
Abstract
Background:
We developed the Engaging Peer Mentors for Opportunity, Well-Being, and Equity Realization (EMPOWER) program to provide leadership training and peer mentoring in a virtual, scalable format. Designed to be widely accessible to women leaders in academic medicine, it combined an asynchronous online curriculum with 1 hour per month group meetings via teleconference with peers and a faculty advisor. This qualitative study assessed the program’s feasibility and impact as well as identified areas for quality improvement.
Methods:
We conducted individual interviews with 34 program participants as well as focus groups with 14 faculty advisors. These were conducted virtually at the program midpoint and following program completion. The Framework Method informed qualitative analysis.
Results:
Beneficial program outcomes included knowledge acquisition/skill development, new or different ways of thinking, a sense of empowerment/self-confidence, and the clarification of personal values/goals. Monthly, 1-hour peer meetings appeared to further facilitate learning and practical application. Barriers included a lack of time to complete didactic activities and to attend group meetings, limitations of an online/virtual format, individual circumstances, and idiosyncratic group dynamics. Recommendations to improve quality and establish best practices included clear communication of well-defined aims/expectations, tailored programming, efficient use of time, minimization of labor/mental load, and enhanced online community-building.
Conclusions:
The benefits program participants and their faculty advisors described reinforce the value of gender-aware leadership development programs, especially those that include peer mentoring. By enhancing accessibility, engagement, and flexibility, programs such as EMPOWER can become more inclusive and effective, ensuring that all promising leaders can thrive in academic medicine.
Introduction
Gender disparities persist in academic medicine. Although the number of women holding leadership roles has grown, structural barriers remain, including persistent salary disparities, 1 sexual harassment, 2 gendered stereotype threats, 3 and more limited advancement opportunities for women compared with their male counterparts. These challenges hinder women’s career progression and perpetuate the underrepresentation of women in all leadership roles,3–5 which in turn, makes it unlikely for institutions to cultivate an inclusive and supportive culture for women in academic medicine. 5
Organizations advocating for women in science have identified mentorship, sponsorship, and leadership support as key priorities to address the challenges women continue to face in academic medicine, helping them navigate the complexities of career advancement. 4 Providing structural leadership development programs and effective mentorship for women can potentially and significantly enhance job satisfaction, career advancement, and productivity.6–8 However, one of the persistent barriers to women’s career progression in academic medicine is the lack of senior women mentors who can serve as role models.7,9 In response, peer mentoring10–12 has emerged as an alternative model that provides both career and socioemotional support.
When structured thoughtfully and implemented within a safe and supportive environment, peer mentoring can help women build the confidence, networks, and strategies to overcome gendered challenges. 11 Beyond mentorship, sponsorship 3 is particularly crucial for advancing women’s careers, as it increases visibility and facilitates access to leadership opportunities. The Hedwig van Ameringen Executive Leadership in Academic Medicine (ELAM®) program is a well-established national initiative to address the need for sponsorship and has played a significant role in advancing gender equity in academic medicine. ELAM® 8,13 offers an in-depth, experiential curriculum that focuses on essential leadership competencies while incorporating facilitated peer mentoring to promote reflection, collaboration, and inspiration. The program has led to notable successes, with alumnae securing high-profile leadership roles, including dean-level positions, and increased research productivity through grants and publications. However, despite its effectiveness, ELAM® has limitations, including restricted scalability and limited reach, as each institution can nominate only a small number of participants; further, the program requires frequent in-person participation, which may not be feasible for all candidates.
Recognizing the need for a more accessible and scalable solution, we developed the Engaging Peer Mentors for Opportunity, Well-Being, and Equity Realization (EMPOWER) program, 14 drawing inspiration from ELAM® while adapting its principles to a fully virtual format. EMPOWER aims to provide fundamental leadership training and facilitated peer mentoring in a way that is more widely accessible to women in academic medicine. A detailed description of the year-long EMPOWER program’s structure and curricular content is reported elsewhere. 14 In brief, the key learning areas EMPOWER addresses are leadership effectiveness, negotiation, strategic career advancement (including sponsorship and self-promotion), and work–life integration. The curriculum features content specifically tailored toward the experiences of women faculty in academic medicine. This includes readings and media presenting on issues related to gender, culture, bias, hierarchical structures, and/or power dynamics that might influence how a woman establishes her leadership style,15–17 approaches negotiations,18,19 or strategizes career networking, sponsorship, and self-promotion,20,21 for example.
An invitation to participate in a pilot of the EMPOWER program was extended to a cohort of women medical faculty in academic positions who had received National Institutes of Health K08 or K23 career development awards from 2006 to 2009, as identified through our prior survey studies. 2 Program participants accessed curricular materials through an online learning platform and met virtually for 1 hour per month with their peer mentorship circles to engage in discussion and collective learning. Each circle was composed of up to six peer members as well as a faculty advisor who facilitated and served as a source of senior guidance and support. Peer circles were composed of members in the same or adjacent time zones, but from different institutions and varying specialties, to facilitate scheduling and ensure confidentiality, respectively. All peer members and their faculty advisors were women, and all faculty advisors were recruited from a list of alumni of the ELAM® program. The peer circle was meant as a forum in which participants could further engage with their peers and faculty advisor on the curricular content as well as topics that are particularly salient to them, including the gendered leadership barriers they might currently have been facing. Moreover, the group discussions and interactive exercises facilitated the sharing of new ideas and differential experiences among peers, allowing for the opportunity to challenge dominant paradigms within academic medicine and their own institutions as well as brainstorm alternative approaches to what constitutes leadership, worthwhile aspirations, and success.
In this qualitative study, we evaluated perceptions of and experiences with EMPOWER by conducting in-depth interviews with participants and their faculty advisors at both program midpoint and after program completion to assess implementation challenges and troubleshoot problems in real time, as well as capture final reflections. By examining their insights, we assessed the EMPOWER program’s feasibility and impact as well as identified areas for quality improvement to optimize this leadership development intervention for women in academic medicine.
Methods
The Institutional Review Board of the University of Michigan Medical School approved this qualitative assessment as part of a randomized trial to evaluate the impact of the EMPOWER intervention. 14 All participants were provided with the required informed consent information and agreed to take part in the study. Documentation of informed consent was waived because the research was considered no more than minimal risk. This qualitative study gained insights into EMPOWER’s feasibility, optimization, and scalability through in-depth, semi-structured, one-on-one interviews with program participants as well as focus groups with their peer circle faculty advisors.
Interviews and focus group guides were developed to assess experiences with and impressions of the program, including perceived benefits and barriers to participation as well as thoughts on how to optimize program implementation. Interviews and focus groups were conducted at the program midpoint (February–May 2023) and after completion (November 2023–February 2024), virtually via teleconference by two senior analysts (R.D.J. and Y.L.). The audio recordings were transcribed by professional transcriptionists.
Interviews were conducted with a sample of 34 out of the 89 program participants. Using a purposeful sampling strategy to maximize the diversity and range of viewpoints (e.g., racial identity and program engagement),22,23 a participant from each of the 16 peer circles was selected for an interview at each time point. If there was no response to an invitation after sending a reminder, another participant was selected. In total, 54 individuals were invited to interview. Of the 54 invited, 20 did not accept the invitation, whereas 34 accepted and completed the interview. Each interview participant only received one invitation and completed one interview at either the midpoint or end of the program, resulting in at least one person per peer circle at each time point (17 at the mid-point and 17 at the end). Interviewee characteristics are presented in Table 1. The length of the interviews ranged from 20 to 60 minutes, with an average length of 37 minutes.
Participant Characteristics
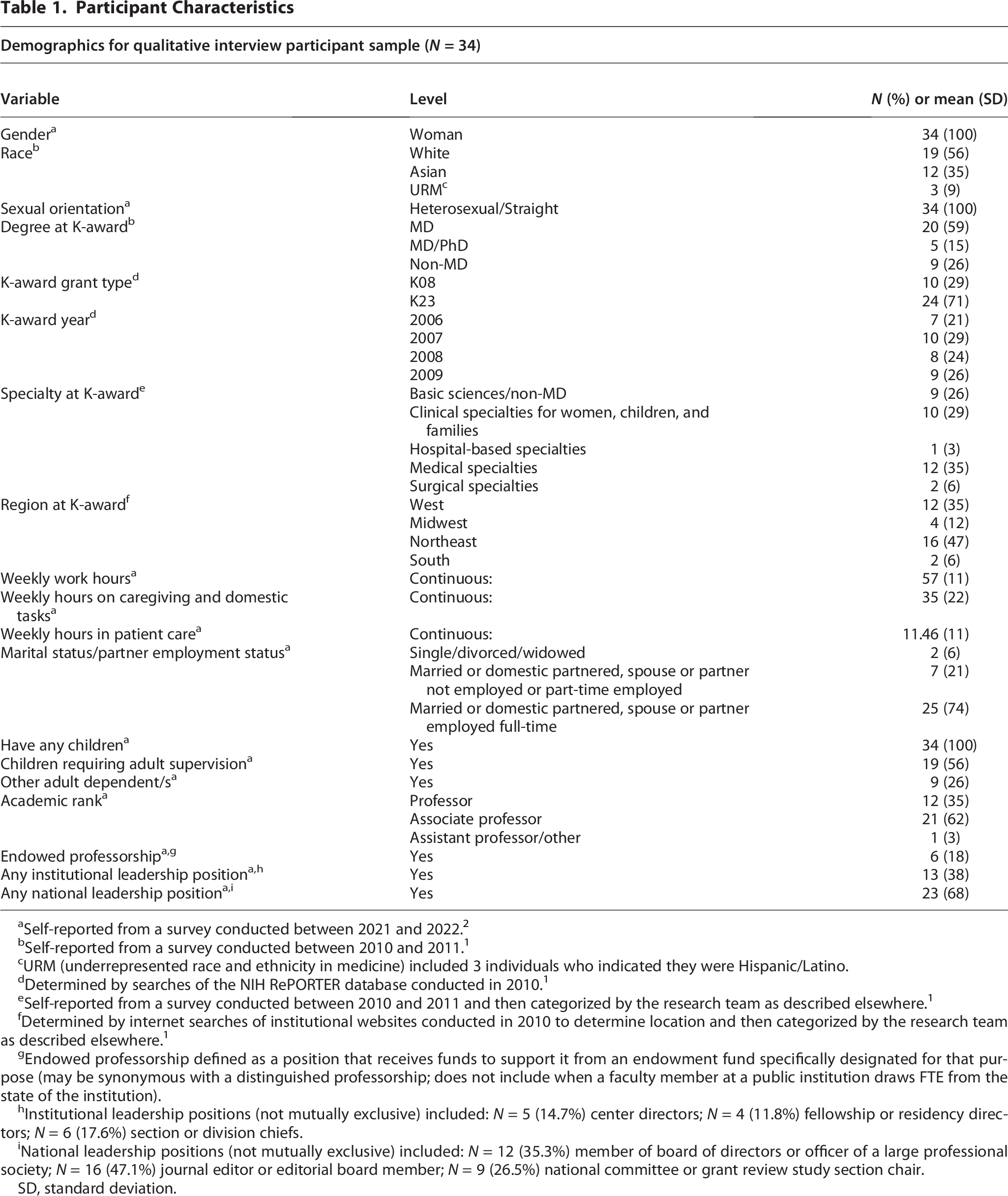
Self-reported from a survey conducted between 2021 and 2022. 2
Self-reported from a survey conducted between 2010 and 2011. 1
URM (underrepresented race and ethnicity in medicine) included 3 individuals who indicated they were Hispanic/Latino.
Determined by searches of the NIH RePORTER database conducted in 2010. 1
Self-reported from a survey conducted between 2010 and 2011 and then categorized by the research team as described elsewhere. 1
Determined by internet searches of institutional websites conducted in 2010 to determine location and then categorized by the research team as described elsewhere. 1
Endowed professorship defined as a position that receives funds to support it from an endowment fund specifically designated for that purpose (may be synonymous with a distinguished professorship; does not include when a faculty member at a public institution draws FTE from the state of the institution).
Institutional leadership positions (not mutually exclusive) included: N = 5 (14.7%) center directors; N = 4 (11.8%) fellowship or residency directors; N = 6 (17.6%) section or division chiefs.
National leadership positions (not mutually exclusive) included: N = 12 (35.3%) member of board of directors or officer of a large professional society; N = 16 (47.1%) journal editor or editorial board member; N = 9 (26.5%) national committee or grant review study section chair.
SD, standard deviation.
All 16 peer circle faculty advisors were invited to participate in the focus groups. Those who responded to the invitation were assigned to a focus group based on overlapping schedules and availability. Seven focus groups were convened in total, with 14 out of the 16 faculty advisors participating in at least one focus group and with 9 able to participate at both time points. The length of the focus groups ranged from 37 to 57 minutes, with an average length of 50 minutes.
The Framework Method informed qualitative analysis of the transcripts. 24 The first analysis phase involved an initial review of the transcripts and multiple iterations of inductive, open coding to allow unexpected concepts to emerge. During this process, 21 transcripts (14 one-on-one interviews and all 7 focus groups) were independently coded by at least two members of the research team. The team would then regularly meet to compare codes, resolve discrepancies, and reach consensus on definitions. The agreed-upon codes were then organized into categories, resulting in a codebook reflecting a working analytical framework. All transcripts were then divided between the two senior analysts (R.D.J. and Y.L.), who each systematically applied the working analytical framework using MAXQDA, 25 a qualitative data analysis software. After all coding was complete, the applied codes from each transcript were further reviewed by a different analyst and summarized in grid tables with associated excerpts for additional review. Thematic saturation26,27 was reached when no new codes or new themes emerged, indicating the breadth and depth of insights had been captured. Throughout the analytic process, the research team repeatedly discussed and reevaluated their impressions and interpretations of the data until consensus was reached on finalized themes.
Results
We present the results of our qualitative analysis, organized into four themes: (1) impressions surrounding EMPOWER program components and the leadership development process/learning cycle, (2) beneficial EMPOWER program learning and professional development outcomes, (3) barriers to EMPOWER program participation, engagement, and commitment, and (4) recommendations to improve EMPOWER program quality and best practices. Exemplar quotes are presented either within the text or in Tables 2 and 3 (denoted in the text as Q and numbered sequentially).
Perceived Beneficial Outcomes in EMPOWER Program Learning and Professional Development

EMPOWER, Engaging Peer Mentors for Opportunity, Well-Being, and Equity Realization.
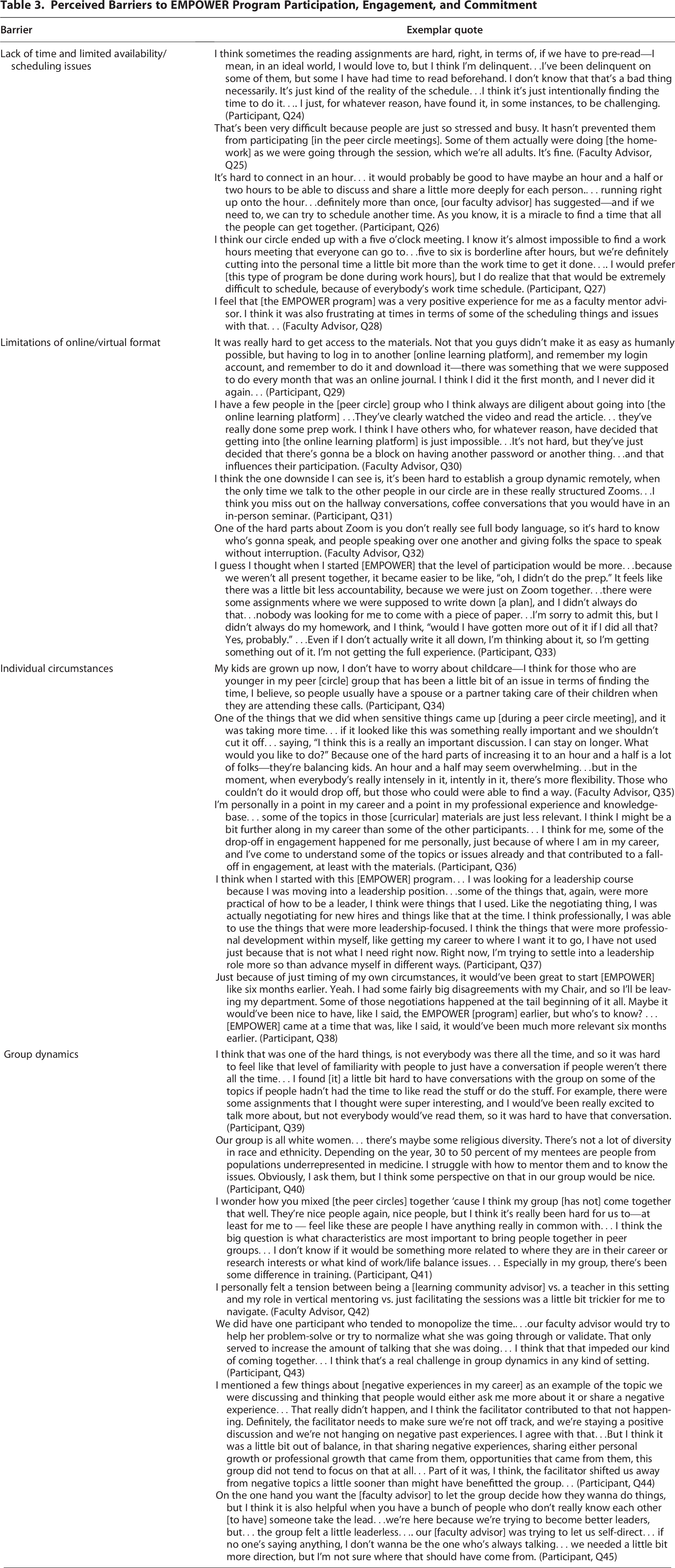
Perceived Barriers to EMPOWER Program Participation, Engagement, and Commitment
Impressions of EMPOWER program components and the leadership development process/learning cycle
Many participants found the online curriculum informative and perceived that the virtual peer circle further facilitated learning and application of knowledge. Peer circle interactions were seen as opportunities for further review of the curricular subject matter as well as additional discussions on salient topics related to career and work–life experiences that, while extending beyond the intended curriculum, were important to participants. These peer exchanges were often described as including elements of reflection, problem-solving, experience sharing, and gathering of feedback as well as receipt of social support and encouragement. This characterization is consistent with the EMPOWER leadership development process and learning cycle, which is the reinforcement of the online curriculum through virtual peer circle interactions (Fig. 1A).

EMPOWER learning cycle and perceived beneficial outcomes. The EMPOWER leadership development process and learning cycle involve the reinforcement of the online curriculum through virtual peer circle interactions
I thought it was—throughout the entire program—it was excellent. I really felt like it was a safe space. They were amazing, inspiring women. I learned a lot from them in how we tried out the material, how we reported back on things, other struggles that had tangential relationship to the EMPOWER curriculum….I just really felt like everyone went out of their way to provide support, and suggestions, and help, and empathy to all of the members of the peer mentoring group. (Participant)
I think that over the course of the year, I think we really helped one another….[The EMPOWER participants] were really incredibly thoughtful in how they helped one another address many of the challenges that they were encountering. They were able to tie the homeworks and the readings into what they were going through and how they might use it. I thought that was actually incredibly powerful. (Faculty Advisor)
Beneficial EMPOWER program learning and professional development outcomes
Perceived beneficial program outcomes were organized into two types of learning and professional development (Fig. 1B). The first reflects content and conceptual learning, including knowledge acquisition, skill development, and new or different ways of thinking. The second involves the practical application of the acquired knowledge, skills, and thought processes to real-life situations at participants’ home institutions, such as exerting influence, making decisions, or pursuing career goals and milestones. This practical application was often associated with the development of participants’ sense of empowerment and self-confidence, as well as the clarification of their values and goals.
Knowledge acquisition/skill development
Many participants described the EMPOWER learning modules as featuring new or alternative information (especially exploration of subject matter that they might not have pursued on their own), structured content that complements, supplements, or reinforces prior learning, and a curricular framework featuring thoughtfully curated content that can be practically applied (Table 2; Q1, Q2).
In addition, many participants noted that the peer circle further increased the extent of their knowledge acquisition and skill development by providing them the opportunity to review curricular topics and practice skills with peers in an interactive setting (Q3, Q4). The discussions with peers also helped contextualize the subject matter in ways that reflected their real-life experiences, especially the challenges unique to women in academic medicine (Q4, Q5). Several participants reported receiving knowledge and feedback, as well as practical suggestions and actionable strategies, for navigating career challenges based on their peers’ experiences, viewpoints, and perspectives beyond their local institution (Q3, Q5).
Different ways of thinking
Participants often commented that they benefited from curricular materials and exercises that introduced them to new or different ways of thinking conceptually about their careers. These included alternative understandings of leadership, a broader perspective when thinking about one’s career path, deeper self-reflection on professional development, and different approaches toward dealing with issues and problem-solving (Q6, Q7, Q8).
Participants reported that the opportunity to meet other women leaders in their peer circle further solidified an alternative outlook on women in leadership (Q9, Q10). Some found that the peer circle discussions often stimulated brainstorming surrounding novel approaches to commonly held challenges in academic medicine and/or facilitated more objective self-reflection (Q9, Q10). Faculty advisors observed that participants were able to compare how commonly held issues were handled at different institutions and gain a wider perspective based on multiple seemingly unbiased viewpoints (Q11, Q12).
Empowerment/self-confidence
Participants reported feeling a sense of empowerment and self-assurance backed by their newly acquired knowledge, skills, and thought processes (Q13). They described improved morale and feeling validated as well as increased leadership self-confidence, especially in terms of being women leaders (Q14, Q15). Some detailed feeling further empowered to start implementing their skills in real-life situations to exert influence and/or pursue action at their own institutions (Q15).
Participants reported receiving social support and validation from their peers when they struggled with self-doubt or external barriers, which would help them persist and advance (Q16). The peer circle also provided a forum where participants could further bolster their sense of resilience through peer discussions on how to assess challenges and identify solutions (Q17). Peers also offered each other much needed encouragement when taking the next steps to pursue goals, achieve new milestones, or choose an alternative path (Q18).
Clarification of values and goals
Participants mentioned that the curricular materials and exercises helped them identify and clarify their ideal career and life goals, while also bolstering their self-assurance about their personal values and choices (Q19). For some, this led to more intentional thought processes as participants pursued their ambitions at their home institutions. One participant shared how setting a goal during the program led to a key conversation with a senior leader at their institution, opening up a leadership opportunity that they were encouraged to pursue. They credited EMPOWER with helping them recognize and seize the opportunity with greater clarity and intention (Q20).
Participants noted that discussions with their peers provided the opportunity to examine and obtain feedback on career goals by sharing and comparing different experiences and viewpoints (Q21). They perceived the peer circle as allowing for the time and space to assess, question, or make decisions about personal values and leadership aspirations without pressure or judgment. For example, one participant valued the opportunity to openly discuss uncertainties about leadership, noting that others in the group shared similar questions and hesitations (Q22). A faculty advisor observed that one participant, after reflecting deeply, decided to focus on enhancing their current role rather than pursuing advancement for its own sake (Q23).
Barriers to EMPOWER program participation, engagement, and commitment
While experiences with the EMPOWER program were mostly positive, with many participants who perceived beneficial learning and professional development outcomes as described above, some participants reported being unable to fully participate at times and, therefore, did not feel that they were able to maximize or realize all the potential benefits. Perceived barriers to full program participation and engagement included a lack of time and limited availability/scheduling issues, limitations of an online/virtual format, individual circumstances, and idiosyncratic group dynamics (Fig. 2).

Perceived barriers to EMPOWER program participation, engagement, and commitment. These barriers were perceived to hinder full participation and engagement and, thereby, the ability to maximize and realize all potential benefits: (1) lack of time and limited availability/scheduling issues, (2) limitations of online/virtual format, (3) individual circumstances, and (4) group dynamics.
Lack of time and limited availability/scheduling issues
The most glaring barrier to program participation and engagement was a lack of adequate time to devote to readings, learning activities, and assignments, due to the various competing demands already placed upon participants with overlapping roles in clinical practice, research, teaching, and administrative duties within academic medicine. Those with more clinical practice, in particular, faced greater challenges with availability and scheduling flexibility. Participants noted that they simply did not have enough time to prepare between each monthly virtual meeting to be able to fully engage in meaningful discussions (Table 3; Q24), although they could still benefit from partially completing the preparatory work or listening to peers who had completed assignments (Q24, Q25). Some felt they needed more time during the peer circle meetings to engage in deeper discussions or bond with peers (Q26); however, they also acknowledged that it would be difficult to request participants to attend meetings for longer than 1 hour given the already limited flexibility and existing constraints in peers’ schedules.
Difficulty in agreeing upon a meeting time that fit everyone’s schedule in the peer circle was a frequently mentioned obstacle (Q27, Q28). Sometimes, there were conflicts between those who were open to scheduling meetings in the evenings or on weekends and others who preferred to meet only during work hours citing work–life balance reasons (Q27). Nevertheless, most participants tried their best to be flexible and accommodate the preferences of others in their peer circle.
Limitations of online/virtual format
Participants’ attitudes toward the use of technology or their level of tech-savviness sometimes hindered their engagement with the online learning platform or participation in the virtual meetings (Q29, Q30). Some observed that building bonds and relationships was difficult when interacting in an entirely virtual space (Q31). Not only could technical difficulties interrupt connections, but communication could feel awkward due to distractions or not being able to read facial expressions or body language (Q32). Participants also noticed that the level of accountability for completing assignments or attendance was lower in EMPOWER’s online environment compared with what they had generally experienced in the past when attending in-person meetings (Q33).
Individual circumstances
Participants’ family caregiving responsibilities were cited as an individual circumstance restricting already limited availability for scheduled meetings (Q34, Q35).
Another perceived barrier was that the program content, goals, or demands at times did not align with participants’ specific needs depending on their career stage. Participants felt that the curricular content was less relevant to them if they were more established in their careers and/or had different professional needs or concerns (Q36, Q37). Some noted that certain curricular content, such as the learning module focused on negotiation, would have been more helpful at a different, often earlier, point in their career trajectory (Q38).
Group dynamics
Participants mentioned various factors that could affect group dynamics in the peer circle, thereby making participation and engagement more challenging. Disparities in preparedness as well as attrition/absences were reported (Q39), often due to the barriers already described above. Additionally, some participants mentioned unbalanced or awkward group composition, such as a lack of diversity that limited the range of perspectives (Q40), or too many differences without enough commonality (Q41).
Some participants noted additional barriers concerning difficulties with group facilitation. There was, at times, a disconnect in terms of the faculty advisor’s comfort navigating the multiple roles needed to meet the various needs and expectations of their peer circle (Q42). These roles included facilitating discussions, ensuring balanced group interactions and meaningful integration of curricular content with real-life examples, serving as the initial group leader (with the goal of eventually enabling peer mentoring and co-leadership within the peer circle), and contributing as a senior mentor and advisor. When the faculty advisor was perceived as ineffective in one or more of these roles, it sometimes negatively affected the functioning of the peer circle (Q43, Q44, Q45).
Recommendations to improve EMPOWER program quality and best practices
Participants shared detailed recommendations to enhance program participation, engagement, and commitment (Table 4). Key suggestions included more clearly communicating program goals, roles, and expectations through orientation and training, as well as customizing content to align with participants’ career stages, interests, and identities. Some suggested that it was important to showcase the program’s benefits to attract motivated candidates whose career goals closely align with the program. In addition, expanding the program beyond mid-career or research-focused participants was thought to increase inclusivity and impact.
Recommendations to Improve EMPOWER Program Quality and Best Practices for Similar Programs a

We recognize that different institutions may have varying resources, rules, and constraints that will affect their desire or ability to implement some of these recommendations. These site-specific variations are to be expected and carefully considered as stakeholders seek to develop programs that optimally meet their institution’s goals and needs. Recommendations marked with an asterisk are optional and can be adapted based on idiosyncratic circumstances and the specific needs of each institution hosting the program.
ELAM, Executive Leadership in Academic Medicine.
Intentionally optimized program structure and efficiency were identified as critical, with recommendations to allocate more time to key topics and assignments while reducing mental burdens by streamlining access to material and email reminders. To improve learning experiences and engagement, participants suggested balancing didactic content with hands-on activities with practical, actionable objectives, integrating peer mentoring opportunities, and dedicating a session for participant-selected discussion topics. To overcome virtual format limitations, incorporating hybrid options with in-person meetings, shared written bios with photos to facilitate introductions and strengthen recognition, alternative communication venues, such as discussion boards, and additional one-on-one sessions could strengthen bonding and networking.
Effective faculty advisors were described as those with a strong belief in the program’s value for fostering leadership in academic medicine, especially those who have a comprehensive understanding of faculty development and a broad range of experiences that allow them to effectively address the challenges experienced by program participants. Providing faculty advisors with training, clear guidelines, and opportunities to incorporate rotating experts could enrich the quality of facilitation. Accountability and engagement can be reinforced through regular feedback, rotating leadership roles within the peer circles, one-on-one check-ins, and faculty advisors recognizing accomplishments while supporting those facing challenges.
Finally, increasing program visibility through institutional support, nomination processes (or a hybrid nomination/open application model for inclusivity), connections with established networks such as ELAM®, and a formal national meeting could boost engagement, opportunities for more widespread professional recognition, and a sense of accomplishment at being part of a broader initiative.
In sum, many program participants and their faculty advisors reported positive experiences and benefits from EMPOWER. In particular, the peer circle appeared to play an important role in reinforcing the learning of curricular content in addition to presenting new, outside perspectives. It also provided needed social support, encouragement, and guidance for how to practically apply skills in pursuit of career goals. Lastly, while some observed barriers prevented them from fully maximizing benefits, many participants recounted rich experiences and impressions. Detailed recommendations were made to improve quality and best practices, helping to reduce barriers and amplify benefits in future iterations of the program. These recommendations are valuable but should be adapted based on institutional goals, available resources, and participant needs to ensure successful and effective implementation.
Discussion
In this qualitative study, we investigated the factors impacting program feasibility, optimization, and scalability through in-depth interviews with EMPOWER participants and focus groups with their faculty advisors. Qualitative analysis of their recounted lived experiences and observations highlighted the peer circle’s important role in enhancing leadership learning and engendering positive professional development outcomes. It also identified the barriers impacting program participation and engagement, informing best practices and opportunities to improve program quality.
The benefits described by program participants and their faculty advisors reinforce the value of women’s leadership development programs, especially those that include a peer mentoring component.10–12 Such peer interactions may be especially useful in providing participants with external information, resources, and feedback that they otherwise would not be able to access at their local institutions due to workplace environment or politics. Participation in a national program with peers from different institutions who share similar experiences may also serve to provide emotional support and validation for isolated or marginalized women faculty while ensuring safety and anonymity. Our findings align with other studies on cross-institutional peer mentoring programs,28,29 which show that these programs facilitate the exchange of external strategies and practices and helped participants feel safer and more comfortable sharing challenges while avoiding institutional politics and confidentiality concerns. Furthermore, the networks formed through the program can potentially evolve into peer sponsorship when sustained over time. The experiences, observations, and recommendations voiced by program participants and their faculty advisors are consistent with what other scholars have previously identified as barriers to online learning in medical education and proposed best practices for ensuring quality and efficiency.30,31 Participants echoed common barriers, such as technological challenges and engagement difficulties in online learning environments. This study also reflects barriers noted in literature on virtual mentorship and peer mentoring, particularly the challenges of cultivating meaningful relationships and maintaining long-term commitment in a virtual setting.11,32 Programs designed to support women’s advancement in academic medicine should reduce, to the greatest extent possible, barriers related to labor and mental load. Evidence suggests that a lack of time and flexibility, which can be further exacerbated by parental or caregiving responsibilities, is especially salient and burdensome for women. 33 These challenges can limit their ability to fully engage in leadership development opportunities to advance in their careers.
That some participants desired more clearly communicated goals, roles, expectations, and training of faculty advisors speaks to the need for extensive preparation and oversight of such initiatives and the tradeoffs of a purely virtual program. Of note, these concerns were articulated even in the context of a program that had been developed via a collaborative expert team over multiple years and with the participation of numerous experts in leadership training. 14 We intentionally developed a strictly virtual program that limited requirements for synchronous participation to maximize flexibility of scheduling in a cohort known to face many competing time pressures, 33 but this approach did involve tradeoffs. Specifically, participants who did not review the extensive materials available to them might have been better served by a program that required a greater time commitment and perhaps some degree of in-person interaction that might have motivated greater engagement. Future programs that desire to pursue a purely virtual format should consider incorporating additional mandatory orientations and trainings to ensure all participants review important content at the outset, consistent use of reiteration/reminders to maximize retention, and dedicated time during meetings to further digest the information about the goals and their roles with their peer circle.
Given the need for scalable programs that can reach emerging women leaders on a broader scale, particularly at a time when academic institutions are facing financial constraints on the ability to support faculty travel, approaches that can reduce the barriers inherent to virtual programming should be further explored and implemented. The virtual format of EMPOWER offers participants flexibility. Evidence suggests that virtual mentorship programs34–36 can increase accessibility, convenience, and cost-effectiveness, all of which are crucial for women in academic medicine who face competing demands, such as caregiving responsibilities or challenges with traveling frequently for in-person meetings. Also, virtual platforms may further equity by enabling quieter voices to be heard, through typing into the chat or virtual hand raises, 36 for example. Interestingly, several participants mentioned that a hybrid format in particular might be preferable and potentially more effective, which is consistent with prior qualitative findings on the preferences of medical faculty. 37 This suggests that while convenience and accessibility is important for busy faculty clinicians, it remains imperative that programs maximize to the greatest extent possible meaningful in-person engagement and longer-term personal connections. Hybrid programs that enhance virtual meetings and an online curriculum by strategically incorporating limited but impactful in-person experiences may provide the best of both worlds. Future structured in-person EMPOWER components could include an initial retreat for participants to meet and outline goals. This could be followed by a midpoint session to strengthen peer interactions and discuss both challenges and opportunities among the group. Finally, a closing symposium to highlight accomplishments and discuss future virtual and in-person interactions could be incorporated into the program. These interactions would strengthen peer interactions and foster a deeper sense of community that could be continued both in person and virtually. Combining virtual sessions with in-person interactions might optimally facilitate enduring peer relationships and foster new connections.
We acknowledge that the in-person interactions also carry with them a financial burden superimposed upon a time burden.34–36 In-person programs carry costs not only for organizers but also for participants. They necessitate travel, time off work, and making the required accommodations at home, including securing childcare, which may be particularly difficult for those at earlier stages in their career, as well as care for adult kin, which may be difficult across many age groups. Moreover, geographic and mobility constraints may further limit accessibility and equity. In under-resourced institutions, these burdens are likely to be even greater, posing an additional obstacle to select participants. The benefits of in-person interactions therefore must be weighed against the cost and accessibility for participants. Ultimately, hybrid models should be designed to promote equity among participants and offer realistic opportunities for participant engagement. By enhancing access and flexibility while preserving the most crucial aspects of in-person communication and networking, hybrid programming can support a more inclusive and effective approach to leadership development if harmonious integration and ideal balance are achieved. This would help ensure that women have the opportunity to thrive in academic medicine despite the challenges they face.
Notably, some participants reported less engagement with the materials or their peer circle if they perceived that the curriculum content, learning goals, or conversation topics were not directly relevant to their career stage or professional interests. Given the limited time available for career development, especially in the context of virtual or hybrid formats, the importance of tailored programming to maximize results while reducing the extra burden of superfluous content seems especially important to consider. To enhance meaning and impact, program designers could consider incorporating goal customization, individualized learning paths, and groups carefully assembled to heighten peer compatibility for more dynamic interactions. To better support such individual needs in navigating career progression and transitions, program planners should seek to incorporate established frameworks, such as the Faculty Career Self-Management Model, 38 or milestones designed for faculty development in academic medicine. 39 These frameworks enable participants to anticipate and reflect on their stage-specific needs, so that they can align program and mentoring opportunities with personal goals as well as seek out more compatible peer groupings and support networks. The recommendations that we present here to improve the EMPOWER program and others like it are informed by the rich experiences of our study participants—highly accomplished women medical faculty, many of whom have limited bandwidth given their leadership roles and responsibilities. These recommendations offer a simple and adaptable guide for administrators of similar virtual programs for women in academic medicine, helping them proactively address barriers prior to implementation to maximize participation, engagement, and commitment. It should be noted, however, that women-only leadership programs do not currently exist in the same way as when the research team initially conducted this study due to recent policy developments and the continually evolving landscape in academic medicine. Nevertheless, these rich qualitative accounts are germane to leadership development programs more broadly.
Moreover, the recommendations herein can serve as a highly informative guide as administrators seek to reimagine how they will develop more widely inclusive and accessible programs going forward that will benefit the advancement of all promising leaders in their academic medical careers. 40 Women’s leadership programs are under increased scrutiny secondary to the legal and political initiatives aimed at gender-specific initiatives,40,41 not necessarily because of waning interest or evidence of ineffectiveness. These pressures underscore the importance of creating programs that offer flexibility, with the ability to shift with institutional directives and changes in society and social norms. The EMPOWER program structure and content are highly adaptable; thus, it can be readily modified in the face of the rapidly shifting landscape of gender-aware leadership development programming toward broad inclusion and accessibility.
However, as championed in a recent statement from ELAM, 41 change in ability to host gender-specific programming does not mean that a program’s mission must completely change, although the strategies to work toward that mission may have to be altered. Like ELAM, programs can continue to challenge and reform the institutional structures that hinder women and others from assuming influential positions. 41 With gender-inclusive programs, total reach can be broadened, furthering dialogue across a wide range of lived experiences. This approach can augment impact and galvanize a wider community of leaders to aim for transformative change. 41 These programs must continue to be evidence-based as they evolve, while continuing to acknowledge and address the gaps that exist in academia among different gender and racial or ethnic groups.
Furthermore, it is important to carefully consider the risks and implications of expanding access to programs versus losing the safety and solidarity that many women valued in gender-specific spaces. In gender-specific spaces, program participants may feel more comfortable discussing sensitive challenges such as bias and discrimination 42 and may benefit from connecting with mentors and peers with similar lived experiences. 43 Gender-specific programming can also offer targeted skill-building particularly for areas in which gender disparities continue to exist, such as negotiation44,45 and sponsorship. 21 Indeed, the loss or dilution of gender-specific spaces poses several possible downsides, including blunted group bonding dynamics resulting from a reluctance to fully share experiences in perceived unsafe spaces, weakened networking opportunities because some may find it more difficult to cultivate peer connections in mixed settings, and pressure to conform to typical “male” leadership norms 46 rather than exploring diverse approaches to leadership.
In light of this, identity-centered cohorts might serve as a middle ground. Identities are complex, and gender is only one of the identities any given person may bring to the conversation. Future programs could seek to invite participants to indicate whether they would prefer to meet in a mixed identities group or a shared identity group. Program administrators can inquire as to what identities are important to participants, whether it be gender, race/ethnicity, medical specialty, region, parental status, career stage, or another factor, and try to organize those shared identity meetings, if possible. If such shared identity spaces are not feasible, programs should foster environments that support and encourage individual participants in voicing issues associated with their identities as they would like to raise them, both in the group setting and to the facilitator or faculty advisor.
This study has potential limitations. Participants who accepted the interview invitation may have been more likely to have been engaged or to hold more favorable views of the program, potentially leading to an overrepresentation of positive experiences. However, we deliberately made efforts to include some participants who were ultimately unable to complete or fully engage in the program to gather data on their unique perspectives and experiences. Since interviews were conducted either at the program’s midpoint or a few months after its completion, this qualitative study did not capture longer-term impacts or reflections on the program. Additionally, the scope of our analysis did not assess for thematic differences between the midpoint and end of the program.
A particular strength of this study is its adherence to rigorous qualitative methods. A purposeful sampling strategy15–16 was used to maximize the diversity and range of viewpoints gathered, and adherence to thematic saturation19,20 ensured that the data collected reflected sufficient depth and variation. Two forms of triangulation 47 were employed to strengthen the validity of the study findings. First, the analytical team varied in training as well as gender and racial identities, which enhanced investigator triangulation and diversity of perspectives. Second, data source triangulation was achieved by gathering both individual interviews with program participants and focus groups with their faculty advisors, which provided complementary accounts that were also inherently different in nature. Another strength of this study is that the rich, detailed information concerning program quality improvement and best practices is based on actual lived experiences and insights of those who participated, ensuring the recommendations are participant-centered and more likely to lead to actionable and meaningful changes that enhance the program for future participants.
Conclusions
Overall, the findings of this qualitative study suggest that the EMPOWER program is a promising, scalable intervention. It can inform the development of future programming that seeks to be inclusive on a broad scale, particularly regarding the gender-aware content that is crucial knowledge for all leaders in academic medicine. Program administrators should thoughtfully consider how to minimize barriers to participation and engagement, especially those associated with limited time and flexibility. Moreover, they should implement best practices for optimizing and improving program quality to enhance individual and group experiences through purposeful planning, tailored programming, intentional recruitment, and efficient implementation.
Ethical Approval
The University of Michigan Institutional Review Board approved this study as part of a randomized trial to evaluate its impact (HUM00185660).
Authors’ Contributions
R.D.J.: Project administration, data collection, analysis/interpretation, writing—original draft, and writing—review and editing. Y.-J.L.: Data collection, analysis/interpretation, writing—original draft, and writing—review and editing. J.D.T. and A.M.B.: Analysis/interpretation and writing—review and editing. N.D.S.: conceptualization, interpretation, and writing—review and editing. C.M.C.: Interpretation and writing—review and editing. K.S.: conceptualization, interpretation, and writing—review and editing. K.C.P.: interpretation and writing—review and editing. E.A.K., E.L.F., A.J.S., I.H.S., and P.A.U.: Conceptualization, interpretation, and writing—review and editing. R.J.: Conceptualization, interpretation, funding acquisition, supervision, and writing—review and editing.
Footnotes
Acknowledgments
The authors thank their colleagues comprising the broader EMPOWER Intervention and Evaluation Team: Dana A. Telem, MD, MPH, Susan M. Pollart, MD, MS; Harriet W. Hopf, MD; Kent A. Griffith, MS, MPH; Nina A. Bickell MD, MPH; Ann Brown MD MHS; Linda A. DiMeglio MD, MPH; Colleen T. Fogarty MD, MSc; Nisha Garg, PhD, MBA; Sheryl L. Heron MD, MPH; Richelle J. Koopman MD, MS; Martha McGrew MD; Karin Muraszko MD; Elizabeth M. Petty, MD; Aina Puce PhD; Anne L. Taylor, MD; Lisa Tedesco PhD; Sharon Turner, DDS, JD; Pamela M. Williams MD; and Peyton C. Kanaly. The authors also thank the program participants and faculty advisors who contributed their insights by participating in the interviews and focus groups.
Author Disclosure Statement
Ms. Jones reports a grant from the National Institutes of Health (NIH; grant R01GM139842 from the NIH to Dr. Jagsi), during the conduct of the study, and a grant from the Doris Duke Charitable Foundation (to Dr. Jagsi), outside the submitted work. Dr. Lin reports a grant from the NIH, during the conduct of the study (grant R01GM139842 from the NIH to Dr. Jagsi). Dr. Thomas reports a grant from the NIH, during the conduct of the study (grant R01GM139842 from the NIH to Dr. Jagsi). Dr. Blake has no interests to disclose. Dr. Spector has no interests to disclose. Dr. Cutter reports a grant from the NIH (R01GM139842), during the conduct of the study; a grant from the Doris Duke Charitable Foundation, personal fees (payment or honoraria for lectures, presentations, speakers bureaus, article writing, or educational events) from Research Consortium for Health Care Value Assessment, RAND Corporation, and Wolters Kluwer, outside the submitted work. Dr. Singer reports a grant from the NIH (R01GM139842), during the conduct of the study; and grants from the NIH, outside the submitted work. Dr. Paradis has no interests to disclose. Dr. Kerr reports receiving a grant from the Department of Veterans Affairs Research Service (IIR 21-024) and being a consultant for the National committee for Quality Assurance, outside the submitted work. Dr. Feldman reports a grant from the NIH (R01GM139842), during the conduct of the study; grants from the NIH, CDC/ATSDR, American Heart Association, Juvenile Diabetes Research Foundation, and the Department of Defense, outside the submitted work. Dr. Stewart has no interests to disclose. Dr. Settles reported funding from the National Science Foundation, outside the submitted work. Dr. Ubel has no interests to disclose. Dr. Jagsi reported receiving a grant from the NIH (R01GM139842) that supported the conduct of the study; she also reported unrelated grants from the NIH, the Doris Duke Charitable Foundation, the American Cancer Society, and the Susan G. Komen Foundation, and personal fees from Hawks Quindel and Mintz Levin Law, the Greenwall Foundation, the Doris Duke Charitable Foundation, the NIH, the Blue Cross Blue Shield Association, the Physicians Education Resource, and the American Medical Association, outside the submitted work.
Funding Information
This work was supported by grant 5R01GM139842-03 from the National Institutes of Health (Dr. Jagsi).