
Abstract
Background:
Chronic constipation (CC) adversely impacts quality of life (QoL). Health literacy (HL) may positively influence QoL, but evidence of this is limited in patients with CC. We examined the association between HL and QoL in patients with CC and explored sex differences.
Methods:
An online cross-sectional survey was conducted among 423 Japanese patients with CC who had been prescribed laxatives for at least 6 months. HL and QoL were assessed using the 14-item Health Literacy Scale and Patient Assessment of Constipation Quality of Life Questionnaire (PAC-QoL), respectively.
Results:
Females had higher functional HL (p = 0.004, Cohen’s r = 0.14), poorer QoL (indicated by higher PAC-QoL scores; p < 0.001, Cohen’s r = 0.17), and greater constipation severity (p = 0.002, Cohen’s r = 0.15) than males. Multivariable regression showed that higher functional HL (regression coefficient [β] = −1.06, 95% confidence interval [CI] [−1.53, −0.60]) was associated with better QoL, whereas higher critical HL (β = 1.34, 95% CI [0.71, 1.94]), female sex (β = 3.73, 95% CI [0.05, 7.18]), part-time employment (β = 3.17, 95% CI [0.54, 5.87]), and greater constipation severity (β = 2.69, 95% CI [2.24, 3.13]) were associated with poorer QoL. These associations did not differ substantially by sex.
Conclusions:
Functional HL was positively associated with QoL, while critical HL was negatively associated with QoL. Although females reported poorer QoL, the association between HL and QoL was consistent across the sexes, suggesting that comprehensive support, including HL interventions, may benefit female patients.
Introduction
Chronic constipation (CC) is a common and heterogeneous condition in which functional constipation (FC) constitutes a large proportion of cases. FC has a global prevalence of approximately 10.1%−15.3%. 1 The prevalence of FC increases with age and is more common in females than in males. 1 In a large-scale survey of individuals who underwent a medical checkup in Japan, the prevalence of FC according to the Rome IV criteria was 2.1%; however, 19.2% were reported to have constipation symptoms. 2 Although FC is not life-threatening, its long-term persistence can lead to CC, which is regarded as a condition that adversely affects quality of life (QoL), impairs work productivity, and increases health care costs. 3 Moreover, a study using the 36-Item Short-Form Health Survey (SF-36), 4 a measure of general QoL, reported significantly diminished QoL, both physically and mentally, in patients with CC compared with controls without the condition. 5 The level of SF-36 scores in patients with constipation was comparable to that in patients with allergies, musculoskeletal conditions, and inflammatory bowel disease. 6
Because of the varying severity of constipation among individuals and the wide array of available treatment options, a high level of health literacy (HL), encompassing an individual’s ability to access, understand, use, and evaluate health information, 7 is essential for patients with CC to determine the most appropriate management approach. In Japan, physicians have predominantly prescribed sennosides and magnesium oxide as the pharmacological treatments for CC for many years. However, since 2012, the launch of numerous new medicines has rapidly expanded the range of available prescription options. 8 In addition, sennosides, magnesium oxide, Chinese herbal medicines, and suppositories for constipation are readily accessible as over-the-counter medications. Moreover, patients with CC are required to continue self-care, such as adequate fiber and fluid intake, increased physical activity, and self-administered abdominal massages in daily life. 9
A meta-analysis revealed a moderately positive correlation between HL and QoL. 10 Nevertheless, some studies have reported negative or no correlations. 11 A survey of patients with chronic heart failure found no relationship between HL and QoL after adjusting for covariates. 12 In patients with type 2 diabetes, one survey indicated that HL was not directly linked to QoL; however, it indirectly influenced QoL through self-care activities and self-efficacy. 13 A survey of patients with acute coronary syndrome revealed a negative correlation between HL and QoL. 14 To the best of our knowledge, there has been limited research on the association between HL and QoL in patients with CC. Therefore, in this study, we aimed to evaluate the association between HL and QoL in patients with CC and explore sex differences.
Methods
Study participants and procedures
In March 2024, an online cross-sectional survey of patients with CC was conducted. The sample size was determined to exceed 400 participants based on the estimation that the total patient population was approximately 4.4 million. 15 This calculation ensured that 385 responses were obtained, which was necessary to achieve a 5% margin of error, a 95% confidence level, and a 50% response rate. The participants were randomly recruited from a pool of individuals registered with Cross Marketing, Inc. (Tokyo, Japan), one of the largest internet survey research companies in Japan. Because the panel is composed of individuals who voluntarily register for online research, some degree of selection bias cannot be ruled out; however, the panel is broad and demographically diverse, and random sampling within this panel is considered acceptable for population-based internet surveys. Patients were eligible for inclusion if they were 18 years of age or older and had CC, defined according to the Japanese Evidence-based Clinical Guidelines for Chronic Constipation 2023. 8 In these guidelines, CC is characterized by symptoms persisting for at least 6 months and fulfilling the Rome IV symptom-based criteria during the preceding 3 months. 16 Consistent with these criteria, eligible patients had been prescribed laxatives by a physician for a minimum duration of 6 months. The exclusion criteria were pregnant patients, health care professionals, and patients receiving opioids for cancer or chronic pain management.
The survey included the 14-item Health Literacy Scale (HLS-14), 17 Patient Assessment of Constipation Quality of Life Questionnaire (PAC-QoL), 18 the Constipation Scoring System (CSS), 19 and demographic and disease-related questions. Demographic characteristics included age, sex, marital status, occupation, and educational level. Clinical characteristics included the clinical department, duration of doctor visits, number of other internal medicines prescribed, and comorbidities such as gastrointestinal diseases (e.g., gastroduodenal ulcers, functional dyspepsia, and irritable bowel syndrome) and diseases related to secondary constipation (e.g., diabetes, Parkinson’s disease, and depression).
This study was conducted in accordance with the principles of the Declaration of Helsinki. Ethical approval was obtained from the Institutional Review Board for Clinical Research at Kyushu University, Japan, on November 24, 2023 (No. 23272–00). An online survey was administered anonymously. Written informed consent was not obtained; however, consent was obtained by presenting an explanation of the research and checking the box for consent.
Measurements
Health literacy
HL levels were assessed using the HLS-14, 17 which was developed for the Japanese population and has demonstrated reliability and validity. The HLS-14 is rated on a 5-point Likert scale, ranging from 0 to 4. The total score ranges from 0 to 56 points, with higher scores indicating greater HL. This scale has three subscales, namely, functional HL, communicative HL, and critical HL, based on the three-dimensional model proposed by Nutbeam. 20 Functional HL refers to basic skills for obtaining and understanding health information, communicative HL involves the ability to interpret and apply information through interaction, and critical HL reflects skills to critically evaluate information for informed decision-making. 20
Constipation QoL
Disease-specific QoL in patients with constipation was assessed using the PAC-QoL, 18 a widely recognized and reliable tool. A Japanese version of the scale was developed, and its reliability and validity were confirmed. 21 It was validated on a 28-item scale and rated on a 5-point Likert scale ranging from 0 to 4. The total score ranged from 0 to 112 points, with higher scores indicating a lower QoL. It has four subscales: physical discomfort, psychosocial discomfort, worries/concerns, and satisfaction.
Severity of constipation
Severity levels of constipation were assessed using the CSS developed by Agachan. 19 The 8-item scale was rated on a 5-point Likert scale; however, one item was rated on a 3-point Likert scale. Hence, seven items were scored from 0 to 4, and one item was scored from 0 to 2, resulting in a total score ranging from 0 to 30. Higher scores indicated greater severity of constipation.
Statistical analyses
Descriptive statistics were obtained by calculating frequencies and proportions for categorical variables and medians and interquartile ranges (IQR) for continuous variables. However, for comparison with previous studies, the means and standard deviations were also included. Sex differences in demographic and clinical characteristics, HLS-14, and PAC-QoL were assessed using the chi-squared test for categorical variables and the Wilcoxon rank-sum test for continuous variables. Effect sizes are reported as Cramer’s V for categorical variables and Cohen’s r for continuous variables. Correlation coefficients between HLS-14 and PAC-QoL scores were calculated using Spearman’s rank-order correlation. Ordinary least squares (OLS) regression was performed to examine the association between the HL subscales and PAC-QoL scores using the total score. Three hierarchical models were constructed: unadjusted, adjusted, and fully adjusted models. The unadjusted model included only the HL subscales as independent variables. The adjusted model also included demographic characteristics such as sex and age. The fully adjusted model further incorporated clinical characteristics, including disease severity and comorbidities. Regression coefficients (β) and 95% confidence intervals (CIs) were estimated using bootstrap resampling (2000 repetitions, bias-corrected, and accelerated method) to account for the potential nonnormality of residuals. The model fit was assessed using the coefficient of determination (R2) and adjusted R2. In the subgroup analyses, sex-stratified analyses were conducted using fully adjusted models. In the sensitivity analysis, robust regression (Huber weighting) was performed to assess the robustness of the findings compared with OLS regression. Outliers were not excluded from the primary analysis, and a robust regression was used to confirm that the findings were not driven by influential cases. Statistical significance was set at p < 0.05. All statistical analyses were conducted using R version 4.3.1 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Description of the participants
According to a report from the research company, of the 18,677 individuals who expressed their willingness to participate in the survey, 763 met the eligibility criteria and 464 provided consent to participate. Of these, 41 discontinued participation during the process, resulting in 423 individuals being included in the final analysis, yielding a response rate of 55.4%. There were no missing values because the online survey was designed to prevent progression to the subsequent screen if any values were missing. The demographic and clinical characteristics of the participants are shown in Table 1. The mean age of participants was 52.2 ± 15.8 years, ranging between 18 and 85 years. Most participants were female (63.1%), married (69.0%), received laxatives from nonspecialized departments (66.2%), and had no comorbidities such as gastrointestinal diseases (70.4%) and diseases related to secondary constipation (65.0%). The mean total HLS-14 score was 34.0 ± 9.0, with a median of 33.0 [27.0–40.0]. Similarly, the mean total score for the PAC-QoL was 45.7 ± 21.8, with a mean item score of 1.6 ± 0.8 and a median of 42.0 [29.0–60.0]. Table 1 presents all variables by sex. Females had significantly higher total HLS-14 (p = 0.020, Cohen’s r = 0.11) and functional HL scores (p = 0.004, Cohen’s r = 0.14), whereas they had more severe CSS (p = 0.002, Cohen’s r = 0.15) and higher total PAC-QoL scores, indicating poorer QoL (p < 0.001, Cohen’s r = 0.17). Males were older (p < 0.001, Cohen’s r = 0.31), had more comorbidities related to secondary constipation (p < 0.001, Cramer’s V = 0.20), and were prescribed a greater number of other medications (p < 0.001, Cohen’s r = 0.18). The effect sizes indicated small-to-moderate differences.
Demographic and Clinical Characteristics, Health Literacy Scale-14, and Patient Assessment of Constipation Quality of Life Questionnaire of Participants, with Comparisons by Sex

CSS, constipation scoring system; HL, health literacy; HLS-14, Health Literacy Scale-14; IQR, interquartile range; PAC-QoL, Patient Assessment of Constipation Quality of Life Questionnaire; SD, standard deviation.
Correlations between HL and QoL
Table 2 presents the correlations between HLS-14 and PAC-QoL scores. An increase in functional HL was significantly correlated with a lower total PAC-QoL score (r = −0.27, p < 0.001), given that lower PAC-QoL scores represent better QoL. In contrast, communicative and critical HLs were positively correlated with total PAC-QoL scores (r = 0.25, p < 0.001 and r = 0.36, p < 0.001, respectively), indicating poorer QoL at higher levels of communicative or critical HL. Consistent with Cohen’s conventions, 22 correlation coefficients in the range of approximately r = 0.2–0.3 are generally interpreted as weak-to-modest associations.
Correlations Among Health Literacy Scale-14 and Patient Assessment of Constipation Quality of Life Questionnaire Total and Subscale Scores (Spearman’s Method)

Note: Because higher PAC-QoL scores indicate poorer QoL, negative coefficients indicate better QoL with higher functional HL, whereas positive coefficients indicate poorer QoL with higher communicative or critical HL.
***p < 0.001.
Multivariable regression analysis
Table 3 presents the results of the multivariate OLS regression analyses of the total PAC-QoL scores. In the unadjusted model, functional (β = −1.63, 95% CI [−2.11, −1.16]) and critical (β = 2.06, 95% CI [1.31, 2.82]) HL subscales were significantly associated with the total PAC-QoL score. After adjusting for demographic characteristics, these associations remained statistically significant. In this model, sex (β = 7.28, 95% CI [3.13, 11.33]), part-time employment (β = 4.47, 95% CI [1.45, 7.64]), and age (β = −0.16, 95% CI [−0.31, −0.02]) were significantly associated with the PAC-QoL. In the fully adjusted models, which included clinical characteristics, functional and critical HLs remained significantly associated with PAC-QoL (β = −1.06, 95% CI [−1.53, −0.60]; β = 1.34, 95% CI [0.71, 1.94], respectively). In this model, CSS was significantly associated (β = 2.69, 95% CI [2.24, 3.13]), but age was not. The model fit improved from unadjusted to fully adjusted (R2 increased from 0.23 to 0.49). An increase in functional HL was significantly associated with lower total PAC-QoL scores, indicating a better QoL, whereas increases in critical HL, female sex, part-time employment, and greater severity of constipation were significantly associated with higher total PAC-QoL scores, indicating a worse QoL.
Multivariable Regression Models of Patient Assessment of Constipation Quality of Life Questionnaire with Bootstrap 95% Confidence Intervals

CI, confidence interval; R2, coefficient of determination; β, regression coefficient.
Subgroup analysis by sex
The results of the OLS regression stratified by sex are presented in Table 4. Overall, the associations between the HL subscales and PAC-QoL scores were generally consistent across males and females. Notably, the association with age was significant in females but not in males. Figure 1 presents a forest plot of the fully adjusted OLS regression for the total PAC-QoL, illustrating the estimates for the overall sample along with the sex-stratified estimates. Although females reported poorer PAC-QoL than males, no other variables showed clear sex-specific differences.
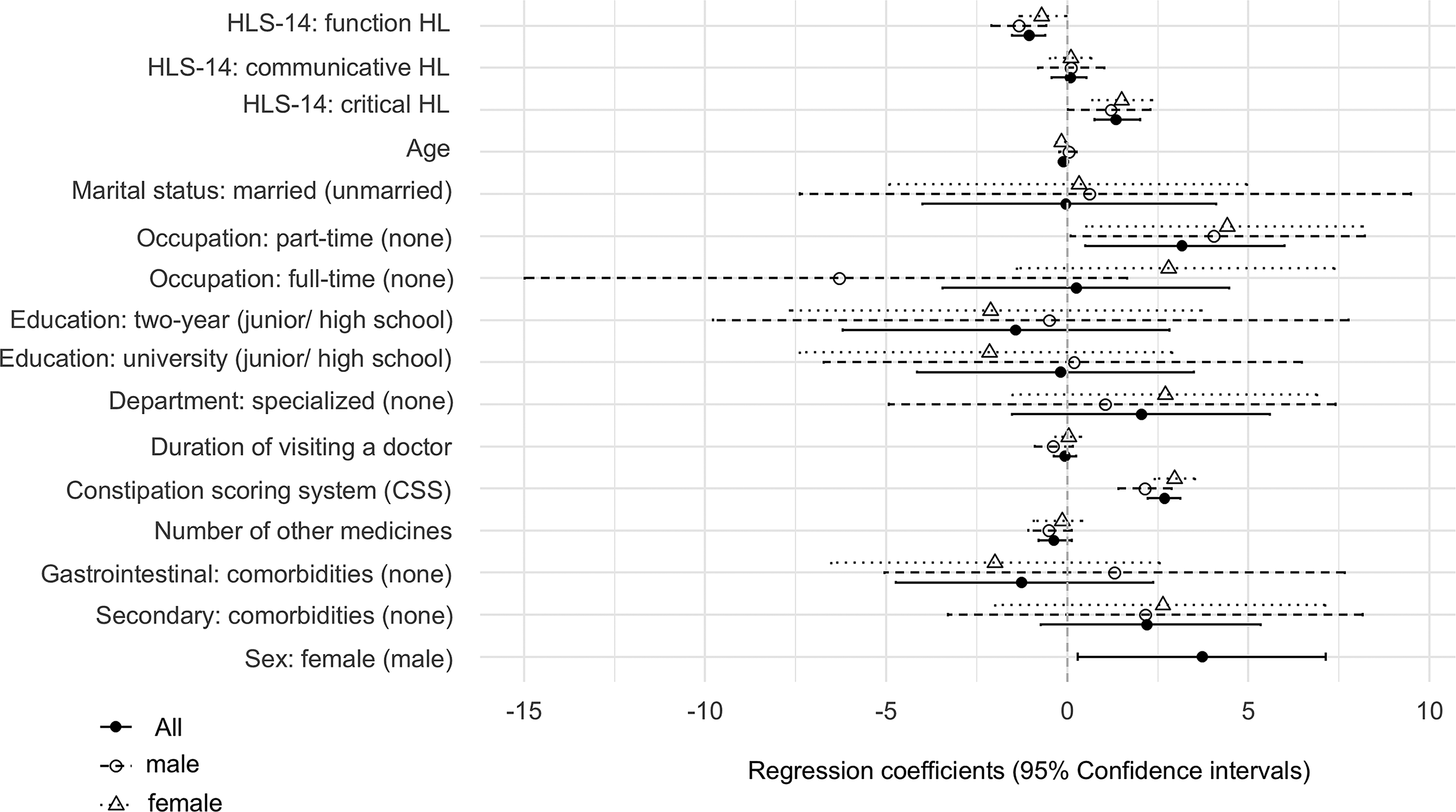
Forest plots of multivariable regression of fully adjusted models of PAC-QoL with bootstrap 95% confidence intervals in the overall sample and by sex. Estimates represent standardized regression coefficients (β) with bootstrap 95% confidence intervals. All participants are shown as solid circles (●), males as open circles (○), and females as triangles (△). CSS, constipation scoring system; HL, health literacy; HLS-14, Health Literacy Scale-14; PAC-QoL, Patient Assessment of Constipation Quality of Life Questionnaire.
Multivariable Regression Models of Patient Assessment of Constipation Quality of Life Questionnaire by Sex with Bootstrap 95% Confidence Intervals

Sensitivity analyses
Robust regression analyses yielded results consistent with the OLS regression (Supplementary Table S1), confirming that the findings were not driven by outliers or other influential observations. The magnitudes and directions of the coefficients remained stable across all methods.
Discussion
This study was conducted as an online cross-sectional survey to evaluate the association between HL and QoL in patients with CC and explore sex differences. Previous research using the HLS-14 scale in Japan reported mean scores of 50.3 for adults aged 30–69 years 17 and 43.9 for those aged 65 years or older. 23 In comparison, the mean score of 34.0 observed in the present study was lower than that reported previously, suggesting that patients with CC have poorer HL than do both the general adult population and older adults. Females had significantly higher total HLS-14 scores and functional HL than males, which is partially consistent with the findings of previous studies. A survey of the general population indicated that females tend to have higher HL than males, a difference attributed to their more frequent use of medical services and higher educational attainment. 24 In contrast, a study of patients with chronic kidney disease reported that males exhibited higher HL than females in domains such as comprehension of medical information and consultation skills. 25 These findings suggest that sex differences in HL may depend on disease context, the type of information considered, and other contextual factors.
In the present study, the mean total PAC-QoL score was 1.6 ± 0.8, which is comparable to that observed in a previous survey of Japanese patients with CC (1.6 ± 0.7). 21 A systematic review and meta-analysis of 12 studies comprising 1805 patients reported a pooled PAC-QoL score of 1.97 (95% CI: 1.70 − 2.24). 26 These findings indicate that Japanese patients with CC may experience slightly better disease-specific QoL than patients in other countries. Nevertheless, a substantial proportion of individuals with severe constipation in Japan rely on over-the-counter medications, highlighting the need for large-scale studies to validate the effectiveness and appropriateness of this practice. In the present study, females demonstrated significantly poorer QoL than males, supporting findings from previous research. 26 Specifically, females reported poorer QoL on the PAC-QoL subscales of psychosocial discomfort and worries/concern, indicating that the psychosocial impact of constipation may differ by sex.
An increase in functional HL is associated with an improvement in QoL. To the best of our knowledge, no previous study has explored the relationship between HL and disease-specific QoL in patients with CC. A systematic review and meta-analysis involving the general population and patients with other diseases identified a moderate positive correlation between functional HL and overall QoL. 10 Furthermore, a survey conducted among patients with lung cancer demonstrated a positive relationship between functional HL and disease-specific QoL, although no significant association was observed between functional HL and general QoL. 27 The authors suggest the need for interventions to enhance functional HL and provide guidance for self-care of the disease. In addition, a study conducted on patients with symptomatic heart failure reported an association between functional HL and disease-specific QoL. 28 This suggests that patients with adequate functional HL exhibit better symptom self-management and enhanced disease-specific QoL.
In contrast, critical HL status was negatively associated with QoL, which may be attributable to the fact that critical HL represents an advanced skill. Nutbeam described critical HL as an “advanced cognitive skill that can be applied to critically analyze information and use this information to exert greater control over life events and situations,” thereby distinguishing it from functional HL. 20 Because critical HL involves a high level of information appraisal and decision-making, individuals with greater critical HL may become more aware of inconsistencies in medical information or limitations in available treatments. Inadequate provision of information regarding constipation during medical consultations may have contributed to the observed negative association between critical HL and QoL. Indeed, patients with chronic idiopathic constipation and irritable bowel syndrome with constipation frequently report dissatisfaction with their medical care, 29 with approximately 54% perceiving their relationship with their doctors as negative. 30 Moreover, constipation may remain difficult to manage even in individuals with adequate functional HL, particularly when symptoms are persistent. Although the present study did not determine causality, it is also plausible that patients experiencing poorer QoL may actively seek more information to improve their condition, thereby developing higher levels of critical HL.
Females exhibited significantly poorer QoL than males; however, no significant sex differences were observed in the strength of the association between QoL and HL. Functional HL was significantly higher in females than in males. This finding suggests that factors other than HL should be considered when evaluating QoL in females. For instance, unstable mental status may have acted as a confounding factor. A study assessing QoL in patients with CC using the SF-36, a measure of general QoL, reported lower QoL among females, particularly in the mental health domain. 5 Moreover, in the present study, CSS scores were significantly higher in females than in males, consistent with previous reports that females experience more severe constipation symptoms. 31 Greater constipation severity has been associated with anxiety and depression. 32 These findings indicate that optimal intervention strategies may need to be sex-specific, thereby warranting further investigation.
Our study has several limitations. First, the cross-sectional design prevented the establishment of causal relationships. Second, selection bias cannot be overlooked because of the use of internet-based surveys. Although it is generally acknowledged that older adults tend to have lower HL, no significant age-related differences were observed in this study. Third, the choice of an internet survey aimed to ensure an adequate sample size of participants with CC; however, an objective diagnosis by a physician was not conducted. To enhance the reliability of subjective assessments, participation required meeting the Rome IV criteria, which allows for self-assessment and a history of hospital visits for at least 6 months. Future studies should include objective physician diagnoses to validate our findings. Finally, considering that relationship with health care providers is a critical determinant of HL, this study focused on patients with CC who were prescribed laxatives during outpatient visits. Consequently, the results may not be generalizable to individuals who do not attend outpatient clinics, necessitating future validation in a broader population.
Conclusion
We conducted an online survey to examine the relationship between HL status and QoL in patients with CC and to explore potential sex differences. The results indicated that functional HL was positively correlated with QoL, whereas critical HL was negatively correlated. Further research is required to confirm this association. Although females reported poorer QoL and greater disease severity than males, the strength of the association between HL and QoL did not differ significantly by sex. These findings suggest that efforts to improve the QoL of female patients should include educational interventions targeting functional HL, as well as comprehensive care addressing mental health needs.
Authors’ Contributions
H.T.: Conceptualization, data curation, formal analysis, writing, and original draft preparation. A.H.: Formal analysis, writing, review, and editing. D.K.: Writing, reviewing, and editing. S.K.: Supervision.
Footnotes
Acknowledgments
The authors would like to thank all the patients who participated in the survey. The authors thank Kohei Fujita (Fujita Medical Clinic) and Hiroko Sata for their support in generating items and modifying the scale.
Author Disclosure Statement
The authors have no conflicts of interest to disclose.
Funding Information
The authors declare that no funds, grants, or other support was received during the preparation of this article. No funding was received for conducting this study.
Data Availability
Datasets supporting the findings of this study are available from the corresponding author upon request. All authors of this study have access to all the data for the study that is ongoing.
Supplemental Material
Abbreviations
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.