
Abstract
Background:
Emergency department (ED) presentations are common for people in their last year of life, but the characteristics of these presentations by regional patients known to palliative care services are limited.
Objectives:
To identify the characteristics and communication that occur when community-based palliative care (CBPC) patients present to the ED.
Design:
A retrospective, cross-sectional study of CBPC presentations to the ED over 12 months.
Setting:
Eligible participants were all regional CBPC patients who attended the index Australian ED between June 1, 2022, and May 31, 2023.
Measurements:
Data acquired included demographics, presentation details, documented communication, and ED discharge information.
Results:
An overall 235 CBPC patients presented to the index ED at least once (427 presentations), constituting 1.23% of all adult ED presentations. The median age was 75 years (interquartile range 65–82), and 82.6% had a primary diagnosis of cancer. The most common ED discharge diagnoses were symptom-related (78/427, 18.3%) and respiratory disease (77/427, 18%). Most (300/427, 70.3%) were admitted. Communication between ED and palliative care services was documented in 18.9% of presentations (81/427). Communication was more likely in patients who were admitted (88.9% vs. 11.1%), in work hours (55.6% vs. 44.4%), or in those with a cancer diagnosis (93.8% vs. 6.2%).
Conclusion:
CBPC patients presented to the ED with a high admission rate, which may indicate appropriate ED presentations. Coordinated care through communication was evident in only a minority of cases. Further studies to explore the complex palliative care needs of patients presenting to the ED and barriers to integrated care between services are vital to providing optimal care.
Key Message
This study describes a high ED presentation and hospital admission rate of known palliative care patients. The main ED diagnoses were symptom-related and respiratory diseases. Documented communication between ED and palliative care services to provide integrated care was limited.
Introduction
Emergency department (ED) presentations by patients with palliative care needs are perceived as avoidable; their use can also be meaningful to their care.1–3 Australian studies show that 80% of people presented at least once in their last year of life and that 12% of presentations for patients over 45 years were due to a life-limiting illness.4,5
There are limited data on patients presenting to the ED with palliative care needs or who are known to palliative care services. Studies of predominantly cancer patients showed the main ED presentations are symptoms related to gastrointestinal problems, lung problems, and pain.6,7 A United Kingdom study of known palliative care patients showed 75.1% were admitted following presentation to ED in comparison with the general population at 24.5%. 8
Factors precipitating an ED presentation are more complex than the admission diagnosis. Cancer patients try to avoid the ED due to the busy setting and anxiety related to waiting for care.9,10 Studies show patients or carers being overwhelmed, both with the change and complexity of care, and having insufficient resources to cope at home.1,11,12 System fragmentation, inadequate control of symptoms, and inability to access urgent review in the community or direct admission to the ward are also factors adding to ED presentations.13–16
Community-based palliative care (CBPC) strives to provide holistic care to people and families in their homes. Services aim to maintain “care in place,” reducing ED presentations and unplanned hospital, admissions, plus integrating palliative care with local health care systems.17–22 The Australian Palliative Care Standards outline high-quality specialist palliative care provision, including effective communication and integrated care. 23 There are little data on the integration and communication between ED and CBPC. Lane et al. showed that hospital staff highly valued communication between clinicians regarding palliative care patients yet were often hindered by other time demands. 24
To increase what is known about this cohort, our study describes the ED presentations and nature of interdisciplinary communication for active CBPC patients presenting to a regional ED. We evaluate the utilization of ED services by patients in our community palliative care service, within the study period, to describe and quantify demographic and clinical characteristics. This study aims to identify this cohort’s most common ED diagnoses and discharge destinations, evaluating frequency plus mode and patterns of communication. The hypothesis is that ED presentations will be common, but documented communication to support integrated care between services may be lacking.
Methodology
This is a retrospective, single-center, cross-sectional study conducted in a regional Australian hospital.
Study setting
This study was undertaken at Bunbury Regional Hospital (BRH), a 193-bed public facility with a 29-bed specialist-led ED, located in a Modified Monash Model (MMM) 2 regional center.25,26 It is the largest of 13 hospitals in the Southwest health region of 23,000 km2 serving a population of 177,000. 25 There are no dedicated palliative care beds at this public hospital.
Over the study period, a palliative care consultation service was available with specialist nursing on-site four days per week within working hours. Specialist medical advice was available during working hours by phone and, as needed, in-person consultation through in reach from the CBPC team. In the after-hours setting, phone consultation was available through a statewide government nurse-led telehealth, plus an on-call specialist medical service. A 10-bed multidisciplinary palliative care inpatient service is colocated within a dedicated ward of St. John of God (private) hospital. Admission is open to public and private patients. The palliative care unit (PCU) does not provide an on-call service but does accept referrals directly from the ED.
The Southwest Community Palliative Care Service (SWCPCS) is a nurse-led multidisciplinary CBPC service that includes specialist physicians and allied health professionals, primarily caring for patients living in their own homes. SWCPCS accepts all progressive life-limiting illnesses across the lifespan, with the majority of patients being adults with malignant conditions. It operates a full team five days a week during office hours, with more limited nursing availability after-hours for complex situations such as procedural work or end-of-life care.
Participants
All patients known to the CBPC who presented to the regional hospital ED between June 1, 2022, and May 31, 2023, were included. The cohort was identified through having an active CBPC registration in the Electronic Palliative Care Information System (ePalCIS) system and patient presentation recorded in ED data for the same period. 22 There were no exclusion criteria.
Data collection
Data were collected through data extraction tools followed by a single reviewer from electronic clinical records through the BOSSnet clinical information system. 27 All variables were as recorded with no cross-reference undertaken. Demographic variables abstracted included age, sex, Aboriginal and Torres Strait Islander status, and residence postcode referenced to the MMM, which indicates rural and remote status. 26 The MMM ranges from metropolitan (MMM 1) to very remote (MMM 7).
Primary admission diagnosis and time of admission to CBPC were collected from ePalCIS. Emergency details include time of presentation, triage category (using the Australasian Triage Scale [ATS], a 5-point numerical scale), documented valid goals of care or advance care planning documentation, discharge destination, and specified inpatient location if applicable. 28 Advance care planning documentation was deemed valid if it was available and current at the time of the ED presentation. Advance care planning documentation included either an Advance Care Directive or Enduring Power of Guardianship. All diagnoses were completed by the treating ED clinician from a specified International Statistical Classification of Diseases and Related Health Problems, 10th Revision, Australian Modification (ICD-10-AM) list. 29 Clinical communication data collected was the communication between services as documented by any party, whether written, verbal, or with local or statewide services.
Data collapsing occurred for statistical analysis. This included defining work hours as 8 am to 4 pm, Monday to Friday. The palliative care admission diagnosis was grouped into cancer and noncancer categories. The 176 ED discharge diagnoses as per ICD-10-AM collapsed into 11 categories based on Ragg et al., with changes made by consensus from the multidisciplinary working group 4 (Supplementary Appendix). The categories include respiratory disease, neurological disease, cancer/cancer-related problem, musculoskeletal diagnosis, cardiovascular disease, urogenital disease, gastrointestinal/biliary disease, symptom diagnosis, metabolic/hematological disorder, other infection, and others. For comparative analysis, all forms of communication plus all types of advanced care planning were grouped together.
Data analysis
After quality checking to identify and rectify potential errors or inconsistencies, the data was collated in REDCap (Research Electronic Data Capture) software, then exported into a Microsoft Excel spreadsheet, followed by SPSS 24.0 for further statistical analysis.30,31 A convenience sample comprised all patients who met the inclusion criteria over the one-year study period. Thus, a sample power calculation was not applicable.
Descriptive statistics were used to characterize the data. Univariate analyses were performed, and continuous data were reported using mean (±SD) or median (interquartile range [IQR]), while categorical data were expressed as numbers (percentage). Chi-squared or Fisher’s exact test was used to compare counts or proportions. The independent samples t test was performed to compare means. The level of statistical significance was set at p < 0.05.
Ethics approval
Ethics approval (LNRP 2023.21) was gained from the Western Australia Country Health Service Human Research Ethics Committee.
Results
Figure 1 shows the study sample process. Study exclusions occurred as the patient involved in the ED presentation was not being actively cared for by CBPC and either had been evidently discharged or refused care. A total of 235 patients, 15.8% of known patients to CBPC, made 427 ED presentations over the index 12-month period. These represent 0.96% of the 44,234 all-age and 1.23% of all adults (426/34,587; 16 years and older) presentations.
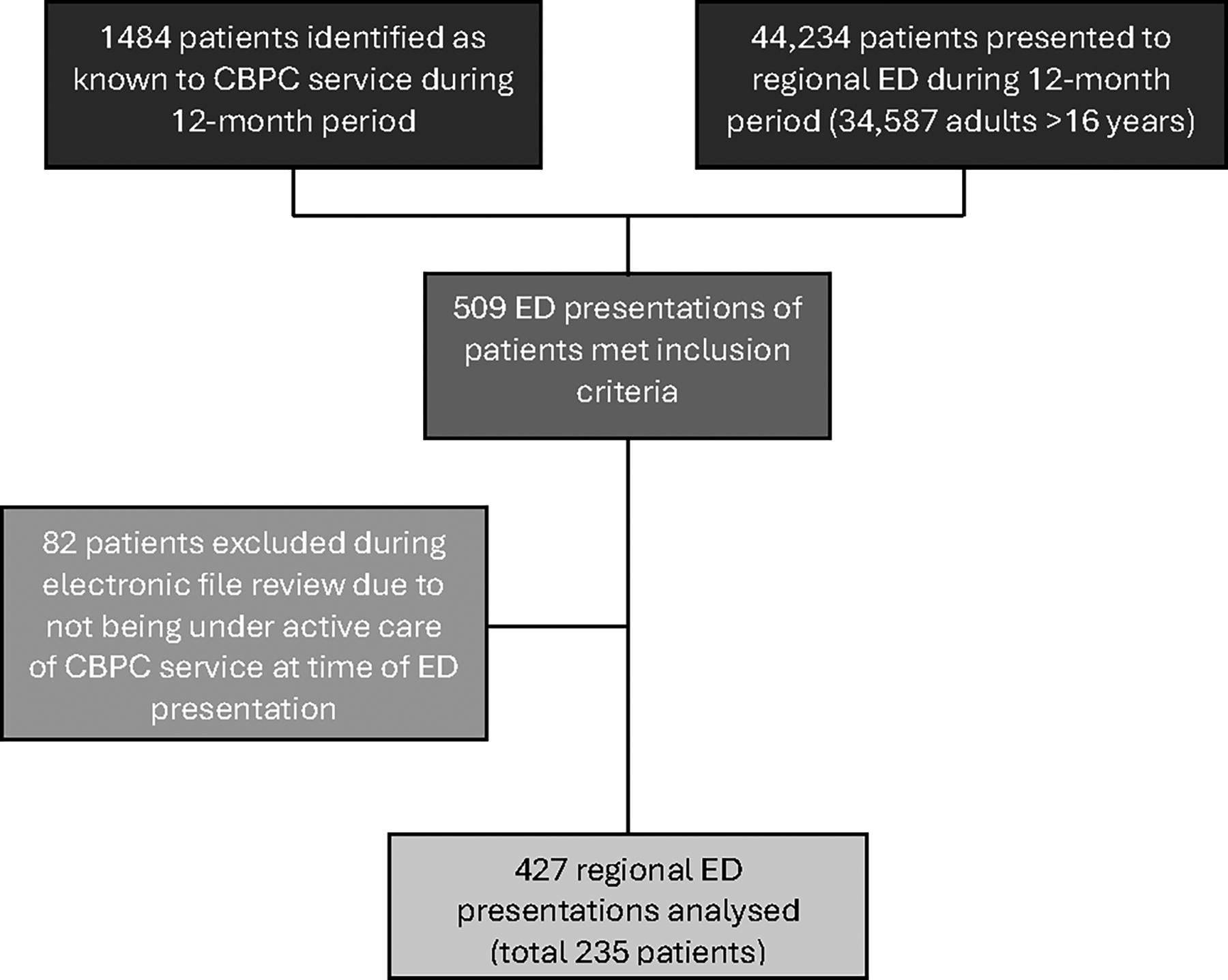
Flowchart of inclusion criteria and study sample process. CBPC, community-based palliative care; ED, emergency department.
Table 1 describes the characteristics of CBPC patients presenting to the ED during the study. There was one presentation of a child under 16 years. Most patients (169/235, 71.9%) were from the regional center (MMM2 location), with 26.4% (62/235) residing in small rural towns (MMM5 location), and had a primary cancer diagnosis (194/235, 82.6%).
Characteristics of Known Community Palliative Care Patients Presenting to Regional Emergency Department
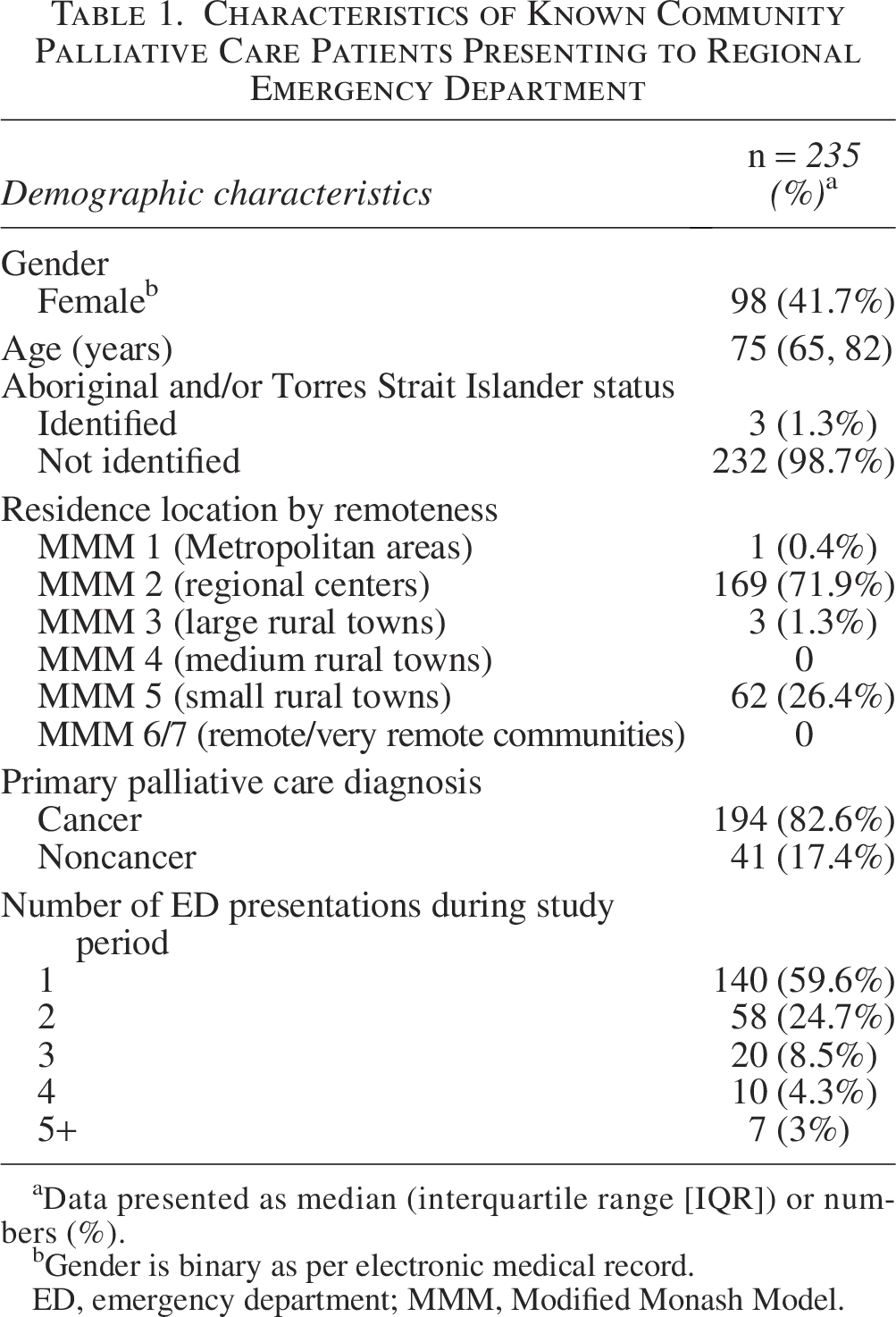
Data presented as median (interquartile range [IQR]) or numbers (%).
Gender is binary as per electronic medical record.
ED, emergency department; MMM, Modified Monash Model.
The clinical characteristics and outcomes of ED presentations are reported in Table 2.
Emergency Department Clinical Characteristics of Known Community Palliative Care Patients
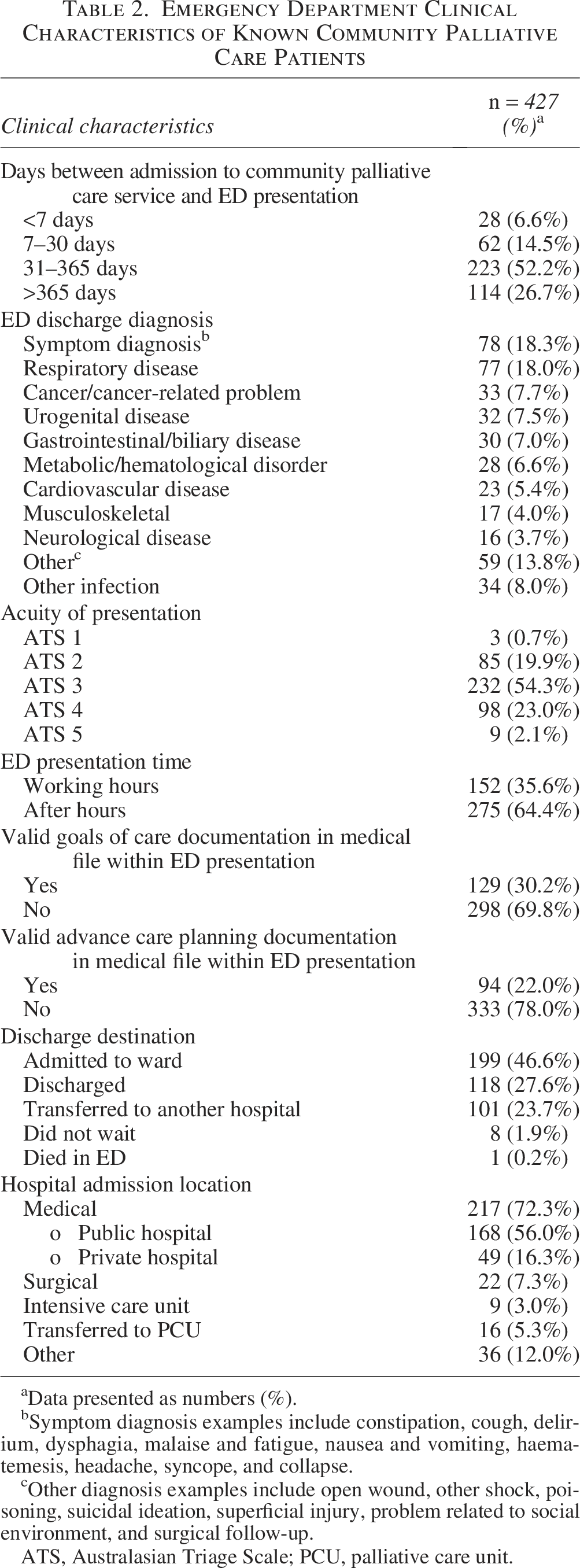
Data presented as numbers (%).
Symptom diagnosis examples include constipation, cough, delirium, dysphagia, malaise and fatigue, nausea and vomiting, haematemesis, headache, syncope, and collapse.
Other diagnosis examples include open wound, other shock, poisoning, suicidal ideation, superficial injury, problem related to social environment, and surgical follow-up.
ATS, Australasian Triage Scale; PCU, palliative care unit.
Most patients only presented twice or less to the ED during the index period (198/235, 84.3%). About half of the presentations were from patients known to the CBPC for between 31 and 365 days (223/427, 52.2%). Overall, 74.9% (320/427) of ED presentations had a high acuity of ATS 1–3, with 2.1% (9/427) being nonurgent at ATS 5. 152 (35.6%) presentations were within working hours. The two most common ED discharge diagnostic groups were symptoms (78/427, 18.3%) and respiratory disease (77/427, 18%). Admission to hospital and transfer to another hospital accounted for a total of 70.3% (300/427) of presentation outcomes. This compares to the general adult population in the same ED during the same period, in which the total admitted or transferred was 34.6% (11,958/34,587). Of those admitted, 72.3% (217/300) were for either public or private medical wards. The total number of those with any documented advance care planning was 195 of 427 (45.6%) ED presentations, or 53.6% (126/235) out of the total patients who presented to the ED during the study year.
Table 3 shows the documented communication between the ED and palliative care services. Overall, communication of any kind was found in 18.9% (81/427) of ED presentations.
Documented Communication Between the ED and Palliative Care Services
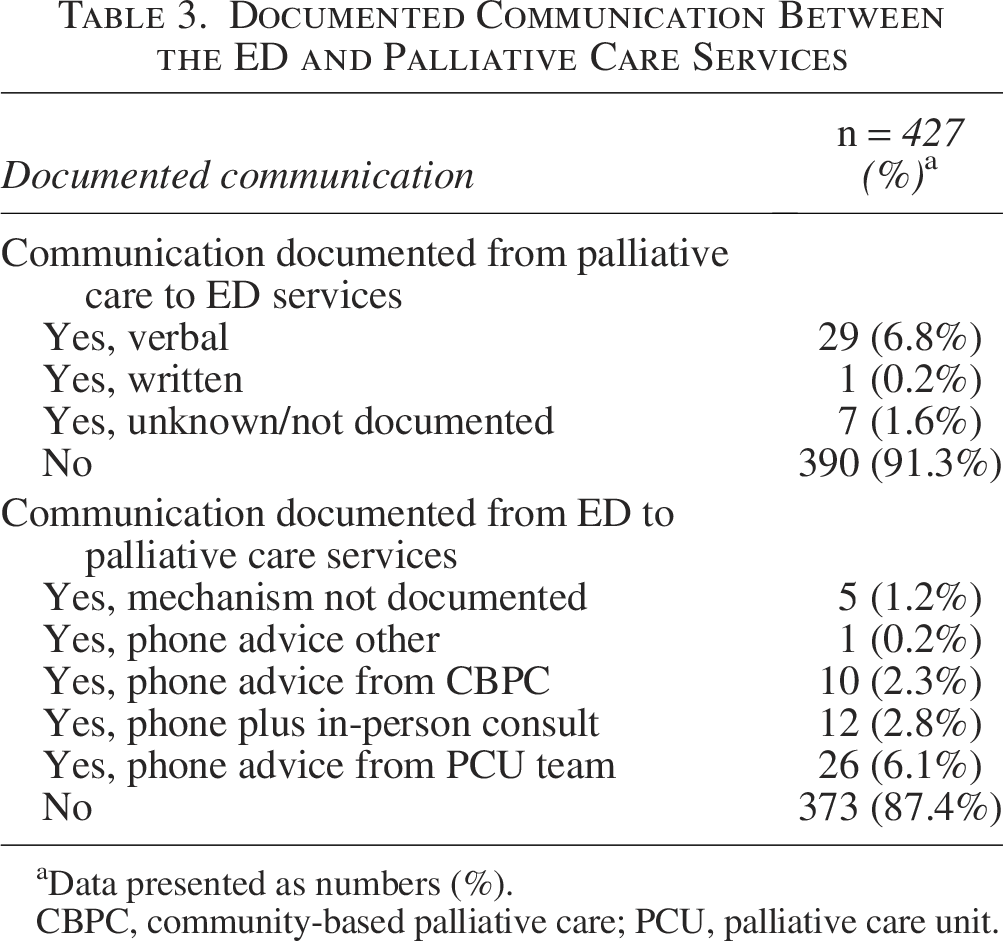
Data presented as numbers (%).
CBPC, community-based palliative care; PCU, palliative care unit.
Table 4 compares variables between ED presentations with documented communication between services and those without. Communication between services was found in 18.9% (81/427) of ED presentations. There were significant differences in documented communication based on time of presentation (55.6% [45/81]) during working hours with communication versus 31% (107/346) during working hours with no communication); the primary palliative care diagnosis (93.8% [76/81] in primary cancer with communication versus 78% [270/346] in cancer with no communication); and discharge destination (88.9% [72/81]) admitted to hospital with communication versus 65.9% (228/346) admitted to hospital without communication).
Comparison of Data by Presence of Any Documented Communication Between Services
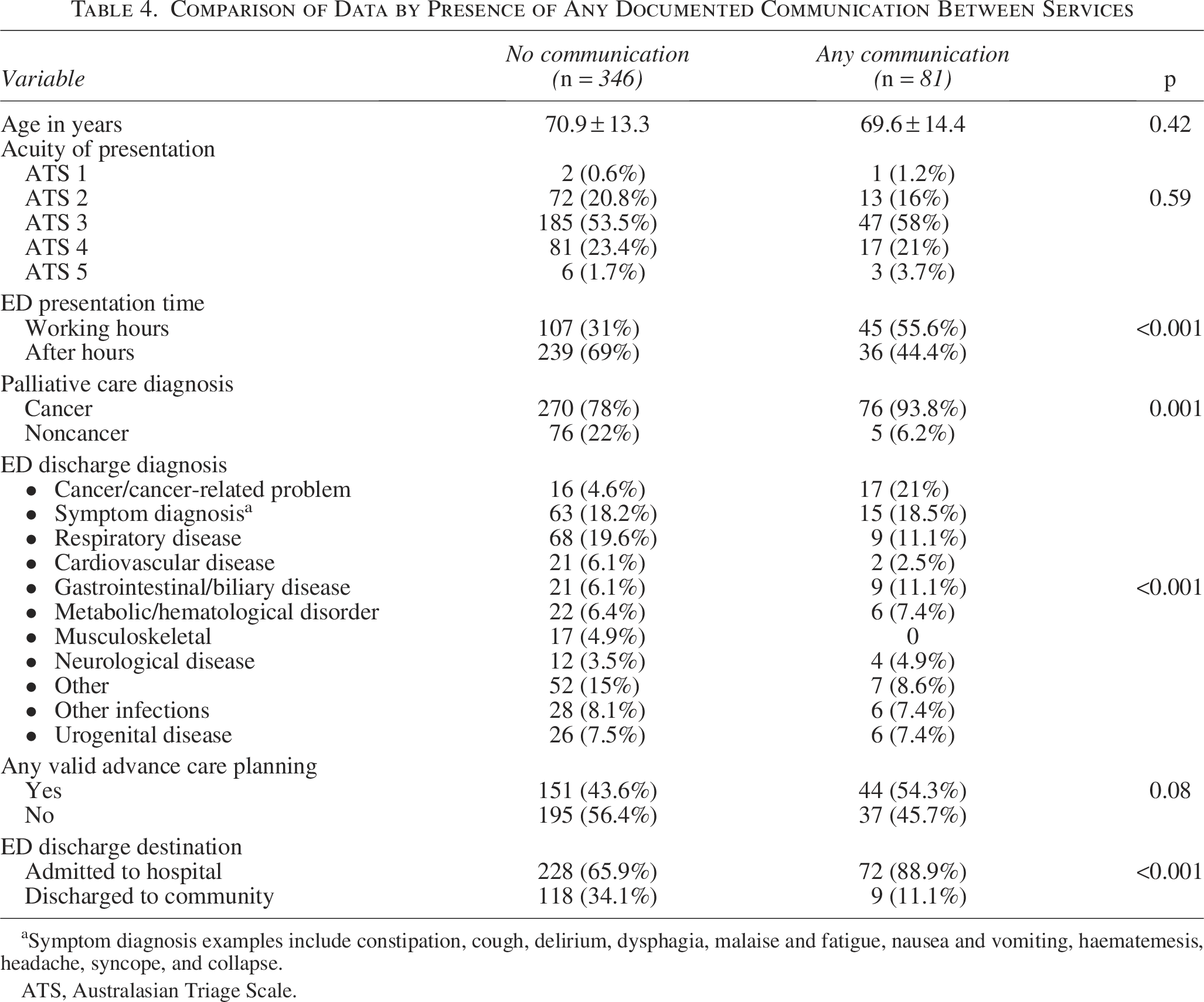
Symptom diagnosis examples include constipation, cough, delirium, dysphagia, malaise and fatigue, nausea and vomiting, haematemesis, headache, syncope, and collapse.
ATS, Australasian Triage Scale.
Discussion
This study has shown that active CBPC patients represent an important proportion of regional ED presentations, with 15.8% of active patients of service, or 1.23% of all adult ED presentations, presenting within the year. The majority had two or fewer presentations (84.7%), with only 3% attending five or more times. This presentation rate is lower than that of other published studies, with a U.K. study showing 29.4% of patients presenting at least once within three months of a palliative care contact. 8 Our results resemble a Belgian study by Maetens et al. who showed those receiving CBPC attended the ED 15.2% in the last two weeks of life, in comparison to 28.1% of those who were not known to the community service. 32 This difference may be related to our study being a single-center study, but it may also represent a true reduction in ED presentations when patients are known to use a CBPC service.17–21
The present study shows that 70.3% of presentations were admitted to the hospital, double that of the general adult population in the same hospital during this 12-month period (34.6% [11,958/34,587]). This may represent a genuine high level of need for patients in this cohort, confirming findings of previous studies, and challenges the notion that many or most ED presentations of palliative care patients are avoidable or unnecessary. 8 Patients in our cohort were triaged higher than national Australian averages for the 2022–2023 financial year, with 56.9% nationally being triaged urgent or higher (ATS 1–3) versus 74.9% in this study, demonstrating a high acuity in ED presentations. 33 In keeping with symptom management as a core palliative care skill, symptom diagnosis was the most common ED diagnosis, with respiratory disease second. This is like an Irish retrospective review of community palliative care patients, 93.5% having cancer, which described symptom presentations of dyspnea, nausea/vomiting/constipation, and uncontrolled pain accounting for 57.5% of ED presentations. 7 Of interest, only 5.3% of patients were admitted in this study directly to the colocated PCU. This should be explored further as it potentially could identify contributing factors such as a lack of bed availability, barriers to after-hours access, uncertain goals of care, or acuity of ED presentations, determining this figure.
The study showed patients were under the care of the CBPC team for a significant time, with 78.9% of them being admitted to CBPC for longer than 31 days at ED presentation. The rate of valid advance care planning documents available at ED presentation was 22%, which, although not a majority of cases, is higher than studies showing a community prevalence of 6% or 15.7% in patients over 65 years in acute hospitals.34,35 Additionally, 30.2% had a valid goal of care documentation, indicating agreed treatment goals and limits, with higher availability than advance care planning documentation. The total of 45.6% who had any form of advance care planning at ED presentation was remarkably similar (46%) to a recent Australian study of patients with life-limiting illness. 4 Our study did not show that documented advance care planning made a statistical difference in communication between ED and palliative care services (p = 0.08). Advance care planning has been demonstrated to prevent emergency hospitalizations for people toward the end of life, although a systematic review in 2022 showed mixed results regarding CBPC improving advance care planning.21,36,37 Notably, a survey of clinicians in a Victorian ED showed that the inability to access information, such as goals of care, is associated with an increase in burdensome but futile medical care. 38
Documented communication was limited from palliative care to ED services at only 8.6% and in return at 12.6% of presentations. Overall, 18.9% of presentations had some form of cross-service communication documented. While there is no benchmark figure, it would be reasonable to reflect that this falls short of meeting the national standard for effective communication and integrated care during the transition between services. 23 This confirms an Australian study with clinicians highlighting the need to improve communication between services. 10 Our data showed 55.6% (45/81) of any communication documented occurred for ED presentations during working hours. The overall figure may be limited by palliative care availability in an after-hours setting, as although 24/7 specialist palliative care clinical advice was available, it may not be well known to ED clinicians or deemed appropriate as urgent communication.
Documented communication occurred more often for patients with cancer diagnoses when they had cancer/cancer-related problems and was less likely for patients with noncancer diagnoses, such as a cardiovascular or respiratory disease diagnosis. This may reflect the higher rates of acuity and admission for oncology patients. 39 While the evidence suggests high confidence by ED physicians in being skilled in pain and end-of-life management related to advanced cancer, it also shows the high complexity and barriers to managing their care in an ED setting.10,40 Additionally, interviews with palliative care patients highlighted the inconsistency of experiences within ED, with COPD patients having overall positive experiences, but cancer patients describing concerns about poor oncology or palliative care expertise. 1 These experiences may be contributing to the communication findings. Communication also occurred more often with admission to the hospital and less likely with discharge from the ED. It also possibly underlies different expectations between the cohorts. Our study did not explore reasons for communication, nor whether CBPC was involved in the reason patients had an ED presentation. It is noted that this study was completed when only limited on-site specialist palliative care consultative support was available.
Limitations
To our knowledge, this research is the first to examine CBPC patients, their interaction with the ED, and communication between the service providers.
This was an unfunded clinically embedded study in a rural setting. The study design was realistic given its real-world setting; however, some limitations are unavoidable. Interpretation of generalizability needs to consider our regional ED setting and limited after-hours palliative care consultation service.
Bias was reduced by utilizing the available data in the medical record without interpretation or reviewer analysis. The inclusion criteria were for “active” community palliative care patients, but did not analyze how extensively the patient was engaged with or the management input from the service. Furthermore, patients attending the ED with a palliative care diagnosis who were not previously known to the CBPC service but may have needed palliative care input during the presentation were excluded. By analyzing the biggest ED in the region for community palliative care patients across the region, we would not have collected data on ED presentations in other hospitals by the same cohort of patients. Furthermore, the diagnoses collated and collapsed into categories were as per the emergency clinicians and are limited to specific institutional coded items, which may not capture the complexity of palliative care needs in presentation or whether related to their primary palliative care diagnosis. Last, the documented communication data will be skewed by the reduced availability of palliative care services in the after-hours setting, and potentially by some contacts affecting care but undocumented.
Conclusion
Community palliative care patients are an important cohort who will present to regional EDs. This study shows that patients known to CBPC have high acuity and admission rates compared to the general population, indicating a high level of need, in contrast to the concept of avoidable ED presentations. Communication between services involved was overall low but higher when patients had a cancer/cancer-related problem or were being admitted. Further research, including multisite and longitudinal studies, would allow for an in-depth analysis of the ED presentations, exploring the patient’s complex needs, whether this is related to their involvement in CBPC service, and the role of different types of communication across services for improving integrated, patient-centered care.
Authors’ Contributions
The authors confirm contribution to the article as follows: Study conception and design: S.B., S.D., O.W., B.P., and M.B.S.; data collection: S.B., O.W., B.P., and S.D.; analysis and interpretation of results: S.B., M.E., S.D., O.W., B.P., and M.B.S.; and draft article preparation: S.B., M.E., S.D., O.W., B.P., and M.B.S. All authors reviewed the results and approved the final version of the article.
Footnotes
Author Disclosure Statement
All authors declare that they have no conflicts of interest.
Funding Information
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.