally conducted as part of Juanita O. Arendse’s doctoral thesis titled ‘An Assessment of the Integration of Palliative Care in the Health System of the Cape Metro District of South Africa’, submitted to the School of Public Health and Family Medicine, Faculty of Health Sciences, University of Cape Town in 2023. The thesis was supervised by Virginia Zweigenthal, PhD and Liz Gwyther, PhD. The manuscript has since been revised and adapted for journal publication. The original thesis is available at: ![]() . The authors acknowledge Michelle Pascoe, PhD, for editing a draft of this manuscript.
. The authors acknowledge Michelle Pascoe, PhD, for editing a draft of this manuscript.
Ethical considerations
Ethics approval (HREC REF: 058/2019) was obtained from the University of Cape Town Faculty of Health Sciences Human Research Ethics Committee, and permission was given by the Western Cape Government Health and Wellness department to access documents not in the public domain. Beneficence and justice were considered throughout to ensure non-maleficence and that participants were treated fairly and impartially. All transcripts were anonymised, all identifiers removed, and pseudonyms used.
Consent to participate
Informed written consent was obtained from all participants, and their identities, perspectives, and the record of discussions were kept confidential, known only to the researchers.
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research received some financial support from the NIH award U54CA284030.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of data and materials
The authors confirm that the data supporting the findings of this study are available within the article [and/or] its Supplemental Materials.
Disclaimer
The views expressed in the submitted article are the authors’ own and not an official position of their institutions.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.