
Abstract
This case-based report compares two residents experiencing progressive neuromuscular diseases who transitioned from palliative care to hospice and underwent ventilator discontinuation in a rural long-term care (LTC) facility. With a focus on effective interprofessional collaboration and communication, it highlights a coordinated approach while navigating system-level barriers, process challenges, and the emotional, cultural, and ethical complexities of goal-concordant end-of-life care. In the absence of well-documented protocols, ventilator discontinuation is feasible in rural LTC settings. To improve the quality of this care option, policies are needed to support the development of standardized practice guidelines, ensure simulation-based staff education to improve coordination, and enhance access to essential resources for residents, their families, and health care clinicians in the LTC setting.
Keywords
Introduction
Individuals requiring prolonged mechanical ventilation often experience poor clinical outcomes, including increased morbidity and mortality. Approximately 20% of patients on mechanical ventilation and/or their surrogate decision maker will elect ventilator discontinuation with the goal of alleviating suffering and minimizing respiratory distress at the end-of-life. 1 While the preferred place of death for most patients is home, the barriers to a home death for patients on mechanical ventilation in the acute care setting are so great that this is often not feasible. 2 For individuals residing in a long-term care (LTC) environment, “home” is where one lives and also receives care, which would include the management of mechanical ventilation when necessary. This case report will provide two examples of mechanical ventilator discontinuation in LTC and highlights the challenges and opportunities for this treatment approach in a rural setting.
Background
Ventilator discontinuation, also referred to as palliative extubation, compassionate ventilator withdrawal, and/or terminal ventilator weaning, is a complex process that involves expertise with mechanical ventilation. 3 For clarity, weaning is the act of decreasing oxygenation and ventilatory support via the mechanical ventilator and allowing the patient to assume greater control of breathing. 4 Extubation is the liberation from mechanical ventilation, and involves the discontinuation of respiratory support and removal of an artificial airway or endotracheal tube. 4 Ventilator discontinuation describes the immediate removal of ventilatory support while an artificial airway (tracheostomy) remains in place. Patients undergoing ventilator discontinuation can experience intense dyspnea, hypopnea, apnea, or cough, and if not well-supported, unnecessary suffering. 1 Individualized treatment plans, which include the administration of opioids and anxiolytics, are the preferred approach to symptom management. 2
Mechanical ventilation and LTC
Most existing literature on ventilator discontinuation focuses on intensive care units, inpatient hospices, or palliative care units. 5 When aggressive medical interventions no longer align with a patient’s goals of care, patients and surrogate decision-makers may elect to discontinue ventilatory support. In such instances, care teams must possess the knowledge and interprofessional expertise to guide a coordinated and compassionate withdrawal process. 2 For patients who are medically stable yet dependent on prolonged mechanical ventilation, a transfer to a skilled nursing facility with a specialized ventilator unit may occur. Despite the increasing prevalence of such scenarios, the processes and outcomes surrounding ventilator discontinuation in LTC settings remain poorly studied and infrequently documented. 6 This evidence gap limits the development of best practices and may hinder the provision of goal-concordant, ethically sound end-of-life care. Without evidence-based guidance, LTC facilities must navigate ventilator withdrawal within a framework designed primarily for rehabilitation rather than end-of-life care.
LTC settings are governed by regulatory standards that emphasize rehabilitation and/or maintenance of function. When residents experience a significant decline in health, the shift in focus from restorative to comfort-oriented care often conflicts with the prevailing culture of recovery. Discontinuation of ventilatory support illustrates this tension, as it challenges the facility’s federally mandated approaches to resident care. In LTC, direct care staff and contracted professionals (including respiratory therapists) who have invested substantial time and emotional energy in residents’ recovery may experience moral and existential distress when care transitions toward ventilator withdrawal, particularly if they witness patient suffering. 1 The introduction of external hospice or consultative palliative care providers can further disrupt established relationships among residents, families, and staff, especially when those providers have not developed trust or familiarity within the care community. These challenges can lead to communication barriers and fragmented decision-making. In rural or underserved regions, limited access to trained clinicians and essential medications for symptom management further compounds these challenges, making it increasingly difficult to deliver coordinated and compassionate end-of-life care.
Guidelines for ventilator discontinuation
Clinicians assisting residents and families with ventilator discontinuation support the development of guidelines for a coordinated and interprofessional approach to increase staff comfort and confidence, ensure symptom management needs are met, and reduce distress for residents, family members, and themselves. 4 While there is limited consensus among experts regarding best practices, 4 a well-developed plan for ventilator discontinuation includes an aggressive approach to symptom management both before and after ventilatory support is discontinued. 1 The existing body of literature describes “a lack of a standard, objective measure for detecting respiratory distress to guide the process and high variability in initiation and escalation of opioids and sedatives.” 7 In addition to standardized assessment and symptom management algorithms, the plan for ventilator discontinuation in LTC should also include additional education and support that addresses the potential emotional burden experienced by family members and health care staff. The complex nature of ventilator discontinuation requires all involved to work together to mitigate the challenges by delivering care that is concordant with the resident’s and family’s expressed wishes and supportive of the interprofessional team (IPT) members involved.
Case Description
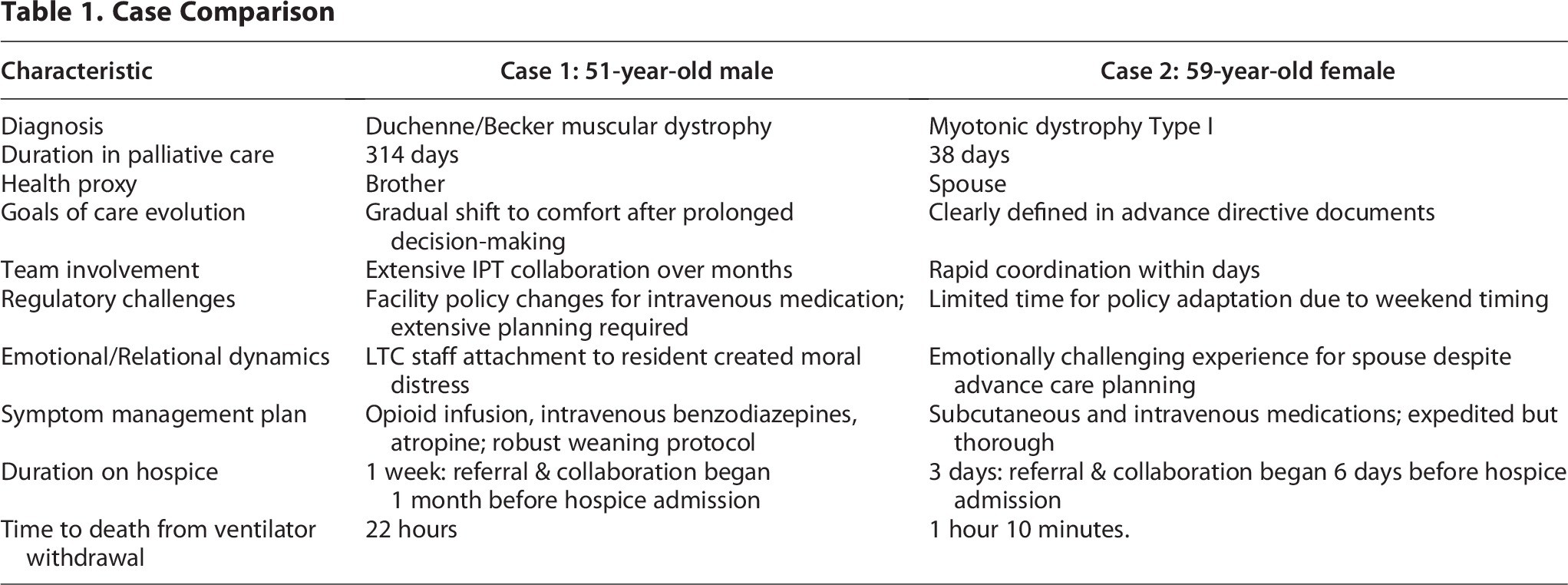
For this case report, ventilator discontinuation refers to the cessation of mechanical ventilation for a patient while an artificial airway (tracheostomy) remains in place. Additionally, patients are referred to as “residents” since the LTC setting is the individual’s place of residence. Table 1 provides a side-by-side comparison of two cases illustrating key information, including the time spent in care transitions, interpersonal, interprofessional, and system-level dynamics, and clinical and ethical complexities encountered in a rural LTC setting.
Case Comparison
The two cases described in this report occurred in Berkshire County in western Massachusetts, USA, with a population of 129,026 as of the 2020 Census data. 8 In this predominantly rural region, access to specialty palliative care in the community is limited, consisting of a physician with part-time availability at an outpatient cancer center and a nurse practitioner employed by a community-based organization providing specialty palliative care in patients’ homes and affiliated skilled nursing facilities. The clinical circumstances and service configuration described in this report reflect the local context, and findings may not be generalizable to other regions in the United States or internationally.
Case 1
Mr. X was a 51-year-old male with Duchenne/Becker muscular dystrophy and chronic respiratory failure dependent on a ventilator via tracheostomy. He had a history of nonischemic cardiomyopathy with a biventricular implantable cardioverter defibrillator and chronic atrial fibrillation. The resident received medically administered nutrition via gastrostomy tube.
He received palliative care for 314 days prior to hospice admission, maintaining a Palliative Performance Scale (PPS) of 30%. The resident’s medical decision-making capacity was determined by the primary team prior to palliative care involvement. Early in his course, he was awake and able to participate in conversations using a speaking valve. Following the capacity determination, he continued to convey his wishes to his brother, who served as the invoked health care proxy (HCP). The palliative care course was characterized by ongoing symptom management and regular discussions regarding disease progression, prognosis, and evolving goals of care with the invoked HCP. From the outset, the medical goal was comfort-focused, with a Medical Order for Life Sustaining Treatment indicating do-not-resuscitate status. Initially, the HCP wished to continue ventilatory support and medically administered nutrition.
Over time, the resident experienced progressive weakness, intermittent fatigue, and pain necessitating frequent adjustments to his analgesic regimen. Approximately 3.5 months post-admission, he could no longer produce words or sounds with the speaking valve; thereafter, the invoked HCP spoke on his behalf. At eight months, further decline was noted, including increased verbal and nonverbal communication difficulties, bilateral upper extremity edema, and increasing lethargy. At 10 months, ongoing discussion with the HCP addressed the resident’s continued decline and the limited likelihood of improvement. Ultimately, the HCP opted for a comfort-based approach, declining further aggressive interventions. Hospice services, including ventilator discontinuation and defibrillator deactivation, were recommended and accepted.
Hospice referral was initiated over a month prior to the planned discontinuation of ventilatory support. The hospice social worker engaged the HCP early to discuss expectations and provide support. An initial IPT meeting, which included the palliative care provider, hospice team, system-wide organizational leadership, and facility quality assurance staff, was convened to review the case to address ethical considerations and the plan for ventilator discontinuation. The goals of the IPT included addressing facility policies, ensuring provider presence during the procedure, and assessing the emotional, psychological, and spiritual needs of all involved. IPT meetings occurred every three days leading up to the discontinuation and expanded to include hospice and facility nurses, pharmacists, respiratory therapists, a pulmonologist, intravenous therapy clinicians, a social worker, and a spiritual counselor. The HCP participated in the final IPT meeting prior to discontinuation.
Hospice admission occurred six days prior to the scheduled date for ventilator discontinuation. Symptom management planning began immediately, with interprofessional coordination to ensure comprehensive interventions before, during, and after the procedure. Plans were made to deactivate the resident’s automatic implantable cardioverter-defibrillator, and all nonessential medications were discontinued. Tube feedings were stopped 24 hours prior to ventilator discontinuation. A peripherally inserted central catheter was placed in anticipation of intravenous opioid and benzodiazepine administration during the discontinuation process. The resident, previously receiving scheduled lorazepam and morphine via gastrostomy tube, was transitioned to a hydromorphone infusion one day prior (parenteral morphine was unavailable due to drug shortages). Injectable diazepam was prescribed and dosed according to onset of action, rather than duration, per hospice pharmacy consultation (parenteral Lorazepam was unavailable due to drug shortages). Atropine drops were ordered for potential management of distressing tracheal secretions.
At the time of ventilator discontinuation, the resident was unresponsive. The hospice registered nurse remained at the bedside alongside the facility registered nurse and the attending provider, offering real-time recommendations for symptom management based on frequent assessments of nonverbal indicators of distress using a modified FLACC (Face, Legs, Activity, Cry, Consolability) scale. The FLACC scale is an observational tool used to assess pain and distress in individuals unable to self-report, such as nonverbal or cognitively impaired patients. The hospice social worker and spiritual counselor provided anticipatory guidance and emotional-spiritual support to both family and staff. The resident died peacefully the day following discontinuation of ventilatory support. In Case 1, key challenges for the team included facility policy limitations on medication administration and medication accessibility.
Case 2
Ms. Y was a 59-year-old female with myotonic dystrophy type I and dependence on ventilator support via tracheostomy. She had a history of an anoxic brain injury, tachyarrhythmia status post pacemaker placement, depression, anxiety, and a suicide attempt. During the initial palliative care consultation, which occurred prior to the Christmas holiday, her spouse (designated as the resident’s HCP) communicated that the resident had documented her end-of-life wishes in a living will. In accordance with these directives, the spouse expressed a desire to proceed with ventilator discontinuation.
The resident received palliative care for 38 days prior to hospice admission, during which the resident’s PPS ranged between 10% and 20%. The palliative care nurse practitioner facilitated discussions with the spouse to clarify the resident’s wishes and provided education regarding hospice services and the ventilator discontinuation process to the spouse and the LTC care staff. Following the holiday, the spouse reaffirmed the decision to pursue hospice and discontinue ventilatory support, and a date was set for the procedure. The spouse requested that arrangements for a celebration of life occur simultaneously, which added another layer of complexity given the situation. The anticipated discontinuation date and hospice admission occurred during a compressed timeline, which meant IPT meetings and medication planning had to be expedited.
IPT meetings occurred on three occasions, up to the day before the discontinuation of ventilatory support, with the spouse participating in the final meeting. Hospice admission occurred three days prior to the scheduled date for ventilator discontinuation. Symptom management planning occurred over a brief period of time and was complicated by limited resources over a weekend. All nonessential medications were discontinued. Tube feedings were stopped 24 hours prior to ventilator discontinuation. A midline catheter was placed in anticipation of intravenous opioid and benzodiazepine administration during the discontinuation process. The resident, also previously receiving scheduled lorazepam and morphine via gastrostomy tube, was transitioned to morphine via parenteral infusion one day prior. Injectable lorazepam was prescribed and dosed according to onset of action, rather than duration, per hospice pharmacy consultation. Atropine drops were ordered for potential management of distressing tracheal secretions.
As in case 1, the hospice registered nurse remained at the bedside alongside the facility registered nurse and the attending provider, offering real-time recommendations for symptom management based on frequent assessments of nonverbal indicators of distress using a modified FLACC scale. The hospice social worker and spiritual counselor provided comprehensive support and education to staff and the spouse. The resident died shortly after the discontinuation of ventilatory support with symptoms well-managed. For Case 2, key challenges for the team included establishing communication with the HCP and expeditious coordination of care.
Discussion
System-level and process challenges
Both cases illustrate barriers to ventilator discontinuation in rural, nonhospital settings as reported by Kaur et al. 5 Nearly two-thirds of patients in hospice settings experience respiratory distress despite pre-medication, emphasizing the consequences of potential medication delays. 5 Limited access to essential medications, reduced staffing and pharmacy support during evenings, weekends, and holidays, and restrictive intravenous medication policies impact timely, symptom-focused care. Many LTC facilities also lack standardized protocols, adequate staff training, and the expertise needed to manage complex ventilator discontinuation, creating vulnerabilities for residents, families, and caregivers. Timely planning in Case 1 allowed the IPT to address these gaps by revising restrictive policies, ensuring medication availability, and providing psychosocial and spiritual support.
In contrast, Case 2 progressed quickly after a holiday, exposing weaknesses in after-hours coverage, communication, and team collaboration. Aguilar and Nicastro 9 acknowledge these weaknesses, including supply chain issues, gaps in training, and provider hesitation, as barriers to care consistency, with a need for clear protocols, proactive planning, and ongoing education. These cases underscore the need for systemic reform and consistent processes. Standardized protocols, proactive planning, reliable medication access, structured workflows, and early engagement of social work and spiritual care can reduce delays, support staff, and promote compassionate, goal-concordant care outside the hospital.
Relational, cultural, ethical, and existential dimensions
The emotional and ethical landscape surrounding ventilator discontinuation was unique in each case. In Case 1, long-standing staff relationships with the resident created deep moral and emotional complexity, especially during a prolonged transition from curative to comfort-focused care. In contrast, Case 2 involved earlier goal alignment between the patient and HCP, which reduced emotional ambiguity. Even so, both cases required careful attention to the emotional readiness of families and care teams, with a focus on providing space and opportunity for emotional and spiritual support before, during, and after ventilator discontinuation. Uncertainty about timing and outcomes added to the ethical weight of the process. Additionally, in Case 1, regular family meetings, interprofessional coordination, and the integration of spiritual and early bereavement care were essential in helping everyone involved find meaning and peace during a difficult transition.
These themes echo prior literature. Ankrom et al. 10 described the nuanced emotional and logistical terrain of ventilator discontinuation in chronic care settings, emphasizing the need for relational sensitivity and structured team planning. Aguilar and Nicastro 9 reinforced the importance of cultural alignment, trust, and interprofessional support. Kaur et al. 1 found that 65% of clinicians involved in discontinuation reported moderate to high emotional burden, with nearly one-third at risk for post-traumatic stress disorder when institutional processes were unclear. Ethical frameworks such as the principle of double effect described by Potter et al. 11 can help teams navigate these situations with confidence, affirming that relieving suffering remains ethically sound even if death is hastened as a result.
Conclusion
The cases presented highlight the need to support a coordinated approach to ventilator discontinuation in LTC and rural community settings at both national and institutional levels. Advance care planning should begin early, ideally when ventilator support is first initiated, so that future ventilator discontinuation can be approached with clarity and shared understanding. Simulation-based training and structured frameworks (e.g., the Respiratory Distress Observation Scale, Campbell’s algorithm) can support preparedness, reduce variability in care, 12 and strengthen team readiness for these complex scenarios, a theme also supported by Yeow and Chen. 3 Policy initiatives should promote consistent standards while allowing room for individualized care and always ensure access to essential medications and equipment to support the delivery of high-quality palliative and end-of-life care.
Change will require alignment in ventilator support practices. 13 Coordinated ventilator discontinuation is feasible in rural LTC settings, but it demands preparation, strong leadership, and systems that ensure ethical clarity and clinical adaptability, supported by guidelines that reflect the complexity of this care.
Footnotes
Author Disclosure Statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding Information
No funding was received for this article.