
Abstract
Background:
Surgical repair of chronic quadriceps tendon ruptures can be daunting, especially after failure of a prior repair. In this setting, tissue quality is usually poor, necessitating graft augmentation. In this video, we describe our technique for Achilles tendon allograft augmentation for revision quadriceps tendon repair.
Indications:
Failed quadriceps tendon repair defined as ongoing extensor mechanism deficit including patella baja, functional deficit, or palpable quadriceps defect with confirmed retear on advanced imaging.
Technique Description:
Patient is placed in the supine position, and a midline incision is extended to the tibial tubercle. Full thickness medial and lateral flaps are raised, nonviable scar tissue is excised, and suprapatellar adhesions are released to ensure full mobilization of the viable remnant quadriceps. A plane is then developed deep to the patellar tendon paratenon from proximal to distal. A reamer is used to prepare a socket just medial to the tibial tubercle. The calcaneal bone block of the Achilles allograft is fashioned to match the recipient site on the tibia with a sagittal saw. The graft is shuttled deep to the paratenon, and the bone plug is fixed to the tibia with an interference screw. Suture from the patellar anchors is then used to place 2 running Krackow stitches spanning the remnant quadriceps tendon proximally. The remnant tissue is subsequently reduced and tied with an anchor pull-through technique. The soft tissue component of the Achilles graft is laid over the repair and oversewn with free nonabsorbable suture. Patient is placed in a brace locked in extension for 6 weeks and allowed to be weight bearing as tolerated.
Results:
Long-term patient-reported outcomes of Achilles allograft reconstruction for revision extensor mechanism repairs are limited. Two studies of 17 reconstructions each reported this to be a reliable and durable option at a mean follow-up of 65 and 52 months, respectively.
Discussion/Conclusion:
Revision surgery for extensor mechanism deficits can be a challenging procedure. Our preference is to perform augmentation with Achilles allograft with bone plug fixation on the tibial side. This allows for augmentation of the entire extensor mechanism, as well as bone-to-bone healing on the tibial side.
This is a visual representation of the abstract.
Video Transcript
This is a technique presentation for revision quadriceps tendon repair augmented with an Achilles allograft to reconstruct the tendon.
Author disclosures are found here as well as available online.
In general, quadriceps tendon tears are more common in men older than 50 years and unfortunately have a relatively high failure rate following surgical fixation. Graft augmentation has been proposed to improve the biology and structural integrity to decrease retear rates, especially in the revision setting.
This example is a 62-year-old man who had a mechanical ground-level fall resulting in a quadriceps tendon rupture 1 year before. He underwent repair at that time using suture anchors, and during his recovery, as he started to complete his rehabilitation, he experienced multiple episodes of instability, weakness in giving way of the knee, and not being able to gain full confidence in the leg. He does have a history of smoking, hyperlipidemia, and prediabetes.
On physical examination, the patient was still able to perform a straight leg raise; however, they did have a visible lag. They did not have any pain or swelling, and there was a palpable gap of the native quadriceps tendon relative to the superior pole of the patella. When we look at the imaging, the patient had relative patella baja likely from his quadriceps tendon insufficiency and only mild patellofemoral arthritis.
Magnetic resonance imaging demonstrated that there were the prior anchors that were placed within the patella, and on sagittal views, we can see, as opposed to a traumatic rerupture, chronic attenuation of the quadriceps tendon and overall redundancy and laxity due to this stretching out and never healing completely.
Based on these multiple factors, the most concerning aspects are related to a failed prior repair making this revision reconstruction or revision repair, a palpable defect with residual laxity and resultant symptoms that are consistent with giving way of the knee, and lack of confidence consistent with this. For this patient, we recommended a revision quadriceps tendon repair augmented with an Achilles allograft reconstruction.
As we start out the procedure, we can palpate the defect proximal to the patella and where the native tendon would sit. We start with a longitudinal incision biased proximately to evaluate the tear itself. We can see the prior sutures from the anchor-based repair that was performed as the primary surgery. We now remove the remaining implants or sutures at a minimum to try to get to a bony bleeding bed on the proximal pole of the patella. It is usually easiest to bovie off the soft tissue on the proximal patella and then use a rongeur to remove this tissue. We can usually get down to petechial bleeding and we should not violate the cortex where the anchors are placed.
Biomechanically, it is becoming increasingly clear that suture anchors are superior for quadriceps tendon repair and reconstruction with regard to decrease gapping during cyclic testing as well as having higher ultimate failure loads. Anecdotally, these make it easier for the tendon to be brought down to the bone intraoperatively and are irrespective of bone quality compared with bone tunnels.
Here, we use two 4.5-mm polyether ether ketone anchors that are double-loaded with regular sutures. These typically have excellent fixation and are usually more reliable than bone tunnels in these revision settings. We then mark out and palpate the native end of the distal quadriceps tendon. This can usually be easily palpable, and we see how far we can still get the tendon to the bone and get good apposition of the soft tissue. We can remove any scar tissue that is formed in the meantime that is structurally irrelevant. In the setting of revisions in graft augmentation, we extended incision distally so we can visualize the patellar tendon insertion at the tibial tubercle. We then bovie down a spot distal and slightly medial to the tibial tubercle, which we undermine the paratenon so we can slide the graft underneath to reach this location. Using a guide pin, we place this just to the side of the tibial tubercle to not affect the patellar tendon insertion, and use an 11-mm reamer that is typically found in an anterior cruciate ligament (ACL) set.
After this hole is created, we prepare our Achilles allograft on the back table. We try to maintain the width of the soft tissue component and measure an 11-mm bone block. We trim the excess soft tissues so this tapers down to the insertion on the planned bone block for later insertion. We reverify the width of the bone block to 11 mm at its entire length and use a small oscillating saw to cut this similar to preparing an ACL bone block for a bone tendon bone allograft. The length of this is typically 20 to 25 mm, and we again rongeur this to be able to fit in an 11-mm sizer. Sutures can be placed for backup fixation through the distal component at the tendo-osseous interface. There is not a need for transosseous sutures for insertion.
Here, we can see passing of the bony component underneath the paratenon. This typically is done easier in a retrograde fashion seen here in the video. We then use a guidewire and a graft pusher to insert the graft into the tibial tubercle. We then use typically a metal interference screw in this setting at 7 by 20 mm. This typically gets excellent fixation; however, we recommend backup fixation, as the metaphyseal bone here has slightly weaker interference fit and can result in the bone block dislodging proximally. Here, you can see a whipstitch placed proximally and distally with a knotless anchor placed distally as backup fixation. We then use the anchors in the proximal pole of the patella to place our locking Krackow suture configuration with at least 4 throws proximal and 4 distally. We first tie down the initial throws which were a modified Mason-Allen configuration to get the tendon down to length and then tie the Krackow after this is complete (Figure 1). We then use the remaining sutures to tie down the graft to the proximal pole of the patella and use #2 Ethibond to tie the graft to the anterior aspect of the quadriceps tendon.
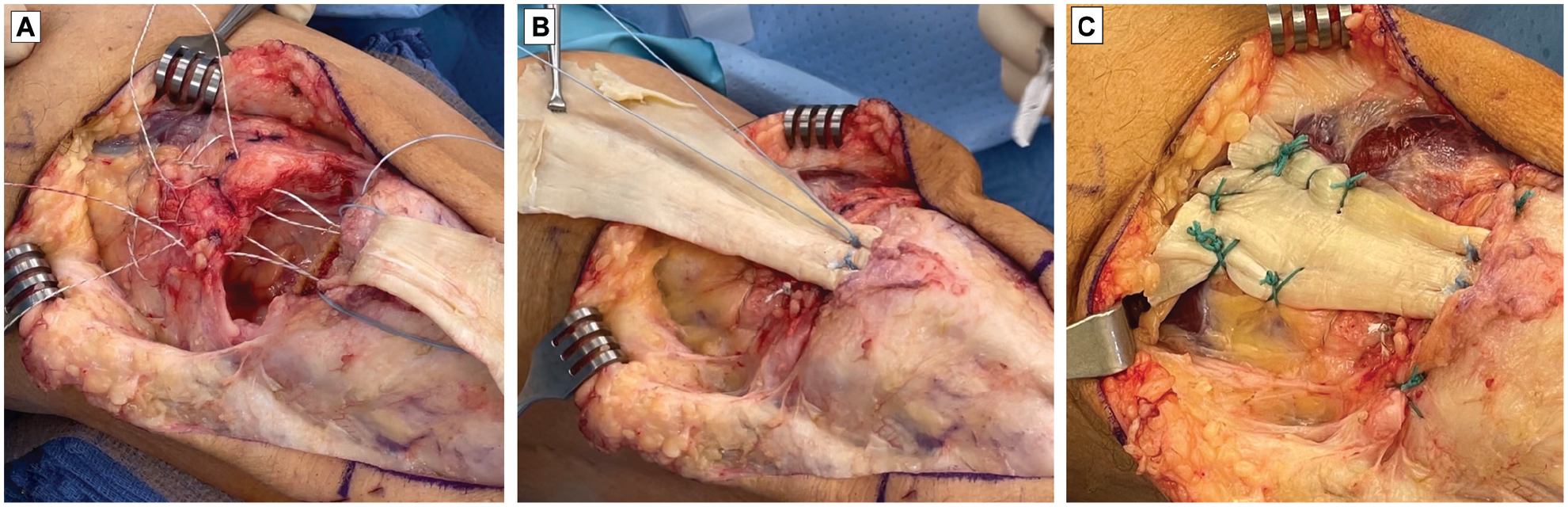
Steps to achieve the final suture configuration utilizing the double-loaded patellar suture anchors for (A) a locking Krackow stitch and (B) modified Mason-Allen stitch, followed by (C) Ethibond sutures for further soft tissue fixation of the graft.
Here, we can now see the final construct with the soft tissue suture configuration proximally and osseous fixation distally with the Achilles bone block being fixated in the tibia to span the entire construct.
Postoperative rehabilitation consists of weight bearing in full extension and a brace locked out without any motion until 6 weeks after surgery. We work on range of motion approximately 15° per week starting at 6 weeks getting to at least 90° of flexion by 12 weeks and full range of motion after that. We limit significant strengthening and squatting-type activities until 3 months after surgery. General pearls and pitfalls include making sure that the retinacular closure is done in a complete method in the setting of a chronic rupture. Sometimes, this requires imbrication as there may not be a formal tear in this area.
It is also helpful to get the bone-to-bone healing with the Achilles allograft in the tibia using an interference screw which can be backed up with a suture anchor as well to prevent displacement in the early postoperative. It is key to get the quadriceps tendon natively down to the proximal pole of the patella even if this requires a quadricepsplasty to obtain this. It is better to have some native tissue connecting as well as the augmentation with the allograft. Care should be taken to avoid chronic patella baja that is not corrected at the time of reconstruction performing a fat pad release as well as scar release adjacent to the patellar tendon.
The outcomes of allograft reconstruction for extensor mechanism injuries have been reported on, and the series seen here followed up 14 patients for an average of 52 months and saw that 25% approximately still had residual extensor lag after the procedure. They did have significant improvements in their patient-reported outcomes in general, and they were able to perform a straight leg raise at the final follow-up and did not have overt failure. The average satisfaction was 6 of 10.
References for this talk can be seen here.
Thank you very much for allowing us to present our technique on quadriceps tendon repair with Achilles tendon augmentation.
Footnotes
Submitted April 22, 2021; accepted June 25, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: A.B.Y. received personal fees from CONMED Linvatec, JRF Ortho, and Olympus; received grants from Aastrom Biosciences, Arthrex, Organogenesis, and Vericel; received nonfinancial support from Smith & Nephew and Sparta Biomedical; and received nonfinancial support and stock or stock options from PatientIQ. S.F.D. received hospitality fees from Medical Device Business Services and Zimmer Biomet Holdings; received education fees from DePuy Synthes Sales and Zimmer Biomet Holdings; and is a board or committee member of American Academy of Orthopaedic Surgeons. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.