
Abstract
Premenstrual dysphoric disorder (PMDD) is comprised of a cluster of affective, behavioral and somatic symptoms recurring monthly during the luteal phase of the menstrual cycle. The disorder affects 3–8% of menstruating women and represents the more severe and disabling end of the spectrum of premenstrual disorders, which includes premenstrual syndrome and premenstrual aggravation of underlying affective disorder. Rigorous and specific diagnostic criteria for PMDD were specified in the Diagnostic and Statistical Manual of Mental Disorders IV (1994) and reaffirmed in the Diagnostic and Statistical Manual of Mental Disorders V (2013) and, consequently, there has been a marked increase in well-designed, placebo-controlled studies evaluating treatment modalities. Although the exact pathogenesis of PMDD is still elusive, treatment of PMDD and severe premenstrual syndrome has centered on neuromodulation via serotonin reuptake inhibitor antidepressants, and ovulation suppression utilizing various contraceptive and hormonal preparations. Unlike the approach to the treatment of depression, serotonergic antidepressants need not be given daily, but can be effective when used cyclically, only in the luteal phase or even limited to the duration of the monthly symptoms. Less, well-substantiated alternative treatments, such as calcium supplementation, agnus castus (chasteberry),
Definition of premenstrual dysphoric disorder
Premenstrual complaints of a physical and emotional nature are common, affecting up to 90% of ovulatory women. Symptom onset can occur up to 2 weeks before menses and resolve soon after the onset of the menstrual period. A symptom-free interval after the end of the menstrual flow and before ovulation is required for the symptoms to be consistent with a premenstrual disorder (PMD) [1]. The most debilitating and severe symptoms are emotional and behavioral, and include irritability, depression, mood lability, anxiety, feelings of ‘loss of control’, difficulty concentrating and fatigue. Physical symptoms often include abdominal bloating, breast tenderness, headache and generalized aches [2,3].
The specific diagnosis of premenstrual dysphoric disorder (PMDD) was introduced by the American Psychiatric Association in Diagnostic and Statistical Manual of Mental Disorders (DSM)-IV (1994) [4], but remained in the appendix as it was believed that additional research was needed to confirm the distinctive-ness of the diagnosis from other disorders [5]. Most recently in the newly published DSM-V (2013), PMDD is no longer in the appendix, but is a full diagnostic category [6]. The diagnosis of PMDD requires at least five of the 11 specific premenstrual symptoms including one of the core mood symptoms (marked depression, anxiety or tension, mood swings or persistent anger and irritability; Box 1). Dysfunction in the home, social and occupational spheres related to the symptoms must be present for most menstrual cycles over the past year, and symptoms must be documented prospectively for at least two menstrual cycles to confirm the premenstrual timing of the symptoms and the postmenstrual symptom-free-interval [6]. The move to include PMDD as a full diagnostic category under mood disorders came after careful review of diagnostic stability in clinical and epidemiologic cohorts. The most potent predictive validator of PMDD as a distinct disorder is the preferential response to serotonergic antidepressants and to certain hormonal treatments [5].
The American College of Obstetricians and Gynecologists [7], the Royal College of Obstetricians and Gynecologists [8], and most recently the International Society for the Study of Premenstrual Disorders (ISPMD) [1], have published diagnostic criteria for PMDs. Specifically, the consensus of the members of the ISPMD was that both premenstrual syndrome (PMS) and PMDD fall under the umbrella of a ‘core PMD’. To be classified as a core PMD, the symptoms need not be specific in type or number, but must be severe enough to cause impairment, and must occur during ovulatory cycles and be absent between the end of menses and ovulation. The ISPMD identified variants of PMD that fall outside of the strict definitions of PMS and PMDD, but that may respond to similar treatment modalities [1]. These variants include: cyclic symptoms occurring without menstruation, such as after hysterectomy (with ovarian retention) or endometrial ablation; premenstrual exacerbation of an underlying psychological or somatic diagnosis; symptoms resulting from exogenous progestagen administration; or symptoms due to nonovulatory fluctuations in ovarian activity.
Diagnostic criteria for premenstrual dysphoric disorder.
Five (or more) of the following symptoms occurred during the week before menses and remitted a few days after the onset of menses. At least one of the symptoms being either 1, 2, 3 or 4:
Marked lability (e.g., mood swings, suddenly feeling sad or tearful, or increased sensitivity to rejection)
Marked irritability or anger
Markedly depressed mood
Marked anxiety and tension
Decreased interest in usual activities
Difficulty in concentration
Lethargy and marked lack of energy
Marked change in appetite (e.g., overeating or specific food cravings)
Hypersomnia or insomnia
Feeling overwhelmed or out of control
Physical symptoms (e.g., breast tenderness or swelling, joint or muscle pain, a sensation of ‘bloating’ and weight gain)
The symptoms interfere with work, school, usual social activities or relationships with others
The symptoms are not an exacerbation of the symptoms of another disorder (e.g., major depressive disorder, panic disorder, dysthymic disorder or a personality disorder)
Criteria A, B and C should be confirmed by prospective daily ratings during at least two consecutive cycles
The symptoms are not due to the direct physiologic effects of drugs of abuse, medications or an underlying medical disorder
Epidemiology
A total of 20–30% of women may be affected by moderate-to-severe symptoms that meet criteria for PMS, and 3–8% will fulfill the strict criteria for PMDD [9]. The prevalence of PMDD is not specific to geography, with similar reported estimates between 3–8% in countries such as India, Iceland, Germany and the USA [10]. Surprisingly, one study found that up to 18% of women lacked only one of the requisite symptoms for a PMDD classification, indicating that many women are ‘near threshold’ for the diagnosis [11]. It has been estimated that 20% of reproductive-aged women have debilitating symptoms causing significant impairment that warrant treatment [12] . Recent cross-sectional surveys undertaken in Europe, Latin America and Asia found that, of 7226 women studied, the most prevalent premenstrual symptoms were of the physical domain - abdominal bloating, irritability, mastalgia and joint/muscle/back pains [10]. However, this survey did not assess the prevalence of PMDD specifically. Certain sociodemographic factors were associated with decreased severity of symptoms such as age extremes (young and old), higher parity and nonsmoking. Although some countries, such as the UK, Brazil, Japan, Korea and Austrialia, were characterized by greater PMS severity, all the other countries did not differ from one another. The global database indicates that premenstrual and menstrual symptoms are not influenced by country or culture [10].
Women with PMDD manifest a 50–78% lifetime incidence of psychiatric disorders such as dysthymic disorder, major depressive disorder, seasonal affective disorder and generalized anxiety disorder [13–15]. The prevalence of the co-occurrence of PMDD with bipolar disorder or schizophrenia has not been established owing to the limited number of prospective studies. However, there are case reports and retrospective studies of women with schizophrenia, which suggests there may be an association [16]. Retrospective studies have noted increased prevalence of severe PMS in women with bipolar disorder [16]. Although PMDD and schizophrenia can co-occur, the premenstrual phase is not specifically a time of vulnerability for psychosis [16]. Case reports suggest that women can manifest premenstrual psychosis [17].
Burden of disease
PMS can have a negative impact on daily functioning at home, in the workplace and in social interactions [18–20]. Specifically, women with PMDD were found to have substantial impairment of productivity in the workplace and a higher rate of absenteeism [21,22]. They were also more likely to visit their physicians and incur higher healthcare costs [23,24]. The adverse effect of PMDD on health-related quality of life was found to be greater than chronic back pain, and comparable to debilitating conditions, such as osteoarthritis and rheumatoid arthritis [25]. The degree of impairment of interpersonal relationships during the late-luteal phase for women with PMDD was comparable to the levels experienced by women with chronic clinical depression [9]. Most concerning is that women suffering from PMDD were significantly more likely to report suicidal ideation than their counterparts without PMS [26,27]. Women menstruate up to 400–500 times over the course of their reproductive years, rendering the burden of illness for PMDD similar to that of dysthymic and depressive disorders [28].
Diagnosis
Crucial to the accurate diagnosis of PMDD is a complete history and accurate documentation of the timing of the symptoms in relation to the menstrual cycle.
The diagnosis of a PMD requires a consistent pattern of psychological, physical and/or behavioral symptoms that begin during the luteal phase, and that resolve completely during menses. The symptoms must be of moderate-to-severe intensity and result in some interference with, or impairment of, daily activities or functioning. Daily prospective charting for two menstrual cycles to accurately confirm the timing of the symptoms is required by all published criteria [1,6]. Retrospective recall of symptoms has low specificity and is considered unreliable [29]. Critical for the diagnosis is a symptom-free week early in the follicular phase, which differentiates a PMD from a psychiatric disorder (which lacks this regularly timed symptom-free interval) [30]. Charting of symptoms also allows clinicians to differentiate between mild PMS and moderate-to-severe PMS and PMDD, and can help exclude exacerbations of underlying psychological conditions [28] . There are several psychometric measures used clinically and in research studies. The Daily Record of Severity of Problems is a validated prospective daily rating scale, which allows women to track 11 symptoms across their menstrual cycle [31]. One retrospective tool, the Premenstrual Symptoms Screening Tool (PSST) has recently been validated as an excellent screener to determine who may benefit from more involved prospective daily recording of symptoms [32]. In practice, a simple rating scale can be devised by asking the patient to list (on a piece of paper or in a computer file) her five or more most significant symptoms vertically and the days of the month (1–31) across the top horizontally, and to circle the days of her menstrual flow. She can then rate the symptoms nightly on a scale from 0 ('none') to 3 ('severe') with 1 being ‘mild’ and 2 being ‘moderate’. Impairment of activities can be denoted by an asterix next to the disabling symptom.
A thorough medical history and physical examination can help to rule out any underlying medical disorders. Attention should also be given to ruling out medical conditions subject to premenstrual flare such as hypothyroidism, anemia, dysmenorrhea, irritable bowel syndrome, interstitial cystitis, endometriosis, chronic pelvic pain, chronic fatigue syndrome, connective tissue and rheumatologic disorders [33].
An understanding of the patient's social history is pertinent, with attention given to any incidents of domestic violence, physical or emotional trauma, or substance abuse, owing to the close association between PMS/PMDD with such a history [34,35]. Screening for psychiatric illnesses, such as dysthymic disorder, major depressive disorder, seasonal affective disorder and generalized anxiety disorder, should be undertaken if indicated, particularly if the daily ratings reveal follicular-phase symptoms suggesting that the PMS may be an exacerbation of an underlying disorder or in the presence of suicidal or homicidal ideation. Family history, past history of major depression and postpartum depression are risk factors for the development of PMDD and affective disorders [13–15].
Many women are not pleased with the request to delay treatment until after the completion of daily ratings, but will often comply when told that accurate diagnosis is important and not possible without the daily ratings. They should also be told that treatment may differ in nature or duration depending on the diagnosis. Recording symptoms and clarifying the relationship with the premenstrual phase can also give the patient a sense of control and help her to educate family members about the neuroendocrine nature of the disorder and, therefore, the patient may find the completion of the daily ratings to be therapeutic. Lifestyle changes that may be helpful to initiate during this time are addressed below and include dietary changes, exercise and relaxation strategies.
Pathophysiology
Fluctuations in ovarian sex steroids
The exact pathophysiology of PMDD is still unknown. The specific timing of the symptoms, triggered by ovulation, peaking in the late-luteal phase and resolving during menses, indicates that the fluctuations in gonadal sex steroids, particularly progesterone, are involved in the pathogenesis of PMDD. Symptoms of PMDD are absent premenarchally and, in nonovulatory cycles [36], disappear in ovariectomized women and those subjected to suppression of ovulation [37–39], and abate with menopause [40–42]. Women with premenstrual disorders also appear to have a differential sensitivity to exposure and/or withdrawal of circulating ovarian sex steroids. Schmidt
Allopregnanolone, pregnanolone & GABA
Investigators have also hypothesized that the metabolites of progesterone, which have been found to have neuroactive properties, might be implicated in the pathogenesis of PMD. Of particular interest are the neuroactive steroids, allopregnanolone or ALLO (3α-hydroxy-5α-pregnan-20-one) and pregnanolone (3α-hydroxy-5β-pregnane-20-one), which are metabolites of progesterone produced in the ovary, adrenal glands and brain [44]. Both ALLO and pregnanolone are positive modulators of the GABA neurotransmitter system in the brain. GABA is the main inhibitory neurotransmitter in the mammalian brain and is crucial for regulation of anxiety, vigilance, alertness, stress and seizures [45]. Some, but not all, studies have shown decreased peripheral ALLO during the luteal phase of affected women [46–48]. Given that this hormone readily crosses the blood–brain barrier, lower ALLO concentrations might result in decreased GABA-mediated neural inhibition [49]. Most clinical evidence and findings from animal models of progesterone withdrawal point to reduced functional sensitivity of the GABA receptor during the luteal phase in women with PMD [50,51]. It has been demonstrated in rats that exposure to progesterone changes the configuration of the GABA receptor, rendering it temporarily insensitive to further modulation by the neurosteroid metabolites of progesterone [52,53].
Serotonin
Important for understanding pharmacologic treatment of PMDD is the role of serotonin (5-HT, 5-hydroxytryptamine) in the pathophysiology of the disorder. Women with PMS/PMDD have been found to have abnormalities in their serotonergic transmission, with a lower density of serotonin transporter receptors [54]. PMDD symptoms can be provoked in susceptible women if tryptophan, the precursor of serotonin, is depleted [55], or if a serotonin antagonist is administered [56]. Peripheral serotonergic function has been shown to be altered during the luteal phase in women with PMS, with decreased platelet uptake of serotonin [57], decreased whole-blood serotonin [58] and decreased platelet monoamine oxidase activity [59]. Peripheral measures of serotonergic functioning are reasonable, since the platelet has similar uptake properties to the serotonergic neuron in the brain. However, a direct role for serotonin in PMDD was suggested by a PET study, which found that daily mood ratings of symptomatic women significantly correlated with changes in brain trapping of 11C-labeled 5-hydroxytryptophan in various brain regions across the menstrual cycle [60].
Cortical reactivity & startle response
Several studies have demonstrated that women with PMDD have altered cortical activity or physiologic arousal relative to healthy comparison patients. Smith
Brian neurocircuitry
Recent studies have indicated that the brain structure and function are altered in women with PMDD [65–67]. Ovarian steroids have been found to modulate activity in brain regions relevant to the symptoms of PMDD, including the prefrontal cortex, reward systems and stress neurocircuitry [68]. Baller
Pharmacologic treatment of PMDD
Pharmacologic therapy is usually indicated for women with severe PMDD. Lifestyle modifications, such as increasing aerobic exercise and dietary changes consisting of increased calcium intake, reduced caffeine intake and increased carbohydrate intake (premenstrually), are helpful for PMS, but usually fail to relieve symptoms of PMDD [69]. Evidence-based recommendations for pharmacologic intervention in the treatment of PMDD include serotonergic antidepressants or medications that suppress ovulation without reintroducing PMS-like symptoms [70]. Three selective serotonin reuptake inhibitors (SSRIs; fluoxetine, sertraline and paroxetine) have US FDA indications for the treatment of PMDD. In 2006, the FDA also approved an oral contraceptive (OC) that consists of 24 days of active pills followed by four placebo pills (24/4 regimen), comprised of a novel progestin, dropsirenone (3 mg) and a low dose of estrogen (20 mg of ethinyl estradiol) for the treatment of PMDD in women desiring contraception [71,72]. Serotonin norepinephrine reuptake inhibitors (SNRIs) have also shown efficacy in smaller studies [73]. Other medications that have demonstrated some utility in the treatment of PMS, but have not been studied specifically for PMDD, include GnRH agonists with low-dose estradiol and progestin add-back [74], the androgenic hormone danocrine [75], and high doses of transdermal estradiol with cyclic or intrauterine progestin for uterine protection [76].
Before starting any pharmacologic treatment, care should be taken to review any previous treatments. As PMDD affects reproductive-aged women, contraception and future plans for pregnancy must be discussed. In addition, a conversation should be held regarding management of side effects and possible teratogenicity if pregnancy should occur [74].
SSRIs, SNRIs & other serotonergic antidepressants
Serotonergic agents (SSRIs, SNRIs, atypical serotonergic antidepressants and serotonergic tricyclics) are considered to be effective treatments for PMDD. These agents alleviate symptoms in up to 60–80% of patients across multiple treatment trials and meta-analyses [77–81]. Unique to patients with PMDD is their rapid response to these serotonergic agents, usually within the first menstrual cycle and generally within 1–2 days. This quick response differs from the treatment of depressive or anxiety disorders, where an effect may take up to 3–4 weeks to appear [70]. The rapid response to therapy among PMDD patients has allowed for intermittent luteal-phase dosing, as well as intermittent symptom-onset dosing [69,82]. The choice of continuous versus intermittent dosing is generally tailored to the individual woman, taking into account symptoms, adverse effects, treatment response and patient preferences [71]. When SSRIs were first evaluated for the treatment of PMDD, they were utilized with continuous daily dosing, but more recent studies have evaluated intermittent, luteal-phase dosing, starting at approximately the estimated time of ovulation and continuing for 14 days per month (Table 1).
Serotonergic medications for the treatment of premenstrual dysphoric disorder: summary of randomized controlled trials.

Steiner et al. found no relief of premenstrual dysphoric disorder symptoms when lower doses of paroxetine (10 mg) were used [89].
Improvement in premenstrual dysphoric disorder symptoms; CR: Controlled release.
A responder typically experiences a >50% reduction in PMDD symptoms, with this response rate to treatment being considerably greater than the placebo response rate [70]. In practice, incomplete responses can be improved by combining an SSRI with another agent, such as the OC pill or an anxiolytic, to address persistent physical or psychologic symptoms, but there are no published studies of these approaches [71]. For example, persistent anxiety on a SSRI can be mitigated by switching SSRIs or adding an anxiolytic during the symptomatic days. Residual physical symptoms, such as pain or bloating, can be managed with particular OCs, analgesics or a mild diuretic, such as the potassium-sparing drug, spironolactone.
Effectiveness of SSRIs in treatment of PMDD
SSRIs are the treatment of choice for severe PMS and PMDD given there efficacy as well as tolerability (Table 1) [69]. They have been shown to improve both emotional and physical symptoms of PMDD and have also demonstrated a positive effect on social functioning [16,83,84]. SSRIs are also the most well-studied psychotropic treatment of PMDD, with several meta-analyses confirming their efficacy, the most recent in 2013 [77–80]. Nonserotonergic antidepressants are not effective for PMDD [69]. SSRIs are the only serotonergic medications the FDA has approved for the treatment of PMDD. The European Medicines Agency indicates that these drugs work, and certain SSRIs are approved in some countries, but neither intermittent nor continuous treatment is approved for use in the UK or continental Europe [74].
SSRIs: continuous versus luteal dosing
Although the most recent meta-analysis evaluating SSRIs in the treatment of PMDD found no difference in the effectiveness of continuous versus intermittent dosing, only three studies evaluating dosing regimens were included with substantial heterogeneity [77,85–87]. In the 2008 meta-analysis, Shah
SSRIs: symptom-onset dosing
Symptom-onset dosing is a newer method of psychotropic treatment of PMDD and entails women taking medication when symptoms begin, or a few days before expected symptoms, and stopping at the onset of menses, or within 3 days after the onset of menses [28]. The theory behind this type of dosing is that there is significant patient variability in the time-to-onset and -offset of PMDD symptoms, and by tailoring a patient's medication regimen to their own cycle can further aid treatment [91]. Recent studies evaluating this symptom-onset dosing have yielded promising results [82,92–94]. Specifically, Freeman
SSRIs dose-response studies
In the latest meta-analysis, there was consistent evidence that even low doses of SSRIs were effective, however, moderate doses were generally associated with larger effect size and a higher response rate [77]. Given the short onset of action of SSRIs, the onset of action should be expected during the first menstrual cycle of treatment. If no effect is seen, the dose may be increased in the next cycle if the patient is without negative side effects [95]. There is also evidence that a higher dose of a SSRI can be more effective in an intermittent dosing regimen. Eriksson
Side effects: SSRIs
Side effects are common with SSRIs, but usually abate after a few days of treatment. The most common side effect is nausea and, for those patients on intermittent treatment, symptoms do not usually return after starting a new cycle [86,90]. Other common side effects include headache, fatigue, diarrhea, dizziness and decreased libido or anorgasmia [95]. Sexual side effects, such as reduced libido and anorgasmia, are disturbing for some patients and can persist throughout treatment, thus affecting relationships [97,98] and resulting in noncompliance [99]. For patients particularly affected by sexual side effects, intermittent dosing is helpful as patients are asymptomatic in the drug-free period [100]. The addition of other medications, such as buspirone, sildenafil or bupropion, can also counter the sexual side effects of SSRIs [85].
As pregnancy might occur while women with PMDD are being treated with SSRIs and SNRIs, adequate counseling should be provided regarding the possible risks of fetal exposure to serotonergic neuromodulators. To date, there is no compelling evidence that one particular SSRI or SNRI is safer or more dangerous in pregnancy [101]. More data exist on older drugs, such a fluoxetine, which may be preferred by some physicians. Many studies have addressed a possible increased risk of persistent pulmonary hypertension in the newborn with SSRI use. Most recently, this link has been partly invalidated by two well-designed studies, one multicenter retrospective cohort and one case-controlled study, both of which eliminated any recall bias [102,103]. Furthermore, the early evidence connecting paroxetine use and cardiac malformations has not been confirmed by prospectively ascertained data from the largest number of paroxetine exposures [104]. There are limitations of the methodology and inconsistency of the findings in the published studies, suggesting that the question of safety of SSRIs in pregnancy remains unanswered until large prospective studies are conducted [105–107]. Of the SSRIs approved for treatment of PMDD, paroxetine is category D, suggesting proved human risk, while both fluoxetine and sertraline are category C, with less adverse risk. However, these categorizations may be outdated and are inconsistent with the latest data.
Serotonin norepinephrine reuptake inhibitors
SNRIs are less well studied, but have demonstrated success in treatment of PMDD. One randomized controlled trial (RCT) found that continuous dosing of venlafaxine was superior to placebo, with a response rate of 60% compared with 35% for placebo. Similar to treatment with SSRIs, treatment response was rapid with 80% of women experiencing symptom relief during their first treatment cycle [73]. However, in an open-label study using venlafaxine in intermittent dosing, there were flu-like symptoms after abruptly stopping venlafaxine [108]. Recently, two open-label studies reported improved symptoms of PMDD with continuous dosing of duloxetine 60 mg daily, but these results need to be replicated in RCTs [109,110].
Other CNS-acting drugs: anxiolytics
There is some reported success with anxiolytics in women with PMDD. Specifically, if a patient's symptoms are predominantly anxiety/tension and/or irritability, anxiolytics might be a good second-line therapy. While some studies have demonstrated a benefit with luteal-phase treatment with alprazolam, others do not show success [111–114]. Anxiolytics are not first-line therapy as they have sedating properties in addition to the potential for abuse. Current recommendations are for benzodiazepine treatment only in the luteal phase to avoid abuse [95].
Buspirone is a 5-HT-1 partial agonist used for generalized anxiety disorder, which has demonstrated some success in the treatment of PMDD [115–117]. Buspirone might be a helpful second drug for patients who suffer from decreased libido/anorgasmia with SSRIs, or even as a solo agent, given its low sexual side-effect profile. The response rate of anxiolytics is still below that of the first-line psychopharmacologic treatment, SSRIs.
Hormonal therapy
The goal of hormonal therapy in the treatment of PMDD is to suppress the hypothalamic–pituitary–gonadal axis and control sex steroid fluctuations in the luteal phase when patients are symptomatic. Different strategies have been tested for suppression of ovulation with: OCs, high-dose estrogen patches; GnRH agonists; danazol (a synthetic partial androgen); and surgical menopause with bilateral salpingo-oophorectomy (Table 2).
Ovulation suppression for treatment of premenstrual dysphoric disorder: summary of randomized controlled trials.
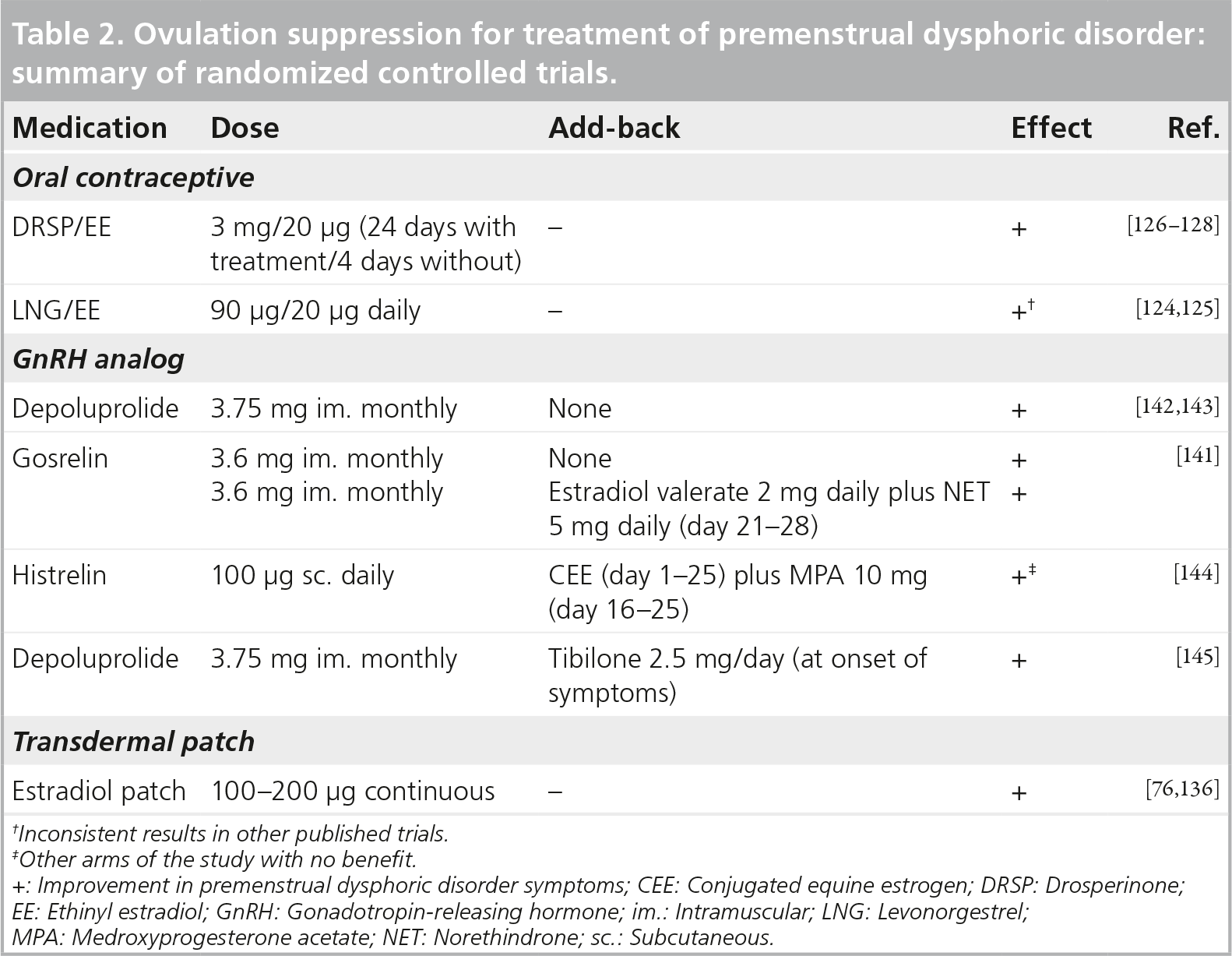
Inconsistent results in other published trials.
Other arms of the study with no benefit.
Improvement in premenstrual dysphoric disorder symptoms; CEE: Conjugated equine estrogen; DRSP: Drosperinone; EE: Ethinyl estradiol; GnRH: Gonadotropin-releasing hormone; im.: Intramuscular; LNG: Levonorgestrel; MPA: Medroxyprogesterone acetate; NET: Norethindrone; sc.: Subcutaneous.
Oral contraceptives
Although OCs are widely used for the treatment of the physical symptoms of PMS, they are generally ineffective in the treatment of PMDD [70,118]. Placebo-controlled trials have been scarce, and historically have had limited success in the treatment of PMDD or PMS [119,120]. In an epidemiologic study of women taking a variety of OCs, 12.3% of patients reported an improvement in mood and 71.4% reported no change in mood after starting OCs [121].
The dosing regimen and progestin formulation of OCs impact the potential reduction of PMDD symptoms. Bäckström
The traditional ‘21/7’ OC regimens allow for continued endogenous hormonal fluctuation, which can mimic some of the physical symptoms of PMS [122]. Patients with PMDD report more symptoms during hormone-free days, suggesting that OCs with fewer hormone-free days are more effective [122,123]. Those OC formulations with 24 active pills and 4 placebo days have demonstrated a more complete suppression of folliculogenesis, but this does not in itself explain the improved symptom relief in PMDD patients [122]. Furthermore, Halbreich
One novel OC comprised 3-mg drospirenone/20-mg ethinyl estradiol 24/4, showed a 50% decrease in PMDD symptoms in 48% of women ingesting active drug versus 36% in placebo [126]. In a crossover trial, Pearlstein
In theory, the success with this formulation lies in drospirenone, which binds to aldosterone and androgen receptors, potentially decreasing the somatic symptoms of bloating and breast tenderness, as well as acne and, perhaps, aggression/irritability. Spironolactone also has antial-dosterone properties and has been shown to relieve symptoms of PMS, notably breast pain and bloating [130,131].
There has been recent investigation into venous thromboembolism (VTE) occurrence with drosperinone-containing contraceptives. VTE risk is highest during the first months of pill usage. Given the usage of drosperinone in a noncontraceptive manner, these OCs are preferentially prescribed to women who are new to OCs and with a higher risk of VTE. An FDA review is currently ongoing, but the FDA labeling suggests an approximately 1.5-fold increased risk of blood clots for users of drosperinone-containing contraceptives, which is comparable to other progestins such as desogestrel and norgestimate [201]. To put this risk into perspective, the risk of developing deep vein thrombosis in women using drosperinone OCs is ten women in 10,000 compared with six women in 10,000 using other hormonal OCs [132,201]. This increased risk of VTE with drosperinone-containing OCs has not been confirmed in large observational studies or clinical trials. In fact, a large postmarketing observational study of over 50,000 European women did not find that women taking drosperinone-containing OCs had a higher risk of adverse cardiovascular events or VTE occurrence [133]. Furthermore, a recent meta-analysis found that all OCs conferred the same increased risk of VTE, except for levonorgestrel-containing OCs [134]. The epidemiologic studies prompting the FDA's warning have been criticized for failing to adjust for history of OC use, family history of thromboembolic events and BMI [135]. Although the verdict is still out whether drosperinone-containing OCs further increase the risks of VTEs, individualized risk assessment should be performed in all patients to identify women with increased risk, due to age, family history, BMI, hypertension and smoking.
High-dose transdermal estrogen
High doses of exogenous estrogen can also suppress the hypothalamic–pituitary–gonadal axis and thereby block ovulation. Two RCTs found women suffering from severe PMS had symptom improvement using 100–200-mg daily doses through a transdermal patch [76,136]. Given the risk of endometrial hyperplasia with unopposed estrogen, patients were given either norethisterone for 7 days per month or a levonorgesterol-containing intrauterine device [76,136]. The intrauterine device containing levornorgestrol is preferable in women with PMDD as systemic progesterone can cause PMS-like symptoms. Furthermore, the transdermal route of 100 μg of estrogen has a lower risk of VTE than equivalent doses given orally [137].
Danazol
Danazol is a synthetic partial androgen antagonist/agonist and gonadotropin inhibitor that also prevents PMS symptoms when dosed to inhibit ovulation. Unfortunately, its ungainly side effects of acne, hirsutism and possible teratogenicity make this an unpopular first-line drug [28]. Sarno
GnRH agonists
GnRH agonism successfully suppresses ovulation by downregulating pituitary gonadotropin secretion and, ultimately, eliminating pulsatile luteinizing hormone and follicle-stimulating hormone secretion. Three RCTs using GnRH analogs have demonstrated improved physical, emotional and behavioral symptoms in women with severe PMS [141–143]. Interestingly, women with severe premenstrual depression had no improvement of symptoms, suggesting that women with depressive symptoms might be adversely affected by the hypoestrogenic milieu created by GnRH analogs [143]. To bypass the ‘medical menopause’ created by GnRH analogs, low-dose estrogen or tibolone (an agent with estrogenic, androgenic and progestogenic effects) can be administered to decrease the negative impact of estrogen deficiency on mood and vasomotor symptoms. In addition, as there is an increased risk of osteoporosis and coronary artery disease with the hypoestrogenic state afforded by GnRH agonist therapy, tibolone or estradiol add-back therapy can potentially limit the deleterious effects of hypoestrogenism on bone and cardiac health [141,144–146]. Leather
Surgical menopause
Removal of bilateral ovaries with or without a hysterectomy is a last-resort measure. When more conservative treatments have failed, surgical menopause can be considered for women with severe, debilitating PMDD [37–39]. After bilateral salpingo-oophorectomy, it is important to replace estrogen until the age of natural menopause to prevent complications of premature menopause, such as osteoporosis and cardiac disease [146]. If the uterus is retained after bilateral salpingo-oophorectomy, progesterone is required to prevent endometrial hyperplasia, which may reintroduce PMS symptoms; therefore, the addition of hysterectomy is preferable. Prior to hysterectomy and oophrectomy, a 3 −6 month trial of a GnRH agonist with estrogen replacement alone is prudent to predict treatment response to surgery and to ensure estrogen replacement is well tolerated, since the long-term effects of estrogen deficiency are of grave concern [147].
Nonpharmacologic & complementary & alternative strategies
Dietary modification
Dietary changes during the luteal phase may result in symptomatic relief for PMS, although no diet modifications have been systematically evaluated, especially for PMDD [69,148]. It is thought that caffeine, sugar and alcohol intake may increase PMS symptoms [28,149]. Increasing complex carbohydrate intake premenstrually has been shown to improve mood, carbohydrate craving and memory in PMS, by potentially i ncreasing tryptophan, a precursor to serotonin [150].
Calcium/vitamin B6
Calcium is one dietary supplement that has the most evidence for the treatment of PMS, although it has not been studied for PMDD specifically [95,151]. Calcium supplementation is thought to regulate calcium homeostasis, specifically as it fluctuates during the menstrual cycle. Furthermore, hypocalcemia has been associated with affective disturbances similar to symptoms of PMD [152]. In two RCTs, calcium supplementation (1200 mg/day in divided doses) was found to manage PMS symptoms, such as mood and physical complaints [152,153].
The effect of vitamin B6 supplementation is more equivocal, with no studies for PMDD and only a few studies finding marginal reduction in symptoms [154]. Caution should be taken in doses >100 mg of vitamin B6, which can cause peripheral neuropathy [69].
Herbal treatments: agnus castus (chasteberry) & Hypericum perforatum (St John's wort)
Agnus castus (chasteberry) has demonstrated promise in the treatment of PMDD. A RCT of chasteberry found superior benefit compared with placebo, with emotional as well as somatic symptoms [155]. Some data find the response rate to chasteberry to be equivalent to that of fluoxetine [156].
Cognitive-behavior therapy, relaxation response & acupuncture
Cognitive–behavior therapy (CBT) is a type of psychotherapy where negative or maladaptive cognitive experiences or thoughts are identified and corrected, promoting behavioral change [161]. Specifically, CBT may include modification of irrational behavior and coping strategies. Reviews of RCTs on CBT for the treatment of PMS and PMDD show weak superiority when compared with placebo [162,163], and only one has evaluated CBT in women with PMDD [163]. CBT has proven to be a successful adjunct to SSRI therapy. When CBT alone was compared with SSRI alone, or in combination, all CBT groups demonstrated significant improvement in PMS symptoms after 6 months of treatment. Furthermore, those treatment arms exposed to CBT had superior long-term improvement [161].
Acupuncture, Qi therapy, reflexology, massage, krill oil, lavender oil, Chinese herbs or transmagnetic stimulation may help symptoms, but these treatments should only be offered after adequate evidence exists [95].
Exercise
It is commonly thought that exercise improves premenstrual symptoms through elevation of β-endorphin levels; however, there is little evidence to confirm this, with only one small RCT conducted [164]. Daley commented on the paucity in literature regarding exercise and reduction of PMSs. In the four interventional studies reviewed, Daley found that women reported reduction in PMS symptomatology after exercise [165]. The American College of Obstetricians and Gynecologists recommends exercise for PMS, but further studies are needed to substantiate this recommendation [7].
Alteration of sleep & circadian rhythm: bright-light therapy & sleep deprivation
There is evidence that women with PMDD have altered biological rhythms of body temperature and melatonin secretion [166]. Specifically, women with PMDD have decreased melatonin secretion similar to patients with major depressive disorder, suggesting a phase advance of circadian rhythms. Sleep deprivation has been proposed to correct the altered circadian rhythms of women with PMDD by affecting the sleep–wake cycle. Studies have found that sleep deprivation increases total sleep time, rapid eye movement sleep and improvement of mood in women with PMDD [166–168]. Bright-light therapy has been very promising in alleviating symptoms of PMDD. Parry
Conclusion
To date, the most effective treatment of PMDD has been neuromodulation through SSRIs. Numerous well-designed trials have elucidated an improvement in PMDD symptoms with serotonergic modulation in women with the disease. For those women in whom symptoms of irritability, depressed mood, lability and anxiety predominate, SSRIs are the first-line therapy.
Although the goal of hormonal treatment is to suppress the gonadal steroid cyclicity that triggers symptoms of PMDD, most OCs have had inconsistent results in alleviating symptoms. Drospirenone-containing OCs have shown efficacy in reducing PMDD symptoms, as well as improving loss of productivity and impairment of social relationships, and are also considered a first-line therapy. High-dose transdermal estrogen and cyclic or intrauterine progestin are also useful as first- or second-line therapy. Although GnRH agonism has also demonstrated success in the treatment of PMS, it is a third-line therapy and should include add-back therapy given the negative sequelae of the hypoestrogenic state on the bone and heart in premenopausal women.
Nonpharmacologic treatments have demonstrated less improvement in the treatment of PMDD compared with SSRIs or suppression of ovulation. These treatments are rarely studied in a rigorous manner, making the evidence for their use less substantial. Calcium supplementation has demonstrated the most promise in treating PMS. Chasteberry has also demonstrated success compared with placebo in the alleviation of symptoms. Potential benefits may exist from behavioral modifications, such as a change in diet, stress reduction and exercise. There is substantial evidence that bright-light therapy and sleep deprivation can reset altered circadian rhythms and alleviate symptoms in women with PMDD. CBT is also probably efficacious and may have an additive effect with SSRI therapy, but this needs to be studied more meticulously.
In the treatment of women suffering from PMDD, care must be taken to optimize symptom relief without incurring debilitating side effects. Since women with PMDD are of reproductive age, contraception should also be discussed and a knowledge of current fertility desires must be ascertained.
Moving PMDD to a distinct mood disorder in the DSM-V could lead to a more rigorous characterization of women participating in clinical trials and research studies, focusing on pathophysiology and treatment [5]. As we continue to learn more about this disorder, treatment will probably become more effective and specific to PMDD.
Future perspective
The treatment of PMDD is hindered by incomplete knowledge regarding its neurobiological basis. PMDD is clearly linked to the physiologic process of ovulation and the ensuing dynamics of the luteal phase of the menstrual cycle. Furthermore, there is ample evidence documenting the role of the serotonergic system in the pathophysiology of this disorder [172]. SSRIs are a first-line therapy for PMDD, with 60–80% of women considered as ‘responders’, experiencing at least a 50% decrease in their symptoms; however, after subtracting the percentage of women who respond to placebo in the RCTs, the percentage of women who actually respond to a drug is closer to 50% [173], and 30–40% of women with PMDD do not completely respond to pharmacologic treatment with serotonergic agents. A similar calculation can be made for the other first-line treatment approach, an OC formulation containing 3 mg of dropsirenone and 20 μg of ethinyl estradiol in a 24/4 regimen. The rise and fall of endogenous sex steroids can be prevented with a continuous intake of an OC, but surprisingly, even when the exogenous steroid concentration is stable, maintained by a constant dose of a monophasic preparation of a synthetic estrogen and a progestin, symptoms are not reliably and invariably improved [124].
This conundrum has yet to be resolved and highlights the fact that there is still much to be learned about the effect of estrogens and progestagens on the brain and on behavior. Further study of estrogen and progesterone activity on intracellular and membrane hormone receptors across the menstrual cycle in women with and without PMDD, may shed light on the differential response to fluctuating sex steroids in PMDD. Discoveries related to neuroendocrine modulation of the menstrual cycle, or the role of polymorphisms in hormone receptors or neurotransmitters will have therapeutic ramifications for treatments with novel selective estrogen or progesterone receptor modulators, or other neuroactive compounds [174,175].
The symptoms, including profound irritability, affective irritability, depressed mood, anxiety, impulsive behavior, and cognitive and sleep disturbances, place PMDD within the spectrum of affective illness. Considerable evidence has indicated that PMDD is not just a variant of depression and anxiety disorder, and that information on the diagnosis, treatment and validation of PMDD is adequate for its qualification as a full category in the DSM-V [5]. The timing, nature of the most commonly reported symptoms, heritability estimates, lack of shared genetic and environmental variance and a distinct therapeutic response profile all separate PMDD from affective or anxiety disorders [5,176].
A recent review stated that “neuroimaging studies are in their infancy with regard to revealing the neurocircuitry and neurochemistry of PMDD” and highlighted the need for biological research on PMDD to identify effective therapies [5]. A possible hypothesis that we are currently testing is whether the core affective symptoms of PMDD reflect a luteal phase-related deficit in emotion regulation. Further studies assessing neural circuitry will hopefully yield knowledge about the neural basis of emotion control and dysregulation in PMDD. Although effects of the menstrual cycle on neural responses to emotion provocation have been noted in healthy women [176,177], cycle effects on emotion regulation or its neural substrates have not been well studied in women with PMDD. Positive results would identify defective emotion regulation and the relevant circuits as therapeutic targets, and would provide biomarkers and a platform for the evaluation of new treatments for PMDD.
In the future, with the goal to improve therapeutic outcome, the identification of endophenotypes for PMDD may allow for the development of personalized pharmacologic therapy based on pharmogenetic data. Endophenotypes are created by separating the behavioral symptoms of PMDD into distinct phenotypes with definite genetic connections. In the treatment of various psychiatric disorders, the combination of neuroimaging, neuroendocrinology and genetic studies shows promise in the search for successful personalized therapy based on genome types and biomarkers. For example, in the case of major depressive disorders, genetic variants have been identified that are associated with different presentations of depression and with response to antidepressant drugs. Neuroimaging studies have also demonstrated that these genetic variants affect emotional processing, and are associated with changes in activity in brain regions that have been implicated in major depression and with specific antidepressant drug responses. It has been suggested that the neural alterations seen in major depressive disorder might be reflected in the serum, and could potentially be useful biomarkers for depression. Studies have investigated genetic variants affecting the CYP450 isoenzyme system (which have an effect on antidepressant metabolism), the serotonin transporter gene, and alterations in enzymes that are important in the degradation of monoamines (e.g., serotonin), inflammatory cytokines and neurotrophic factors [178,179].
Executive summary
Diagnosis of premenstrual dysphoric disorder (PMDD) requires a pattern of psychologic, physical and/or behavioral symptoms that begin during the luteal phase and resolve completely during menses.
While 20–30% of women will be affected by moderate-to-severe symptoms meeting criteria of premenstrual syndrome, 3–8% will meet the criteria for PMDD delineated by the Diagnostic and Statistical Manual of Mental Disorders V.
Women with PMDD have a 50–78% lifetime incidence of other psychiatric disorders.
Given symptom onset triggered by ovulation, it has been established that fluctuations in sex steroids are involved in the pathogenesis of PMDD.
The GABA neurotransmitter system is believed to be altered in women with PMDD, with altered functional sensitivity of the GABAAreceptor.
Lowered serotonin activity is etiologic to PMDD, given the relevant research and specific response to serotonergic agents.
Brain neurocircuitry may be altered in women with PMDD, with recent studies indicating abnormal brain activation in the dorsolateral prefrontal cortex and cerebellum compared with healthy controls.
The US FDA has approved three selective serotonin reuptake inhibitors (SSRIs) for the treatment of PMDD (fluoxetine, sertraline and paroxetine), and each have demonstrated improvement of PMDD symptoms in several randomized controlled trials.
Continuous dosing and luteal phase dosing of serotonergic drugs have been found to be equally effective in alleviating symptoms.
Efficacy is generally demonstrated at the lower end of the recommended SSRI dosing.
Second-line treatment or treatment of residual anxiety after SSRI therapy includes luteal phase administration of anxiolytics, such as buspirone and benzodiazepines. Long-term benzodiazepine use can exacerbate depression.
Oral contraceptives (OCs) with standard dosing regimen of 21 days of treatment with 7 hormone-free days have not been shown to be effective in the treatment of PMDD.
OCs given in a continuous daily regimen with no hormone-free days have demonstrated possible success in PMDD treatment.
OCs containing dropsirenone and 20 μg of ethinyl estradiol in a 24/4 dosing schedule are approved by the FDA for the treatment of PMDD in women who are also seeking contraception. These OCs demonstrated alleviation of PMDD symptoms in several randomized controlled trials and meta-analyses.
High-dose transdermal estrogen blocks ovulation and improves PMDD symptoms, but requires a progestin to protect the endometrium.
Danazol, a synthetic partial androgen antagonist/agonist, and gonadotropin inhibitor can relieve PMDD symptoms, but has unwanted side effects of hirsutism and acne, and can virilize a fetus if conception occurs during therapy.
GnRH agonists are a third-line therapy that should be used with add-back estrogen and progestin therapy to alleviate negative health consequences of hypoestrogensim.
Surgical menopause should be a last resort for young women and used only in very limited situations.
Calcium has improved symptoms in women suffering from premenstrual syndrome and may help women with PMDD.
Bright-light therapy can be effective for PMDD.
Chasteberry has been found in small studies to have superior benefit when compared with placebo, with emotional and somatic symptoms of PMDD.
Behavior modifications, such as diet, exercise and relaxation techniques, have proven successful in treatment of PMS, but have not been studied rigorously for PMDD.
Congnitive-behaviour therapy has been found to have modest improvement in PMDD symptoms, but may be more effective as an adjunct to serotonergic therapy in women suffering from behavioral symptoms of PMDD.
Future targeted treatments should focus on the estimated 30–40% of women suffering from PMDD that do not respond to, or who can not tolerate, current pharmacologic and or behavioral treatments.
Study of neuroendocrine modulation of the menstrual cycle, with attention to ovarian steroid activity on membrane and intracellular hormone and other neurotransmitter receptors, could lead to novel therapeutic targets.
Research on the neural circuitry in women with PMDD can yield knowledge about the neural basis of emotional control and dysregulation in PMDD, which can potentially lead to targeted treatments if significant pathology is found.
The search for endophenotypes in PMDD, by separating the behavioral symptoms of PMDD into distinct phenotypes with definite genetic connections, might guide personalized and targeted pharmacologic therapy.
This approach has not yet been explored adequately for PMDD. One relevant investigation that demonstrated the potential of this approach investigated phenotypic profiles related to stress and pain in women with history of PMDD and major depressive disorder [14]. Biomarkers related to the sympathetic nervous system, hypothalamic–pituitary axis and pain showed, not only unique phenotypic differences, but also important common features. Women with PMDD, with or without a history of major depressive disorder, demonstrated blunted stress reactivity compared with control women when assessing biomarkers related to sympathetic nervous system activation. However, there was no evidence for heightened sensitivity to experimental pain in women with PMDD after controlling for a history of major depressive disorder [180].
Thus far, serotonin-related phenotypes, such as variation in the serotonin transporter gene [181] and in the transcription factor AP-2 β, have not been found in women with PMDD [182]. Success in this area will help clarify the etiology of the symptoms of PMDD, and provide biomarkers for assessing behavioral and pharmacological interventions to ameliorate this disorder.
Financial & competing interests disclosure