
Abstract
Objective:
To determine the prevalence of obesity among a cohort of pregnant patients with high compared with low adverse childhood events scores.
Study design: Descriptive study methods:
The study was part of a large study of adverse childhood events among pregnant women seeking care in a safety net hospital from June 2022 to June 2023. The patients were seen in a variety of settings (a routine prenatal clinic, a high-risk clinic, an antepartum testing unit, an obstetrical ultrasound unit, and a labor and delivery suite). They were randomly approached and asked to complete a previously validated questionnaire for their Adverse Childhood Experience score (ACE score). Their body mass index (BMI) on their first visit was recorded. BMI was categorized as overweight (BMI > 25), class I obesity (BMI > 30), class II obesity (BMI > 35), and class III obesity (BMI > 40). This study was approved by the Valleywise Institutional Review Board.
Results:
Three hundred and forty-nine patients were approached and 320 agreed to complete the questionnaire. Eighty percent of patients had an initial prenatal visit BMI >25 and 62% had an initial BMI that was categorized as obese. Patients with a high ACEs score were more likely to have a BMI in the obese category compared with those in the low-risk group with an odds ratio of 1.34 (95% CI [0.7907–2.2798], p = 0.275).
Conclusion:
Maternal obesity is a well-known risk factor for numerous adverse obstetrical and neonatal outcomes. While the CDC reported a national prepregnancy obesity rate of 29.0% in 2019, our patients were 2.14 times more likely to be obese. Obesity was more prevalent in women with high ACEs scores. Safety net hospitals should be cognizant of marked increase in obesity in their obstetrical patients, especially those with high ACEs scores, and develop interventions that incorporate trauma-informed care.
Introduction
The prevalence of obesity among women in the United States has been increasing over the last 20 years. In 2017–2018, the prevalence of women who were overweight or obese in the United States was 41.9%. 1 More specifically, the prevalence of severe obesity (defined as a body mass index [BMI] > 40) was found to be more prevalent in women (11.5%) compared with men (9.6%). 1 This is especially important to consider in women of childbearing age as maternal obesity has been previously associated with poor obstetrical outcomes such as gestational diabetes, proteinuric preeclampsia, induction of labor, cesarean delivery, postpartum hemorrhage, genital tract infections, urinary tract infections, wound infections, birthweight above the 90th percentile, and intrauterine fetal demise.2,3
There have been several studies showing a positive correlation between adverse childhood experiences (ACEs) and increased BMI.4–7 The ACE questionnaire was developed by Dr. Vincent Felitti in the early 1990s to examine the relationship between ACEs and the physical and mental health of adults.8,9
With the rise in national pre-pregnancy obesity rates to 29.0% in 2019, 10 we sought to determine the prevalence of obesity among a cohort of pregnant patients receiving care at an urban safety net hospital in Phoenix, Arizona who participated in a larger study of their ACEs score.
Methods
The study was conducted between June 2022 and June 2023 among patients seeking obstetrical care at a large urban safety net hospital in Phoenix, Arizona, who participated in a study of adverse childhood events. Some of the experiences that are included in the questionnaire relate to experiencing or witnessing violence, abuse, neglect, and having a sense of familial instability through separation or incarceration. 9 Scores of 4 or more on the ACE questionnaire are categorized as high risk and are generally associated with long-term health consequences. 6
The study size was determined to be approximately 18% of the total deliveries in the department, which was thought to be an adequate representation of the patient population. The inclusion criteria were women aged 18 or older presenting to a Valleywise clinic with proficiency in English or Spanish. Patients were excluded if they denied consent to participate, were not fluent in either English or Spanish, or if they were currently incarcerated. A high ACEs score was defined as a score of 4 or more. 11 The BMI on the initial prenatal visit was recorded. BMI was categorized as overweight (BMI > 25), class I obesity (BMI > 30), class II obesity (BMI > 35), and class III obesity (BMI > 40). 12
Pregnant patients seen in a variety of settings (a routine prenatal clinic, a high-risk clinic for patients with complicated pregnancies, an antepartum testing unit, an obstetrical ultrasound unit, and a labor and delivery suite) were randomly approached and asked to complete a previously validated questionnaire for their ACEs score (Fig. 1) in either English or Spanish. Spanish interpreters were available upon request. Written consent was obtained prior to the administration of the survey.

ACES questionnaire. ACES, Adverse Childhood Experience score.
Data collected from patient records included maternal age, language, gravidity, parity, gestational age at time of survey, initial visit BMI, past medical history, medications, prior outcomes, zip code, and marital status.
Clinical documentation of maternal and obstetric data from the EMR were abstracted by the authors of the study and stored in a Research Electronic Data Capture (REDCap) database along with ACE questionnaire score.
A χ2 test of independence and odds ratio were performed to examine the relationship between ACE scores and BMI. The online calculator at vassarstats.net was utilized for all statistics. This study was approved by the Valleywise Institutional Review Board.
Results
Three hundred and forty-nine patients were approached and 320 agreed to participate and completed the questionnaire, 279 questionnaires were completed in English and 41 in Spanish (Fig. 2). Subjects ranged between ages 18 and 48 with a mean of 28.65 years old. Initial visit BMIs ranged from 16.59 to 71.17 kg/m2 with an average BMI of 32.66 kg/m2. Eighty percent of total patients in the study had an initial prenatal visit BMI >25 and 62% had initial BMI that was categorized as obese. Of those patients, 81 subjects (25.3%) had an ACEs score of ≥4, indicating high risk, while 239 had low ACEs scores. Among the 81 high risk patients, 10 were categorized as overweight and 54 were categorized as obese (25 class I, 16 class II, 13 class III) (Fig. 3a). Among the low-risk ACE score patients, 50 were categorized as overweight and 143 were categorized as obese (65 class I, 47 class II, 31 class III) (Fig. 3b). Patients with a high ACE score were more likely to have a BMI in the obese category compared with those in the low-risk group (Fig. 4) (95% CI [0.7907–2.2798], p = 0.275).
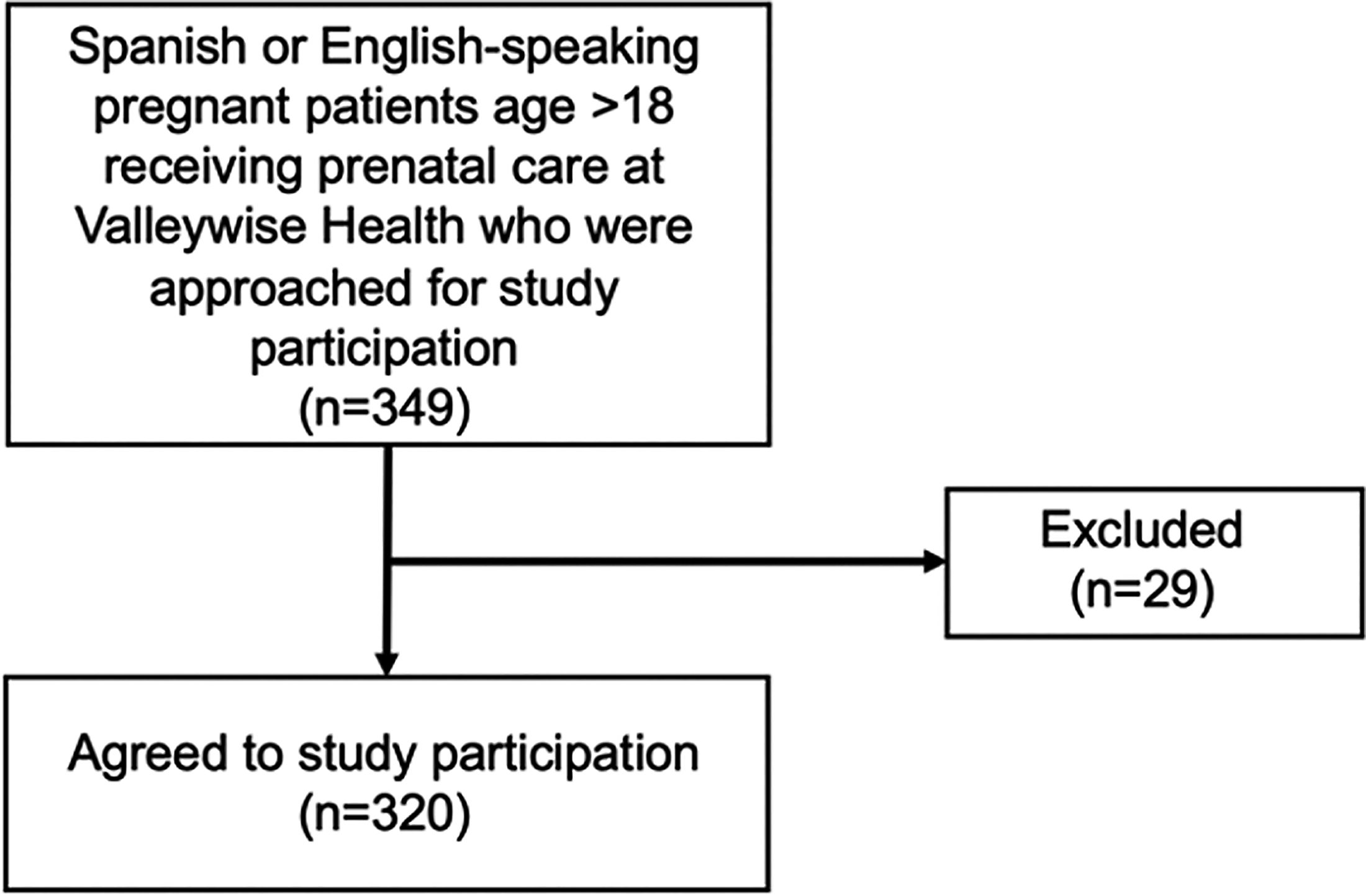
Enrollment.
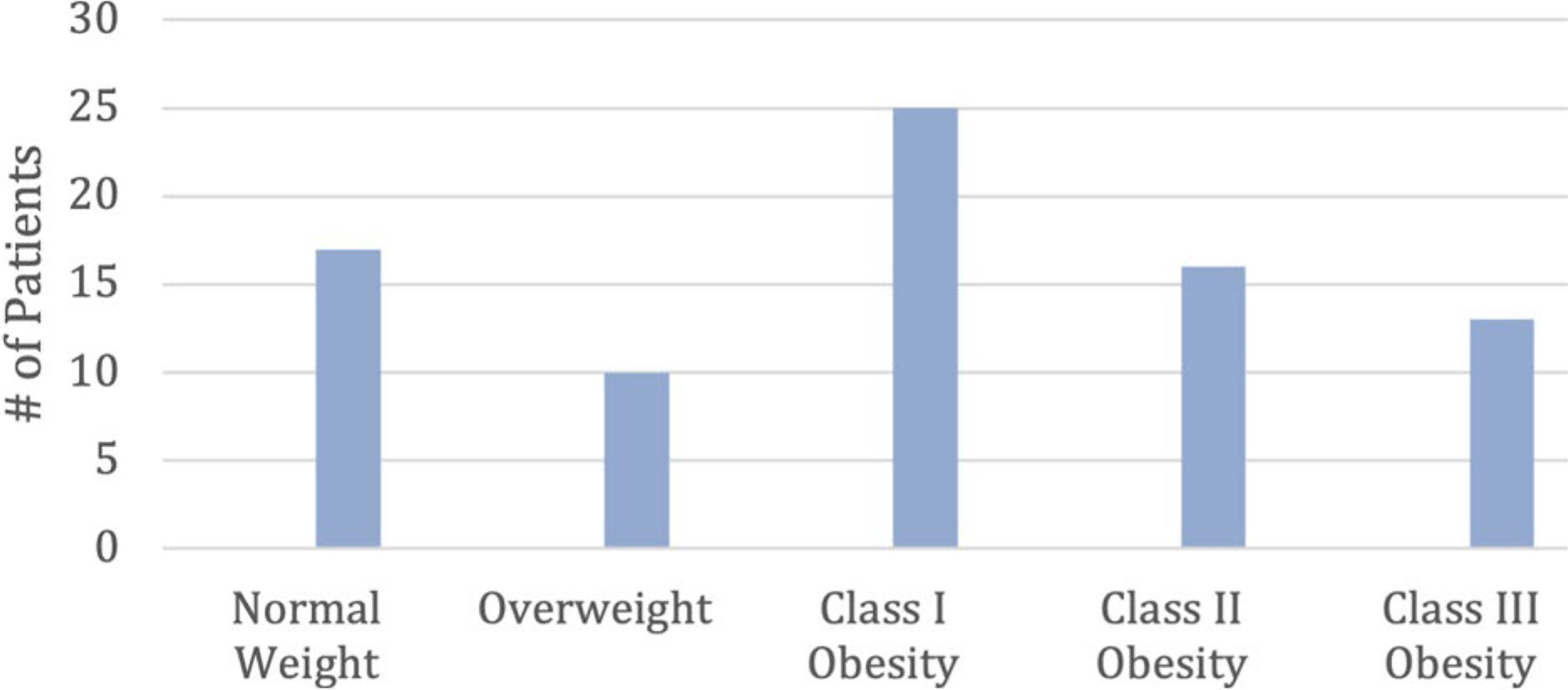
The number of patients in each weight category.
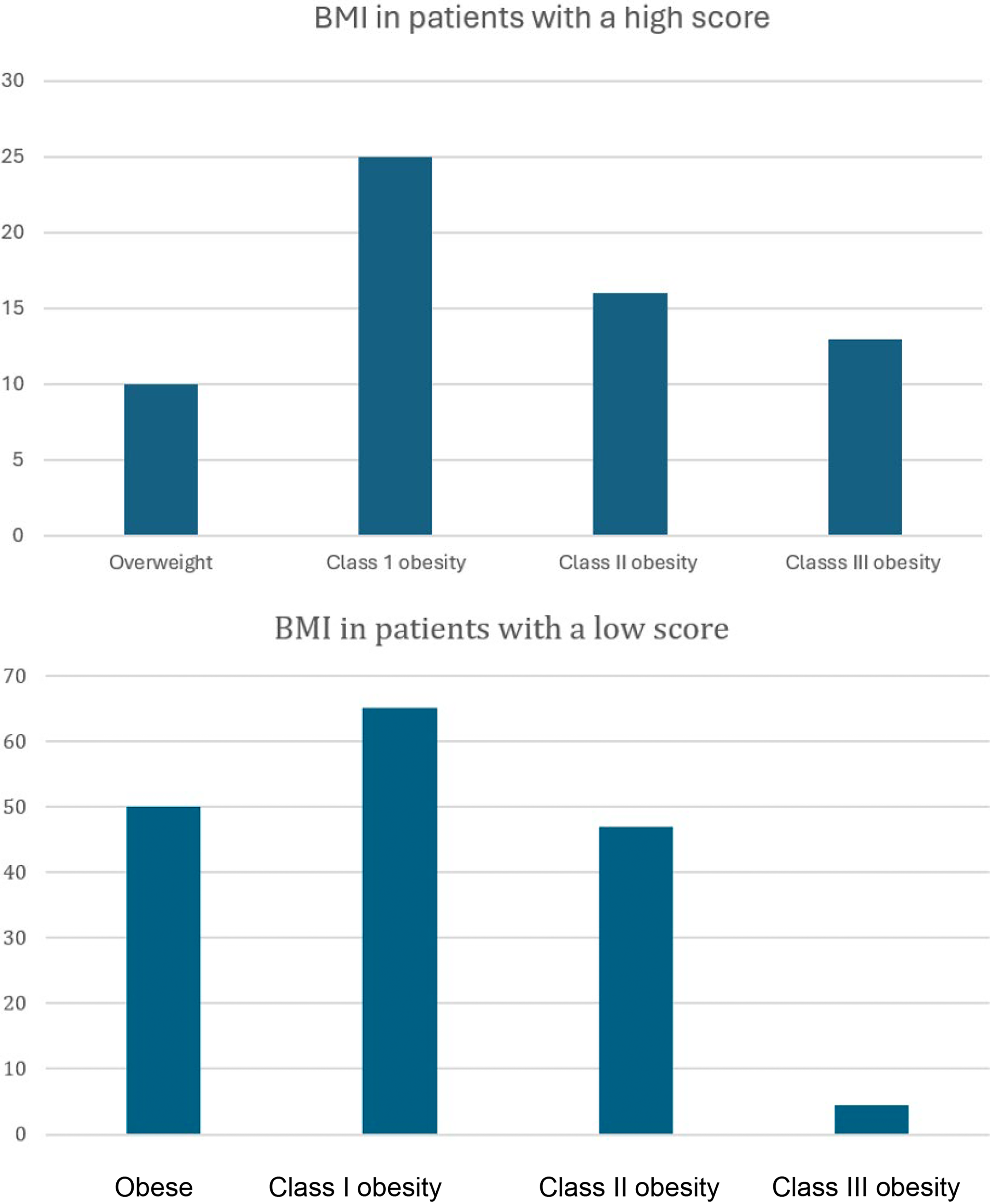
BMI in patients with a high ACES score compared to patients with a low ACES score. BMI, body mass index.
Discussion
Maternal obesity is a well-known risk factor for numerous adverse obstetrical and neonatal outcomes. The CDC reports a national prepregnancy obesity rate of 29.0% in 2019. In comparison, our patients were 2.14 times more likely to be obese. Obesity was more prevalent in women with high ACEs scores. Th.
During pregnancy, women have the opportunity to receive care regardless of socioeconomic status, which makes this time period the ideal time to address some of the social impacts of health that affect patients. With the increased number of visits associated with pregnancy, this allows time to educate patients about risk reduction, as well as give the patient an opportunity to receive mental health and nutritional consultations.
There is always a concern that asking patients about past trauma will result in revisiting painful memories and causing the patient distress. Anecdotally, we have not found this to be an issue. Our facility is fortunate to have dedicated on-site social workers who provide short-term counseling as well as referrals to our behavioral health colleagues. It is clear from the literature that childhood trauma has widespread effects on health and significantly impacts the risk of multiple adverse outcomes. 6 As such, we feel it is imperative to address the history of trauma recognizing the need to provide appropriate support to patients. We recognize that other providers may not have as easy access to behavioral health referrals as we do so we would encourage them to become familiar with what resources their communities offer and perhaps to become advocates for starting programs if none are available.
Some strengths of our study include that this screening tool has been previously validated in multiple populations and is easily completed, and the vast majority of patients (320/349) agreed to participate in the study. In addition, the questionnaire was available in both English and Spanish, which are the languages that most of our patients speak and interpreters were available upon request. Another strength as outcome data were available on most who enrolled in the study.
Some limitations of our study included that, as a safety net hospital, the majority of patients at Valleywise Health Medical Center have limited financial resources and do not reflect all socioeconomic groups. The hospital has a large refugee population many of whom do not speak English. It was prohibitively expensive to have the study materials translated into a language other than Spanish and we did not have the resources to support such a cost. We hope to be able to include such patients in future studies since there are very few studies looking at ACEs scores in refugee patients. The limited data that is available shows refugees have a higher rate of ACEs compared with the general population. 13 The hospital treats a number of women who are incarcerated and therefore ineligible to participate unless there is specific approval from the IRB. Our experience with incarcerated women has taught us that many have had extensive childhood and adult trauma. We hope to be able to include women who are incarcerated in a future study. Another limitation of the study was that we only looked at the total ACEs score and did not study which adverse events were more common or if there were a combination of events that really impacted the rate of obesity. Other limitations include that the questionnaire was given by a researcher who did have an established relationship with the patient. Patients may have been reluctant to share their history with someone they did not know. Patients may have been embarrassed to share these details and prior work has shown patients may have been in denial to the extent of their trauma.14,15
In conclusion, this study emphasizes the importance of including the ACE questionnaire as part of the generic intake screening in the obstetrical clinics, especially in safety net hospitals. Such institutions should be particularly cognizant of the impact of a high ACEs score on the risk of obesity in their obstetrical patients and develop trauma-informed interventions that address this risk factor. There is still the need for continued research on this topic, particularly with some of the less studied populations such as refugees and inmates. Additionally, it remains to be seen if a high ACEs score has a similar impact on obesity in a broader segment of socioeconomic status. However, it is clear that patients with a high ACEs score who seek care in a safety net hospital should be recognized to be at significant risk for obesity and likewise, to understand that obese patients in that setting have more commonly suffered past trauma and would benefit from trauma-informed care.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.