
Abstract
Introduction:
Hospice care (HC) in the Netherlands is available for patients with life expectancies <3 months. Little is known about expectations of patients who might be in need of HC. This study aims to gain insight into expectations of patients regarding HC in order to ameliorate HC to become driven by patient needs.
Design:
A generic qualitative study, using semistructured interviews and thematic analysis, is performed in the Netherlands from January to June 2018. A purposeful sample of 13 participants was drawn.
Results:
Participants expected hospice admission only when the burden became unbearable and a home death cannot be reached. Participants expected a homely atmosphere, where one can continue the life lived at home as much as possible. Participants supposed empathic professional caregivers, capable of providing appropriate care. The general practitioner is expected to stay involved in the care process due to the mutual trust. Medical and daily care are required to be provided by competent professionals, where volunteers are expected to provide supportive care. All caregivers are supposed to provide a listening ear and “being there” for participants. Social care and spiritual care are generally projected to be private matters, unless it is requested.
Conclusions:
Patients in the palliative phase who might be in need of HC have specific expectations. Perceptions of HC in the public domain should be nuanced in response to these expectations, and information provision on HC should be improved. Then, expectations could be met to make HC more driven by patient needs and future oriented.
Introduction
Hospice care (HC) has developed into various initiatives worldwide, 1 since the first hospice was founded in 1967. 2 Hospice care aims to optimize quality of life of patients in their last months of life and their families by minimizing suffering in the physical, psychological, social, and spiritual dimensions. 3 -6 Multidimensional suffering is complex, 7 as all dimensions are interrelated, described as the “total pain” experience. 7 A multiprofessional approach is required to address hospice patients’ needs. 8,9 In the Netherlands, the number of inpatient hospices increased from 86 in 2007 10 to 292 in 2014 and is divided into volunteer-driven hospices and professional-driven hospices (Figure 1). 6,11,12 Patients with life expectancies less than 3 months are predominantly admitted to hospice for last resort. 3,4,13 Although research in HC is scarce, 1,14 international studies showed that terminally ill patients want to stay in control of their life, care, and things related to loved ones. 15 -20 In the Netherlands, 68% of the population preferred to die at home and 27% in a hospice. 21 Nowadays, the realization of dying at the preferred place is an important quality indicator for “end-of-life care.” 22 Although we know how many people want to die in HC 21 and their reasons for dying there, 20 no insight into needs and visions of patients about HC is available. To make HC more driven by patients’ needs and thereby more future oriented, it is necessary to gain this insight. 4,20,23 Thus, the project “HOPEVOL: HC that is appropriate and is according to patients’ wishes in the palliative terminal phase of illness” was launched. 14 The aim is to ameliorate the quality of HC from the perspective of patients themselves. To the best of our knowledge, there are no studies describing expectations for HC from the perspective of patients in the palliative phase who might need HC in the future. Expectations are a major determinant for patient satisfaction in health care and are expressed as desires, wishes, and hopes. 24 Geurts et al provided a dynamic framework (Figure 2) consisting of 3 elements to evaluate expectations of patients, including structure, process, and outcome of care (SPO). 24 -26
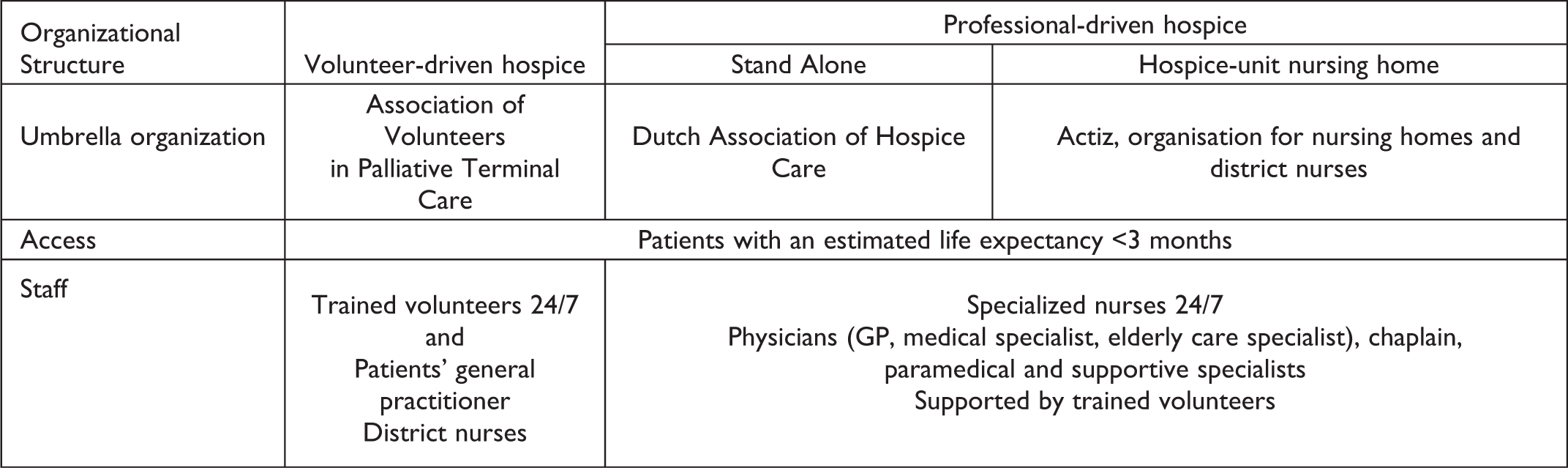
Palliative and hospice care in the Dutch health-care system. 3
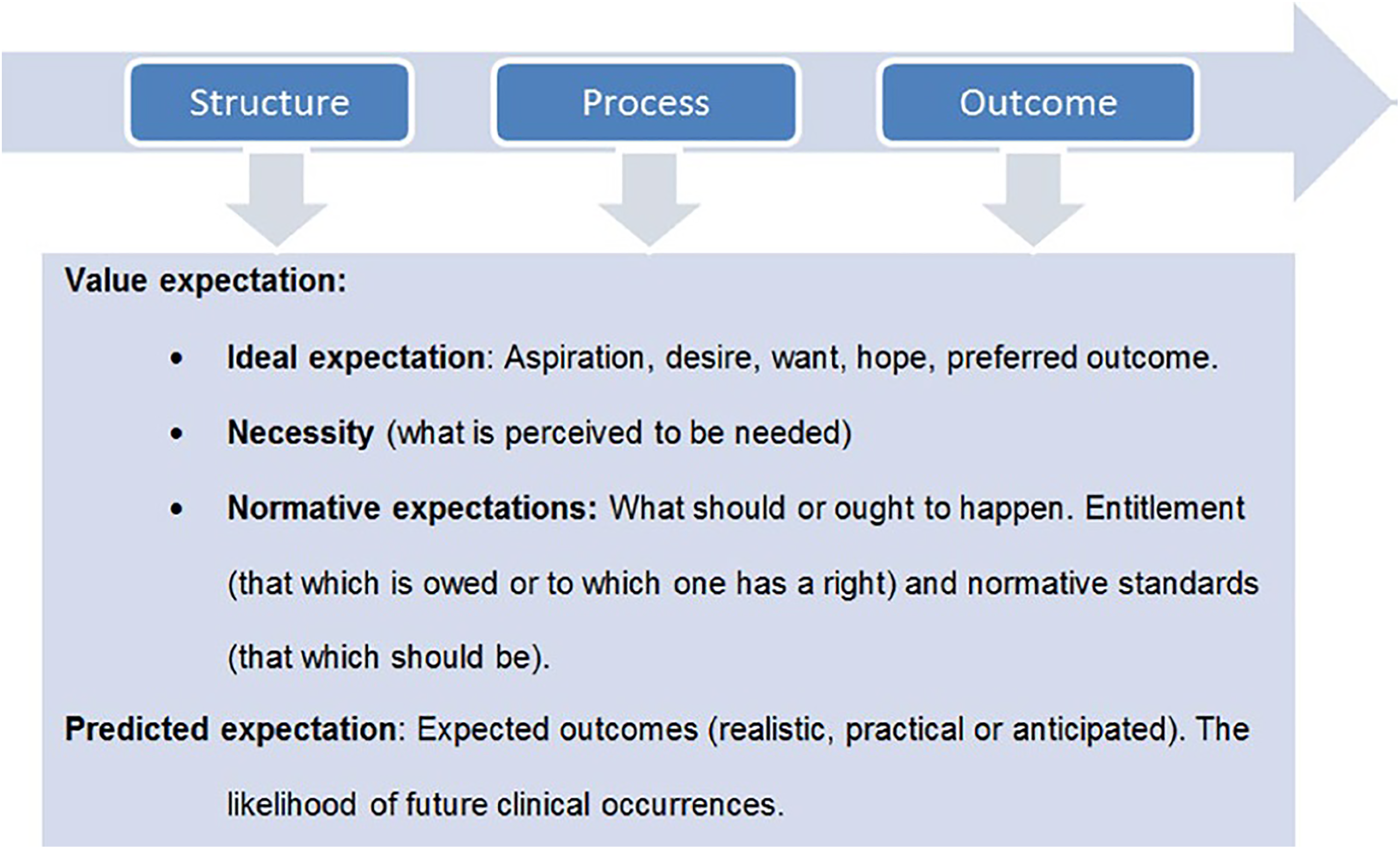
Structure, process, and outcome of care framework.
Expectations are divided into value expectations (ideals) and predicted expectations (more realistic expectations). 24 -26 Awareness of patients’ met and unmet expectations enables the understanding of patients’ perspectives 27 and thus contributes to demand-oriented care. In order to answer the research question “what are expectations of future hospice patients for HC in Dutch society,” this framework is used 24 .
Method
Design
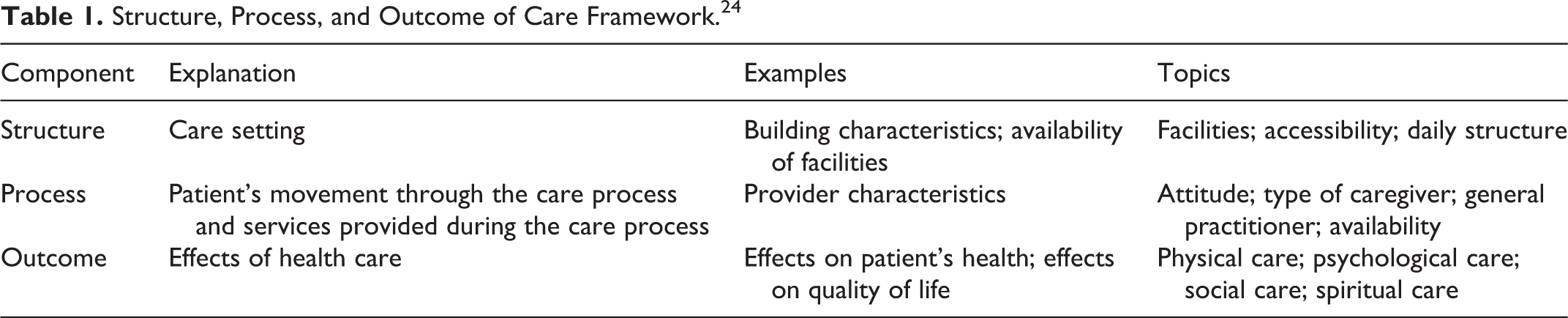
A generic qualitative exploratory design was used 28 to gain insight into expectations for HC of patients in the palliative phase who might be in need of HC in the future. 29 -31 Data were collected using semistructured interviews based on the SPO framework (Table 1) which were thematically analyzed. 28,32
Structure, Process, and Outcome of Care Framework. 24
Population
The population of interest was patients with a life-limiting illness, living at home in the Netherlands. The study population consisted of home-dwelling patients with an estimated life expectancy of less than 1 year. 5,33 Patients who received HC were excluded. To obtain a more abstract view on HC expectations, 2 patient representatives, trained to represent the patient perspective in quality and research projects in palliative care (PC), were recruited. 34
Data Collection
Semistructured interviews were conducted between March and June 2018. 31,35 A topic guide based on the SPO framework (Table 1) was used and tested in a pilot interview. 24,27,35 This topic guide was revised during the iterative process of data collection and analysis. 35,36 Each interview started with a general question, to ease participants, into talking more fluently. 35 Next, the researcher (R.B.) complemented the participants’ image with information about HC and proceeded with more specific questions, adapted to the participants’ circumstances and level of knowledge. Keynotes were used to record feelings and thoughts of the researcher (R.B.). 37 Different probing techniques such as remaining silent, echoing, and asking for elaboration were used to gain insight into expectations. 36 During the interviews, data were summarized, so participants were allowed to correct errors and check whether the interviewer understood the participants correctly, as a member check. 28 Interviews were audio-recorded and transcribed verbatim. Data collection continued until data saturation was reached. 36
Procedures
Eligible patients were identified and invited to participate in the study by general practitioners (GPs), waiting lists of hospices, and home care organizations. Additionally, patient representatives were recruited. 38 Participants were first identified and approached by their caregivers. After permission, eligible participants received information about the study by a researcher by phone and mail. When verbal consent was obtained, appointments were made at the participants’ preferred setting, mostly at their own home. Written informed consent was obtained before the interviews started. Interviews were performed by R.B., a case report form was completed to collect demographic data, and emotional support by a trained hospice nurse was offered.
Data Analysis
Collection and thematic data analysis followed an iterative process
28,39,40
carried out independently by 2 members of the research team (R.B. and Mv.K.): Interviews were transcribed by R.B. and transcripts were read and reread.
39
Initial codes were generated using NVivo11.
39,41
After every 3 interviews, R.B. and Mv.K. consulted each other. If no consensus was reached, a senior qualitative researcher within the research team (Ed.G.) was consulted. Codes were collected into potential concepts to give shape to the expectations. Concepts were reviewed by checking if they worked in relation to the coded extracts (level 1) and the entire data set (level 2). Themes were formed. Each theme was named and defined clearly. Final analysis took place, and the research question and literature were related to the themes.
39
To ensure that no thoughts of the researchers were lost and to reflect on patterns, memos were used. 31 Quotes to clarify the results were translated by the researchers (R.B. and Mv.K.) and checked by Ed.G. Peer feedback was provided by the research team to enhance the quality of the process and the results. 31 Researcher triangulation was used to ensure the validity and reliability of the data. 31,42
Ethical Considerations
This study was conducted according to the principles of the Declaration of Helsinki. 43 Prior to the commencement of data collection, the Medical Research Ethics Committee (reference-number 18-098/C) of the University Medical Centre of Utrecht (UMCU) reviewed the study to ensure that it fell outside the Medical Research Involving Human Subjects Act. 44 A quality check was performed within the UMCU, and the study was approved. All participants gave permission to their caregivers to be contacted by the research team, according to the Medical Treatment Contracts Act. 45 Participation was voluntary, and all participants were informed they could stop or refuse at any time. Informed consent was obtained before the interviews took place. 29,31 Patient confidentiality was ensured by anonymizing all data.
Results
Fifteen respondents were approached, but 2 patients died before the interview took place. Thirteen participants enrolled in the study, 7 men, aged from 34 to 93. One participant was from Surinam origin, and the other participants were Dutch. All demographic data are shown in Table 2. The median interview duration was 52 minutes (range: 24-84).
Demographic Characteristics.
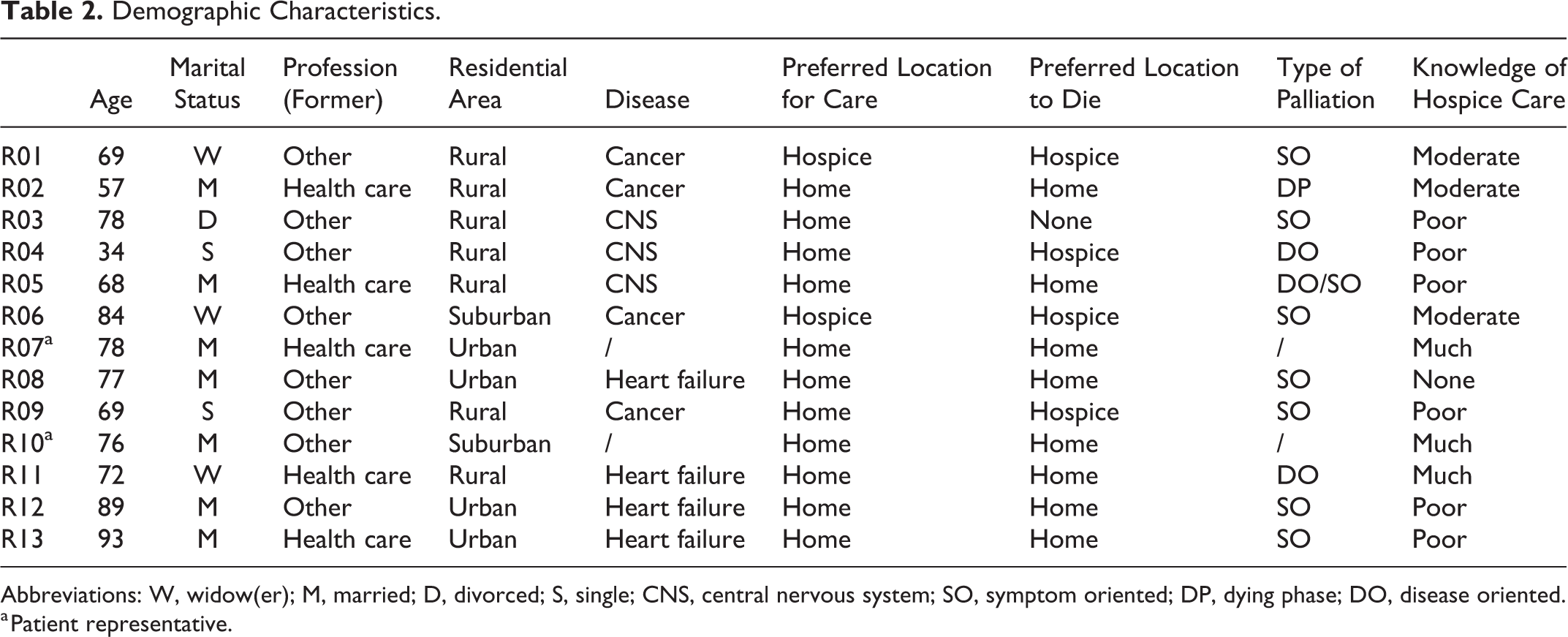
Abbreviations: W, widow(er); M, married; D, divorced; S, single; CNS, central nervous system; SO, symptom oriented; DP, dying phase; DO, disease oriented.
a Patient representative.
Perspectives on HC
Perspectives on HC was seen as an overall theme, not being included into the SPO framework.
25
Participants were not aware of the different reasons for hospice admittance and saw hospice as the “final destination,” a place to die. In my opinion a hospice is only intended for the final part. When you are lost, when there is no hope left. You are just waiting for death. I will not go to a hospice for fun, so I have to be too far gone to go there.
Results Regarding Structure, Process, and Outcome of Care.
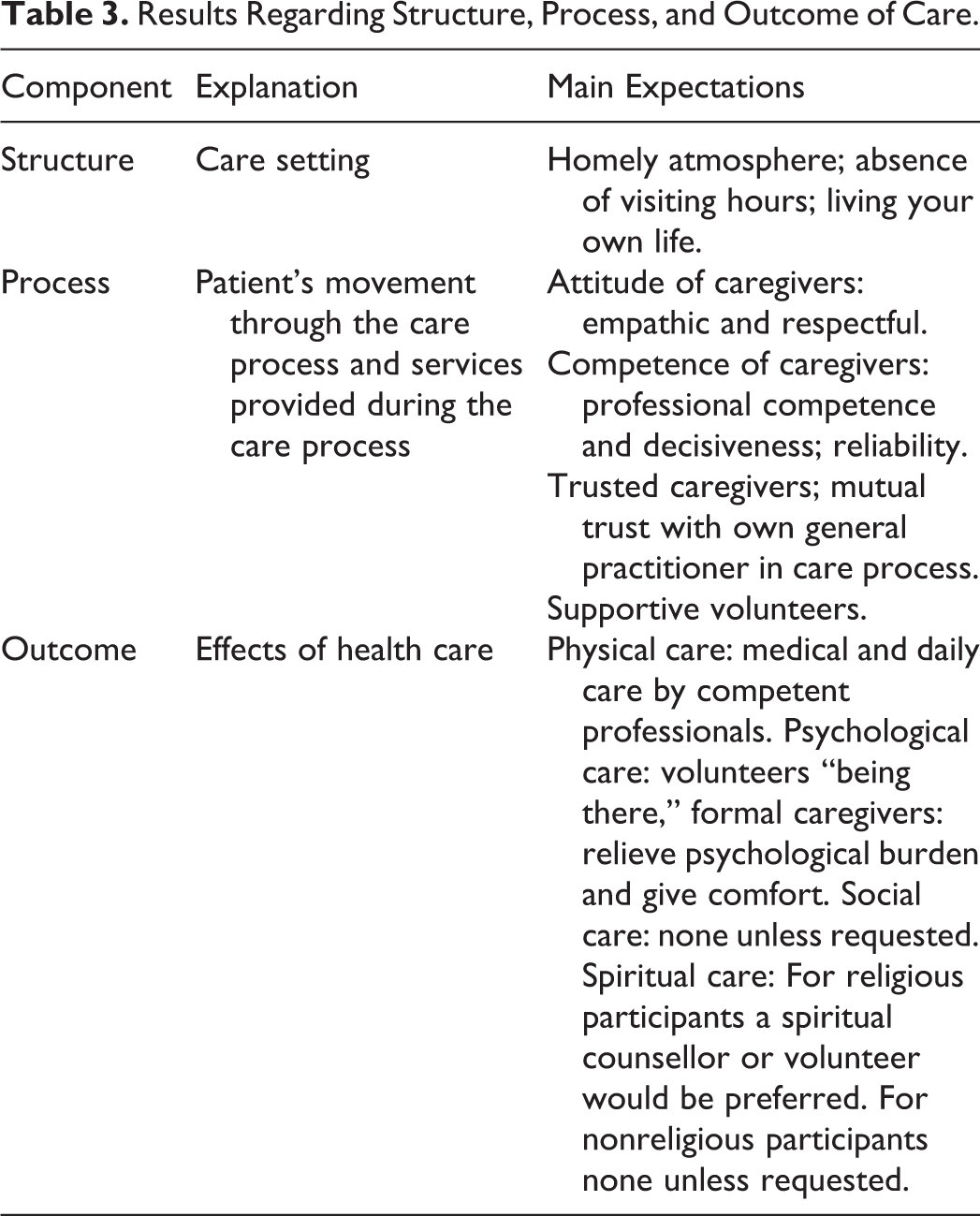
Structure of Care
Atmosphere
A homely, comforting, safe, and cozy atmosphere was perceived as an important necessity. And there you see very big differences between a hospital or a hospice that accompanies the final phase. There is, well, at least 500% difference between them…I think the hospital is very cold, very, cool. And you preferably need to leave as fast as you can, because they need a room. While a hospice is, yes, very different There is room for a picture and some small personal stuff you could put there, so you keep a piece of yourself with you. Yes, it sounds safe, it sounds good, let me put it like that.
Living your own life
All participants stated the importance of continuing the life they lived at home when admitted to hospice, with loved ones able to visit at any time. You should not have visiting hours. Visitors should come whenever they want…But, let me put it differently. Visitors, that is a different case. You should adjust to one another. My kids, they should walk right in, they should not make an appointment…Just like home actually. I would not want to share my despair and my emotions with others. I want to keep them for myself and for my loved ones. That is why a private room is very important to me. Yes, imagine when you are lying there, especially then it is very important to have dinner with your family, because it is the daily life we always lived, it should continue as long as possible. That in a reasonable way, that respect is shown for the life you lived before, which you really want to continue as much as possible until you die. To hear sounds, also from outside, to know that life, that life continues. You are facing death but it is good to hear life at the same time.
Process of Care
Attitude of caregivers
All participants expected that hospice caregivers have a calling to care for dying people. Caregivers are expected to be available at any time, providing appropriate care by discussing patients’ needs and wishes. Empathy and respect are viewed as driving attitudes. You will accompany people at the end of their life which won’t always be easy. So you will automatically have a sort of professionalism to ease those people as much as possible, it comes from within you, or else you would not work there. Well, that is the thing that appeals to me in a hospice.
Competences of caregivers
Professional competence, decisiveness, and reliability were qualities specifically attributed to professional caregivers. Additionally, volunteers were expected to be trained and complement professionals. I think the professionals will experience a time pressure, because it all depends on money. And the volunteers they got the time and they like it, it beautifully complements each other.
Trusted caregivers
Almost all participants expected their GP could still have a significant role in end-of-life care when admitted to hospice because of the highly appreciated mutual trust. He comes here every week. Sometimes twice a week. And then we talk about things…And because you have that bond with your general practitioner, that connection, that has to stay! A specialized physician knows more than a general practitioner. He could advise you, your husband, your children. A general practitioner could do this as well, but a specialized physician is better at it.
Outcome of Care
Physical care
Participants expected to experience physical symptoms and reduced ability of self-care and professionals are expected to provide medical care accordingly. Professionals are expected to respect and fulfill a patient’s end-of-life preferences; otherwise they would rather die somewhere else. Volunteers were perceived to provide supportive care. It depends, in my case, I am already disabled of course. So I would prefer a nurse providing care instead of a volunteer…If it considers medical care, and daily care like dressing up. A volunteer should comb your hair or polish your nails. I do not think a volunteer is educated to provide daily care like dressing up and that sort of care.
Psychological care
Most participants did not expect psychological complaints when admitted to hospice. They do expect conversations with professionals to relieve psychological burden and to comfort patients when feeling lost. Volunteers were expected to have a supporting role by providing a listening ear and “being there,” which is thought to be of inestimable value when in psychological need. Probably. I already have psychological complaints. Not that I am unstable, I do not think so, but. It is very pleasant to pour out your heart.…(I: And if you would want support with psychological complaints, what kind of caregiver would you expect?) A listening ear.
Social care
Over half of the participants stated social care to be a private matter with their loved ones, where volunteers and professionals should not interfere unless requested. Some participants did not expect social care needs. However, participants who did expect social care pointed out that volunteers could provide practical help on request. I think it has to come from within oneself. Look, when I have a relationship with you. Emotionally another person cannot help me with that, nor help you to say goodbye to each other. I think it has to come from within oneself. Well looking at the funeral, if my daughter needs help, she knows everything, but you never know. That they accompany her, yes, take care of her. I think that is important. (I: That they will take care of your children?) (Patient is emotional while looking at a picture of her family.) Especially my grandchildren.
Spiritual care
Talking about life and death is perceived to be comfortable by almost all participants. All religious participants preferred a spiritual worker or religious volunteer to provide spiritual care. All nonreligious participants stated that spiritual care is a private occasion provided only by loved ones unless it is otherwise requested. But, what you do have with fellow believers, with them you could talk easier at the moment you are in mental need, than when it is not the case. Because then there is a sort of a blockage.
Discussion
This study aimed to explore expectations of HC by patients in the palliative phase who might need HC in the future in order to further develop future proof HC in the Netherlands. Patients with a life-limiting disease and their representatives expected admittance in a hospice only when dying at home becomes unbearable. For all components of the SPO framework, 24 only value expectations were found. Reasons for this could be the lack of experience of the participants with HC or that participants have specific expectations of caregivers working in HC. Regarding “structure of care,” participants expected a place with a homely atmosphere where you can continue the life you lived, together with your family. In “process of care,” participants expected empathic and professional caregivers, able to provide appropriate care. Also, having their personal GP involved in the care process is expected to be advantageous because of the mutual trust. In “outcome of care,” medical and daily care are expected to be provided by professionals, with volunteers providing supportive care. All caregivers are expected to provide a listening ear and “being there” for patients. Social and spiritual care are mainly expected to be private matters.
Existing literature shows the importance of experiencing a homely feeling in the palliative phase. 18,21 Our study found that patients with a life-limiting disease expected hospices to have homely and comforting atmospheres, where you can feel safe. Furthermore, the continuation of daily life is very important 20,46,47 for terminally ill patients, 20 older patients, 46 and patients with cancer receiving PC. 48 Freedom, privacy, and the absence of visiting hours are seen as important components in this matter. 20 It appears that patients expect to be able to continue daily life and to stay in control. Consistent with literature, 20 patients do not expect visiting hours and valued privacy and freedom for themselves and their families. Respect for patients’ privacy is also a part of the mission and vision statements of hospices in the Netherlands. 4 Caregivers’ attitude in the palliative phase is essential for patients receiving PC and is expected to be personal. 49 Expectations of patients in this study can be seen as very similar, although they add that they also expected their caregivers to be empathic and competent. Moreover, patients explicitly want their own GP to stay involved, due to the mutual trust. In another study, hospice staff members also confirmed that PC patients saw the loss of their own health-care provider as a major concern. 47 In a study with oncology outpatients, there were 3 important perceived benefits of HC: good pain management, the availability of medical care, and having medical staff on call. 50 This study endorses these findings. Patients expect medical care to would always be available, delivered by medical staff. This medical care is expected to be good, without exception. Next to the medical care, patients expect that all caregivers would have conversations with them, but especially volunteers should provide a listening ear and to “be there.” This is also defined as the essence of a volunteer’s task, according to the literature. 51 The national Quality Framework Palliative Care (2017) 51 sets standards for PC in general, the importance to mark the palliative phase on time, so that proactive care planning can be provided to minimize suffering in this framework. 52 The definition of PC also declares the importance of an early identification of multidimensional problems. 51 The expectation of going to a hospice only when it becomes unbearable at home gives some friction because, when admitted to HC, all admissions would be in times of crisis. Meaning, it would be too late to provide the desired temporary admission and/or proactive care. It is therefore important to nuance the perceptions in the public domain in response to the results of this study and to give respite care and temporary admissions more publicity. Also, health-care professionals should be aware of these options and refer patients to HC timely.
It is important to make a distinction between value and predicted expectations (Figure 1), especially in clinical practice. 24 Most participants had very specific expectations of HC and provided value expectations, and no predictive expectations were found. In order to supplement the found value expectations with predictive expectations, an interview study should be performed with the patient admitted to HC. Also, HC in the Netherlands is inpatient care. Probable future patients are unfamiliar with the possibilities of HC being provided in their home. Therefore, information provision to care providers in primary and secondary care should be improved so that patients’ understanding of HC can be enhanced, and all expectations can be met.
Most previous research in HC is performed with older adult patients, relatives, or caregivers instead of patients in the palliative phase. Dying patients appreciate to participate in research, believing their contribution to be important, especially when it could help others. 45 The participants in this study cover a large distribution of characteristics, providing maximum variation in phases of palliation, diseases, and experiences with HC which is an important strength of this study. A broad insight into expectations is therefore shown, 41 complemented with the more abstract view of patient representatives. 34 We cannot assume that the emerged themes of this study would have arisen with a sample in another country because of worldwide differences in HC. Since data saturation was reached, we believe that many themes will also emerge with another sample in the Netherlands. The use of researcher triangulation, 31,42 member checks, 28 and memos during the entire process of data collection and analysis 31 strengthens this research. However, the study was limited because of the patients’ vulnerability, inclusion of participants for this study was difficult, resulting in a convenience sample, whereas the aim was a purposeful sample. The inclusion of younger participants could have contributed to the current results.
Conclusion
The general expectation of future hospice patients is that they prefer to die at home but that when staying at home becomes unbearable admission to a hospice is only expected in the dying phase. In case of admission, patients expect appropriate care, in line with the current standards and evidence. They have high expectations of HC concerning SPO. This creates tension in patient referral and possibly a stigma for HC. This might cause a delay in accepting HC, thereby resulting in suboptimal care delivery. The image of HC in the public domain should be more nuanced as a reaction to these expectations. Further research is needed on patients admitted to hospice and their families in order to see if their expectations are met. However, perceptions about HC in the public domain should be nuanced when responding to these expectations, and the information provision about HC should be improved. Then, future-oriented expectations could be met, and HC could be more fully driven by patients’ needs.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research was funded by ZonMw, projectnumber 844001406