
Abstract
Background:
Hip arthroscopy is technically demanding with a steep learning curve, and labral repair is an important component of the surgical treatment of femoroacetabular impingement (FAI) syndrome. As hip arthroscopy indications and techniques are evolving, it is important to remain focused on teaching techniques that are easily mastered and have a measurable benefit to patient outcomes.
Indications:
Patients with FAI syndrome and labral tear who have failed conservative treatment may benefit from hip arthroscopy, labral repair, and femoroplasty.
Technique Description:
Labral repair is an essential component of the surgical treatment of FAI syndrome. The hip is accessed in standard fashion, and multiple knotless anchors are used for labral repair. Repair sutures are passed around the labrum in an inverted fashion. This inversion technique ensures the labrum is not everted away from the acetabular rim and that the final position of the labrum will restore a good suction seal on the femoral head. Femoroplasty and capsule closure are always performed.
Results:
Patients can reliably expect improvements in hip pain and function. A cohort of 62 patients was investigated, and these patients demonstrated significant improvement in multiple patient-reported outcomes related to physical function, activity, and pain at 2 years after hip arthroscopy. Forty-seven percent stated they felt “completely better” at 2 years postoperatively.
Discussion/Conclusion:
Good hip arthroscopy technique in the proper patient can yield excellent results. The inversion labral repair technique reliably restores the suction seal and prevents eversion of the labrum to preserve normal function.
Patient Consent Disclosure Statement:
The author(s) attests that consent has been obtained from any patient(s) appearing in this publication. If the individual may be identifiable, the author(s) has included a statement of release or other written form of approval from the patient(s) with this submission for publication.
This is a visual representation of the abstract.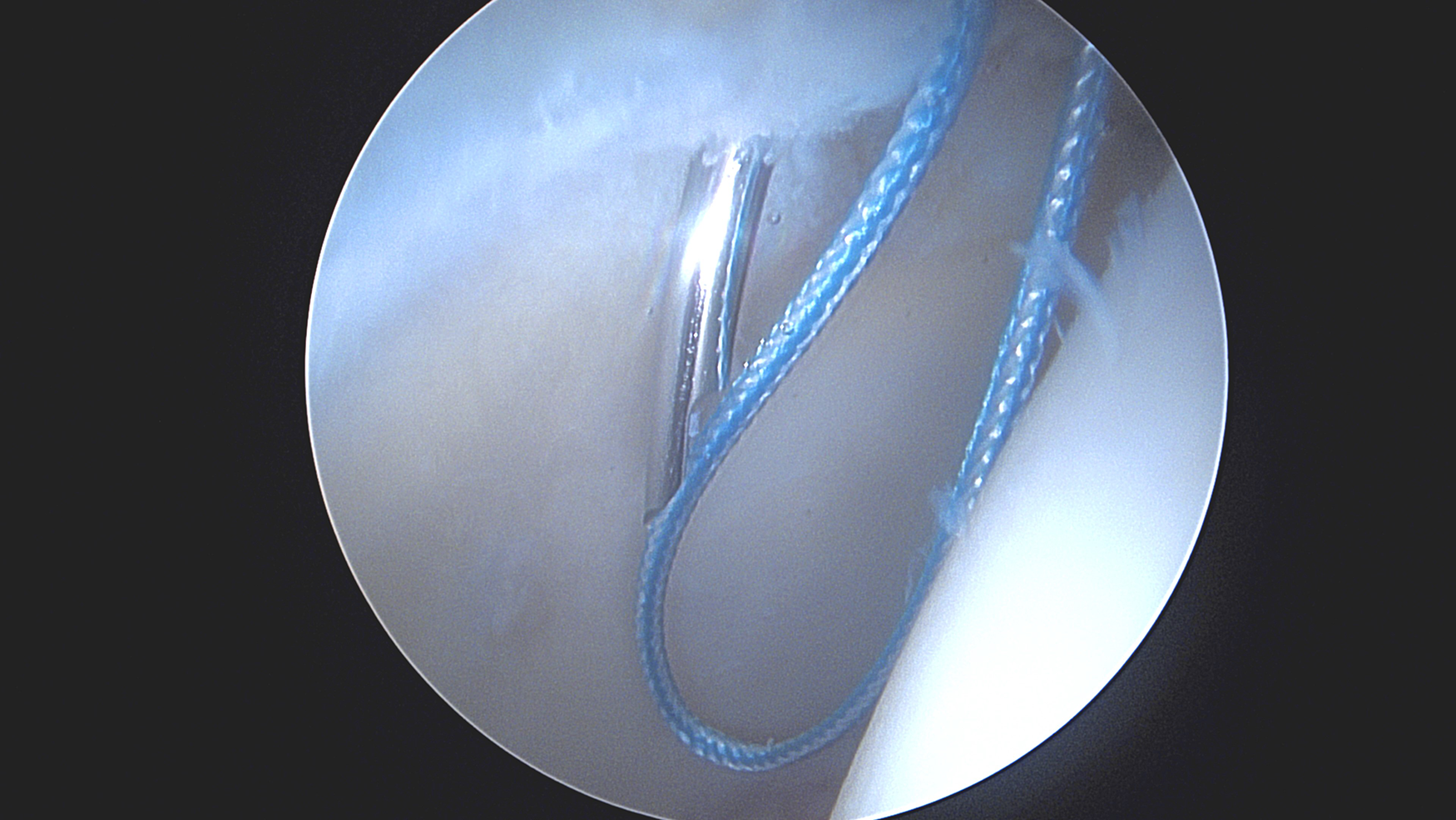
Video transcript
This is a presentation from the University of Maryland School of Medicine on Knotless Labral Repair Using the Inversion Technique in Hip Arthroscopy. Our authors have nothing to disclose.
Background
The prevalence of hip arthroscopy is growing and has increased by 85% between 2011 and 2018 in the United States. 7 Hip arthroscopy is technically demanding with a steep learning curve, and labral repair is an important component of surgical treatment of femoroacetabular impingement (FAI) syndrome.4,6 Re-establishing the labral suction seal on the femoral head is essential for optimizing hip biomechanics and improving stability.1,5 As hip arthroscopy indications and techniques are evolving, it is important to remain focused on teaching techniques that are easily mastered and have a measurable benefit to patient outcomes.
To highlight our labral repair technique, we present a case of a 30-year-old male with left hip pain. Dunn 45 pelvis radiograph demonstrates large cam lesions bilaterally. Magnetic resonance imaging (MRI) of the left hip demonstrates tearing of the anterior and superior labrum. This patient was diagnosed with FAI syndrome and labral tear.
Indications for surgery in this patient are failure to improve with 6 weeks of hip-specific physical therapy and anti-inflammatory medication. The contraindications to hip arthroscopy are dysplasia and osteoarthritis, with specific measurements shown here. Typical measurements for dysplasia are a lateral center edge angle less than 25°, anterior center edge angle less than 25°, and Tonnis angle >10°.
Technique Description
A hip distractor extension is placed on a regular operating room (OR) bed and a friction foam pad is used to provide traction. The C-arm comes in perpendicular from the contralateral side. After the hip is prepped and draped, the greater trochanter is marked out by palpation as well as the anterior superior iliac spine (ASIS) and a medial “do not cross” line going distally. The anterolateral portal is marked out just anterior and proximal to the anterior corner of the greater trochanter. The mid-anterior portal is marked halfway between the anterolateral portal and the ASIS line, and the distal anterolateral accessory (DALA) portal is marked. Finally, a posterolateral portal at the posterior superior aspect of the greater trochanter is used if labral reconstruction is necessary. The hip is accessed in standard fashion.
An arthroscopic ablation device is used to develop a plane between the capsule and the labrum. A 4-mm round bur is used to prepare a bony bed for anchor placement. An all-suture knotless anchor is placed through the DALA portal. Drilling is done under direct arthroscopic visualization and is confirmed fluoroscopically to ensure proper placement. Placing the anchors through the DALA portal improves the trajectory to avoid intra-articular penetration while also allowing the anchor placement to be close to the edge of the acetabular rim. This placement helps with maintaining the labrum on the rim for the suction seal on the femoral head. After the anchor is seated by pulling tension, a looper is introduced through the mid-anterior portal, and the blue repair stitch is pushed into the joint for easy retrieval. A suture passer is introduced through the mid-anterior portal and used to pierce the labrum from outside to inside at the chondrolabral junction. This pass is used to pass the repair stitch around the labrum in an inverted fashion. The looper is used to retrieve the repair stitch. The looper is then introduced through the DALA portal and used to retrieve the repair stitch that has been passed and the shuttling stitch. The repair stitch is then guided with a probe and tensioned appropriately. Due to the inverted direction of passing the repair stitch, the labrum rolls nicely toward the articular surface when tensioned. Passing is done in this inversion technique to avoid eversion of the labrum. The standard passing technique shuttles the repair suture in the opposite direction and can have the tendency to evert or pull the labrum up and away from the acetabular rim. Eversion of the labrum leads to a gap between the femoral head and the labrum, thus losing the suction seal effect of a normal or well-repaired labrum. The inversion technique ensures the suction seal between the labrum and femoral head is restored. Re-establishing a suction seal is important for optimizing hip biomechanics and improving stability.1,4 The tail of the repair stitch is then cut flush.
These anchors are preferred because the pilot hole is quite small at 1.8 mm allowing more points of fixation along the length of the tear, and because of the ease of use for precise tensioning of the labrum. In this patient, 3 suture anchors are used to provide adequate fixation for the length of the tear. To determine the entire length of the tear requiring repair, chondrolabral junction injury, intrasubstance labral injury, and acetabular articular cartilage injury are all considered. The number of suture anchors used is based on the length of the tear with anchors typically spaced about 8 mm apart. Anchors are typically placed anteriorly first, then progressively superior, and finally posterior if needed. Traction is removed and the suction seal between the labrum and the femoral head is clearly visualized without any gapping. This inversion method controls the final position of the labrum well and avoids unwanted eversion.
This video demonstrates the same inverted repair technique in the right hip of a different patient. A looper is introduced through the mid-anterior portal, and the blue repair stitch is pushed into the joint for easy retrieval. A suture passer is introduced through the mid-anterior portal and used to pierce around the labrum from outside to inside, and this pass is used to retrieve the repair stitch from around the labrum. Using the mid-anterior portal provides the optimal trajectory for passing around the labrum. The looper is used to retrieve the repair stitch. The looper is then introduced through the DALA portal and used to retrieve the repair stitch that has been passed and the shuttling stitch. This can be easily done by pushing all 3 strands into the joint, pulling back on the tail of the shuttling stitch, and only retrieving the desired sutures. This step ensures that sutures are not tangled in the cannula or the deep soft tissues. The repair stitch is then guided with a probe and tensioned appropriately. The DALA portal should be used for the shuttling and tensioning to allow for traction to be pulled in line with the trajectory of the initial anchor placement, which avoids failure of the knotless tensioning mechanism or anchor pull-out. Again, in this inversion technique, the labrum rolls in nicely toward the femoral head due to the inverted direction that the suture was passed around the labrum. Eversion of the labrum from the typical circumferential technique is avoided. Finally, the repair stitch tail is cut flush with the acetabulum above the labrum.
Here, we demonstrate this entire technique one additional time. The circumferential passing of the repair stitch around the labrum is preferred over a labral-based or mattress repair because it does not violate the intrasubstance of the labrum and it provides a robust grasp of the entirety of the longitudinal labral fibers. Passing of the repair stitch in this inverted fashion ensures that the chondrolabral junction is reduced back to the acetabular rim, and that the labrum stays nicely on the edge of the acetabular rim toward the femoral head to re-establish a good suction seal. This is important to optimize hip biomechanics, fluid dynamics, and improve stability.1,5 In summary, the steps in this video, when performed together, demonstrate a unique but easily reproducible and reliable way to ensure restoration of the labral suction seal on the femoral head and to avoid eversion of the labrum that can occur with prior repair techniques. The goal is to appropriately restore the normal labral anatomy and hip stability, and avoid pitfalls related to knotless anchor placement and function.
Intra-articular work is followed by femoroplasty, and the capsulotomy is always closed afterward.
Tips for avoiding potential complications include obtaining adequate hip distraction to avoid chondral injury, and not using a perineal post to avoid nerve complications. It is important to not simply debride the labrum as this has been shown to have inferior outcomes. 3 Labral repair should be performed, and reconstruction can be performed if necessary.2,3 Repairing the capsule is critical for hip stability and good patient outcomes. As with all surgery, proper patient selection is crucial.
Postoperatively, patients are allowed 20 lbs of weightbearing with the foot flat on the ground, for 2 weeks, after which they wean their crutches and progress to weightbearing as tolerated. For the first 6 weeks, patients avoid combined hip extension past neutral and external rotation to protect the capsular repair. Patients are given the medications listed here for pain and heterotopic ossification prophylaxis and follow a progressive rehab protocol. Return to sport can occur as early as 6 months postoperatively, and multiple hip-specific tests and outcome scores are utilized, including resolution of symptoms with sport-specific drills.
Discussion
A cohort of 62 patients demonstrated significant improvement in multiple patient-reported outcomes related to physical function, activity, and pain. Forty-seven percent of the cohort of patients stated they felt “completely better” 2 years postoperatively. Good hip arthroscopy techniques in the proper patient can yield excellent results. The inversion labral repair technique reliably restores the suction seal and prevents eversion of the labrum to preserve normal function. Thank you.
Footnotes
Submitted December 15, 2023; accepted February 28, 2024.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.