
Abstract
Background:
Use of cannabis during pregnancy and breastfeeding is increasing. Mental health concerns are reported as common reasons for maternal cannabis use, but little is known about the use of psychiatric medications in this population.
Objectives:
This study aimed to describe psychiatric medication use among pregnant and breastfeeding mothers who used cannabis for mental health concerns.
Design:
Anonymous, online cross-sectional survey.
Methods:
Data were collected from May 2018 to August 2019 among pregnant and breastfeeding mothers who used cannabis. This study included mothers who reported cannabis use for mental health concerns (n = 1363). The survey assessed the timing of cannabis use (during pregnancy and/or lactation); use of cannabis to address depression, posttraumatic stress disorder, or anxiety; use of psychiatric medications; psychiatric distress (Patient Health Questionnaire-4); and demographic information. Differences between groups were examined using t-test and chi-square test in SPSS.
Results:
The mean age was 29.7 years; most were married (62%); 74% were White non-Hispanic, 9% Hispanic, and 17% Black, Indigenous or other People of Color. Mental health symptoms prompting cannabis use included anxiety (96%), depression (75%), and posttraumatic stress disorder (36%). Only 24% of respondents (n = 322) reported concomitant use of psychiatric medications, primarily selective serotonin reuptake inhibitors (72%, n = 232) and benzodiazepines (21%, n = 68). The composite Patient Health Questionnaire-4 showed most respondents had no (61%) or mild (27%) psychological distress; 14% screened positive for depression; and 17% screened positive for anxiety. Respondents who used psychiatric medications more often screened positive mental health concerns.
Conclusion:
Most mothers who used cannabis for mental health concerns were not taking psychiatric medications. This may be due to a mismatch between perceived mental health and screening results, un- or under-treated mental illness, or preference for cannabis over psychiatric medications. Improved management of perinatal mental health and effective patient education about risks of cannabis versus medication use are needed.
Introduction
The legalization of cannabis across 33 states in the United States and other countries has increased cannabis use and changed perceptions toward this practice. 1 A study using data from the National Survey on Drug Use and Health indicated that from 2005 to 2012, the number of individuals who used cannabis and believed cannabis use to be safe during pregnancy increased from 25.8% to 65.4%. 2 Data from the 2017 Pregnancy Risk Assessment Monitoring System (PRAMS) showed that 9.8% of women self-reported cannabis use before pregnancy, 4.2% during pregnancy, and 5.5% after pregnancy. 3 Coy et al. 4 further analyzed the PRAMS data and found that out of the 5.5% that used cannabis postpartum, 47.2% did so while breastfeeding. Cannabis use during the perinatal period is of concern because early prenatal exposure to cannabis can affect the development of the endocannabinoid system which can impact the development of executive function and regulation of the emotional system and cognition in the offspring. 1 Gestational cannabis exposure has been associated with decreased time in a quiet sleep state, tremors, a decrease in the early cognitive performance of infants, as well as adverse effects on sustained attention and short-term memory. 5 Furthermore, it is known that the psychoactive component of cannabis, delta-9-tetrahydrocannabinol, transfers into breast milk, which may impact postnatal brain development.6,7
Some pregnant and breastfeeding women use cannabis to manage symptoms of depression and anxiety.8 –10 An estimated 18% of women are diagnosed with depression before becoming pregnant, and an additional 8%–13% of women are diagnosed with depressive or anxiety disorders during pregnancy.11,12 Kaiser Permanente published data showing that women with a history of trauma, high depression scores, and/or an anxiety diagnosis were more likely to test positive for cannabis use during their pregnancy.13,14 Similarly, the National Survey on Drug Use and Health indicated that women diagnosed with depression were three times more likely to use cannabis while pregnant. 15 One study found individuals who used cannabis perceived a 50% reduction in depression and a 58% reduction in anxiety and stress after use, but the long-term baseline levels of depression increased over time. 16
Pharmacologic treatments for mental health conditions include first-line medications like selective serotonin reuptake inhibitors (SSRIs). However, mental health problems are often undiagnosed or untreated either because mental illness is not recognized among perinatal women, because they opt for nonpharmacologic treatments, or because they are unable or unwilling to use medications.17,18 To compound this, many overestimate the potential risks of antidepressant use in the perinatal period while underestimating the risks of untreated depression. 19 A qualitative study among pregnant women who used cannabis reported that women may either stop or refuse to start taking antidepressants during pregnancy in an effort to avoid side effects due to the “chemical” nature of medications. 9
It is unknown whether or to what extent psychiatric medications are used among pregnant and breastfeeding mothers who also use cannabis for mental health concerns. Understanding the concurrent use of these drugs will provide information that may guide healthcare professionals in counseling about cannabis use and treatment of mental health concerns during pregnancy and postpartum. This study aimed to describe the use of psychiatric medications among mothers who used cannabis to address a mental health concern.
Method
Survey development and recruitment
An online survey was developed by researchers specializing in psychology, pharmacology, lactation, and obstetrics and gynecology to collect cross-sectional data from mothers who used cannabis during pregnancy or lactation. It was pretested and revised based on feedback from 300 mothers who had used cannabis while pregnant or breastfeeding. 10 The final survey contained 88 questions (some with multiple parts) that were mostly multiple choice in 8 sections: eligibility screening, demographics, pregnancy history, infant-feeding, infant sleep, cannabis use, use of other substances and medications, and emotional and mental health. An open-ended question was provided at the end of the survey, which is not reported here (full survey provided in Supplement 1). Several questions required responses to continue with the survey; however, most questions were optional, allowing respondents to skip questions that they were not comfortable answering; this was described to survey respondents in the introduction page prior to beginning the survey. The survey was completed anonymously, no personal identifiers were collected, and no incentives were provided for completing the survey. The survey was conducted using Qualtrics (Qualtrics, Provo, UT), and it limited completion from an IP address to a single submission to prevent multiple participation.
The survey was distributed through the InfantRisk Center website from May 2018 to August 2019. A combination of convenience and snowball sampling was used. The survey was shared via the InfantRisk Center’s website and social media page, and social media pages from one of the authors (K.K.-T.). Participants were recruited through a Facebook group that supported mothers using cannabis during pregnancy and breastfeeding. We also asked individuals to share the link and further distribute the survey. Completion of the survey was considered as consent to participate. The Checklist for Reporting of Survey Studies (CROSS) guidelines were followed. 20 This study was approved by the Institutional Review Board (IRB) at Texas Tech University Health Sciences Center (A18-4037).
Sample
Demographic data collected included mother’s age, number of children, age of the youngest child, educational attainment (high school or less, some college, bachelor’s degree or higher), marital status (married or partnered, single, or other), and the use of tobacco (yes/no) or alcohol (yes/no). Detailed race and ethnicity data were collected; due to low numbers in many racial and ethnic groups, they were combined into three categories: (1) White non-Hispanic, (2) Hispanic, and (3) Black, Indigenous, and people of color (BIPOC). The IRB specifically requested that the survey not ask about the respondents’ state of residence because cannabis is not legal throughout the United States and they feared there might be legal consequences for participants, particularly for pregnant and breastfeeding mothers.
Individuals included in the study were mothers of at least 18 years of age who used cannabis during pregnancy or while breastfeeding. The survey received a total of 2165 responses. From the total pool of responses, 246 did not meet the inclusion criteria (244 answered ⩽1 question, 2 respondents were <18 years of age). Of the remaining 1919 respondents, 263 were excluded due to excess missing data. Another 293 were excluded because they did not report using cannabis to address a mental health concern (Figure 1). The final analyses were conducted using a sample size of N = 1363.
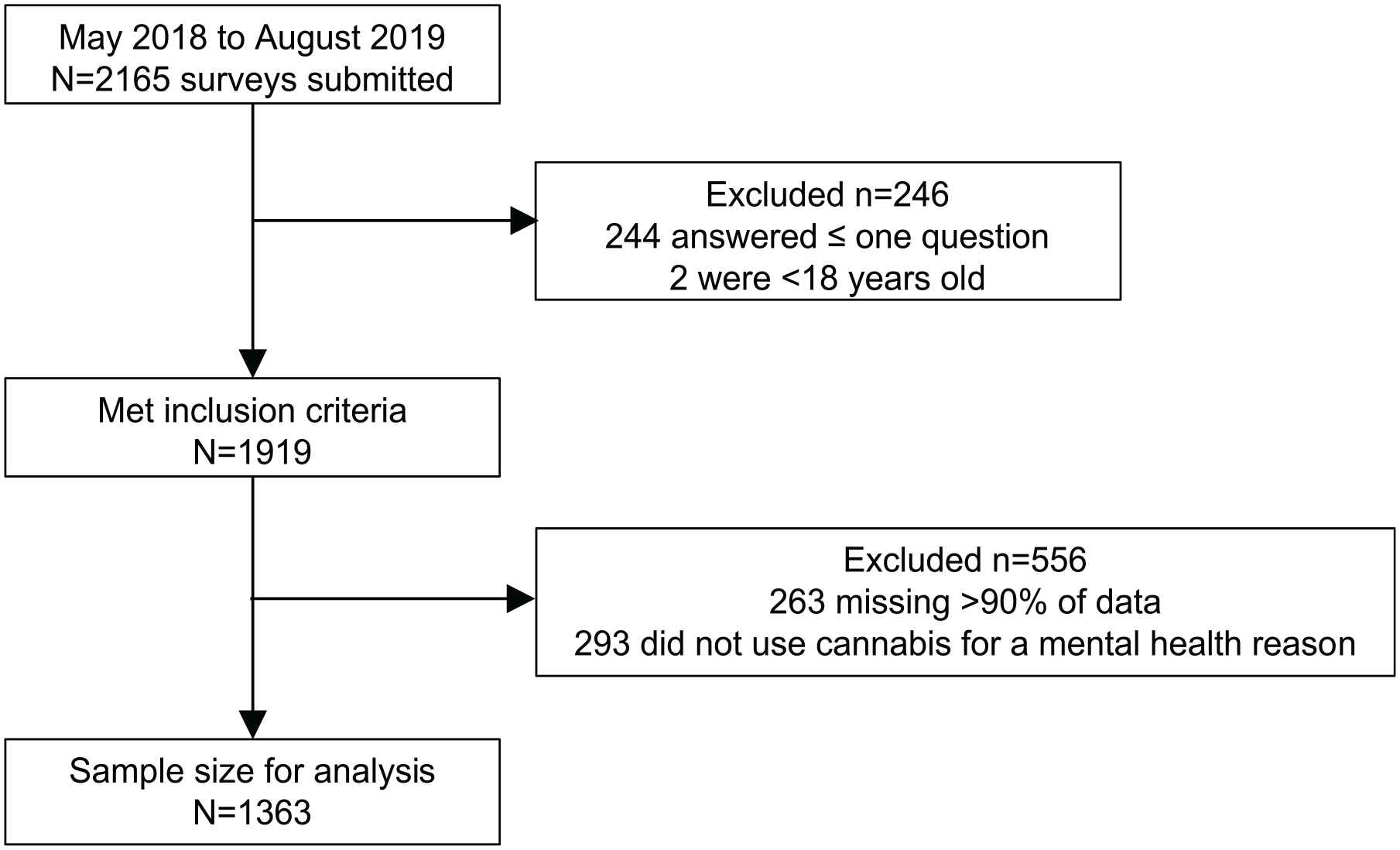
Flow diagram for study sample based on inclusion and exclusion criteria.
Measures
Cannabis use
Questions were developed for this survey that asked about reasons for cannabis use, frequency and timing of cannabis use, and use of psychiatric medications. The survey asked mothers whether they used cannabis during pregnancy, breastfeeding, or both. Mothers were also asked whether they considered cannabis a “more natural alternative to medications.” The frequency of cannabis use was ascertained from two questions that assessed the number of times per week and number of times per day that cannabis was used. They were categorized as less than daily (<7 times per week), low daily (1–3 times per day), or high daily (4 or more times per day). Mothers were also asked about conditions that they might be using cannabis to treat. They were given a list of symptoms and asked to check all that applied. Options included: anxiety, depression, PTSD, or other health concerns. A subsequent question asked respondents to indicate from a list of 26 common psychiatric medications, any medications that were taken to address mental concerns. Respondents could select all that applied and were provided an “other” category with the opportunity to write-in other medications.
Patient Health Questionaire-4
The Patient Health Questionaire-4 (PHQ-4) was included as a screen for anxiety and depression. The PHQ-4 is a measure that combines the PHQ-2 with 2 items from the Generalized Anxiety Disorder-2 (GAD-2) Scale. The GAD-2 accurately predicted generalized anxiety disorder, panic disorder, and social anxiety disorder. 21 Several recent studies have validated its use with pregnant and postpartum women including the Listening to Mothers in California survey (N = 2539), which found it valid for all mothers in their sample including racial/ethnic minorities. 22 A study from Spain also validated the PHQ-4 for pregnant women, comparing it to the PHQ-9 and PHQ-2. 23 The PHQ-9 was originally validated in both a primary care sample and a sample of obstetricians/gynecologists patients (N = 3000 in both groups). 24 Finally, a study from rural Pakistan of women at risk for postpartum depression found that it had “excellent psychometric properties to screen for perinatal depression,” with a sensitivity of 93.4% and a specificity of 91.7%. 25
The PHQ-4 was analyzed separately for depression and anxiety screening and as a composite score. 21 Positive depression screening was considered a score of ⩾3 on the PHQ-2 questions. Positive anxiety screening was defined as a score of ⩾3 on the GAD-2 questions. For the composite score, responses were classified as having no psychological distress (PHQ-4 score of 0–2), mild psychological distress (PHQ-4 score of 3–5), moderate psychological distress (PHQ-4 score of 6–8), or severe psychological distress (PHQ-4 score of 9–12). 21
Statistical analyses
In this descriptive study, means and standard deviations were used to describe continuous variables. Frequencies were used for categorical variables. Differences between the mothers who used psychiatric medications and those who did not were assessed using t-tests and Chi-square tests. Missing data in research on substance use is a known challenge. 26 Missing data of <8% was considered acceptable. Two variables exceeded this threshold: PHQ-4 (n = 170, 12%) and frequency of cannabis use (n = 150, 11%). Data were differentially missing for PHQ-4 between those who did (6%) and did not (15%) use psychiatric medications (Chi-square 18.3, p < 0.001). Data were also missing for frequency of cannabis use between those who did (8%) and did not (12%) use psychiatric medications (Chi-square 4.5, p = 0.03). In consideration of data justice for our population, we assume that these data are missing completely at random rather than omitting participants with missing data. 26 All analyses were conducted using IBM SPSS Statistics Version 28.0 (Armonk, NY: IBM Corp.).
Results
Demographics
The mean age of respondents was 29.7 (SD 5.9) years and the average age of first cannabis use was 16.6 (SD 4.0) years. The majority of the sample (75%) used cannabis during both pregnancy and breastfeeding, and the majority (74.3%) identified as White non-Hispanic. A large portion of the sample (43.7%) reported alcohol use, while 16.4% reported using tobacco. Demographics of the sample are presented in Table 1. The sample was primarily recruited from a Facebook group that supports pregnant and breastfeeding women in their cannabis use. A link for the survey was also posted on the InfantRisk website and on social media of one of the authors (K.K.-T.).
Characteristics of respondents by use of psychiatric medications.

BIPOC: Black, Indigenous, and people of color.
Continuous variable p-values are from t-tests, categorical variable p-values are from chi-squares; the bold p-value indicates statistical significance.
Use of cannabis for mental health concerns
Cannabis was used by 96% (n = 1301) of the sample for anxiety, 75% (n = 1028) for depression, and 36% (n = 494) for PTSD (Figure 2). The overwhelming majority (98.7%) believed that cannabis was a more natural alternative to medications.

Proportion of respondents (N = 1363) self-reporting mental health symptoms and their use of cannabis alone or cannabis with psychiatric medications. PTSD = posttraumatic stress disorder.
Use of psychiatric medications
Just under one-fourth of respondents (24%, n = 322) concomitantly used psychiatric medications. SSRIs (n = 232) were the most commonly used psychiatric medication, followed by benzodiazepines (n = 68) (details of medications reported in Table 2). Of the individuals taking psychiatric medications, 241 reported taking one psychiatric medication, 61 reported taking two, and 20 reported taking three or more medications.
Psychiatric medications used by survey respondents.

Women who used psychiatric medications and those who did not were similar in demographic characteristics. Age of first cannabis use was the only significant difference (Table 1). Those who used psychiatric medications first used cannabis at a slightly older age (17.2 ± 4.7 years) than those who did not use psychiatric medications (16.5 ± 3.8 years) (p = 0.01). Few other differences existed between these groups. Tobacco use tended to be higher among respondents who used psychiatric medication, but this was not significant (p = 0.052). There were slight differences in race/ethnicity between these groups (higher proportion of White non-Hispanic respondents using psychiatric medications); however, this was not statistically significant (p = 0.07).
Current depression and anxiety
Among the participants who completed the PHQ-4 (n = 1193), responses ranged the full spectrum of possible composite scores from 0 to 12. Of the total sample 14.2% screened positive for depression, 17.3% screened positive for anxiety, and 22% screened positive for one or both of these. The proportion who screened positive was significantly different by psychiatric medication use group; 31% screened positive among those who used psychiatric medications versus 20% among those who did not (Chi-square 16.0, p < 0.001).
Based on composite PHQ-4 scores, 60.7% of the total sample (n = 725) were categorized as having no psychological distress, 26.6% (n = 318) as having mild distress, 9.6% (n = 114) as moderate, and 2.7% (n = 36) as having severe psychological distress (Figure 3). Regardless of psychiatric medication use, the majority of respondents fell within the categories of no psychological distress or mild psychological distress. There was a statistically significant difference in the distribution of psychological distress (as categorized by PHQ-4; Chi-square 32.8, p < 0.001) between mothers who used cannabis with versus without psychiatric medications (Figure 3). Larger proportions of the mothers taking psychiatric medications had moderate or severe psychological distress. Among those with moderate or severe distress, 44% (n = 50) and 36.1% (n = 13), respectively, also used psychiatric medications. The missing data between those who did and did not use psychiatric medications limits our ability to draw conclusions about these observed differences.

Proportion of respondents who screened for differing degrees of psychological distress (none, mild, moderate, or severe) according to PHQ4 survey, and their use of cannabis alone or cannabis with psychiatric medications. Note: Distributions were tested for differences via Chi-square. Chi-square 32.8, p < 0.001.
Discussion
Among a sample of pregnant and breastfeeding women who used cannabis to address a mental health concern, only a quarter used a psychiatric medication. Mirroring these findings are those from the general population where mental illness is often not treated with medications or left untreated. According to the National Alliance on Mental Illness, 1 in 5 US adults experience some type of mental illness. 27 Yet, only 46% of those affected received treatment in 2020. 27 In the United States, 19% (48 million people) have anxiety, 8% (21 million people) have depression, and 3.6% (9 million people) suffer from both of these conditions in a given year. 27 Prevalence among perinatal individuals is similar, with 1 in 5 women experiencing mental health problems like depression, anxiety, PTSD, or obsessive-compulsive disorder. 28 The numbers rise considerably if women experience violence or are from a high-risk group. 29 Byatt et al. 30 reported that 75% of women with mental health problems do not receive treatment. This is consistent with our findings.
The high proportion of reported mental distress is particularly concerning because of the increased risks to both mother and infant after perinatal women screen positive for depression and/or anxiety. 31 However, only 22% of women who screen positive for depression actually follow through with the referral.30,32 In our study, only 25% of the pregnant and breastfeeding women who used cannabis to treat depression or anxiety also used a psychiatric medication. This meant that either mothers were untreated, they used non-pharmacologic treatment (such as psychotherapy), or they self-medicated with cannabis.
For women taking medications, stopping during pregnancy is risky. Womersley et al. 33 concluded that women who discontinued their antidepressants while pregnant were three times more likely to struggle with a subsequent episode of depression compared to those who continued their treatment throughout their pregnancy. Untreated depression during pregnancy is associated with increased risk of preeclampsia, preterm birth, low birth weight, inadequate diet, and failure to seek prenatal care. 18 Furthermore, untreated mental illness has also been associated with increased risk of fetal harm due to increased use of substances like caffeine, tobacco, alcohol, and recreational drugs. The effects of untreated mental illness can be so devastating that a 20% increase in suicide attempts has been noted among adolescent mothers.12,18,33
Major medical organizations provide little direction regarding the pharmacological treatment of mental health disorders, with statements supporting psychopharmacology for “some pregnant patients” or upon an individualized consideration of risks and benefits. 34 This lack of concrete direction may contribute to physician uncertainty about recommending pharmacologic options when offering interventions for mental illnesses perinatally. 35
A 2012 study of postpartum depression found that women were more likely to be prescribed medication treatment (with or without counseling) if their medical practice received specialized training. 36 A 2022 review on the knowledge, attitudes, and decision-making process of patients and providers regarding antidepressant use during pregnancy found that while physicians were confident in these skills, many overestimated the teratogenic risk, and between 20% and 74% avoided starting an antidepressant during pregnancy. 35 Furthermore, between 24% and 47% would recommend discontinuing antidepressant use once pregnant. 35 Clearly, there is a wide range of opinions among physicians regarding this topic. Ultimately, such variations in practices based on provider beliefs, comfort levels, and a lack of guidance of high-quality recommendations leave many women untreated for depression. 35
All mothers in our sample reported using cannabis to address mental health concerns, yet less than a quarter screened positive for anxiety or depression, and 88% were classified as having mild or no psychological distress in the composite PHQ-4. Although substantial differentially missing data for PHQ-4 limits our ability to draw conclusions about psychological distress between those who did and did not use psychiatric medications, the rate of self-reported symptoms (100% of the sample) is higher than it appeared on the PHQ-4. This mismatch between PHQ-4 results and self-report can be easily explained. First, the PHQ-4 asks about symptoms in the past 2 weeks. The questions about health issues that mothers treated with cannabis could have occurred at any time. That number, by definition, will be higher than a scale that focuses only on current symptoms. Second, this mismatch may result from the way that the word “depression” is used by laypeople to describe feeling down or sad, and “anxiety” may be used to describe stress rather than pathological depression or anxiety which have clearly defined criteria according to the DSM-5.37,38 Third, their treatments (pharmaceutical, cannabis, or other) may have been effective, meaning that they were not depressed or anxious when they completed the survey.
Regarding the low rate of use of medications, many mothers and providers fear the effects of psychiatric medication on the fetus or infant, or they are concerned about pressure to take these medications. 39 Womersley et al. 33 found that only 33% of women thought it was acceptable to use SSRI medications during pregnancy. Colaceci et al. 40 found that attitudes about psychiatric medications among breastfeeding mothers fell into one of the three categories: to discontinue breastfeeding to take their medication, to “endure the pain,” or to use natural products that they believe are safer than prescribed pharmacologic agents. 40 In a qualitative study, many women described choosing to use cannabis over acetaminophen or psychiatric medications, in an effort to avoid “chemicals” or side effects from a medication. 9
In contrast, some pregnant or lactating women perceive cannabis as a natural alternative to medications.9,40 This perception was prevalent in our sample and could help explain why the majority of respondents were not taking psychiatric medications despite reporting mental health concerns. Chang et al. 9 found that many mothers were aware of the risks and, thus, avoided smoking tobacco during their pregnancy, even though it is natural; conversely, they continued cannabis use, reporting limited knowledge or no knowledge of the potential risks. 9 Women in their study believed that cannabis “elevates your mood” while psychiatric medications “suppress your mood” and that the “chemicals [in antidepressant medications] mess with you.” 9 Similarly, a Swedish study by Kvillemo et al. 41 reported that individuals who used cannabis used it to reduce anxiety, associated its use with a “calm and cozy” effect, and believed public health information about its harms were not credible. 41 In our study, some respondents also used other natural medications such as St. John’s Wort (n = 10). St. John’s wort is a flowering plant that is native to Europe and Asia (Hypericum perforatum), and is the most widely prescribed antidepressant in the world. 42
Many societal stressors may contribute to the development or worsening of mental illness perinatally. Risk factors for peripartum depression include lack of social support, financial stress, food insecurity, poor physical health, stressful life events, and intimate partner violence.43 –45 While we may advocate for and aim to address improvements in economic, health, and societal equity, such situations are often inadequately addressed, and pregnant and postpartum individuals experience substantial challenges. If such hardships cause mental distress or illness to the point of self-medicating with cannabis, a conversation about risks and benefits of medications versus cannabis use is warranted.
Healthcare providers should inquire about and address maternal use of cannabis to self-treat mental illness as evidence suggests that it may exacerbate symptoms. 46 Our findings showed that half of the mothers used cannabis daily, with 32.8% using cannabis up to three times daily and 17.6% using cannabis four or more times daily. The National Academies of Sciences, Engineering, and Medicine (NASEM) report that frequent cannabis use, especially with high doses, may cause feelings of anxiety and paranoia. 47 Furthermore, heavy cannabis use is associated with an increased risk of the development of depressive disorders as well as thoughts of suicide, suicide attempts, and death by suicide. 47
Cannabis use can cause neuropsychological impairment, particularly when used during adolescence. Its use can decrease motivation, and heavy use is associated with apathy, and a reduced ability to concentrate, follow routines, or successfully master new content. 48 Notably, these symptoms are similar to those of depression, so it may be difficult to distinguish the symptoms of cannabis use from those of depression. Cannabis use is also associated with cognitive impairment, which may put both the mother and child at risk. Beyond depression, cannabis use is considered a preventable risk factor for psychosis. 49 The age of onset of psychosis appears to be correlated with the age of onset of cannabis use. 48
The effect of in utero exposure to cannabis on the cognitive development of the offspring remains unclear as methodological challenges of studies to date limit the conclusions which can be drawn.50 –52 Importantly, a lack of clear data in humans does not equate to a lack of risk. Animal studies, which tend to use higher doses than would be consumed by humans, have demonstrated that prenatal exposure to cannabis increases the excitability of the dopamine neurons in the offspring which may lead to enhanced impulsivity, hyperactivity, loss of sustained attention, and increased sensitivity to drugs of abuse. 53 It is unclear how such findings relate to humans. 54
Some mothers, including in the present study, report using cannabis while pregnant to address anxiety. Unfortunately, some research reports higher anxiety among children exposed to cannabis prenatally. Rompala et al. 55 reported greater anxiety, aggression, and hyperactivity levels in young children exposed to cannabis, as well as alterations in gene expression which may suggest possible mechanisms for these phenotypic differences.55,56 These findings suggest the potential for long-term neurodevelopmental impacts on the next generation, effects that are not widely known by the public. 56
On average, individuals in our sample used cannabis for the first time around the age of 16. This is very similar to the average age of first cannabis use in females across the United States which is 16.3 (SD 3.2). 57 This age may be important because many parts of the brain are still developing during this time and into early adulthood. 58 Research suggests that when comparing the amygdala size of 16- to 18-year-old females, the amygdala volume of those who used cannabis was larger than that of those who did not use cannabis.58,59 This finding is associated with more self-reported depression and anxiety. 58 Similarly, cannabis use can impact the development of the prefrontal cortex, an area of the brain which has been implicated with major depression.58,60
Cannabis–drug interactions have been established in vitro that involve cytochrome P450 (CYP) enzymes, including CYP1A2 and CYP3A4. 61 Based on these data, several drug interactions may exist between cannabis and the medications that our study respondents reported using. Cannabis is a substrate of CYP3A4, and St. John’s Wort, which was used by 10 survey respondents, is a CYP3A4 inducer. The induction of this enzyme may decrease the serum concentration of cannabis, thereby reducing the effects of cannabis in individuals. Cannabis is also a CYP1A2 inducer and may decrease the serum concentration of CYP1A2 substrates, such as duloxetine, clozapine, and olanzapine, potentially decreasing the therapeutic effects of these medications. Though in vivo data on these drug interactions are limited, cannabis smoking cessation is among the implications of two cases of intoxication with CYP1A2 substrates (clozapine and olanzapine).62,63 The subsistence of adverse reactions from cannabis–drug interactions remain unknown, and merit future study.
Although the differences in psychiatric medication use by race/ethnicity in our sample did not reach significance, our sample may not have been large enough to capture possible differences. An analysis of the National Ambulatory Medical Care Survey (NAMCS, 2006–2010) and the National Hospital Ambulatory Medical Care Survey (NHAMCS) demonstrated marked differences in rates of provider-reported maternal depression diagnoses by race during prenatal visits. 64 They found that non-Hispanic White women were more likely to be diagnosed with depression than non-White women (5.7% vs 2.9%). Furthermore, among those with a depression diagnosis, non-Hispanic White women were over three times more likely to report antidepressant use during pregnancy compared to non-White women (adjusted odds ratio [aOR] 3.3, 95% CI 2.1, 5.3). 64 As there are clear influences of race and ethnicity on antidepressant use during pregnancy, the inclusion of cannabis into the discussion also merits further investigation.
Strengths/limitations
A strength of this study is that, to our knowledge, it is the first study to examine psychiatric medication use among pregnant and breastfeeding women who used cannabis. In addition, even after applying exclusions to the sample, a substantially large number (>1000 respondents) remained for analysis. Finally, the use of a validated screening tool for psychiatric distress allowed us to examine whether medication use was related to degree of distress.
This study has several limitations. First, the data were self-reported and subject to recall bias; notably, there was a large range in age of the youngest child, thus substantial time had lapsed for some participants since pregnancy or breastfeeding. Second, the survey did not ask about medication prescriptions or compliance, only use. Misclassification bias may be present for respondents who were prescribed medications but opted not to take them, particularly in the context of demographic analysis such as race and ethnicity. In addition, because this study was a cross-sectional online study, it may have been subject to selection bias because we recruited largely from a group of mothers using cannabis who may not be representative of the population. Most of the respondents of the survey identified as White, so the data are not representative of all mothers who use cannabis to treat a mental health condition. However, the demographics of our sample are consistent with those of the Centers for Disease Control and Prevention in their PRAMS data, which also found higher use among White mothers with low income. 65 Our data, and those of the CDC, may also reflect minority women’s reluctance to report cannabis use in surveys due to fear of possible consequences, such as child removal, and distrust in institutions. Finally, due to the descriptive nature of this study and a dearth of available literature about cannabis and psychiatric medication use among perinatal women, a priori power calculations were not performed. Future studies may use these data from our descriptive research to power a study to more thoroughly examine differences among perinatal women who use cannabis to address mental health concerns.
Conclusion
Of 1363 respondents who used cannabis to address perceived mental health concerns, more than 75% of these respondents did not use prescription psychiatric medications. The low rate of prescribed psychopharmacotherapy could suggest that patients are undiagnosed and untreated, or that these women may have opted to use nonpharmacologic methods, such as psychotherapy, exercise, acupuncture, or support groups. 66 All of these methods effectively treat even major depression in perinatal women.
As for medications, prescribers are often reluctant to treat pregnant and postpartum women with psychiatric medications because of possible effects on the fetus or infant. This hesitation about pharmacotherapy may create a barrier to care so mothers use cannabis as their primary psychiatric drug. Simultaneously, women who use cannabis during the perinatal period usually believe it is a safe and effective alternative to traditional medicine, reflecting a lack of accurate information and knowledge among perinatal women. Focused education should be a high priority for mothers who use cannabis to address mental distress; an emphasis should be placed on the increased risk of anxiety and poorer mental health of children exposed to cannabis during development.
Coordination of care between obstetricians/gynecologists and mental health professionals will be key to addressing appropriate screening and treatment of mental illness among pregnant and breastfeeding women. Building trust between the mother and provider is crucial to foster open conversations about cannabis use. Rapport-building is especially necessary because women who use cannabis while pregnant or breastfeeding may perceive it as safe. Future studies should identify the best strategies to educate mothers on the risks of cannabis use during the perinatal period and improve the identification of mental health concerns and guidance for health professionals to address mental health concerns among perinatal women.
Supplemental Material
sj-docx-1-whe-10.1177_17455057231199391 – Supplemental material for Psychiatric medication use among pregnant and breastfeeding mothers who used cannabis for mental health concerns: A cross-sectional survey study
Supplemental material, sj-docx-1-whe-10.1177_17455057231199391 for Psychiatric medication use among pregnant and breastfeeding mothers who used cannabis for mental health concerns: A cross-sectional survey study by Diego Regalado, Meghan E. Connolly, Kaytlin Krutsch, Amy Stark, Kathleen Kendall-Tackett and Christine D. Garner in Women’s Health
Supplemental Material
sj-docx-2-whe-10.1177_17455057231199391 – Supplemental material for Psychiatric medication use among pregnant and breastfeeding mothers who used cannabis for mental health concerns: A cross-sectional survey study
Supplemental material, sj-docx-2-whe-10.1177_17455057231199391 for Psychiatric medication use among pregnant and breastfeeding mothers who used cannabis for mental health concerns: A cross-sectional survey study by Diego Regalado, Meghan E. Connolly, Kaytlin Krutsch, Amy Stark, Kathleen Kendall-Tackett and Christine D. Garner in Women’s Health
Footnotes
Acknowledgements
The authors acknowledge Teresa Baker, MD, and Thomas W. Hale, PhD, RPh, Professors at Texas Tech University Health Sciences, School of Medicine, and Christina Young, MD, and Allison McBrayer, MD, who were at the time Medical Students at Texas Tech University Health Sciences Center, for their role in the development of the data collection instrument.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.