
Abstract
Background:
Patellar instability with symptomatic cartilage lesions in young patients is a challenging problem to treat. The use of osteotomies to correct malalignment and fresh osteochondral allograft transplantation (OCA) to address cartilage lesions and patellofemoral dysplasia is a viable treatment option for carefully selected patients.
Indications:
The patient is a 22-year-old woman with medial patellar instability caused by iatrogenic distal femoral external rotation and uncontained grade IV patellofemoral lesions. The patient was indicated for OCA because the lesions were too large for an osteochondral autograft transfer system (OATS) and were uncontained and not amenable to autologous chondrocyte implantation. Bipolar OCA also addresses the patient’s patellofemoral dysplasia by restoring a more morphologically normal patellofemoral joint. The external rotation and mild varus deformity are corrected with a biplanar distal femoral osteotomy. Correction of malalignment is necessary prior to OCA transplantation to avoid abnormal graft loading and thereby decrease the risk of graft failure.
Technique Description:
(1) Diagnostic arthroscopy and fluoroscopic examination under anesthesia. (2) Lateral closing wedge de-rotational distal femoral osteotomy. (3) Bipolar OCA with tibial tubercle osteotomy and removal of hardware.
Results:
In this case, the patient had significant improvement in her symptoms and had full knee range of motion with a normal gait at 3 months after surgery. Depending on a patient’s preoperative function and the specific pathology, full recovery can take considerably longer. A successful outcome is considered return to activities of daily living without significant pain. Return to higher level athletic activities is significantly more unpredictable. Graft survival of bipolar patellofemoral OCA is variable, and the literature is limited by the small number of procedures performed, but published series range from 60% to 85% at 5 years.
Discussion/Conclusion:
A successful outcome in these unique, complex cases depends on good patient selection, preoperative planning, and surgical execution. Patellar instability can be reliably treated when the predisposing anatomical factors are appropriately corrected. Bipolar OCA can provide significant improvement in pain and function, but continues to have the highest rate of graft failure compared with other sites within the knee, and should be considered a salvage operation for patients with significant limitations in activities of daily living.
Patient Consent Disclosure Statement:
The author(s) attests that consent has been obtained from any patient(s) appearing in this publication. If the individual may be identifiable, the author(s) has included a statement of release or other written form of approval from the patient(s) with this submission for publication.
This is a visual representation of the abstract.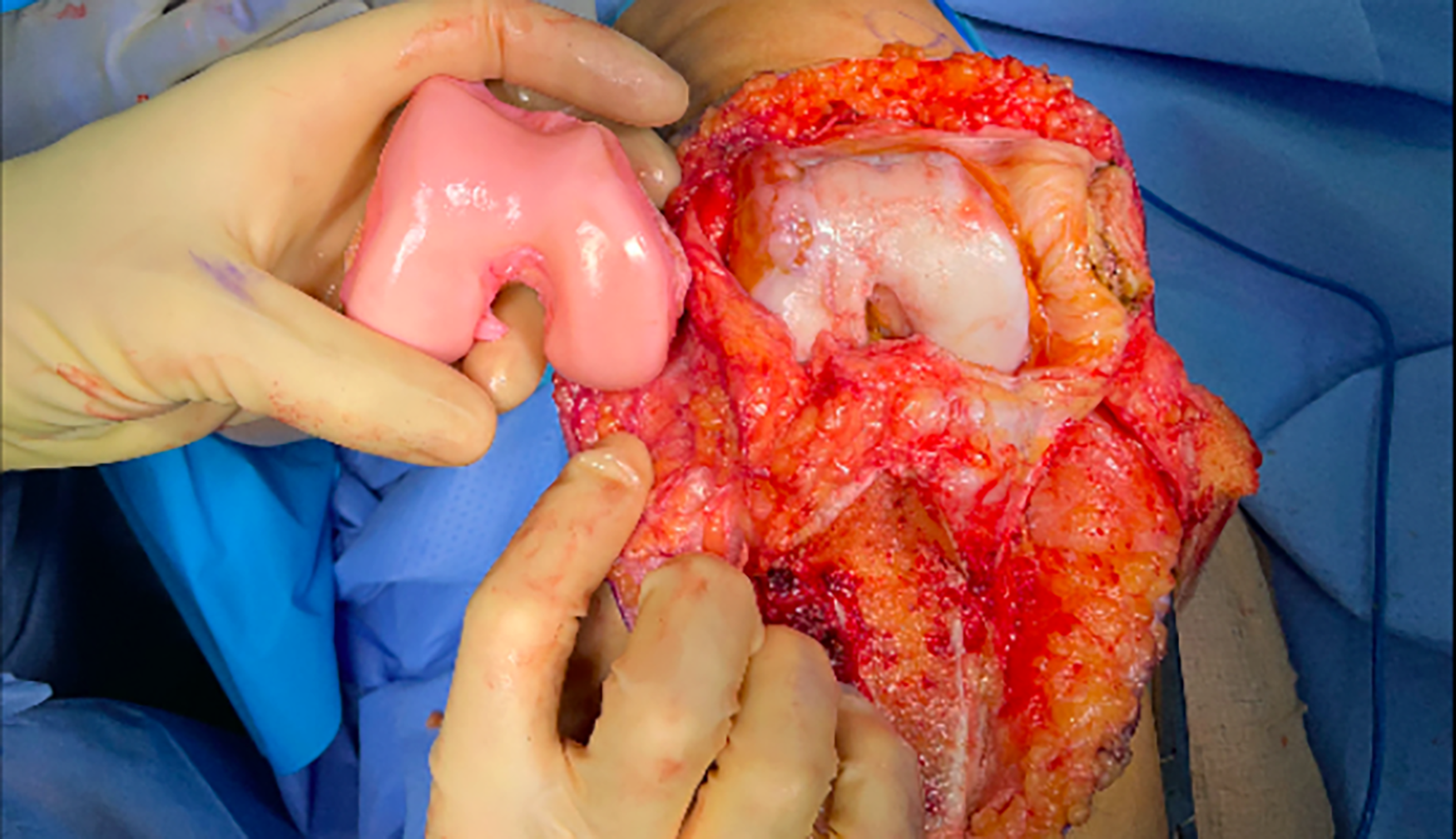
Keywords
Video Transcript
This video will describe a case of medial patellar instability with bipolar patellofemoral cartilage lesions treated with a de-rotational distal femoral osteotomy, osteochondral allograft transplantation (OCA), and tibial tubercle osteotomy (TTO).
Disclosures are as follows and can be found in the American Academy of Orthopaedic Surgeons (AAOS) website.
Background
Medial patellar instability is a rare condition that is usually iatrogenic.6,7,9 Up to 91% of cases are related to prior lateral release surgery. Iatrogenic external rotation of the distal femur is a less common cause that should be considered in patients with a prior distal femoral osteotomy. 10
Bipolar OCA has been used to address both cartilage damage and trochlear dysplasia in patients with patellar instability.
Successful treatment of both patellar instability and cartilage lesions requires careful examination of a patient’s alignment in all planes.1,2,4,5,8
This video will review the workup, surgical planning, and technique used to treat young patient with iatrogenic medial patellar instability and patellofemoral arthritis.
The patient is a 22-year-old female presenting with right knee pain and a history of patellar instability with multiple prior surgeries.
The patient experienced lateral patellar dislocations beginning at age 7 which were treated unsuccessfully with a medial patellofemoral ligament (MPFL) repair. She subsequently underwent a distal femoral and TTO at age 11, which led to partial improvement in her symptoms.
Due to persistent pain, she underwent a diagnostic arthroscopy which revealed significant patellofemoral cartilage damage leading to her referral to our center.
On physical examination, she has increased laxity with a Beighton score of 6.
She has a positive inverted J sign with her patella entering the groove from medially. Her patella has decreased lateral and increased medial translation, while the contralateral side has increased lateral translation. Examination of her hips demonstrates mild increased external rotation and decreased internal rotation compared to the contralateral side.
Initial radiographs demonstrate patellofemoral dysplasia, a positive crossing sign, and mild varus coronal alignment. Her Caton-Deschamps ratio is normal.
A computed tomography (CT) scanogram is obtained to evaluate the patient’s femoral rotation. She is found to have 3° of retroversion compared with 16° of anteversion of contralateral side.
Axial CT demonstrates a severely dysplastic trochlea, making measurement of the tibial tubercle-trochlear groove (TT-TG) distance more unreliable.
The patient is indicated for a diagnostic arthroscopy and examination under anesthesia with fluoroscopy. This allows for accurate determination of the patient’s coronal, sagittal, and patellar stability. Arthroscopy allows for staging of the cartilage lesions and a cartilage biopsy if indicated.
Examination under anesthesia demonstrates less than 2 quadrants of lateral translation, while the patella can be dislocated from the trochlea medially. The patella enters the groove from medial at 45° of knee flexion. Hip examination demonstrates her femoral retroversion.
Arthroscopic evaluation from a superolateral portal with a 70° scope allows excellent evaluation of patellofemoral tracking. Here, the increased medial translation can be appreciated, as well as the decreased lateral translation. Viewing from the lateral recess, the patella can be seen entering from medial. Bipolar grade IV cartilage lesions are confirmed.
The patient has medial patellar maltracking and medial patellar instability caused by iatrogenic distal femoral external rotation and varus from her prior distal femoral osteotomy.
Her patellofemoral joint has bipolar, diffuse grade III with focal grade IV lesions.
There are no degenerative changes or meniscal pathology in the medial or lateral compartments.
Bipolar OCA was chosen to treat the patient’s uncontained grade IV patellofemoral lesions. OCA was chosen because the lesions were too large for an osteochondral autograft transfer system (OATS) and were uncontained and therefore not amenable to autologous chondrocyte implantation. 3 The patient’s young age precluded the use of a patellofemoral arthroplasty. Furthermore, bipolar OCA transplantation would also address the patient’s patellofemoral dysplasia by providing her with a morphologically normal patellofemoral joint.
To address her iatrogenic 20° external rotation deformity and mild varus coronal alignment, the patient was also indicated for a de-rotational, biplanar distal femoral osteotomy. With this degree of femoral malrotation, the senior author has found that isolated soft tissue stabilization procedures are generally insufficient. Furthermore, correction of the patient’s coronal and rotational alignment is necessary prior to proceeding with OCA transplantation to avoid abnormal graft loading and decrease the risk of failure of both grafts.
The osteotomy was planned to match the patient’s contralateral femoral version and to place the patient in a neutral mechanical alignment.
In cases requiring complex, technically demanding biplanar osteotomies, the senior author favors the use of patient-specific instrumentation to allow for more accurate correction in 2 planes.
Technique Description
The patient is positioned supine.
A sterile tourniquet is applied and a subvastus approach is made with a wide surgical exposure to allow placement of the specific cutting guides.
The planned osteotomy is then verified with fluoroscopy.
The osteotomy is made, with care taken to protect the neurovascular bundle.
The correction is made, and the lateral plate is applied.
The stability of the construct allows the patient to be made partial weightbearing with crutches initially and advanced to weightbearing as tolerated 2 weeks after surgery.
Follow-up radiographs at 3 months demonstrate healing of the osteotomy.
Long leg standing views confirm the patient’s neutral mechanical axis.
A CT scanogram is also obtained to confirm the rotational correction and osteotomy healing. On the axial images, the patella now tracks more centrally.
The second stage of the patient’s reconstruction will entail a bipolar OCA transplantation, lateral retinacular imbrication, lateralizing TTO, and possible lateral patellofemoral ligament (LPFL) reconstruction.
The patient is again positioned supine.
A lateral parapatellar arthrotomy is made to allow for later imbrication. The TTO is performed first to allow better exposure. Here, the allograft distal femur can be seen. A jig is used to perform the osteotomy. The patient’s native trochlea is then cut freehand. Matching the native and allograft trochlea is technically demanding and done with sequential freehand modifications. Attention is then turned to the patella. With a native thickness of 20 mm, 10 mm of patella is resected and replaced with a 13-mm-thick allograft plug to account for the flat, dysplastic native patella. The allograft plug is press fit into a socket and reinforced with two 3.5-mm headless compression screws. The trochlear graft is fixed with multiple 4.0-mm headless compression screws. The tibial tubercle is provisionally lateralized. Patellar tracking is checked prior to any retinacular closure. Once the patella is tracking centrally, the osteotomy is fixed and the lateral retinaculum is imbricated. Patellar tracking and stability are again checked to verify no LPFL reconstruction is needed.
A continuous passive motion (CPM) machine and physical therapy are started on post-op day 1. The patient is allowed to be touchdown weightbearing with a brace locked in full extension and crutches. At 2 weeks, gradual advancement to weightbearing as tolerated and full passive range of motion are allowed. Open-chain active extension started at 6 to 8 weeks pending healing of the TTO. At 12 weeks, the goal is for patient to have a relatively normal, pain-free gait, but this is highly variable based on the complexity of the surgical procedures and pre-existing pathology.
Results
Postoperative radiographs demonstrate a centrally tracking patella, stable fixation of the graft, and healing of the TTO.
A CT scan is obtained at 6 months after surgery to check for graft incorporation.
Potential surgical complications are listed here. The patellofemoral joint sees tremendous forces and has the highest reported failure rate for OCA transplantation. Even with excellent surgical planning and execution, bipolar patellofemoral OCAs must be considered a salvage procedure reserved only for patients with severe disability that impairs activities of daily living.
At 4 months after surgery, the patient has a near-normal gait, full range of motion, no recurrent instability, and minimal pain.
Footnotes
Submitted December 13, 2023; accepted January 30, 2024.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.