
Abstract
Background:
Palliative care is essential to quality of life for people with life-limiting illness and can strengthen health-system performance. In Greece, however, services remain fragmented—especially in emergency departments (EDs), which serve as safety nets yet lack structured training, pathways, and tools for end-of-life care. We propose the Hellenic Emergency Palliative Care Project (HelP CaPe): a pragmatic, government-sponsored, multicomponent intervention to integrate palliative care into two high-volume EDs (Nikaia General Hospital, Athens; Larissa General Hospital).
Methods:
HelP CaPe includes (1) culturally adapted education for emergency clinicians using the Education in Palliative and End-of-Life Care-Emergency Medicine curriculum; (2) ED-based palliative care hubs that deliver symptom relief, minor procedures, goals-of-care conversations, and family support; and (3) formal linkages to home- and community-based services to improve continuity. Design and implementation draw on comparable resource-constrained models, including Hospice Ethiopia, and align with Greek preferences for home-based care. Evaluation will track patient experience and utilization (avoidable admissions and repeat ED visits), clinical processes (analgesia and minor procedures), and clinician outcomes (satisfaction and burnout).
Conclusion:
Leveraging existing emergency medicine infrastructure, HelP CaPe addresses key gaps—limited training and absence of structured pathways—while building capacity for sustainable service delivery. The initiative aims to reduce unnecessary ED demand, enhance goal-concordant care, and relieve pressure on EDs, with potential wellness benefits for clinicians through diversified practice. If successful, HelP CaPe will offer a scalable model for integrating palliative care within EDs in Greece and other health systems facing similar constraints.
Background
Palliative care improves quality of life for people with serious illness and strengthens health systems, yet services in Greece—especially within emergency departments (EDs)—remain underdeveloped.1–5 Greek EDs function as safety nets and frequently become the default destination for patients with advanced disease, but clinicians lack structured training, tools, and pathways to address palliative needs. 6
Greece’s palliative services are historically fragmented and underfunded. Provision is limited, poorly integrated within the health care system, and often Non-Governmental Oraganization-led. 7 Palliative care is not consistently embedded in medical education, and discontinuity in outpatient services drives patients to often overcrowded, understaffed EDs during crises. Concurrently, ED overcrowding and rotating on-call patterns compound delays and variability in care for the seriously ill.8–11 These factors collectively justify the classification of Greece as an underserved setting for both emergency and palliative care and highlight the urgent need for practical, scalable interventions. Without emergency palliative care training, the acute, procedure-focused nature of emergency care may clash with the longitudinal, goal-aligned needs of patients nearing end of life. However, integrating palliative care into routine ED workflows may optimize care, minimize suffering, and offer health system benefits. 12
Evidence on ED-based palliative care is promising but uneven: studies suggest benefits in communication, symptom control, and length of stay, yet outcome measures are inconsistent, and most interventions do not build durable ED capacity in primary palliative care. In the United States, there have been mixed results with palliative care integration into Emergency Medicine: a recent trial in JAMA failed to show an impact. 13 Earlier studies demonstrated that interventions such as palliative care consultations in the ED can improve communication around goals of care, reduce symptom burden, and shorten hospital stays.14–17 Reviews of models targeting cancer patients in oncologic ED settings similarly show potential benefits in aligning care with patient preferences and reducing resource utilization. 18
However, the literature also reveals several persistent gaps. First, most existing programs are located in high-income countries, with strong infrastructure and established specialty palliative care teams; there is very limited published evidence from settings where EDs are resource constrained or where palliative care is not yet well integrated. Second, there is inconsistency in which outcomes are measured—some focus on hospital length of stay, others on ED revisits, quality of life, clinician experience, or cost—but seldom all together. Third, few models include capacity building (training ED staff in primary palliative care) rather than relying solely on specialist palliative care consults.
Against this backdrop, we propose an intervention called the Hellenic Emergency Palliative Care Project (HelP CaPe), which will (1) create ED-based palliative care hubs in two locations in Greece, paired with (2) culturally adapted Education in Palliative and End-of-Life Care-Emergency Medicine (EPEC-EM) training, and (3) formal linkages to home and community services, as a pragmatic, scalable model. Our proposed intervention has the potential to transform palliative care delivery in these two locations by offering patients timely access to palliative care while alleviating pressure on overcrowded EDs and busy ED physicians and other clinicians. More importantly, it paves the way for a sustainable model that helps to prioritize dignity, comfort, and compassion for patients with incurable disease. Please see Table 1, which summarizes the value proposition of integrating palliative care into emergency medicine and specifically how this intervention addresses both patient needs and health system pressures while improving clinical care and cultural alignment.
The HelP CaPe Value Proposition
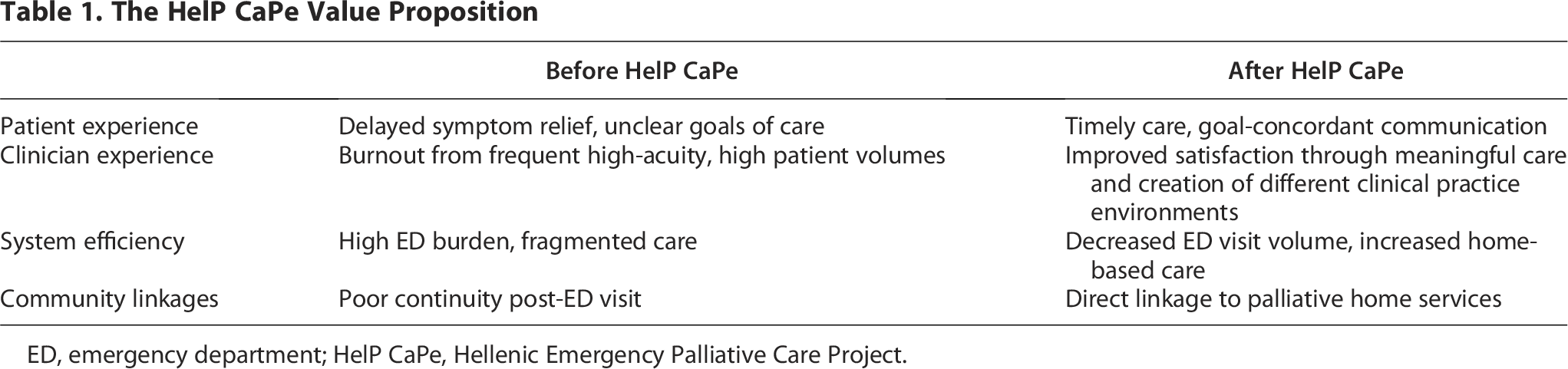
ED, emergency department; HelP CaPe, Hellenic Emergency Palliative Care Project.
In summary, HelP CaPe is a novel, sustainable, and scalable emergency palliative care intervention. It will also provide a necessary extension of the ED-based palliative care literature by expanding into new geographic and resource settings, integrating multiple components (education, hubs, referral linkages), and systematically addressing both patient- and system-level outcomes. HelP CaPe has the promise to fill important evidence gaps and help shift practice globally toward more responsive, context-adapted ED palliative care.
Intervention
The HelP CaPe intervention takes a pragmatic approach to addressing the unmet palliative care needs in Greek EDs by leveraging the existing infrastructure of EDs, which in Greece are not open every day but rather on a rotating schedule, such as one day in two or four, leaving days when the ED is closed to emergency patients but will be open to palliative care patients with emergency needs. The intervention is funded by the Prefecture of Larissa, Greece. The underlying conceptual framework integrates CFIR, Reach, Effectiveness, Adoption, Implementation, and Maintenance (RE-AIM), and COM-B into a theory of change for ED-based palliative care integration in Greece (Fig. 1).19–21 The intervention bundle has three components: (1) train clinicians with EPEC-EM (culturally adapted for this setting); (2) create palliative care hubs in two Greek EDs during off days; and (3) provide formal linkages to community-based palliative care. We hypothesize that HelP CaPe will improve patient reported outcomes and clinician well-being while reducing ED visits and avoidable admissions, thus adding value to the health system (Fig. 1).
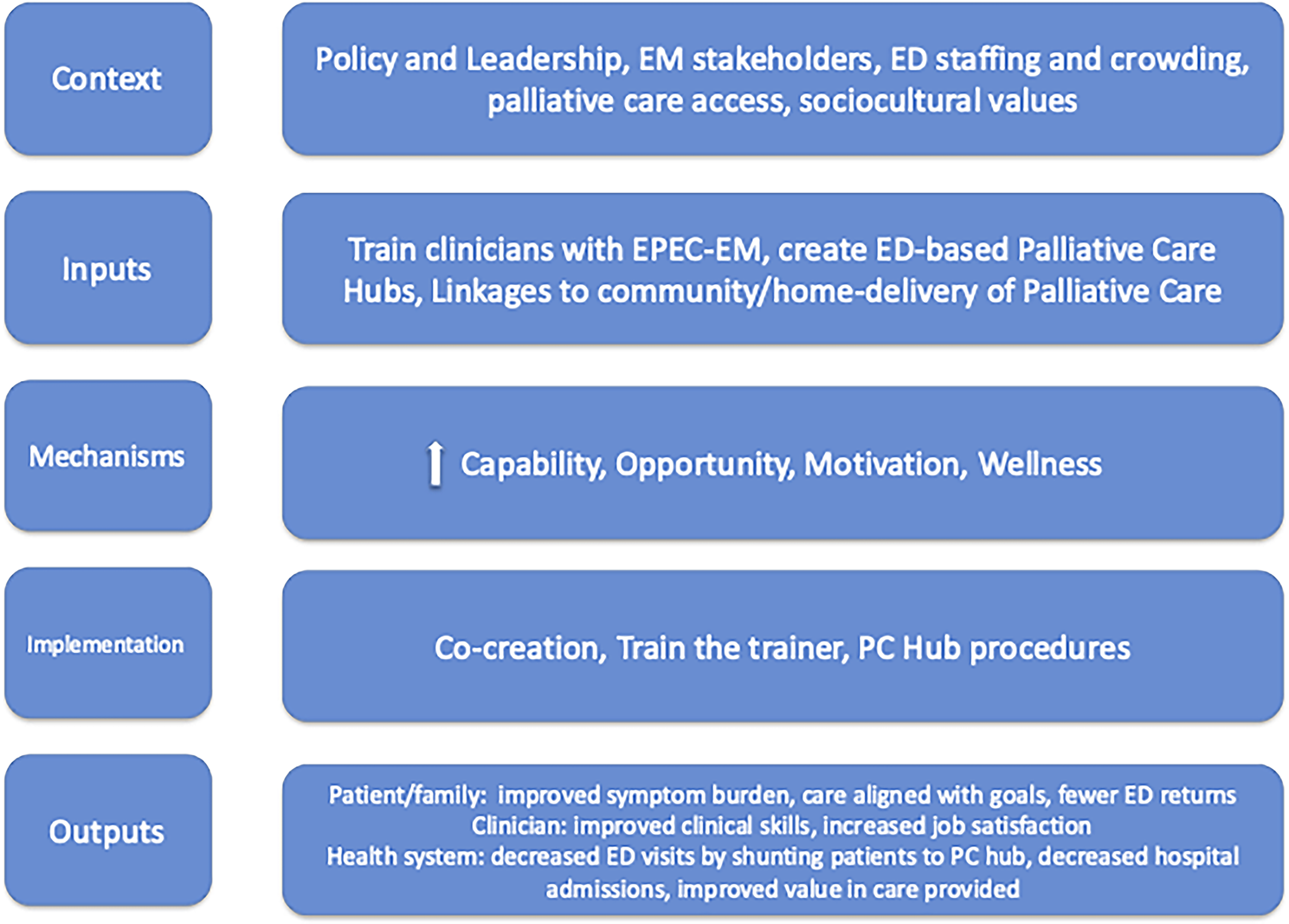
HelP CaPe conceptual framework. HelP CaPe, Hellenic Emergency Palliative Care Project.
Train clinicians with EPEC-EM
HelP CaPe will equip a cadre of emergency physicians with palliative care skills through the EPEC-EM, which is a training program in primary palliative care, focusing on basic palliative care skills in symptom management and medical decision making.22,23
It has been adapted for the Greek setting both linguistically and culturally with the input of a multidisciplinary team. While EPEC-EM Greece training will be taught in English as a common intermediary language, content will be taught at a 3-day workshop in Larissa, Greece, via cross-cultural dyads, which include one EPEC-EM trained, U.S.-based faculty member and one Greek clinician or allied health professional. The workshop is planned for April 2026.
Create ED-Based palliative care hubs
Palliative care hubs will be created in Nikaia and Larisa EDs, staffed by emergency physicians and nurses, with consultation from social workers and chaplains as needed. All public hospital EDs in Greece operate on a rotational schedule: some are open one day out of four, others one day out of two, while smaller EDs (e.g., in the Greek Aegean Islands) are open daily. Both Nikaia and Larissa General Hospital are public hospitals in Greece: Nikaia
General Hospital ED is located in the greater Athens area and is one of the largest and busiest EDs in Greece. Nikaia operates every one in four days and sees a volume of approximately 1100 patients in 24 hours while on call. Larissa General Hospital ED serves a city of approximately 160,000 people. The ED is open one day out of two and treats approximately 320 patients in the 24 hours it is on call. Both EDs suffer from overcrowding and staff burnout.7,24
Palliative care hubs will offer specialized interventions for patients with palliative care needs during ED off-days. These interventions include recognizing and treating pain and other unpleasant symptoms; providing medical advice for caregivers who perform the majority of in-home care due to the lack of in-home palliative care infrastructure; goals of care conversations; interventions (such as thoracentesis, paracentesis, foley catheter placement, and intravenous fluid hydration); coordination of the use of other hospital resources as needed; and referral to community-based resources.
Linkages to Home-Based palliative care
In Greece, formal home-based palliative care services—beyond what families can deliver—remain a major gap in the Greek health care system. In the Athens area, Galilee Palliative Care Center is the main provider of comprehensive home-based palliative care. 25 Outside of Athens, access is far more limited and fragmented. In Larissa, for example, informal care networks exist through local churches and a small cancer patient support organization, but structured services are lacking. As a result, responsibilities for symptom management, hygiene, and feeding at the end of life often fall entirely on families, who function as the backbone of outpatient palliative care.
To address this, the Larissa pilot will emphasize training and supporting family caregivers during visits to the palliative care hub. In Nikaia, we will establish referral pathways to existing home-based services like Galilee. At both sites, we plan to pilot home visits by palliatively trained emergency nurses, supervised by a physician palliative care champion. This will constitute Phase IV of our project, described in detail in the following section.
Implementation
Our implementation plan comprises six phases, taking place over two years. At the time of the writing of this article, we are finishing phase 1. The implementation plan is summarized in Table 2.
Summary of Implementation Plan by Phase
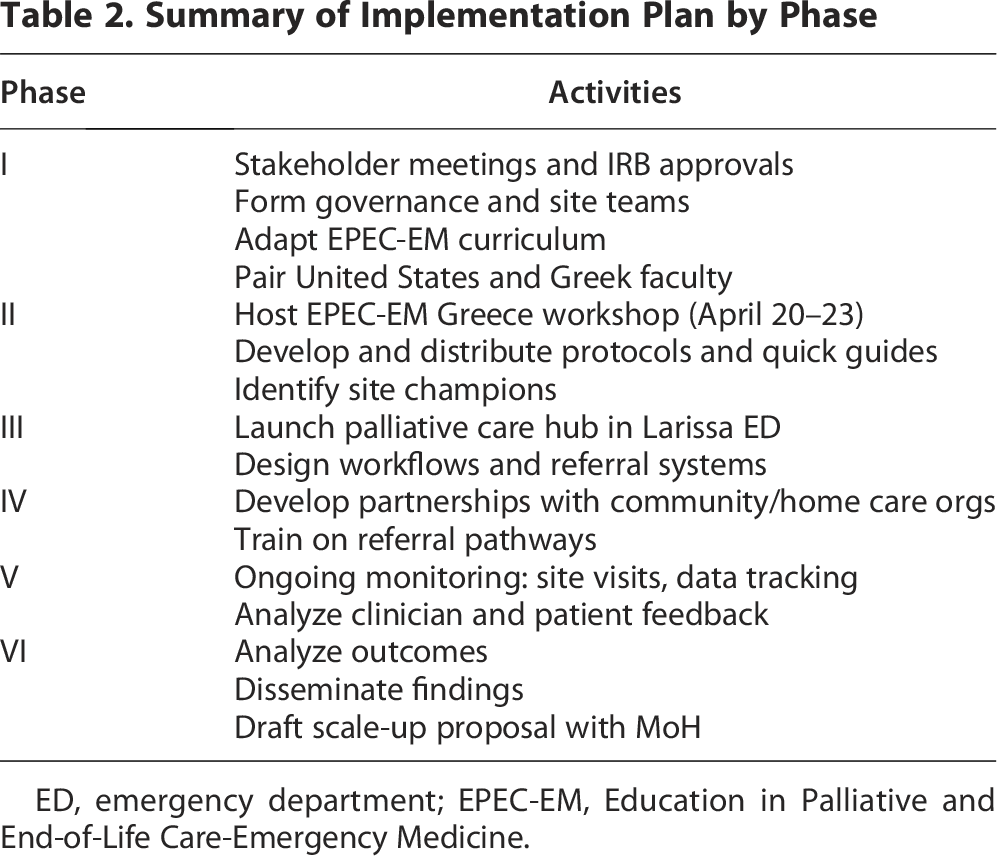
ED, emergency department; EPEC-EM, Education in Palliative and End-of-Life Care-Emergency Medicine.
Phase 1 is centered on Planning and Stakeholder Engagement (months 0–4). The seven objectives of this phase are (1) to secure institutional approvals and align with hospital leadership at Nikaia and Larissa General Hospitals (2) establish project governance, working groups, and define roles (3) finalize the implementation timeline and key performance indicators. The key activities of this phase are for stakeholders to travel to Ethiopia to participate in an EPEC workshop and shadow during home hospice visits with Hospice Ethiopia; conduct stakeholder meetings (stakeholders include ED leadership on both sides, palliative care, nursing, social work, and MoH reps); form a bi-institutional project steering committee and local site leads; adapt the EPEC-EM curriculum for Greek context (language, case examples, and cultural alignment); create the teaching program by hour for the 3-day workshop; identify and confirm Greek and United States faculty dyads for teaching the EPEC-EM Greece workshop; and forward and back translate the SPICT tool into Greek.
Phase 2 is focused on clinician training and capacity building (months 4–8). Our objectives in this phase are to emergency physicians and nurses with primary palliative care skills through EPEC-EM Greece and build interdisciplinary awareness and collaboration across these front-line health care teams. Our key activities in Phase 2 are to host a 3-day EPEC-EM training workshop in Larissa (April 20–23, 2026) for 40 emergency physicians, nurses, and social workers, which is sponsored by the Larissa government, introduce the SPICT tool and train users on use, develop and distribute quick-reference guides for symptom management and communication and identify internal champions within the ED teams at both Nikaia and Larissa hospitals.
In Phase 3, we will launch the ED-based Palliative Care hub in Larissa, Greece (months 8–12).
Objectives include operationalizing palliative care delivery during ED off-call days via a palliative care hub staffed by emergency physicians, nurses, and social workers in the Larissa General Hospital Emergency Department. Patients will be identified at triage by a study doctor using the SPICT tool. Stable patients with nonlife-threatening conditions who screen in will be referred to the palliative care hub for treatment. Unstable patients or those with potentially life-threatening conditions will be triaged to the main ED. Once stabilized, ED clinicians will be able to refer the patient to the hub if that is appropriate. The hub will provide emergency palliative care services, including symptom management, minor procedures (e.g., paracentesis, thoracentesis, foley catheter placement, IVF rehydration), and family support. During this phase, our key activities also include optimizing workflows and referral pathways to the palliative care hub from the ED. In this phase, we will plan to have the hub open 2 days per week.
Phase 4 is centered on community integration and continuity planning (months 6–12). In this phase, our objectives are to strengthen referral systems from the ED to home-based palliative services currently delivered through several local nonprofit organizations while investigating strategies to increase home-based delivery of palliative care in this setting, possibly through liaising with palliative care hub staff. The important activities in this phase include identifying and partnering with existing nonprofit organizations delivering home-based palliative care and training ED staff on criteria for referral to these community partners as well as primary care networks to ensure appropriate follow-up.
In Phase 5, we will focus on monitoring, evaluation, and analyzing collected data (ongoing from months 8–24). During this critically important phase, we will evaluate the outcomes of our pilot and refine the intervention as dictated by these results. This in turn will inform sustainability and scalability planning for Phase 6 (expand project to Nikaia General Hospital Emergency Department). The key indicators in this evaluation include number of clinicians trained, number of patients seen by palliative care hub, nonhub ED revisit rates for palliative patients, clinician satisfaction and burnout metrics (pre–post survey) and patient and family satisfaction (qualitative interviews). The key activities in this phase include monthly site implementation check-ins, quarterly data review and feedback sessions, and an end-of-Larissa-pilot evaluation and stakeholder debrief at month 16.
Finally, in Phase 6 we are focused on scale-up planning and dissemination (months 12–24). In this final phase, our objectives are to identify key lessons learned at Larissa to adjust the model for rollout to Nikaia Hospital Emergency Department in Athens, Greece. We will also be actively advocating for policy and funding support for wider dissemination. Our activities will include publishing the Larissa pilot results and lessons learned in a peer-reviewed journal, hosting a dissemination webinar, and presenting our results at a European Emergency Medicine conference (European Society of Emergency Medicine as well as the Greek National Conference for Emergency Medicine). We will also prepare a written scale-up proposal for other Greek hospitals and regional networks, to be delivered to the Greek Ministry of Health.
Evaluation
We will assess the impact, feasibility, and sustainability of the HelP CaPe pilot using the RE-AIM framework. 20 This mixed-methods evaluation integrates quantitative metrics and qualitative data from patients, families, clinicians, and hospital leadership.
Reach
We will measure how effectively HelP CaPe reaches seriously ill, palliative-eligible patients in the ED. Outcomes include the proportion of eligible patients identified and seen by the palliative care hub; the number and characteristics of patients and families receiving goals-of-care discussions or symptom-focused interventions; and referrals to home- and community-based services. We will administer post-visit surveys to all hub patients/families and conduct targeted in-depth interviews to assess the patient and families experience in the palliative care hub, including symptom relief and goal-concordant care.
Effectiveness
Effectiveness will be evaluated at three levels:
Adoption
Adoption will reflect uptake by clinicians and sites. Measures will include number and proportion of physicians, nurses, and social workers completing the EPEC-EM Greece training; pre/post changes in clinician knowledge and confidence; use of the ED-based palliative care hub; and visible leadership endorsement.
Implementation
Implementation will focus on reliability in real-world Greek ED conditions. We will track hub use by patient volumes, documented goals-of-care discussions, referrals to community-based services, and completion of post-visit surveys. We will conduct interviews and focus groups with clinicians, administrators, community palliative partners, and family members to identify successes and barriers (staffing, space, cultural expectations) and adaptations.
Maintenance
Maintenance will assess durability at 9–12 months. We will evaluate continued function of the palliative care hub; patient volumes seen in the hub, referrals to home- and community-based services; and the presence of additional EPEC-EM training sessions. Results will inform a presentation at the Greek National Emergency Medicine conference (2027), presentation at an international conference, open-access publication in an international journal, a final report to the Ministry of Health, and policy brief to guide scale-up across additional Greek hospitals.
Discussion
While the idea of integrating palliative care hubs into the ED is promising, there are several barriers to consider. First, the lack of specialized training in palliative care among many Greek health care providers must be addressed. As a training program in primary palliative care, the EPEC-EM curriculum provides a robust training framework to prepare emergency physicians and other clinicians to provide palliative care. Training ED staff in the fundamentals of palliative care would be a cornerstone of this initiative, ensuring that clinicians can provide the appropriate level of care to their patients, whether they are staffing the ED or the palliative care hub.
There are a number of ethical and equity aspects of care to consider in this pilot project to ensure that no patient populations are inadvertently excluded. The Greek health care system adheres to the basic principles of socialized medicine, providing full free medical coverage for anyone who needs it. By definition and in clinical practice, no population is excluded from health care. Palliative patients are identified as those presenting to the Emergency Department with poorly managed symptoms in the setting of life-limiting illness, as identified by the SPICT tool. All patients receiving palliative care either in the ED, the PC hubs, or at home will be under the umbrella of the National Health System regulations and National Ethics regulations. In addition, patient/family support groups provide an integral and extra layer of wraparound protection of patients’ rights.
Because families remain at the heart of symptom management and home-based palliative care, individuals without a strong family unit may be more likely to present to the hospital. Another complicating factor is one’s ability to communicate pain, as nonverbal patients or those with dementia represent populations especially vulnerable to poor symptom management. HelP CaPe represents an attempt to standardize palliative training for medical professionals in the care of all palliative patients, regardless of their diagnosis, age, gender, or family status.
Securing sustainable funding is essential for the continued operation of these palliative care hubs and their associated staffing needs. The pilot is currently supported by the Ministry of Health of the Prefecture of Larissa, reflecting a strong governmental commitment to enhancing the quality of care across all stages of illness. While Greece’s national health care system faces significant budget constraints, this investment holds the potential for meaningful long-term savings by reducing avoidable hospital admissions and high-cost interventions for terminally ill patients. Demonstrating improved patient outcomes, shorter hospital stays, and lower overall health care expenditures through this pilot could lay the foundation for broader systemic reform and national scale-up.
If successful, this pilot project could not only improve the care of patients with incurable disease in two Greek EDs but also create a replicable model that can be expanded to other hospitals across the country. It would mark a significant shift toward more compassionate, patient-centered care that recognizes the needs of individuals in the final stages of life. Furthermore, it would offer an opportunity to educate health care professionals and the public about the importance of palliative care and its role in enhancing the quality of life, rather than simply extending it. In the end, the need for palliative care in Greece is clear. By embedding palliative care within emergency medicine and expanding home-based care, Greece can prioritize dignity, compassion, and quality of life for its most vulnerable patients while adding value to its health system.
Authors’ Contributions
D.B., E.R., and D.T. wrote the main article text. J.H., E.A., A.U., and J.R.L. provided important edits. All authors reviewed the article.
Footnotes
Author Disclosure Statement
All authors decline conflict of interests.
Funding Information
This project is funded by the Prefecture of Larissa Government, in Larissa, Greece.
Consent for Publication
All authors consent to publication of this article.