
Abstract
Purpose:
The aims of this study were to (1) examine experiences of health care delivery and quality of care among women with hormonal mood disorders across the reproductive life course, and (2) investigate the associations of these factors with mental health status related to their hormonal mood disorder.
Methods:
Participants (467) with a self-reported diagnosis of premenstrual syndrome (PMS)/premenstrual dysphoric disorder (PMDD) or perimenopausal depression completed an online survey between June 2023 and September 2023. We performed a factor analysis to explore the underlying structure of items measuring perceptions of health care experiences. Descriptive statistics and logistic regression models were conducted to examine reported health care delivery and quality of care for hormonal mood disorders across the reproductive life course and associations with mental health status related to their hormonal mood disorder.
Results:
Nearly two-thirds of women with PMS/PMDD (62%) and over one in three with perimenopausal depression (41%) consulted more than one provider for medical help and underwent delays in diagnosis and treatment for more than one year (58% and 35%, respectively). Patients indicated negative health care experiences and quality of care across the reproductive life course. Among those, both patients with PMS/PMDD and patients with perimenopausal depression were almost three and four times more likely, respectively, to report fair/poor reproductive mental health outcomes.
Discussion:
This research offers insight into understanding reported deficiencies in health care delivery and quality of care for hormonal mood disorders and strategies for how to improve women’s mental health outcomes across the reproductive life course.
Introduction
Advancing research on women’s mental health across the reproductive life course is a priority to reduce women’s health inequities.1,2 Reproductive life course research investigates women’s health across the reproductive lifespan: in utero, puberty, the menstrual cycle, pregnancy and postpartum, and menopause. 3 Women are especially vulnerable to certain health problems during certain stages of the reproductive life course that are associated with reproductive hormones. The premenstrual phase and perimenopausal transition within the reproductive life course are linked with the onset of select hormonal mood disorders in women, specifically, premenstrual syndrome (PMS), premenstrual dysphoric disorder (PMDD), and perimenopausal depression. 4
These hormonal mood disorders are characterized by biological vulnerability and sensitivity to periods of hormonal instability and fluctuations. Women with moderate to severe symptoms experience marked depression, irritability, anxiety, loss of control, and even suicidality.4–8 Undiagnosed and untreated hormonal mood disorders can profoundly impact women’s quality of life by adversely affecting daily functioning, education, work, interpersonal relationships, and caregiving.5–7 PMS, PMDD, and perimenopausal depression represent a “continuum of vulnerability” based on both the sequential biological ages that they occur at and the many shared pathophysiological etiologies, symptomologies, and life impacts.4(p331)–8 Therefore, we applied a reproductive life course perspective and collectively considered these conditions in the study of health care delivery, quality of care, and relationships to hormonal mood disorder mental health outcomes.
Findings from previous research have indicated that women seeking care for premenstrual phase or perimenopausal transition hormonal mood disorders experienced deficiencies in the care of their conditions.9–12 It is unknown whether and how these patterns persist today, and if so, whether hormonal mood disorder mental health outcomes are affected. The aims of this study were to (1) examine perceptions of health care delivery and quality of care among women with hormonal mood disorders across the reproductive life course, and (2) investigate the associations of these factors with mental health status related to their hormonal mood disorder.
Materials and Methods
Sample and procedures
Participants were recruited using targeted online advertisements on social media sites by third-party partner research panels associated with Qualtrics. An incentive equivalent to $5 to 6 was offered to eligible participants to complete a survey. The anonymous survey was available online between June 2023 and September 2023. Eligible participants (1) resided in the US, (2) were assigned female sex at birth, and had a self-reported prior diagnosis of either (3a) PMS/Premenstrual Dysphoric Disorder and were between the ages of 18 and 45, or (3b) Perimenopausal Depression and were between the ages of 40 and 55. The study was approved by the Institutional Review Board, and participants provided informed consent.
Data collection and measures
We designed the survey instrument using existing survey questions that were adapted for the present study. Specifically, the survey items were based on the following: (a) a study on PMS diagnosis and treatment patterns conducted by Kraemer and Kraemer (1998); (b) the Patient Satisfaction Questionnaire III, originally developed and validated through the Medical Outcomes Studies; (c) research on measures designed to assess health care services consultation experiences and quality of care from the patients’ perspective; and (d) a scoping review indicating reliability and validity of a single self-rated mental health (SRMH) item in assessing mental health status.10,13–17 Researchers report significant relationships between single SRMH and mental disorders. SRMH is employed as a stand-alone indicator in small- and large-scale studies, the World Mental Health Composite International Diagnostic Interview, and national epidemiological surveys, including the Canadian Community Health Survey and Medical Expenditure Panel Survey. 17
The instrument collected basic demographics, including education, income, geographic location, and race/ethnicity. The specific survey items to collect data on health care delivery and quality of care are included in Table 1. Participants were asked to respond based on their perceptions of their overall experiences with the health care providers they had consulted for their hormonal mood disorder. Reliability of the survey was tested using Cronbach’s alpha, with a value of 0.88, indicating good reliability. Validity of the survey was confirmed by face assessment and content subject-matter expert review, and construct validity was established by factor analyses.
Survey Items
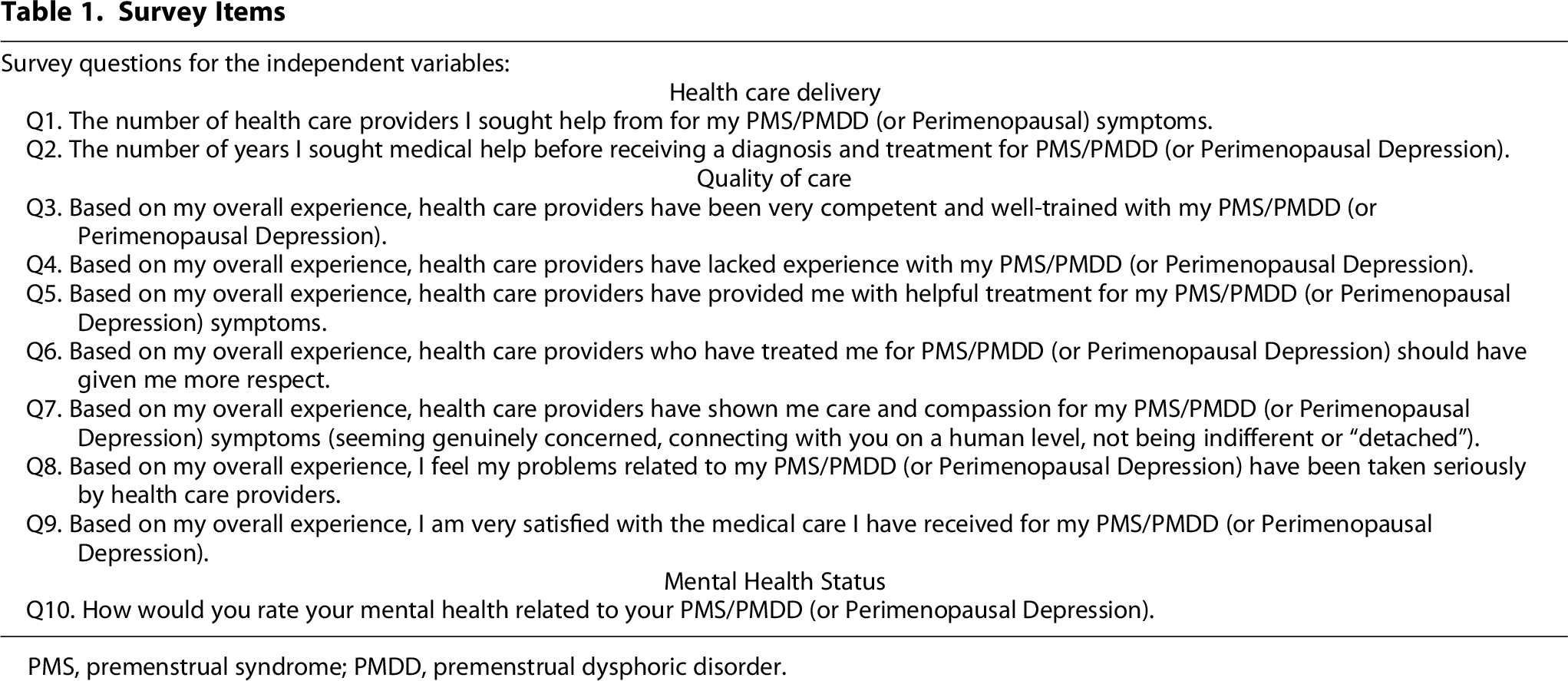
PMS, premenstrual syndrome; PMDD, premenstrual dysphoric disorder.
Responses to health care delivery questions Q1 and Q2 about number of providers consulted and time to diagnosis and treatment were dichotomized to maintain adequate sample size in all cells. The number of providers patients sought care from was measured as 1 provider through >7 or more providers and collapsed into a dichotomous variable (one provider (49.3%), > 1 provider (50.7%). Time to diagnosis and treatment for PMS/PMDD or perimenopausal depression was captured as time in years (<6 months through ≥6 years) and dichotomized for analysis as ≤1 year (54.2%) and > 1 year (45.8%). Quality of care was measured using seven items to capture perceptions of health care experiences (Q3–Q9) measured on a five-point Likert scale. For descriptive analysis, we collapsed the measures into strongly agree and somewhat agree and strongly disagree, somewhat disagree, and neutral, according to the method described by Joeng and Lee (2016). 18 Joeng and Lee (2016) reported that the five-point Likert scale (1 = strongly disagree, 2 = somewhat disagree, 3 = neutral, 4 = somewhat agree, 5 = strongly agree) can be collapsed into a dichotomous scale of 1 through 3 = disagree and 4 and 5 = agree, as shown by statistically significant empirical Bayes correlation coefficients. The dichotomous scale performs well compared with the five-point Likert scale, and such collapsing can replace the original scale in the analysis phase of a study. 18
Responses to Q4 and Q6 were reverse coded for analysis.
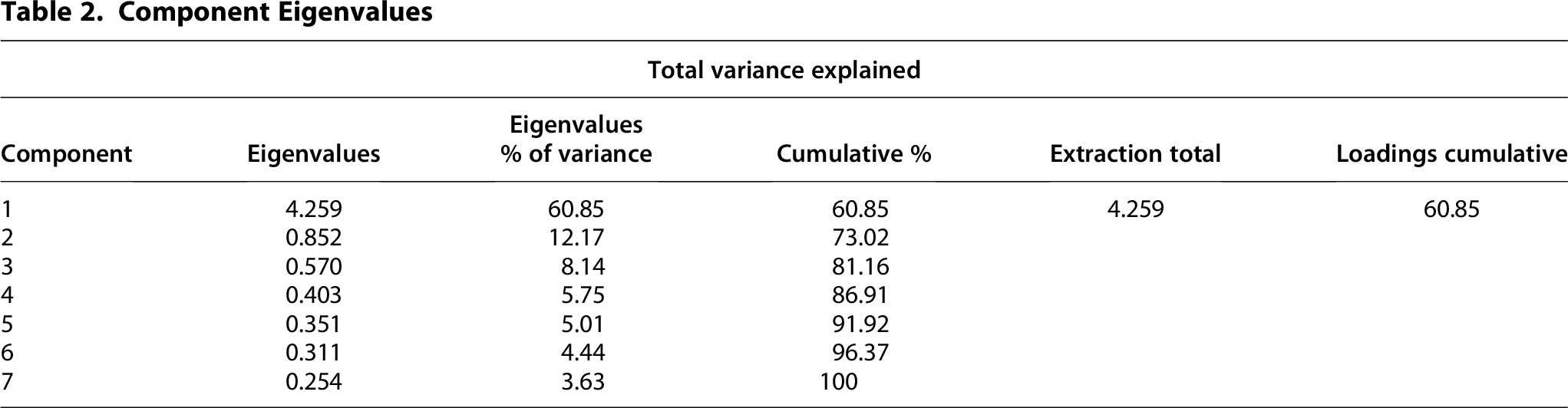
We performed an exploratory factor analysis on the survey items representing the study participants’ overall perceptions of their health care experiences (Q3–Q9). Following standard practice, factors with eigenvalues >1.0 were retained (Table 2). The independent items clustered around one main construct. The factor consisted of all items included in the factor analysis: provider competency and training, provider clinical experience, patient-perceived helpfulness of treatment, provider demonstrating care and compassion, provider taking patient problems related to their diagnosis seriously, provider showing respect to patient, and overall patient satisfaction. The reliability of the survey was tested using Cronbach’s α value, with a value of 0.88, indicating good reliability. The factor, labeled Overall Health Care Experiences, explained 60.8% of variance reported in patients’ overall perceptions of their health care experiences with providers consulted for their hormonal mood disorder. The median of the total factor analysis scores was used to create two categories, i.e., positive experiences vs negative experiences. The single item to measure hormonal mood disorder mental health status was dichotomized according to prior study approaches (excellent/very good/good vs fair/poor). 19
Component Eigenvalues
Statistical analysis
All statistical analyses were conducted using SPSS version 29 (IBM Corp, Armonk, NY). Descriptive data, reported as frequencies (%), were calculated for sample demographics and the independent variables. Forward selection was applied to test for potential covariates in regression models (age, race/ethnicity, education, income, state—US region) with an α value of 0.05 criterion to enter. Only two were associated with mental health status: racial/ethnic identities (p = 0.014) and income (p = 0.019). These two covariates were included in all adjusted logistic regression models.
We examined the associations of the number of providers and time to diagnosis with mental health status in adjusted binary regression models. We performed an adjusted logistic regression model to examine the association of overall health care experiences with hormonal mood disorder mental health status. Lastly, the relationship between overall health care experiences and hormonal mood disorder mental health status was investigated by diagnosis of PMS/PMDD and perimenopausal depression. In all adjusted regression models, the variable, positive experiences with health care providers, was used as the reference category for the independent variables, and excellent/very good/good mental health status related to their hormonal mood disorder was selected as the reference category for the outcome. An α value of 0.05 was applied to determine statistical significance. The effect size was reported as an odds ratio (OR) with a 95% confidence interval (CI).
Results
A total of 467 participants who were assigned female sex at birth and were diagnosed with PMS/ PMDD (n = 217) or Perimenopausal Depression (n = 250) completed the survey. The sample representation of race/ethnicity was 46% Nonwhite (n = 213) and 54% White (n = 254). The majority of respondents had low levels of education with a high school diploma or some college (53%), were low-to-middle income (78%), and were from the Southern region of the United States (52%) (Table 3). It is noteworthy that our sample was composed of a more diverse representation of the wider population of women diagnosed with PMS/PMDD and perimenopausal depression compared with prior studies examining these conditions.10–12,20
Sample Characteristics (n = 467)
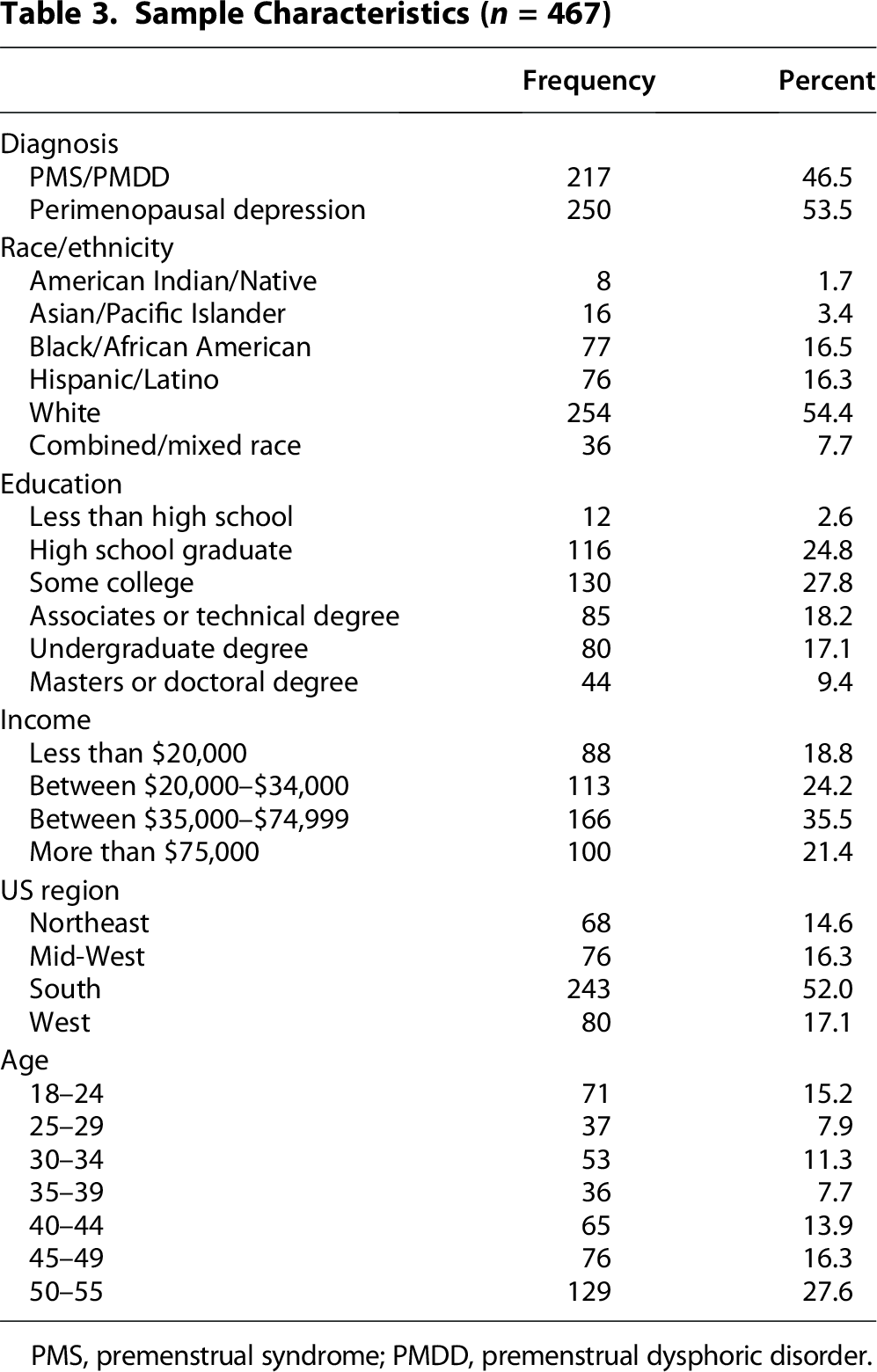
PMS, premenstrual syndrome; PMDD, premenstrual dysphoric disorder.
Health care delivery
The majority of patients with PMS/PMDD consulted with more than one provider (62%), and 58% experienced a delay in diagnosis and treatment for over one year. Forty-one percent of patients with perimenopausal depression consulted with more than one provider, and 35.5% had a delay in diagnosis and treatment for over one year.
Based on binary logistic regression and adjusting for race/ethnicity and income, the number of providers (OR 1.33, 95% CI 0.901–1.96, p = 0.152) and time to diagnosis and treatment (OR 1.27, 95% CI 0.857–1.88, p = 0.235) were not significantly related to hormonal mood disorder mental health outcomes (data not shown).
Quality of care
Approximately one in four patients with PMS/PMDD (25.3%) and perimenopausal depression (26.0%) did not agree that the health care providers they consulted for their condition were very competent and well-trained, nor did they offer helpful treatment (26.3% and 23.2%, respectively). Approximately half of patients diagnosed with PMS/PMDD and perimenopausal depression stated their providers lacked clinical experience in diagnosing and treating their condition (46.5% and 53.2%, respectively). Between 22% and 31% of women with PMS/PMDD and perimenopausal depression did not believe they were treated with care and compassion, nor were they taken seriously by their health care providers (27.7% and 21.6%, respectively). A majority stated they should have been treated with more respect (PMS/PMDD 72.8%, perimenopausal depression 56.8%). One in five patients with PMS/PMDD (20.7%) and perimenopausal depression (22.4%) were dissatisfied with their care.
A higher percent of women who perceived negative health care experiences compared with positive experiences reported fair/poor mental health status related to their condition (Table 4).
Frequencies of Patient Reported Hormonal Mood Disorder Mental Health Status by Positive/Negative Health Care Experiences

The factor, overall health care experiences, was significantly related to hormonal mood disorder mental health status. Patients who reported negative overall health care experiences with their health care providers were 2.98 times more likely to have poorer mental health related to their hormonal mood disorder compared with patients who had positive overall health care experiences with their health care providers (OR 2.98, 95% CI 1.99–4.44, p < 0.001) (Table 5).

Hormonal Mood Disorder Mental Health Status: Excellent/Very Good/Good (ref).
OR = Odds ratio, CI = Confidence Interval, p = p value.
Models control for race/ethnicity and income.
In examining the relationship between the factor overall health care experiences and mental health status by diagnosis, patients with PMS/PMDD who had negative overall health care experiences were 2.56 times more likely to report fair or poor mental health related to their condition compared with patients who had positive overall care experiences (OR 2.56, 95% CI 1.37–4.79, p = 0.003). Patients with perimenopausal depression who had negative overall health care experiences were also more likely to report fair or poor mental health related to their condition compared with patients who had positive overall health care experiences (OR 3.84, 95% CI 2.20–6.71, p < 0.001) (Table 6).
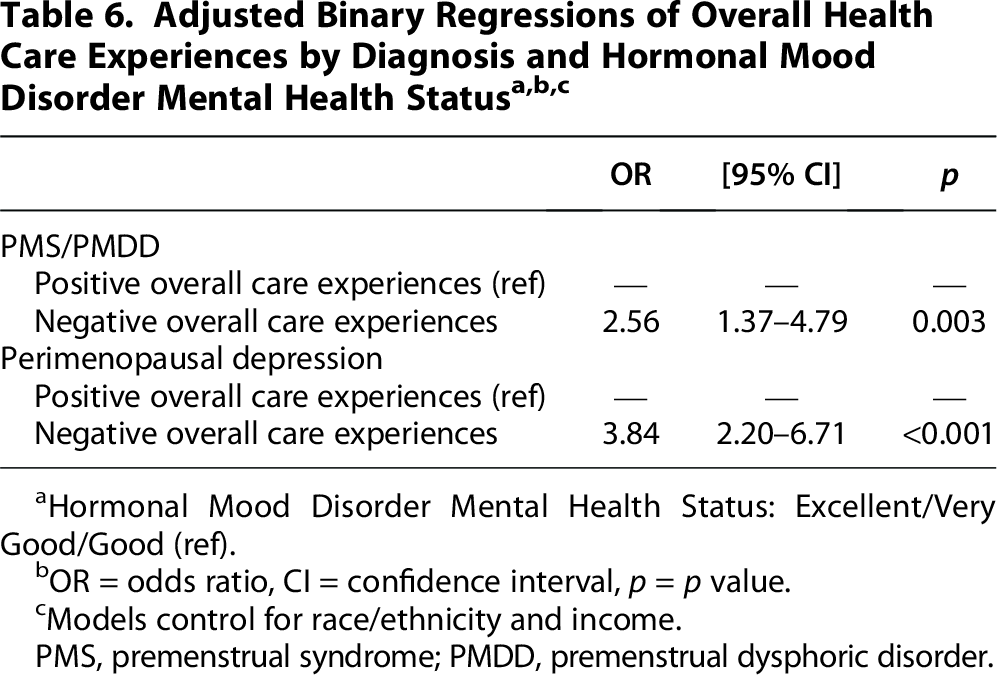
Hormonal Mood Disorder Mental Health Status: Excellent/Very Good/Good (ref).
OR = odds ratio, CI = confidence interval, p = p value.
Models control for race/ethnicity and income.
PMS, premenstrual syndrome; PMDD, premenstrual dysphoric disorder.
Discussion
Findings from this study advance our understanding of health care delivery and quality of care experienced by women with hormonal mood disorders across the reproductive life course and contribute to understanding how these factors are associated with mental health. A previous study indicated that patients who sought care between 1974 and 1994 experienced a delay in diagnosis and treatment of PMS: an average of 3.8 physicians were consulted over a period of 5.3 years. 10 Another study in 1986 similarly reported that most women sought care from multiple providers. 21 Our study aligns with previous research and indicates that the majority of patients with PMS/PMDD continue to experience a delay in diagnosis of over one year and consult more than one provider. We also found similar patterns for patients with perimenopausal depression. Our findings indicate that delays in diagnosis and treatment persist today, despite advances in research and medicine that collectively offer the opportunity to successfully care for women with these conditions.5,6,22–26 Our findings are supported by the World Health Organization’s statements that women who meet criteria for mental health disorders fail to be identified and diagnosed by their provider. 2 Unaddressed PMS/PMDD and perimenopausal depression may have substantial implications for patients seeking help. Importantly, these women may experience problematic sequelae such as high levels of distress and symptoms of depression, irritability, anxiety, loss of control, and even suicidality when left untreated over an extended time period during which women “may deteriorate irreparably.” 6 (p185)
In our study, we found that almost half of patients with PMS/PMDD and patients with perimenopausal depression perceived their health care providers as lacking experience in diagnosing and treating their condition. Some researchers have suggested that physicians may fail to effectively diagnose and treat moderate to severe PMS/PMDD due to insufficient awareness, training, and competency; however, the rationale for failure to diagnose and treat perimenopausal depression has not been previously considered. 11 Provider competency involves integration of evidence-based medicine in provision of care, health care provider expertise, and clinical experience that collectively support recovery of patients suffering from health conditions.27–30 Although gold-standard screening tools capturing PMS, PMDD, and perimenopausal depression exist, the extent of widespread adoption and standardized use across health care settings is unknown.31–33
Over 1 in 4 patients in our study reported that their providers did not offer helpful treatment for PMS or PMDD. Kraemer and Kraemer (1998) also reported that women with PMS perceived provider care as ineffective and overwhelmingly unsuccessful. 10 More recently, Kulkami (2018) reported that providers showed a lack of symptom recognition and provision of effective treatment in patients experiencing perimenopausal depression. 6 Prior research suggests an overall lack of adherence and/or consistency in the provision of therapeutic pharmacological management of PMS and PMDD according to medical consensus guidelines, while treatment patterns for perimenopausal depression have not been investigated. 34
Thirty to fifty years ago, patients with PMS reported that they were treated disrespectfully and were not taken seriously by their health care providers. 10 Our study indicates that this pattern continues today for women across the reproductive life course. More specifically, many patients with PMS/PMDD and perimenopausal depression did not believe they were taken seriously by the health care providers they had consulted, nor were they treated with respect. These findings are compatible with the Kaiser Family Foundation 2022 Women’s Health Survey that found 46% of young women reported negative interactions with providers and stated they dismissed their concerns, assumed something about them without asking, believed they were lying, blamed them for their health problems, or discriminated against them. 35 Gender bias that suggests women manifest a proneness to emotional symptoms is a widely recognized barrier to accurate diagnosis and treatment of mental disorders among women experiencing emotional distress. 2
Many patients with PMS/PMDD and perimenopausal depression were not satisfied with the care they received for their condition and reported adverse health care experiences with providers. Patient satisfaction is recognized as a central pillar in health care delivery and essential to achieving positive health outcomes, especially in mental health environments.36–39 Low satisfaction is associated with an increase in symptoms and poorer quality of life in patients with mental illness.38,40
We found that negative overall health care experiences with providers are associated with adverse hormonal mood disorder mental health. Both patients with PMS/PMDD and patients with perimenopausal depression were almost three to four times more likely to report fair/poor mental health related to their condition based on negative health care experiences with providers they consulted. Adverse hormonal mood disorder mental health can have profound consequences on quality of life by harmfully impacting daily functioning, education, work, interpersonal relationships, and care of others.5–7
Based on patient experiences, health care delivery is underserving women living with hormonal mood disorders, deficiencies are reported across the reproductive life course, and women’s mental health is adversely affected.
Limitations
It is possible that women who faced extreme barriers in health care services and adverse patient experiences remain undiagnosed and untreated for PMS/premenstrual dysphoric disorder and/or perimenopausal depression, and therefore, did not meet inclusion criteria for the study. Further, women who have had extreme experiences (either positive or negative) with health care services and quality of care may have been more likely to participate in the study and threaten internal validity by skewing the results in either direction. 41 To mitigate the potential for a negative skew, we offered an incentive to improve the quality of our research, according to a meta-analysis showing that monetary incentives increase overall response to electronic health surveys. 42 Collapsing the Likert scale with the neutral response in the negative experience group may have biased the results toward the negative direction, leading to potential misrepresentation of the data. This study also relied on self-reported diagnosis.
Implications for practice
Women who report deficiencies in health care delivery and quality of care for hormonal mood disorders across the reproductive life course are more likely to experience adverse mental health outcomes. Several measures can be adopted to address this issue. First, provider recognition of “reproductive life stage elements of health and wellbeing” is a cornerstone to reduce hormonal mental illnesses among women.43,44 It may be beneficial for health care providers to gain further understanding of women’s hormonal mood disorders through specialized medical training programs designed to focus on mental health conditions across the female reproductive life span. 45 This approach may also facilitate integrated treatment plans and care coordination between primary care providers, gynecologists and midwives, psychiatrists, and mental health professionals to improve hormonal mood disorder mental health through efficient and effective diagnosis, treatment, and follow-up. 46 Future studies may want to distinguish between PMDD and PMS and examine health care delivery and quality of care experiences and mental health outcomes separately. We also recommend further exploration into gender bias in medical care related to women’s hormonal mental health.2,35 It is essential to direct special attention toward creating positive experiences and person-centered sexual and reproductive health services that are empowering, supportive, compassionate, and respectful.47,48 Our study may serve to both inform future research and clinical practices by highlighting health care delivery and quality of care issues to address and advance women’s reproductive mental health.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.