
Abstract
Background:
Ovarian tissue cryopreservation (OTC) is the only fertility preservation (FP) option available for prepubertal patients and has been endorsed by major medical societies. While disparities in adult FP care are well documented, the impact of social determinants of health on pediatric OTC utilization remains poorly understood.
Methods:
We conducted a retrospective study of 228 pediatric patients (≤14 years) referred for OTC from January 2011 to March 2023 at the University of Pittsburgh Medical Center and 19 collaborating U.S. centers. Analyses included: (1) comparison of OTC utilization per capita based on payment modality (Center-funded vs. Non-center-funded; n = 208), (2) association between socioeconomic status, assessed by the Distressed Communities Index (DCI), and OTC utilization (n = 186); (3) demographic predictors of OTC uptake (n = 62). DCI scores were derived from patient zip codes.
Results:
OTC utilization was 2.12 times higher at centers offering Center-funded services compared with those requiring payment. Patients in the Center-funded group had significantly higher median DCI scores (49.66 [18.22–67.01]) than the Non-center-funded group (26.99 [10.53–56.58]; p = 0.035), indicating greater socioeconomic disadvantage. Younger age was associated with lower OTC utilization (median age 2.00 years [1.25–6.00] for non-users vs. 8.00 years [4.00–11.00] for users; p = 0.016).
Conclusions:
Financial barriers, including socioeconomic disadvantage and out-of-pocket costs, significantly reduce pediatric OTC utilization. Additionally, younger patients are less likely to undergo OTC. Addressing these disparities through policy reform and financial support programs is critical to ensuring equitable access to FP care.
Keywords
Introduction
Chemotherapy, radiation, and other therapies can harm or destroy sperm, 1 eggs, 2 or the reproductive organs themselves,3–6 leaving patients at risk of infertility.7,8 In prepubertal girls, the risk of infertility following gonadotoxic treatment varies considerably (15–72%), and likelihood of risk depends on multiple factors, including but not limited to age at exposure, type of treatment, and the use of specific agents.9–11 For many, this loss of fertility is an unexpected and emotionally distressing aspect of their treatment. 12 Fertility and cancer societies around the world acknowledge this critical concern13,14 and recommend that patients with a diagnosis or treatment plan that may cause infertility should be counseled about their fertility risk and fertility preservation (FP) options.15–18 Prepubertal patients with ovaries cannot cryopreserve eggs. Therefore, the recommendation is to cryopreserve ovarian tissue.19,20 In 2019, the American Society of Reproductive Medicine (ASRM) recommended that the experimental label could be removed from ovarian tissue cryopreservation (OTC) after reports of more than 130 live births from the transplantation of cryopreserved ovarian tissue. 18 While some insurance plans cover FP, many do not, leaving patients to shoulder these expenses themselves, 21 which may amount to tens of thousands of dollars. The financial implications of these procedures and long-term cryostorage of ovarian tissues may lead some patients to forgo FP, a decision that can have long-lasting consequences for their quality of life.22,23
Social Determinants of Health (SDoH) has become an essential framework for understanding how health outcomes are shaped not just by biological factors but also by a wide range of social and environmental influences.24,25 Studies have consistently shown that socioeconomic status significantly impacts health outcomes.26–28 Likewise, ethnic disparities impact access to fertility care,29,30 and outcome of in vitro fertilization. 31 32 These disparities extend to FP, where geographic access (distance) to centers capable of offering FP services and socioeconomic status impact access and utilization of oocyte or embryo cryopreservation.33,34
This retrospective study investigated the SDoH impact on OTC utilization. To determine the socioeconomic status of patients, we used the Distressed Communities Index (DCI) score, a tool that measures U.S. communities’ economic health using seven metrics, which are detailed in the methods. 35
To the best of our knowledge, SDoH has not yet been assessed for the pediatric patient population requiring OTC. Studies so far have focused more on the technique36–38 and its possible outcomes39,40 but not on the socioeconomic parameters affecting the utilization of this procedure in the U.S. health care system. Therefore, the objective of this study was to evaluate the impact of SDoH and other parameters on the utilization of OTC among young patients (≤14) who are at risk of infertility.
Methods
Study design and setting
We report a retrospective multicenter analysis of patients who contacted the University of Pittsburgh Medical Center (UPMC) Magee Center for Reproduction and Transplantation (CRT) to pursue OTC between January 1, 2011, and March 31, 2023. The study population included patients treated at CRT as well as those referred from 19 collaborating institutions across the United States. Characteristics of participating centers are summarized in Supplementary Table S1.
Participants
Patients aged 14 and younger who sought OTC for FP through the Fertility Preservation Program at the UPMC were included in this study. Age 14 was the upper limit in accordance with the definition of childhood cancer criteria; OTC is the only FP option for most of those young patients.41–43 UPMC provides OTC processing and cryopreservation services for patients in the Western Pennsylvania region and 19 collaborating institutions across the United States that were included in this study. For patients treated at UPMC, the initial FP consultation also took place at UPMC, allowing capture of both patients who pursued OTC and those who did not. In contrast, for patients referred from the 19 collaborating institutions, we only received those who had already been selected to proceed with OTC following their initial consultation at the local center. As a result, analyses of utilization vs. non-utilization could only be conducted for the UPMC cohort, whereas the collaborating center cohort reflects only patients who ultimately underwent OTC. If performed at another center, ovarian tissue was transported for processing and cryopreservation to UPMC in Pittsburgh. Data were collected for all patients from UPMC as well as patients who were referred to our center after initial FP consultation at a collaborating institution, from January 2011 to March 2023.
This retrospective study was approved by the University of Pittsburgh Institutional Review Board (STUDY23040134). Informed consent was waived due to the presence of minimal risk and deidentified data. This study reported results according to the Strengthening the Reporting of Observational Studies in Epidemiology reporting guideline for cohort studies.
Data sources
This deidentified dataset included patient demographics, medical indication for FP, FP treatment plan and utilization, and zip code at the time of contact from the UPMC FP program or collaborating center.
Study groups
We compared patient groups by mode of payment for OTC: Center-funded vs Non-center-funded. The Center-funded cohort included patients whose OTC service expenses were covered through research or institutional/philanthropic funds and were available to all patients treated at UPMC and six collaborating institutions that covered those costs. The Non-center funded cohort consisted of patients who underwent the surgery at one of the remaining 13 collaborating centers without a funded option. Non-center-funded payment expenses are set by the collaborating centers, which may or may not submit to insurance, and ranged from $4,500 to $30,500.
Per capita estimates
We calculated the utilization of OTC per 1,000,000 individuals based on the metropolitan statistical area (MSA) 44 of UPMC and collaborating centers. Centers offering OTC are all large tertiary care centers for large geographic areas. In instances where multiple centers reside within the same MSA, the number of participants in the centers was summed and divided by the MSA population, which was counted only once. Because we used the center’s MSA for this analysis, even patients without zip codes were included in the Center-funded (n = 98) and Non-center-funded (n = 110) cohorts (Fig. 1).

Diagram of study design for patient groups included in both analyses. SDoH influencing OTC utilization, DCI, Distressed Communities Index; OTC, ovarian tissue cryopreservation; SDoH, social determinants of health; UPMC, University of Pittsburgh Medical Center.
Demographics and socioeconomic identification
Data sources
Socioeconomic status was calculated by assigning the Distressed Communities Index (DCI) score based on the patient's zip code. The DCI covers 99% of the U.S. population and combines seven economic indicators (education, housing vacancy, unemployment, poverty, median income ratio, employment change, and business change) to generate a single index score, with a range from 0 (least distressed) to 100 (most distressed). 35 The DCI is available at the zip code level for areas containing at least 50,000 people. DCI was chosen as a validated, nationally standardized proxy for SDoH that enables comparison across geographic regions and has been widely applied, including in health research.45,46 For this analysis, patients with missing zip codes or DCI information (n = 31) were excluded. In addition, a subclassification of DCI was made by dividing DCI scores into high (≥50) and low (<50).
Two separate analyses focused on the SDoH influencing OTC utilization were performed (Fig. 1). The first analysis compared demographic and clinical characteristics between the Center-funded and Non-center-funded cohorts. The second compared demographic and clinical characteristics between patients/families who utilized OTC and those who did not at UPMC. Patients who were not recommended to proceed with OTC due to medical contraindications or did not meet research study eligibility criteria were excluded.
Statistical analysis
Demographic and clinical characteristics were described as proportions for categorical variables and medians and interquartile ranges (IQRs) for continuous variables. Significance between groups was assessed using Fisher’s exact test for categorical variables. A two-sided Wilcoxon two-sample test was used for the analysis of continuous variables. P-values <0.05 were considered significant. Data analysis was conducted using the R statistical computing software (version 4.2.3.).
Results
A total of 228 FP referrals were received by UPMC or collaborating centers between January 2011 and March 2023. OTC was utilized by 208 of 228 patients who were referred (Fig. 1).
Per capita utilization analysis
The 208 patients who utilized OTC were almost equally distributed among the Center-funded (n = 98) and the Non-center-funded (n = 110) cohorts. While both cohorts had a similar number of patients, the population served by the Center-funded centers (n = 21,112,673) was smaller than the one served by the Non-center-funded centers (n = 50,276,057) (Fig. 2). OTC utilization rate per capita for the Center-funded cohort was 4.64 OTCs per 1,000,000 compared with 2.19 OTCs per 1,000,000 in the Non-center-funded cohort. Consequently, OTC utilization was 2.12 times more prevalent when funding was provided (Fig. 3A).

Payment modality for ovarian tissue cryopreservation in various metropolitan statistical areas.

Distribution of OTC utilization by payment modality (Center-funded vs. non-funded).
Social demographic of health analysis
The analysis of payment modalities includes 186 patients with zip code information who completed OTC. No significant differences were observed in their baseline characteristics such as age, race, and reasons for FP between those in the Center-funded (n = 91) or the Non-center-funded (n = 95) cohort (Table 1). However, the Center-funded cohort had a significantly higher median DCI score, reflecting greater socioeconomic distress (median [IQR] = 49.66 [18.22–67.01]) vs. the Non-center-funded cohort (26.99 [10.53, 56.58]; p = 0.035; Table 1). When categorized, nearly half of the Center-funded cohort were from high-distress communities (49%), whereas only one-third of the Non-center-funded cohort were classified as high distress (34%; p = 0.037; Fig. 3B).
Baseline Characteristics of Patients Who Utilized Ovarian Tissue Cryopreservation by Modality of Payment
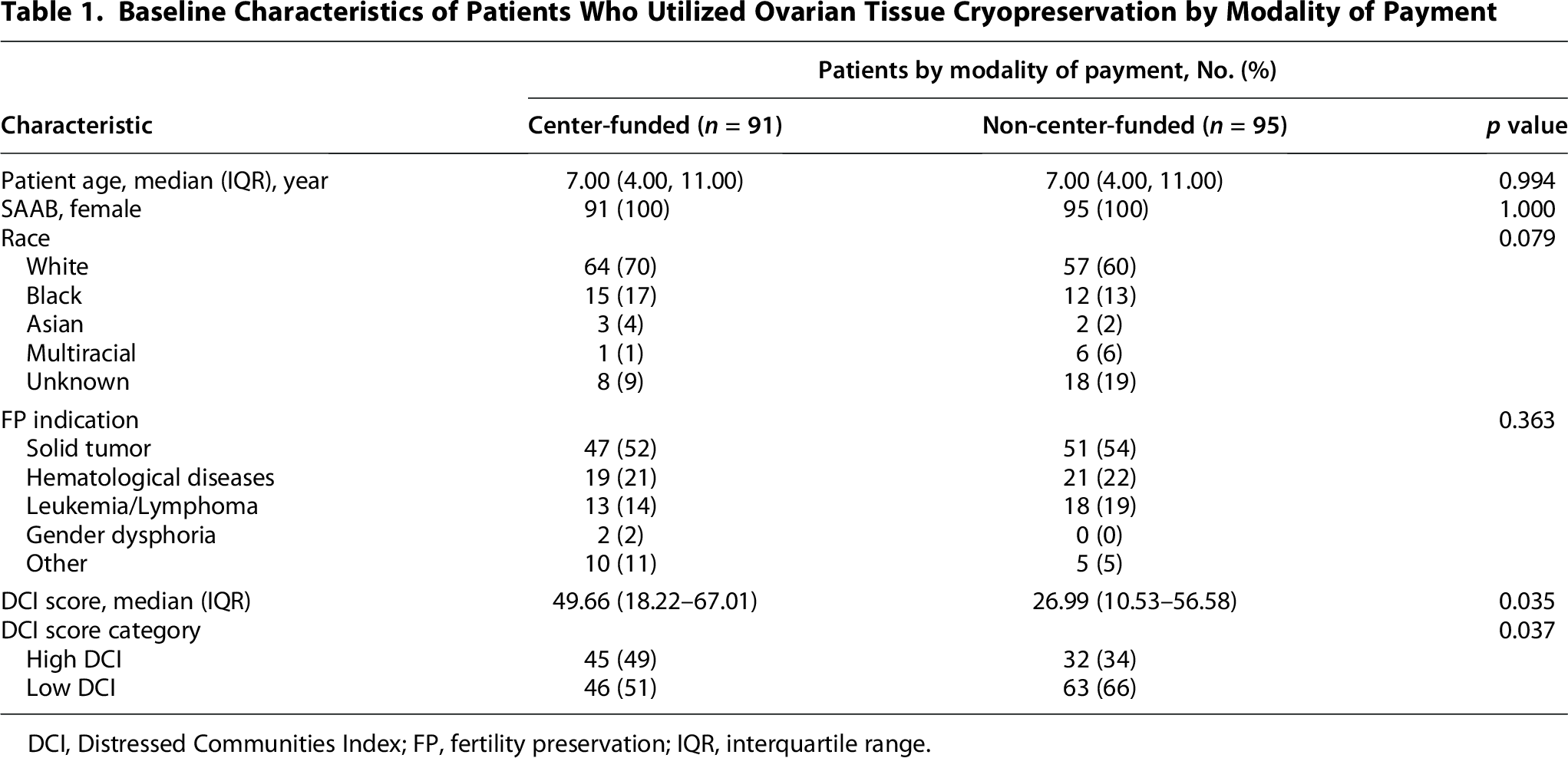
DCI, Distressed Communities Index; FP, fertility preservation; IQR, interquartile range.
Analysis by OTC utilization
When analyzing OTC utilization at UPMC, no demographic or socioeconomic differences were noted between patients who utilized OTC (n = 55) and those who declined (n = 7) (Table 2). However, a significant age difference was observed between the two cohorts. The patients who utilized OTC tended to be significantly older (age 8.00 [4.00–11.00] years) compared with those who declined OTC (age 2.00 [1.25–6.00] years; p = 0.016).
Baseline Characteristics of the UPMC Patients Consulted for Ovarian Tissue Cryopreservation
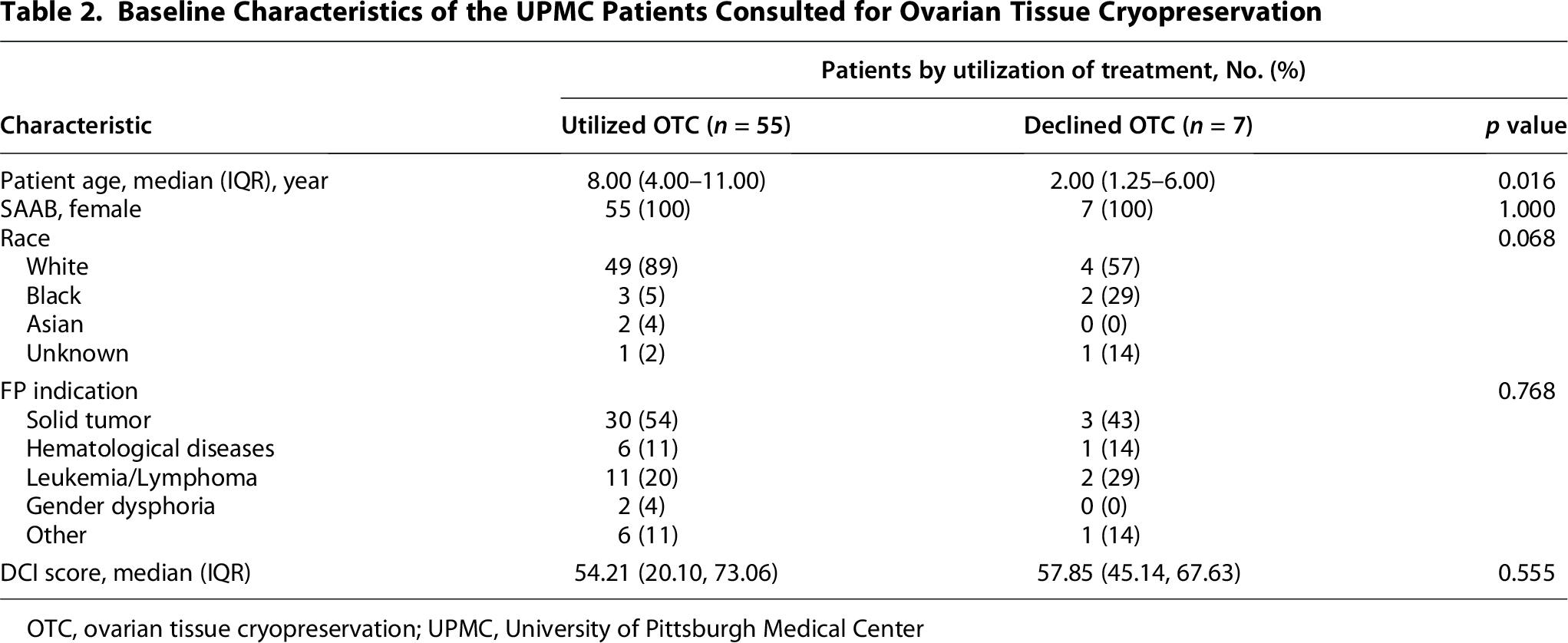
OTC, ovarian tissue cryopreservation; UPMC, University of Pittsburgh Medical Center
Discussion
We analyzed retrospective data from a large FP center (UPMC) that provides OTC services locally and to collaborating centers throughout the United States. This analysis aimed to identify factors contributing to disparities in the utilization of OTC for FP among young patients (≤14 years old) with ovaries. We found that socioeconomic status, cost of procedures, and age impacted the utilization rate of OTC.
Previous studies have highlighted significant disparities in access to FP among young individuals, influenced by gender, socio-demographic factors, and race.47–50 In the pediatric oncology context, the United Kingdom has observed notable geographic variations in FP access for cancer patients. 51 Similarly, in the United States, disparities in geographic access to oncology centers offering oocyte cryopreservation for FP have been documented. 34 These geographic differences exacerbate existing inequalities, particularly in financial coverage for FP. Currently, only 18 states mandate insurance coverage for FP, further underscoring the financial disparities in FP access. 52 Our study reveals a financial disparity in access to OTC in the United States and suggests that lack of financial coverage limits the utilization of this procedure. Patients living near centers offering Center-funded care utilized OTC at a much higher rate than patients who paid for this service. This may suggest that expanding insurance coverage for this FP option could significantly increase OTC utilization. These data are especially relevant as the ASRM recommended in 2019 that OTC is no longer experimental. Thus, OTC can be offered as a conventional FP option, like egg and sperm freezing, that could potentially qualify for insurance coverage. 18
Looking more specifically into the population that utilized OTC, we found that the socioeconomic backgrounds of the patients were different in the Center-funded cohort vs. the Non-center-funded cohort (Table 1). Our findings suggest that Center-funded OTC expands access for patients from socioeconomically distressed communities, enabling utilization for this population. This aligns with prior evidence that has highlighted socioeconomic disparities within the health care system and how this impacted access to health care services,53–55 and differences in medical outcomes.56–61 Additionally, factors such as the utilization of various medical services have been found to correlate with socioeconomic status.62,63 For instance, patients with lower socioeconomic backgrounds are more likely to exhibit lower utilization of outpatient care and to use emergency services at a higher rate.64,65
Our finding indicates that families with higher socioeconomic distress are less likely to pursue OTC when the family needs to pay to access this procedure. This finding is concerning, as numerous leading medical societies recommend FP prior to treatments associated with infertility.15,18,66–68 Furthermore, studies have shown that cancer survivors express a desire for parenthood.69,70 It has been well-documented that infertility among long-term survivors of childhood cancers contributes significantly to feelings of grief and psychological distress.71,72 Therefore, OTC should be accessible to all patients regardless of socioeconomic status. This study highlights socioeconomic disparities in utilization of FP care that should serve as a call to action. Infertility is an unfortunate side effect of treatments for cancer and other conditions. FP treatment for this side effect should be covered by insurance similar to treatments for the many other known side effects of cancer therapy (anti-mimetics, antibiotics, hematopoietic support, breast reconstruction). With childhood cancer survival rates surpassing 85%, 73 families can start planning for a full and productive (and reproductive) life after a cure from the time of their initial diagnosis.
Limitations
We recognize the limitations in our study. This was a retrospective study, so we were limited in the type of data that could be retrieved from each patient, and some data (e.g., zip code) were missing for some patients. In addition, the lack of personal data on SDoH leads us to use the DCI at the zip code level to determine the socioeconomic status. Even though the use of DCI is a well-known method reported in previous SDoH analyses,45,46 it might be possible that individual patient-level resolution of the data would yield more accurate results. We recommend conducting prospective studies, including SDoH surveys at enrolment, to reduce those biases. This analysis included only patients who were referred to and made contact with a center performing OTC. Patients not counseled, referred, or offered OTC were not captured, and SDoH factors may also influence these groups.
The estimation of per capita utilization based on the collaborating center’s population using MSAs is limited. This method does not account for variations in cancer incidence and type across different geographic areas, both of which influence the need for OTC. Adjustment by cancer incidence rates could not be conducted because approximately 30% of patients in our cohort had non-malignant disorders with gonadotoxic preparations for bone marrow transplant. Additionally, patients who traveled from outside the MSA to the providing center may be misrepresented. As a result, the findings regarding the impact of socioeconomic status on OTC utilization may not be fully generalizable. We suggest conducting additional studies based on further data sets in other geographic areas to validate and expand upon these findings. Finally, the utilization analysis was based on a relatively small subset of patients treated exclusively at UPMC, limiting the strength and generalizability of these findings. Larger studies that include patients from their first inquiry within an FP program are needed to validate these observations.
Conclusions
Patients face numerous barriers to comprehensive cancer care, including FP, that can impact quality of life after cure. Major metropolitan areas in the United States offer different coverage options for young patients requiring OTC. We learned that when payment is required, the per capita utilization of OTC is less than half of the per capita OTC utilization when the costs are funded. In addition, patients who pursue OTC tend to live in areas (zip codes) with higher socioeconomic status (lower DCI). This results in a double disparity for those living in areas without Center-funded OTC and with lower socioeconomic resources. This study identified disparities in access to OTC and potential opportunities for strategic change to enhance care equality for young patients. This study also revealed that OTC utilization is lower for the youngest patients. More studies will be needed to understand the basis for this age disparity. We hope that identifying disparities in access to FP health care will lead to policy reforms and other financial assistance mechanisms that improve access to FP care for people in disadvantaged and under-resourced areas.
Authors’ Contributions
In this study, the concept and design were developed by M.S., L.M.W., A.C.Z., and K.E.O., with A.C.Z. ensuring data access and integrity. M.S., A.C.Z., and L.M.W. contributed to the methodology. T.C. conducted the statistical analysis. All the authors contributed to the data analysis and interpretation. M.S. and A.C.Z. wrote and edited the article, while final review, editing, and approval were carried out by K.E.O.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The authors are supported by the Eunice Kennedy Shriver National Institute of Child Health and Human Development (HD114210), the UPMC Magee Center for Reproduction and Transplantation and an anonymous donor to Magee-Womens Research Institute and Foundation.
Data Availability Statement
The data underlying this article will be shared upon reasonable request to the corresponding author.
Supplemental Material
Abbreviations
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.