
Abstract
Uterine lipoleiomyoma is a rare benign tumor composed of smooth muscle and mature adipose tissue. We report a case of a 53-year-old perimenopausal woman who presented with vaginal spotting for 2 months. Transvaginal ultrasonography revealed a hyperechoic submucosal mass with a hypoechoic rim at the anterior uterine wall measuring 37 × 39 mm. Hysteroscopic resection was performed, and histopathology confirmed lipoleiomyoma characterized by bland spindle cells mixed with mature adipocytes and thick-walled blood vessels. The patient recovered uneventfully and remained asymptomatic during follow-up. This case highlights the importance of recognizing this rare benign variant of leiomyoma, particularly in perimenopausal women.
Introduction
Uterine lipoleiomyoma is an uncommon, benign mesenchymal neoplasm, recognized as a distinct variant of common uterine leiomyoma. The incidence was reported by Willen et al. in 1978, to be 0.03%–0.2% of all surgically removed uterine leiomyomas and reported by Akbulut et al. in 2014 1 to be up to 2.9% in some series of benign uterine tumors. Lipoleiomyoma is a variant of leiomyomas so they contain similar features. Over 80% of them are found in postmenopausal women, and they can still grow after menopause, unlike usual uterine leiomyoma. 2 These tumors are usually incidental findings; however, some may have severe symptoms. The preoperative diagnosis of lipoleiomyoma may be challenging due to its rarity and nonspecific imaging appearance; however, histopathological evaluation remains definitive and straightforward. Their defining histological feature is the presence of an intimate admixture of mature adipocytes and benign smooth muscle cells. 1 Due to its rarity and often incidental discovery, understanding their characteristics, clinical behavior, and diagnostic features is crucial for appropriate clinical management. This report aims to provide a comprehensive synthesis of the current knowledge regarding uterine lipoleiomyoma.
Methods
The case report was reviewed and approved by the Institutional Review Board (IRB) of Chulabhorn Royal Academy (EC 024/2565). Written informed consent was obtained from the patient for publication. The protocols of animal experiments were followed in accordance with the Guidelines for the Care and Use of Laboratory Animals and were supervised by the Chulabhorn Royal Academy.
Case Report
A perimenopausal 53-year-old female presented at our clinic with vaginal spotting for 2 months. Her regular menstrual period was 3 months ago with an interval of 2–3 months. She denied any abdominal discomfort, abdominal pain, frequent urination, changes in bowel habits, or constitutional symptoms. The patient’s body mass index (BMI) was 27.8 kg/m2. Laboratory review revealed normal thyroid function and lipid profile, with no history of diabetes mellitus or hyperlipidemia. Her only comorbidity was well-controlled essential hypertension. The last pelvic examination was 1 year ago with a normal cervical screening result. The patient had two children and gave birth naturally. She denies a family history of cancer and any past surgery. Abdominal and pelvic examinations were unremarkable. Transvaginal ultrasonography showed a retroverted uterus with irregularities in the endometrial lining suspected endometrial polyps, a hyperechoic mass with hypoechoic borders at the anterior wall of the uterus sized about 37 × 39 mm, and unremarkable both ovaries (Fig. 1). The uterine mass did not have increased vascularity on the Doppler study.
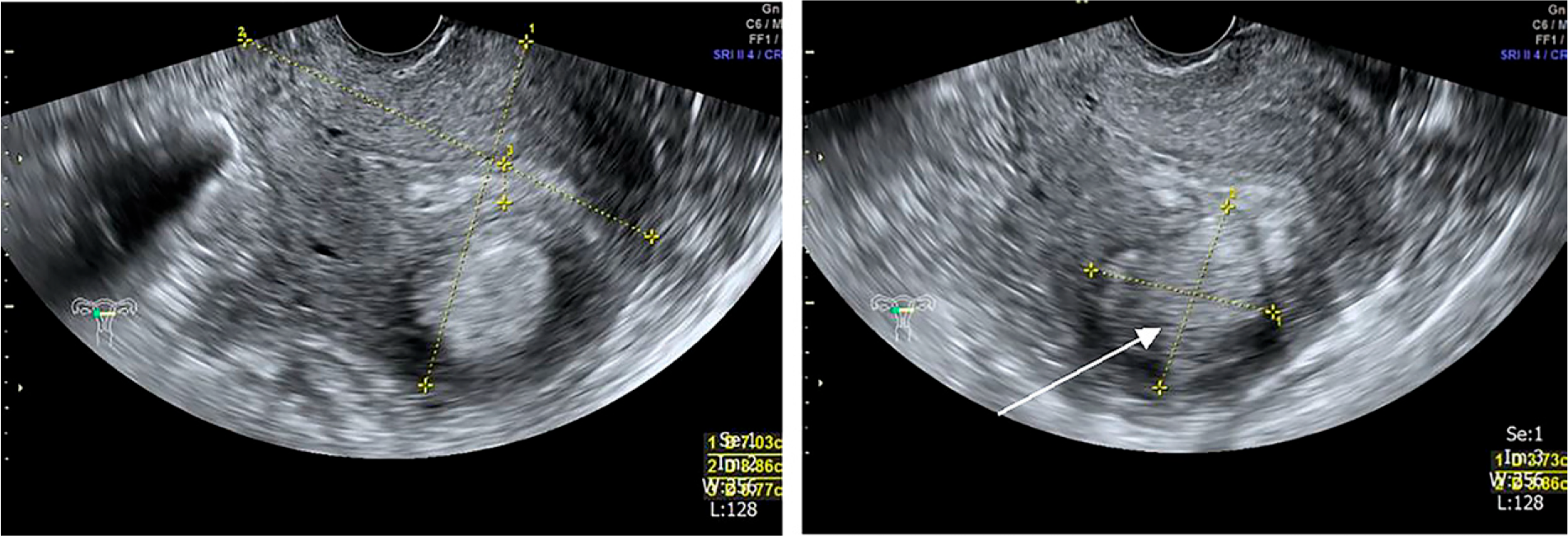
Transvaginal ultrasound shows retroverted uterus size 70 × 89 mm, irregularities of endometrial lining, endometrial thickness 7.7 mm, and hyperechoic mass with hypoechoic border at anterior wall of uterus size 37 × 39 mm (arrow).
Due to her abnormal uterine bleeding, hysteroscopy was scheduled. We performed an uneventful 50 minute procedure. Atrophic endometrium was observed, with a yellow intrauterine mass size about 4 cm protruding from the anterior wall of the uterus, normal both tubal ostia (Fig. 2). We performed hysteroscopic resection of the intrauterine mass and retrieved multiple soft, yellow tissues of uterine mass and were sent for pathological examination. After the procedure, the patient had a full recovery and discharged from the clinic.

Hysteroscopy showed yellow intrauterine mass size about 4 cm protruding from anterior wall of uterus (arrow).
Microscopic findings show fragmented tissue consisting of the interlacing fascicles of spindle cells containing uniform blunt-ended nuclei without mitosis. There are thick-walled blood vessels and nests of adipocytes set in the tumor, suggestive of lipoleiomyoma (Fig. 3). After the surgery, the patient has not menstruated and did not have any vaginal spotting, as she may be in menopausal transition, so we decided on conservative treatment and plan follow up her clinical.

Discussion
Uterine lipoleiomyoma is a variant of uterine leiomyoma and can have similar clinical presentations. It is formally defined as a rare, benign variant of leiomyoma characterized by a mixture of mature adipocytes and bland, spindle-shaped smooth muscle cells. 1 It falls under the broader category of lipomatous uterine tumors, which also encompasses pure lipomas (composed almost entirely of fat cells) and fibrolipomyomas (containing significant fibrous tissue alongside fat and smooth muscle). 3 Uterine lipoleiomyoma is consistently described as a rare entity. 1 Older literature frequently cites an incidence ranging from 0.03% to 0.2% of all surgically removed uterine leiomyomas. 3 Some sources place it at less than 0.2% of all benign uterine tumors, 4 while others mention figures like 0.35% or up to 2.1%. 1
From a review of previous literatures, the demographic profile of patients with uterine lipoleiomyoma is quite distinct from that of patients with conventional leiomyomas:
Most patients are asymptomatic; others may present with abdominal discomfort, abnormal vaginal bleeding, pelvic pain, constipation, increase urination frequency. Ultrasound is the first choice of imaging to diagnose lipoleiomyoma, as for other uterine tumors. The ultrasound will show a well-circumscribed mass, hyperechoic with a partially hypoechoic rim, and poor vascularity on color Doppler examination. CT and MRI can help in diagnosis and are more specific in demonstrating the origin of the tumor and fatty component. 8 However, even with CT or MRI, lipoleiomyoma is hard to diagnose. A retrospective study was performed, in 51 patients that were diagnosed with lipoleiomyoma postoperatively, only 14% were correctly diagnosed. If they can be diagnosed before surgery, some patients can avoid unnecessary procedures. 9
Mostly, it is located in the uterus, although cervical, ovarian, broad ligament, and retroperitoneal locations have been reported. 10 The etiology is not clear; however, there are many hypotheses. The most accepted theory is that there is a fat metamorphosis of smooth muscle cells into adipose tissues. 11 Some suggested that there is an impairment in fat metabolism in patients with lipoleiomyoma and is associated with concomitant metabolic disorders, 12 in which this patient has essential hypertension.
Given the presence of fat and its origin within the female pelvis, several entities must be considered in the differential diagnosis of uterine lipoleiomyoma. Differential diagnoses include:
Lipoleiomyomas have similar presentations as leiomyomas, but they can grow larger in postmenopausal women, unlike leiomyoma that usually decrease in size in the postmenopausal period. In our case, the patient was overweight (BMI: 27.8 kg/m2) and multiparous (para 2) but had no metabolic disorders such as diabetes, hyperlipidemia, or hypothyroidism. These findings partially align with prior reports suggesting a possible association between lipoleiomyoma and obesity or parity. Treatment is surgical removal of the tumor if the patient is symptomatic, the diagnosis is unclear, or there is a concern for malignancy. 13 The tumor is benign and has a good prognosis after long term follow-up. If the patient is asymptomatic and the diagnosis is unquestioned, conservative treatment is appropriate. After resection of the lesion, our patient did not have abnormal uterine bleeding, her menstrual interval has been lengthening, and menopausal transition is suspected.
Conclusion
Uterine lipoleiomyoma represents a distinct, rare, benign variant of leiomyoma, uniquely characterized by the histological admixture of mature adipose tissue and smooth muscle cells. It typically manifests in postmenopausal, often obese, women and is frequently discovered incidentally. While often asymptomatic, it can present with nonspecific symptoms similar to conventional leiomyomas, such as abnormal bleeding or pelvic pressure.
Diagnostic evaluation relies heavily on imaging, with ultrasound often providing initial suspicion due to the characteristic hyperechoic appearance with a hypoechoic rim. CT and, particularly, MRI with fat-suppression sequences are crucial for confirming the presence of macroscopic fat, determining uterine origin, and differentiating lipoleiomyoma from other pelvic masses. However, a definitive diagnosis requires histopathological examination, which reveals the characteristic cellular composition and absence of malignant features.
The prognosis for uterine lipoleiomyoma is excellent, reflecting its benign nature. Malignant transformation is exceedingly rare. Management is guided by symptomatology, with asymptomatic lesions often managed conservatively through observation. Surgical intervention, typically hysterectomy or myomectomy, is reserved for symptomatic patients or cases with diagnostic uncertainty.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This research project is supported by Chulabhorn Royal Academy.