
Abstract
The evaluation, classification, and treatment of significant bone loss after total knee arthroplasty (TKA) continue to be a complex and debated topic in revision TKA (rTKA). Despite the introduction of new evidence and innovative technologies aimed at addressing the approach and care of severe bone loss in rTKA, there is no single document that systematically incorporates these newer surgical approaches. Therefore, a comprehensive review of the treatment of severe bone loss in rTKA is necessary. The Stavros Niarchos Foundation Complex Joint Reconstruction Center Hospital for Special Surgery, dedicated to clinical care and research primarily in revision hip and knee replacement, convened a Management of Bone Loss in Revision TKA symposium on June 24, 2022. At this meeting, the 42 international invited experts were divided into groups; each group was assigned to discuss questions related to 1 of the 4 topics: (1) assessing preoperative workup and imaging, anticipated bone loss, classification system, and implant surveillance; (2) achieving durable fixation in the setting of significant bone loss in revision TKA; (3) managing patellar bone loss and the extensor mechanism in cases of severe bone loss; and (4) considering the use of complex modular replacement systems: hinges, distal femoral, and proximal tibial replacements. Each group came to consensus, when possible, based on an extensive literature review and interactive discussion on their group topic. This document reviews each these 4 areas, the consensus of each group, and directions for future research.
Keywords
Introduction
The Management of Bone Loss in Revision Total Knee Arthroplasty (rTKA) symposium was created with the purpose of developing a systematic and comprehensive review of leading practices in the approach and treatment of severe knee bone loss following a total knee arthroplasty (TKA). Participants sought to achieve consensus when possible. Prior to the symposium, the steering committee and invited participants created a list of questions that fell into 4 categories: (1) preoperative workup and imaging, assessing anticipated bone loss, classification system, and implant surveillance; (2) achieving durable fixation in the setting of significant bone loss in revision TKA; (3) managing patellar bone loss and the extensor mechanism in cases of severe bone loss; and (4) considerations regarding complex modular replacement systems: hinges, distal femoral, and proximal tibial replacements. This was followed by an extensive literature search for each topic, with results made available to the expert participants. Attendees separated into their designated panels to develop a preliminary consensus statement; these were presented to the entire group for comment, discussion, and further refinement into a final comprehensive document. After the symposium, the final document was circulated to all participants for their input and approval. The results of the symposium, which are presented in this extensive review article, reflect the current recommendations of the international group of expert revision knee surgeons and biomechanical engineers, with relevant supporting evidence.
Panel 1: Assessing Preoperative Workup and Imaging, Anticipated Bone Loss, Classification System
This panel focused on the preoperative evaluation and assessment of knee bone loss following TKA to provide guidance that may influence surgical management in a revision procedure.
Question 1. What Is the Standard Preoperative Radiographic Evaluation for a Patient Undergoing an rTKA With Associated Bone Loss?
The standard and required preoperative radiographic evaluation consists of radiographs in anteroposterior (AP), true lateral, and merchant views with the use of a magnification marker [90]. The AP view should preferably be obtained in weight bearing position with an extended leg. The patella should face toward the X-ray beam to avoid rotational errors. The X-ray beam should be targeted parallel with the slope of the tibial baseplate (Fig. 1a). This allows a visualization of the interface between bone and implant and reveals possible pathologies in this area. The true lateral view is an orthogonal view of the AP projection. It should be obtained with the patient laying on the side of interest with 30° of knee flexion (Fig. 1b). A correctly obtained true lateral view shows a superimposition of medial and lateral femoral condyles and an open tibiofemoral and patellofemoral joint space. It allows assessment of femoral, tibial, and patellar component position and fixation as well as radiolucent lines. Merchant views should be obtained in a supine position with the knee flexed at 45° and the knee held with a fixed platform to relax the quadriceps muscle (Fig. 1c). A correctly obtained merchant view shows a patella without superimposition of any bony structures and a good visualization of the patellofemoral joint [12,137]. This facilitates an evaluation of patellar alignment, bone quality and implant fixation.
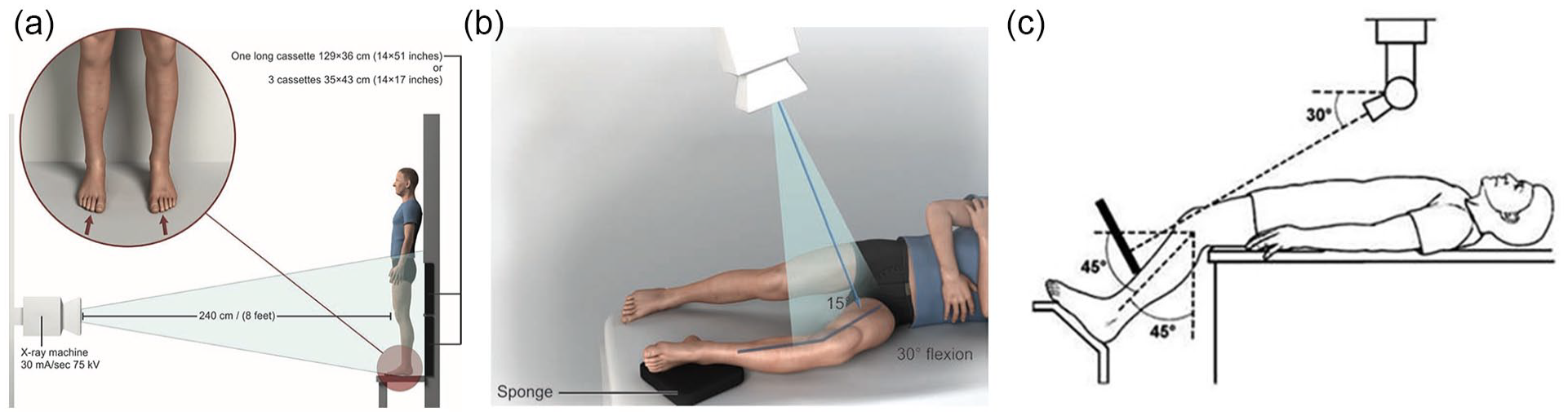
Patient positioning for (a) anteroposterior view (b) lateral view, and (1c) a merchant view.
Radiographs can help to assess periprosthetic lucency or osteolysis, wear of the polyethylene liner, heterotopic ossification, reactive bone formation, and periprosthetic fractures. The radiograph’s greatest weakness is that it provides a 2-dimensional analysis of a 3-dimensional structure. Although radiographs are the current standard of detecting osteolysis, they have been shown to be inaccurate and to substantially underestimate bone lesion size [112]. The sensitivity for the detection of osteolytic defects has been reported to be low (0% small defects [mean 0.7 cm³] to 66% large defects [mean 3.5 cm³]) [144,194]. The main problem is that radiographs are highly technician-dependent and that bony lesions are obscured by femoral and tibial implants (Fig. 2). Fig. 2a represents a good quality lateral knee X-ray where the X-ray is taken perpendicular to both the femur and tibia allowing for visualization of the bone, cement, and implant interfaces. In contrast, Fig. 2b represents a poor-quality lateral knee X-ray in which the X-ray is not taken perpendicular to the femur or tibia, thus obscuring the visualization of the bone, cement, and implant interfaces. Nevertheless, radiographs are an inexpensive and readily available tool for assessment of implant positioning, stability, and integrity and do provide useful information about bone damage.
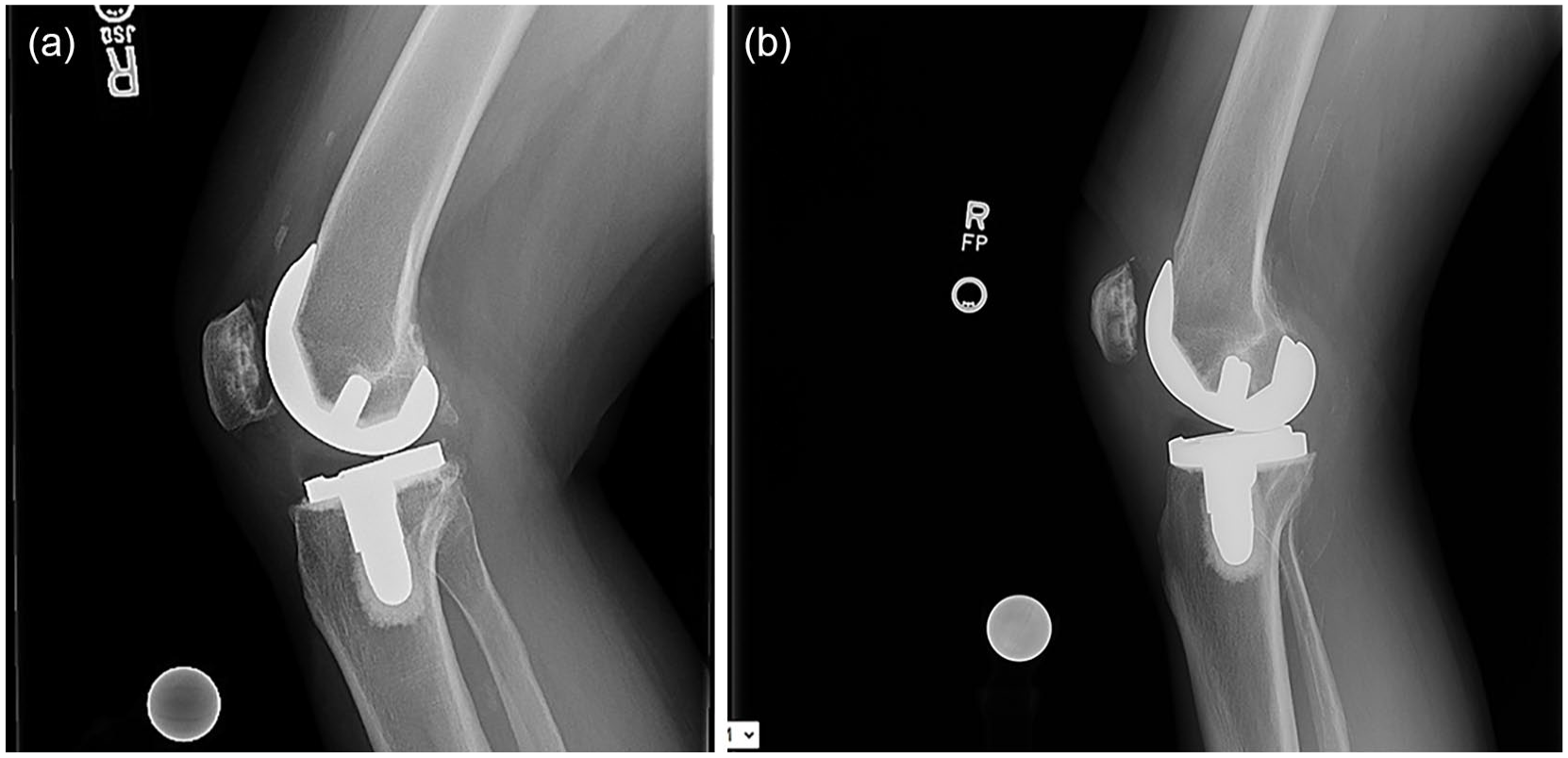
(a) A good quality lateral knee X-ray where the X-ray is taken perpendicular to both the femur and tibia allowing for visualization of the bone, cement, and implant interfaces. (b) A poor quality lateral knee X-ray where the X-ray is not taken perpendicular to the femur or tibia obscuring the visualization of the bone, cement, and implant interfaces.
Furthermore, it is recommended that the proximal femur and distal tibia are incorporated in the films to provide important information about alignment, other potential surrounding implants (such as a hip replacement), and relevant bone deformities. These images can be taken either as long-leg radiographs (LLR) or as separate AP and lateral radiographs of the femur and the tibia. Weight bearing LLR are an adequate tool for analyzing alignment preoperatively and postoperatively and are commonly used in orthopedic surgery. Alignment measurements are reported to be reliable with good intraobserver and interobserver reliabilities [29]. Nevertheless, several studies showed a significant impact of rotation of the lower limb during radiographic assessment on measured parameters. Thus, malrotation in LLR leads to altered measurements of component alignment and hip-knee-ankle angles (internal rotation decreases and external rotation increases hip-knee-ankle and coronal femoral as well as tibial alignment angels) [4,125,131]. Surgeons need to be aware of those potential measurement errors and repeat LLR or calculate rotational corrections in case of rotational errors. McGrory et al [138] compared 124 primary TKAs with patients prospectively randomized to either receive or not receive a preoperative LLR. They found no significant benefit of LLR regarding the obtainment of a neutral mechanical axis in uncomplicated TKAs. However, LLR are helpful in preoperative planning to help prevent postoperative malalignment, especially in cases with preexisting femoral or tibial deformity.
Oblique and fluoroscopically assisted views can be considered additional radiographic evaluation tools [37,145], but the clinical relevance of such additional imaging techniques remains unclear due to inconsistent study results.
Question 2. When Should Advanced Imaging (Magnetic Resonance Imaging [MRI], Computed Tomography [CT]) be Utilized in the Setting of Severe Bone Loss, and What Is the Unique Benefit of Each in Assessing Bone Loss? Does Anatomic Region Influence the Selection of Imaging Modality?
Advanced imaging (MRI/CT) should be utilized when osteolysis is suspected on standard radiographs. MRI or CT might be beneficial for further delineation of osteolysis [33,87] and may be useful for estimating the amount of bone loss present after TKA. This can aid with planning for rTKA, as it can help surgeons determine if they should order special implants (hinge knee prosthesis), augments, or cones/sleeves (which are not always readily available in the surgeon’s working environment). Metal artifact reduction sequences (MARS), such as Slice Encoding for Metal Artifact Correction (SEMAC) and Multi-Acquisition Variable Resonance Image Combination (MAVRIC), should be used [90,106]. Both MRI and CT have been shown to improve the sensitivity of detecting osteolysis around TKA [112,129,137,147,148]. However, to evaluate bone loss in TKA the expert panel prefers CT scans over MRI sequences, because MARS MRI images are more challenging to interpret given scatter from the metal, and a specially trained radiologist with appropriate experience is necessary but not always available [147]. The expert panel does not recommend advanced imaging such as MRI or CT for routine evaluation prior to revision TKA due to cost and increased radiation exposure (caused by CT).
What is the unique benefit of each in assessing bone loss?
CT scans are limited by metal artifact, which can obscure surrounding bone and soft tissue [167]. Metal reduction techniques are recommended [177]. CT scans can reveal changes in the surrounding bone that might not be apparent on radiographs and radiographically occult evidence of loosening, osteolysis, fracture and reactive bone formation [167]. MRI imaging is superior for assessing soft-tissue complications and it is valuable for evaluating the component-bone interface for osteolysis with metal artifact reduction sequences [167]. MRI can detect osteolysis that is not visible on radiographs [33] and can show synovial changes due to particle disease before osteolytic lesions become apparent [190]. Interpretation might be difficult, and a special, technically trained radiology team for recording the sequences might be helpful, although MRI sequences have improved [147]. In general, implants made of titanium or zirconium have less metal artifact scatter than prostheses made of cobalt/chrome/molybdenum alloys and are therefore less difficult to evaluate in MRI sequences [194].
Does the anatomic region influence the selection of imaging modality?
In the zonal fixation of revision knee arthroplasty, 3 anatomical regions (epiphysis, metaphysis, and diaphysis of the tibia and femur) can be used to support revision implants [208]. However, to our knowledge, no study shows a difference between the epiphysis, metaphysis, and diaphysis regarding imaging modality selection. One study found that MRIs have increased sensitivity for detecting defects in the femur compared w CT scans [129]. Therefore, the expert panel agreed that the anatomical region does not influence imaging modality selection.
Question 3. How Well Does Preoperative Imaging Predict Intraoperative Bone Loss, and Does Etiology of Revision (Infection, Osteolysis, Aseptic Loosening, etc.) Impact Prediction Accuracy?
In general, all preoperative imaging modalities underestimate the amount of intraoperative bone loss. They are unable to predict the exact amount of bone that will be lost intraoperatively during implant as well as cement removal or debridement of nonviable bone.
X-rays are reported to have a low sensitivity and specificity for the detection of osteolytic lesions (0% small defects [mean 0.7 cm³] to 66% large defects [mean 3.5 cm³]) [144,194]. The main problem is the bony lesions may be obscured by the femoral and tibial implants. Comparing the sensitivity of bone lesion detection between femur and tibia, Endo et al [55] found that detecting lesions in the distal femur is more difficult (97% tibia vs 46% femur). This could be explained by a larger surface area of the femoral component as well as the geometry of the box or pegs. The sensitivity of X-rays in detecting osteolytic lesions highly depends on the correct acquisition technique and rotation of the implant and is therefore technician-dependent. Even the introduction of oblique views could not demonstrate a significant improvement in detecting osteolytic lesions [112].
CT and MRI with metal artifact reduction sequences have been shown to be a useful and reproducible tool for evaluating the component-bone interface regarding osteolysis [55,87,194,208]. Using a human cadaver model, Solomon et al [194] found significantly higher sensitivities of MRI (89%) and CT (83%) compared with fluoroscopically guided X-rays (66%). With a mean lesion size of 3.5 cm3, no differences in the accuracy of defect volume measurements between CT and MRI were revealed. In contrast, Minoda et al used a pig knee model to compare the efficacy of MRI, CT, and X-ray in detecting smaller bone lesions (mean lesion size of 0.7 cm³). None of the small osteolytic lesions were detected using MRI or X-ray, whereas CT had a sensitivity of 61.5% and a specificity of 64.1%. In conclusion, CT may be beneficial in detecting smaller osteolytic lesions around TKA implants. Table 1 shows previous reports on sensitivity and specificity of the respective imaging modalities.
Previous reports on sensitivity and specificity in detecting osteolytic lesions of X-ray, MRI, and CT
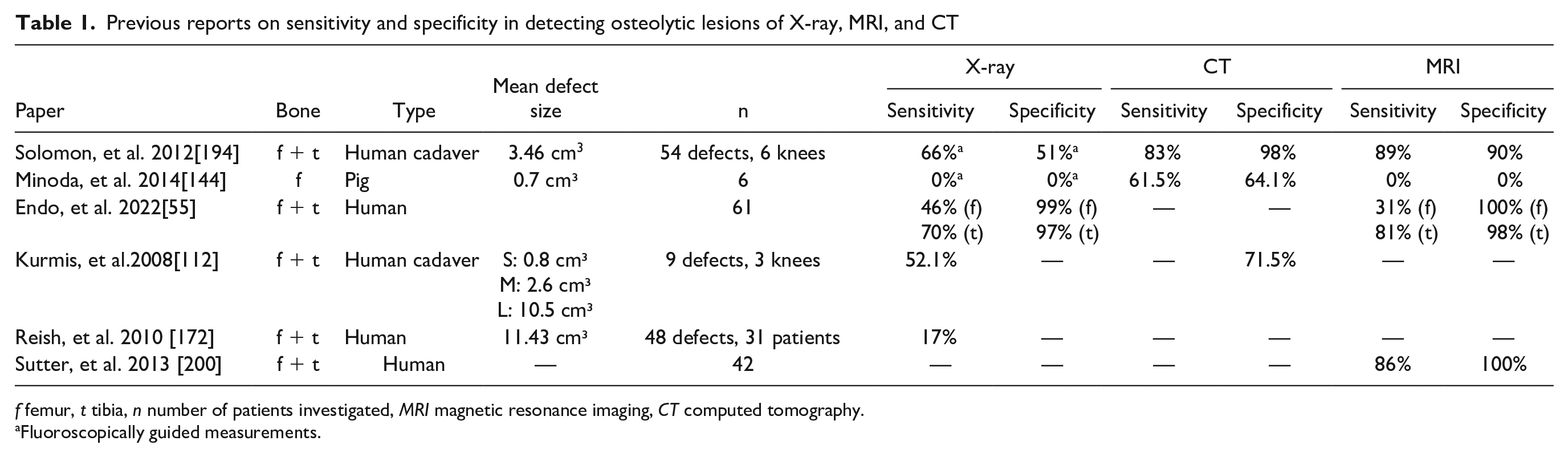
f femur, t tibia, n number of patients investigated, MRI magnetic resonance imaging, CT computed tomography.
Fluoroscopically guided measurements.
In the case of aseptic loosening, bone loss might be more predictable as the host bone is more likely to be viable. In general, detecting the viability of bone is difficult. Diederichs et al [52] found that both MRI and SPECT/CT may be able to differentiate between nonviable and viable bone tissue. They investigated patients prior to girdlestone arthroplasty and compared radiological and histopathological results. Nevertheless, metal artifact resulted in false-positive results. In conclusion, detecting periprosthetic nonviable bone is difficult and prone to error.
If infection is considered, but cultures are inconclusive or negative, further imaging might be useful. CT has a limited role, but IV contrast could help to find fluid collections and fistulae [90]. MRI has been reported to detect extracapsular spread of infection, abscess formation, and the appearance of lamellated hyperintense synovitis in the setting of infection; thus, MRI may be able to distinguish between septic and aseptic cases [166,167]. Three-phase bone scan can be beneficial to detect periprosthetic infection, but is not specific, as increased radiotracer uptake correlates with both infection and loosening [71], as well as normal remodeling in the first 2 years after implantation. If a joint aspiration culture is positive, infection is considered likely and no further imaging is recommended. Nevertheless, MRI and CT might give additional information regarding the extent of the infection and the quality of bone [69].
The presence of metallosis might complicate the detection of bone loss due to the artifact from metal particles. The pathomechanism of periprosthetic tissue destruction is complex and multifactorial. Articular wear of the prosthesis can result in particle accumulation, which in turn results in osteoclast upregulation and osteoblast downregulation leading to osteolysis [14]. The amount of liner polyethylene wear does not predict the volume of osteolysis as the response may be host and polyethylene specific. Li et al [121] found that wear can be diagnosed on MRI synovitis patterns and Koff et al [108] revealed a significant relation between synovitis on MRI and liner wear. Furthermore, Li et al [121] suggested that qualitative differences in the appearance of the synovium after TKA can allow for distinction between particle induced synovitis, infection, and nonspecific synovitis. These differences in synovitis patterns may contribute to the volume of osteolysis.
Question 4: What Are the Current Strengths and Weaknesses of the (Existing) Preoperative Bone Loss Classification Systems? In What Areas Can They Be Improved? Do These Classification Systems Adequately Address the Concept of Zonal Reconstruction, and Should That Be the Key Element in a Classification System?
The Anderson Orthopedic Research Institute classification (AORI) is a commonly used classification system used to describe femoral and tibial bone loss on plain radiographs and to guide the management of bone defects in primary revision TKA [58]. Mulhall et al [150] showed a good reliability and moderate-to-good overall agreement between preoperative and intraoperative evaluation of bone loss. In addition, they found that preoperative radiologic AORI assessment underestimates intraoperative bone loss (14% of tibial and 17% of femoral assessments). However, since the grading system was developed in 1999, it predates current reconstructive techniques. Furthermore, it does not address the concept of zonal fixation. In cases of more extensive bone loss in metaphysis and diaphysis of the femur and the tibia, there is a need for a more robust classification system to guide surgical options in revision TKA [181].
The modern Knee Society radiographic evaluation system is a descriptive classification system that provides a uniform method of determining preoperative and postoperative alignment and radiolucency and accommodates for the increased variety of implant geometries [142]. It incorporates evaluation of alignment in the coronal, sagittal, and patellofemoral plane and divides the surfaces of the tibial, femoral, and patellar components into zones. However, this system remains descriptive rather than predictive or prognostic because correlations are missing between radiographic findings, intraoperative bone loss, and postoperative outcomes [142].
The classification of bone loss in failed stemmed components in total knee arthroplasty is a new classification system for failed rTKA with stemmed components. It is based upon the location and degree of bone loss in the tibial and femoral metaphysis and diaphysis [181]. The amount of bone loss and its location were assessed on AP and lateral radiographs. A moderate to strong interobserver reliability of the method was found (ICC femoral: 0.62 and ICC tibial: 0.71) [181]. It partially considers the concept of zonal fixation, but the benefit is limited to stemmed components.
The University of Pennsylvania system is a continuous numeric classification system designed to map and quantify the amount of bone loss preoperatively on radiographs and intraoperatively [155]. It resembles a finite-element grid onto which the areas of bone defects that are seen on AP and lateral radiographs can be superimposed. Mulhall et al [150] showed good overall agreement between preoperative and intraoperative evaluation of bone loss. The system was more accurate in predicting tibial bone loss than femoral bone loss and there was a significant difference between the assessment of the AP radiograph and the intraoperative grid. In conclusion, this system gives an estimation of bone loss and could be used for research purposes, but is not practical for routine clinical use.
Another classification system for bone defects in revision TKA was developed by Belt et al They rated bone defects by their severity (none vs mild vs moderate vs severe) in 3 different zones (epiphysis, metaphysis, and diaphysis). The strengths of this system include its consideration of the containment of the defects and the concept of zonal fixation. It is a descriptive and subjective grading system with a moderate reliability in the epiphysis (intraobserver reliability 0.55 [95% CI 0.40 to 0.71]).
The strength of all of the classification systems presented lies in describing the localization of osteolytic lesions. The main weakness is that they generally poorly predict intraoperative bone loss. In addition, clinical and evidence-based outcomes based on the degree of bone loss and zonal fixation are lacking to drive the reconstructive techniques and to anticipate the prognosis of different surgical reconstructions. In conclusion, current classification systems used for bone loss do not adequately address the concept of zonal reconstruction, and zonal reconstruction should be a key element in developing a new classification system. A potential future classification system should help plan for the surgical reconstruction.
Question 5: Monitoring Patients With Osteolysis After TKA: What Is the Optimal Algorithm and When Is It Appropriate to Consider a Revision in the Setting of Implant Recall?
Osteolysis after TKA is a common cause of loosening and revision surgery. Osteolysis is defined by the Knee Society as an expansile lytic lesion adjacent to an implant that is greater than or equal to 1 cm in any one dimension or increasing in size on serial radiographs or CT scans [84]. Osteolysis can be both asymptomatic or symptomatic and is primarily diagnosed with radiographic follow-up [154]. Advancements in implant design and polyethylene manufacturing have largely mitigated osteolysis after TKA; however, there have been designs that have been recalled due to high rates of premature loosening secondary to massive osteolysis [97]. Other causes of osteolysis are infection, tumor, and endocrine abnormalities, and these causes should be considered when monitoring osteolysis. We outline an algorithm for monitoring patients with osteolysis both in the setting of the natural history of a TKA and in the setting of an implant recall with premature osteolysis (Fig. 3). We also discuss when it is appropriate to consider a revision in the setting of an implant recall.
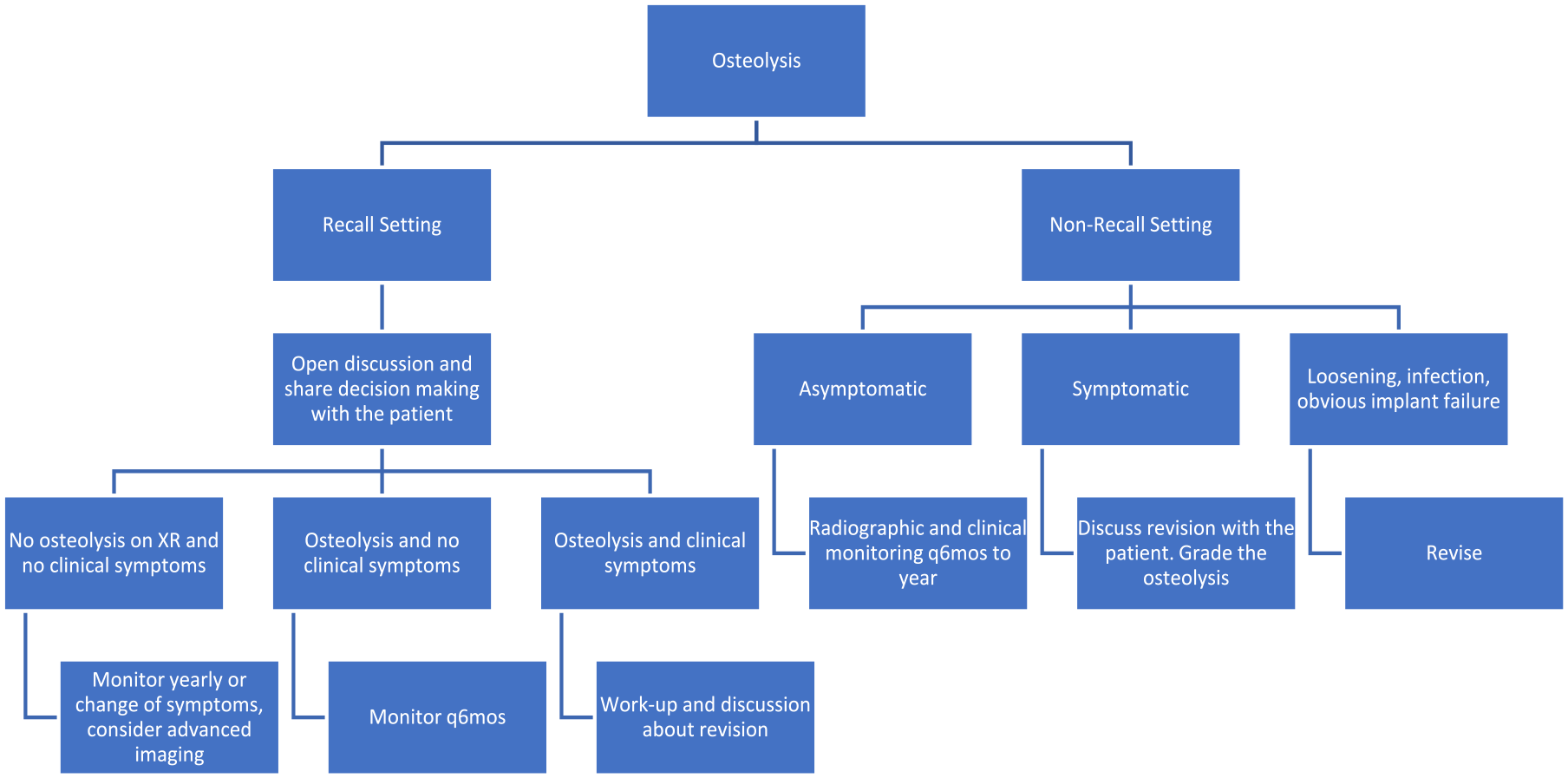
Algorithm to monitor patients with osteolysis after total knee arthroplasty (TKA).
Routine follow-up after TKA is more frequent within the first year. Depending on the preference of the treating surgeon, within the first-year patients return for follow-up at variable intervals with and without radiographs. All surgeons in the consensus group endorsed a return to clinic at 1 year with clinical and radiographic follow-up. After the first year, most surgeons in this consensus group preferred patients to come back at 5-year intervals if asymptomatic. However, if the patient develops pain or an effusion prior to the 5-year interval, the patient should follow-up between surveillance periods.
The clinical significance of osteolysis depends on the size of the lesion(s) and the patient’s signs and symptoms. If a patient presents with mild osteolysis, no symptoms, and no effusion, it is recommended to discuss that there are early signs of wear and bone loss that should be monitored more closely with annual visits. If the patient presents with mild osteolysis and pain or an effusion, they should have further evaluation to determine the cause. Evaluating for infection is important in any patient presenting with bone loss and pain or swelling. If the patient has moderate to severe osteolysis and no symptoms, follow-up should be 6 months to 1 year with symptom change. However, some patients may elect to move forward with revision surgery without symptoms if they have massive osteolysis and impending loosening or failure. This is reasonable and part of shared decision-making. Patients with clinical symptoms and effusions with radiographic osteolysis should have workups including infection and consideration for MRI, CT or bone scan as above. If the components are well-fixed, liner exchange or revision TKA should be discussed, which would be dictated on the severity of osteolysis, implants used, and implant fixation at the time of surgery. If the implants are loose, a full revision is recommended. If one component is loose, a single component revision may be considered. However, in the setting of an implant recall, a full revision may be indicated depending on the nature of the recall.
For implant recalls, the surgeon should establish a protocol with the treating institution to ensure all patients who have received the implant are informed. Patients should return for clinical and radiographic follow-up regardless of symptoms. Shared decision-making between the patient and surgeon should be emphasized in all settings, but especially in the setting of an implant recall as patients will have many questions and concerns. Revision TKA may not be the right solution for all patients despite having a recalled implant. The recommended follow-up for a recalled implant is similar to what is outlined for those without a recall if asymptomatic: 6 months to 1 year clinical and radiographic follow-up for asymptomatic knees with mild osteolysis. If the patient has obvious clinical loosening, severe osteolysis, or progression of osteolysis, recurrent effusions with or without pain, a revision TKA should be discussed with the patient. If the patient has an asymptomatic knee, and there is minimal to no osteolysis seen on plain radiographs, further imaging with CT scans and/or MRI should be considered to define a baseline of osteolysis that may not be readily seen on plain radiographs.
Panel 2: Achieving Durable Fixation in the Setting of Significant Bone Loss in Revision TKA
Questions 1 and 2: Does Bone Quality (Sclerotic/ Osteoporotic) Impact Implant Selection and Fixation Type (Fully Cemented vs Hybrid)? Fully Cemented vs Hybrid Stem Fixation: Are Certain Bone Loss Patterns Better Suited for a Particular Fixation Method?
In revision TKA, diaphyseal fixation of the femoral and tibial components can be achieved with fully cemented stems or with uncemented stems in a hybrid construct (epiphyseal and metaphyseal cementing). Stem fixation is beneficial to provide load sharing and protect the joint surface from excessive stress and implant loosening [220]. Some surgeons advocate for cemented stems while others prefer so-called hybrid fixation (uncemented stems). Each method of fixation has advantages and disadvantages, and each may be appropriate depending on the operative findings (Table 2) [147,158,220].
Pros and Cons of each fixation methods.
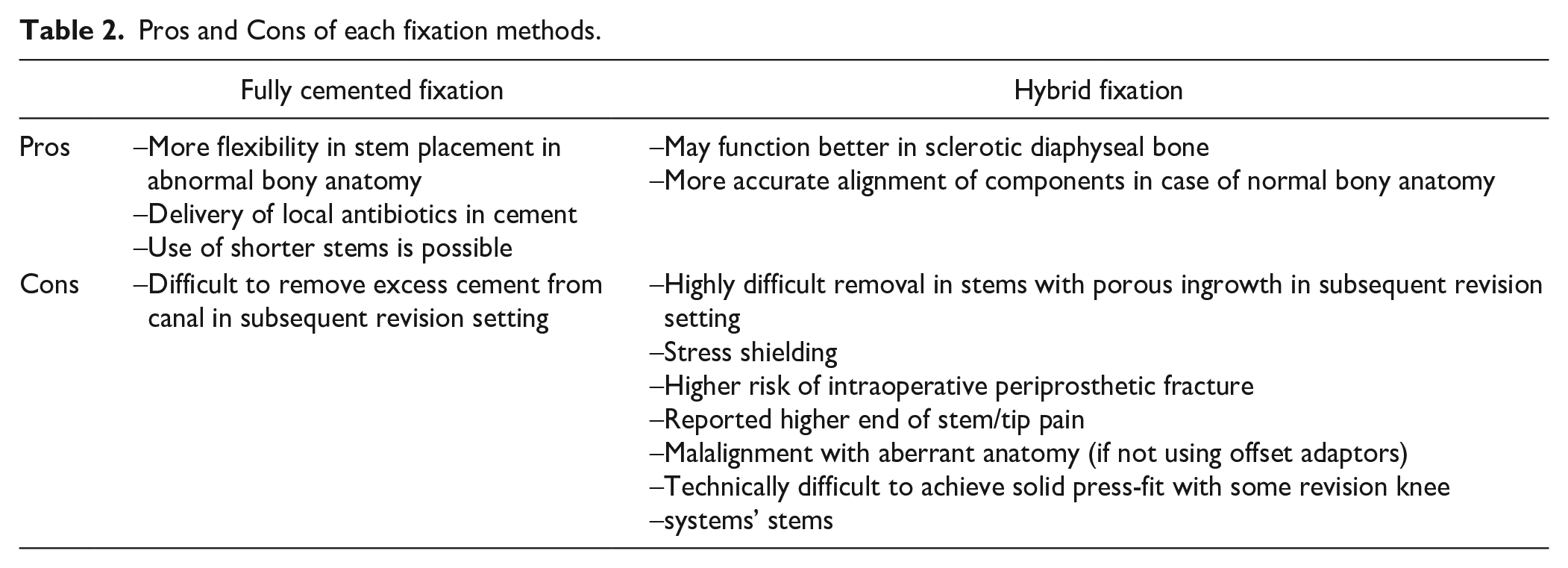
There is no consensus in the literature for the use of fully cemented versus hybrid constructs in revision TKA. One systematic review of 7 studies (1179 stems) compared hybrid versus fully cemented stems. There were significantly lower failures rates with the use of hybrid stems compared with cemented stems. However, a trend was noticed (with no significant difference) in favor of the use of hybrid stems in all-cause re-revision, aseptic re-revision, and radiographic failure, compared with fully cemented constructs [185]. The combined radiographic failure and all-cause re-revision rate was 23% with cemented stems and 16.8% with hybrid constructs. Although cemented stems are considered technically easier and allow the surgeon more flexibility in component positioning, this review recommended hybrid fixation, whenever possible, due to the slightly lower failure rate [185]. However, these conclusions were limited by multiple confounding variables in the study.
In contrast, in a report of 275 revisions with rotating hinge components, van Laarhoven et al [207] noted higher rates of survival free from aseptic loosening for fully cemented stems compared with hybrid fixation. In a single surgeon retrospective study of 84 total knee revisions with stemmed femoral components, at a mean of 6 year follow-up, Lachiewicz and O’Dell noted no statistically significant difference in reoperation for loosening between cemented and uncemented stems. However, the authors’ power analysis noted that an adequately powered study would require over 200 knees [114]. In a randomized controlled trial using RSA analysis, Heesterbeek et al [85] and Kosse et al [110] concluded that cemented and cementless stems in revision TKA were equally stable at 24 months and 6.5 years follow-up time.
In a cadaveric experimental and computational study, hybrid fixation with a long uncemented stem combined with a cemented metaphyseal component was most effective in reducing the strain in the proximal tibia for condylar constrained knee (CCK)-type implants [171]. However, the greatest biomechanical advantage of a stem was noted when the bone underneath the tibial tray had poor quality. Another cadaveric study reported similar biomechanical behavior between short cemented and long uncemented stems when combined with a trabecular metal cone [140]. A recent experimental cadaveric and computational study compared long hybrid and short fully cemented stems in the presence of cones to address moderate contained metaphyseal defects (Fig. 4) [168], and reported that long uncemented stems provide little biomechanical advantage over short stems for tibial fixation. The biomechanical behavior of short cemented tibial stems was similar whether cones or cement alone were used to address the defect. For femoral fixation, a cadaveric study reported that long cemented or uncemented stems result in comparable biomechanical behavior as short cemented stems for treating AORI IIA and III type defects [79]. However, this study cautioned that the quality of bone structure will influence fixation.
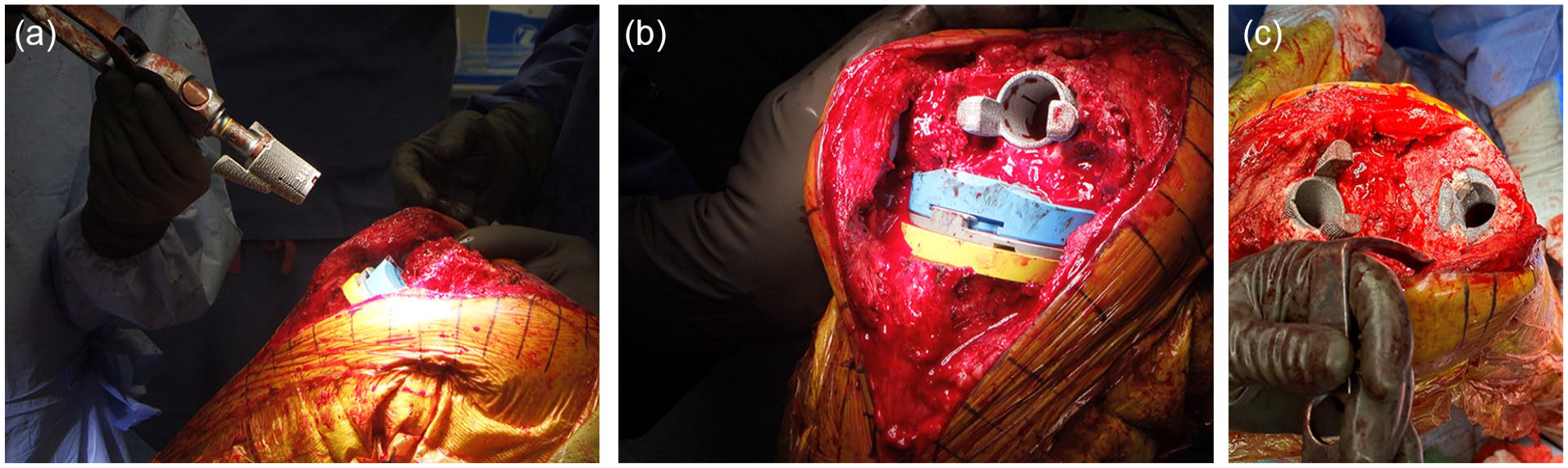
(a) Insertion of femoral cone. (b) Use of femoral cone. (c) Use of cones in both femur and tibia.
In summary, the choice of cemented vs hybrid fixation in revision TKA should take into consideration multiple factors including patient anatomy, etiology of revision surgery, and level of constraint of implant required for stability (Table 2). Without evidence of clear superiority in survivorship of either method of stem fixation, the decision should be made by the treating surgeon based on the aforementioned variables and clinical experience.
Question 3. Does Augment Size Impact Construct Stability and the Need for Additional Metaphyseal Fixation?
Metal augments are widely used in revision TKA for reconstructing both tibial and femoral defects, but there is little reported data on their success and impact on fixation and longevity of revision constructs. Augments are fabricated in various sizes and are screwed into or cemented to revision components. In one review, Sheth et al [186] advocated for the use of augments when at least 40% of the bone-implant interface is unsupported with instability of the trial component.
Both wedge and block augments are available for the proximal tibia. Wedge augments often require the surgeon to resect less bone, but block augments seem better in resisting biomechanical shear forces and unloading stress [186,220]. Subsequently, wedge augments are more susceptible to mechanical failure due to the application of greater shear forces at the implant-bone interface [39,186]. Compared with the use of bulk allograft, block augments provide immediate support, shorter surgical times, and no issues with resorption, but have disadvantages including cost, lack of customizability, and no biologic restoration of bone stock [186].
For distal femoral bone loss, posterior augments are helpful in providing rotational stability and decreasing the flexion gap, while distal augments provide axial stability and help in joint line restoration. One disadvantage of distal femoral augments is the resultant decrease in the contact area between the anterior and posterior flanges of the femoral component, the femoral box and the host bone, with possible decreased stability at the bone-implant interface [95]. Other risks of augments include fretting, corrosion, and potential for disassociation between the metal augments components and the femoral or tibial implants [95].
In a review of the literature, Zhang et al [220] reported failure rates of wedge augments of 17% requiring revision for implant migration, with approximately 50% prevalence of radiolucent lines at the wedge augment bone interface. The survival rate of metal augments for AORI II type defects has been reported at 92% at 11 years follow-up, with an incidence of radiolucent lines of 15% [186]. The impact of augment size on construct stability and the threshold at which augments necessitate additional metaphyseal fixation is not well defined in the literature and requires additional study. However, as increasing augment thickness, decreases bone implant contact area, surgeons should consider increasing implant bone surface area and fixation with either longer stems, larger diameter stems, metaphyseal fixation via cones or sleeves, or a combination of both, to improve long-term durability. The work group consensus was that >5-mm distal femoral or tibial augments endangers zone 1 fixation and require increased fixation in zones 2 and 3. Additional biomechanical and in vivo studies are needed to evaluate the effect of varying sizes of block augments on fixation. Further investigation is also needed to determine the optimal fixation method to unitize augments with tibial and femoral components.
Question 4. How to Achieve Fixation With Various Bone Defects (Sclerotic/Osteoporotic/Segmental Defects)? The Role of Zonal Fixation in Revision Knee Replacement?
Treatment of bone defects in revision TKA requires the surgeon to define the extent of the defect and plan the reconstruction strategy. The AORI classification is widely used in rTKA for classifying bone defects, using both preoperative radiographs and intraoperative surgeon inspection. In a review of revision TKA, Zhang et al proposed that AORI I and IIA-type defects can be treated using basic methods including primary implants, cement, screws, autologous versus allograft bone grafting, and metal augments.
However, AORI IIB and III type defects require more sophisticated reconstruction with block and wedge augments, metaphyseal sleeves or cones, and in some cases, custom-made augments [220] The concept of zonal fixation was introduced as a key framework for achieving implant fixation in TKA [147]. Zonal fixation references 3 zones in the distal femur and the proximal tibia.
Zone 1, the epiphysis, is often compromised in the revision setting but can sometimes be restored with techniques such as augmentation. Bone cement is the typical form of fixation in this zone. Oh and Scuderi [158] recommend the use of cement or impaction grafting to treat zone 1 cavitary defects <5 mm, while those between 5 and 10 mm may benefit from cement and screw “rebar” reconstruction. Larger defects benefit from metal augmentation in this zone.
Zone 2, the metaphysis, is essential for fixation as it is close to the joint surface, provides better stability in the axial plane, and can help to restore the joint line. Zone 2 fixation can be achieved with cement, metaphyseal cones, or sleeves. Cones and sleeves are beneficial in this zone as they provide immediate press-fit stability and long-term ingrowth for durable fixation [158]. For massive, combined zone 1 and 2 defects, allograft, in the form of cancellous bone chips, bulk structural allograft, or both may be beneficial, particularly for younger patients with a primary goal of restoration of bone stock [158].
Zone 3 fixation is achieved with cemented or uncemented stems and helps to offload the metaphyseal and epiphyseal fixation [147]. In cases of a deficient diaphysis or sclerotic bone, diaphyseal impaction grafting has been described as a technique to combine with cones to attain stable fixation [20]. Another option might be uncemented, diaphyseal engaging, ingrowth stems, but revisability might be an issue. The early literature on the concept of zonal fixation advocates achievement of fixation in at least 2 of the 3 described zones with a preference for solid fixation in all 3 zones, if possible [147,158].
Question 5: What Are the Benefits of Cones vs Sleeves? Is There a Bone Loss Pattern Better Suited for One or the Other?
Both cones and sleeves can theoretically provide biologic fixation in the metaphyseal region, for initial rigid, durable, long-term fixation. Differences between them are noted in Table 2. Determining the benefits of a cone vs a sleeve is not greatly helped by a review of the literature, which is comprised of retrospective, uncontrolled, level IV studies, from centers that sometimes have exclusive experience and bias with one or the other implant. There are multiple published systematic reviews and meta-analyses of the results of cones and sleeves, which have largely demonstrated no difference in aseptic survivorship, radiologic outcomes, and patient-reported clinical scores [64,104,174,219]. These are all limited by their review of level IV studies, with high degrees of selection bias and poor quality short and medium-term evaluations. Furthermore, it is difficult to generalize the published results of 1 specific highly porous cone, with over 20 years of experience, and 1 specific type of sleeve, with over 15 years of experience, to relatively new cones and sleeves introduced by multiple implant manufacturers.
It is generally accepted that cones and sleeves should be utilized for AORI IIB and III type defects [36,58,113]. In some reports, both cones and sleeves have been utilized routinely in revisions with AORI I and IIA-type bone loss, at the intraoperative discretion of the surgeon to “enhance metaphyseal fixation” in patients, and with revisions using highly constrained and rotating hinge knee prostheses [36,86]. This makes interpretation of the results of cones and sleeves even more problematic. A nonrandomized study of both devices at one institution reported no important differences between the results of revisions with sleeves or cones at a mean follow-up time of only 41 months [86]. The study with the longest follow-up for sleeves found a 97.8% implant survivorship at 10 years, with no sleeve revised for aseptic loosening.
The decision to use a metaphyseal cone or sleeve is multi-faceted and has been generally determined by surgeon experience and bias, or institutional bias/preference (based on costs), but the shape, size, and location of the bone deficiency may be a critical factor in selection. There may also be a difference if the defect to be treated is in the proximal tibia or distal femur. Highly porous metal cones are currently available from many implant manufacturers in multiple sizes, shapes, and asymmetric geometries. Stepped and lobed designs have been generally utilized for larger and asymmetric tibial defects. Porous tantalum (PT) cones (as opposed to titanium) require a high-speed burr (broach is also available) to contour the metaphyseal bone to achieve maximal bone contact [156]; these cones have an additional advantage in that the cone itself can be contoured with a high-speed burr to alter the shape and size if needed. As sleeves are proprietary to a single company (DePuy Johnson & Johnson), a single component (tibia or femoral) revision may necessitate a sleeve for metaphyseal fixation of the component being revised for compatibility between systems.
Peripheral and uncontained tibial defects, particularly if large and associated with angular (usually varus) deformity of the tibia, are more amenable to treatment with an asymmetric tibial cone, with or without an additional metal augment fixed to the tibial tray component. Smaller, more central, and contained tibial defects may be more amenable to treatment with either a sleeve or a symmetric cone. For treatment of femoral type III defects, in which both epicondyles and their ligament origins are intact, a full femoral cone provides the most increased area for distal cement fixation. Central or AORI IIB type femoral defects, or knees in which a rotating hinge prosthesis is needed for collateral ligament deficiency, are amenable to treatment with a sleeve or a smaller cone. There are currently no prospective, randomized studies comparing the outcomes and complications of sleeves vs cones in any of these scenarios.
The ultimate choice of metaphyseal fixation should be at the discretion of the treating surgeon considering the particular bone loss pattern, as well as familiarity with the system.
Question 6. Best Practice for Cone Preparation: How to Prevent Bone Fracture in Sclerotic Bone? How to Assess Appropriate Cone Size (Sufficient Axial Rotation Stability)?
A complete or segmental sclerotic bone shell typically occurs in the metaphyseal regions of the knee during the process of aseptic loosening. If the shell is left intact, gaps may form between the bone bed and the revision implant. However, creating some bleeding surface without cortical fracture allows bone marrow and vascularity to reach the implant surface. In multiple animal models, a “crack revision” technique has been described in which a splined tool is used to circumferentially perforate the sclerotic bone rim before insertion of a revision implant [109]. This resulted in significantly higher push-out strength and energy to failure compared with control revision procedures without perforation of the sclerotic bone [140,168,171].
While fracture rates with cones are generally low (under 2%) [100,203], one study reported a fracture rate as high as 24% (7/29) when using tantalum cones [209]. When preparing the bone bed, surgical technique, with either a burr or a rasp, is important in the presence of sclerotic bone and to avoid a fracture. Metaphyseal sleeves with a broaching technique against sclerotic bone have been reported to have an intraoperative fracture rate from 1.9% to 6.5% [13,36,76]. When broaching for a sleeve, the surgeon should sequentially increase in broach size until axial and rotation stability is obtained. While broaching, the surgeon should properly maintain alignment of the broach (in coronal and axial planes) as translation of forces may result in iatrogenic fractures. In the presence of sclerotic bone, the broach may also deviate away from the sclerotic side. The use of a reamer and a high-speed burr to remove sclerotic bone may allow a safer and more accurate broaching technique, but there is little evidence in the literature to support this statement [169]. It is also uncertain that a small or nondisplaced intraoperative fracture influences the outcome. The work group consensus was that an unstable fracture affects the structural support or mechanical stability of the implant and requires fixation.
There has been an evolution of cone design, instrumentation, technique of insertion, shapes, and sizes within each individual company, and there is variation between multiple companies. Newer cones (often referred to as “second-generation cones”) require cannulated reaming of the medullary canal until a stable circumferential endosteal fit is reached and adequate rotational stability is achieved. The reamer system (which is marked to delineate size and depth of the corresponding cone) matches the actual cone geometry, and thus the bone preparation for current cone systems have been simplified from the traditional burring technique used in the earlier generation of cones. There is also a new generation of tibial sleeves with more ingrowth surface area potentially enhancing osseointegration. The surgeon should ensure that excessive bone is not removed during this process. There is no literature on what percentage of the cone needs to be in direct contact with host bone; however, the consensus is that more cone surface area for direct contact with host bone would lead to a higher likelihood of long-term durable fixation. The surgeon should not ream away excessive “good bone” just to get complete circumferential contact. If the shape and size of the bone defect make it impossible for a perfect circumferential press-fit on all sides of the cone, an asymmetric cone can be used, or bone voids may be filled with bone graft, substitute, or cement. When impacting the real cone, the surgeon must control the depth of impaction to prevent an iatrogenic fracture. In some instances, the goal may be for the implant to rest on the cone for additional axial stability, whereas in others it is really intended to improve the cement implant interface strength; this is left to surgeon discretion, based on intraoperative findings.
Question 7. How Do Cones Impact Stem Fixation and Stem Length?
There are multiple studies exploring the effect of stem size and fixation in revision TKA, [43,101] emphasizing the importance of cementless stem canal fill and engagement, but no difference between cement versus cementless fixation of stems. However, there is very little literature examining the role of stems in the context of cones.
There are no biomechanical studies that directly compared cones and sleeves to address metaphyseal defects. A series of computational studies involving sleeves reported minimal to no advantage of using stems for improving the primary stability of the construct [9-11]. One computational and biomechanical study involving cones reported minimal advantage of a long hybrid stem compared with a short cemented stem for stability of the construct. This study concluded that both constructs result in relative motion between the cone and the bone compatible with bone ingrowth [168]. Although these studies are not directly comparable due to differences in the loading and study design, both reported relative motions between the sleeve or cone and the bone of similar magnitude: Maximum values ranged between 9 and 36 µm for sleeves combined with long stems and 13 µm to 23 µm for the cone combined with long stems.
Another biomechanical study reported that a short cemented tibial stem had similar varus/valgus displacement, internal/external rotation, compression, and lift-off micromotion values under loading compared with a cementless diaphyseal stem. The addition of a tibial cone improved compression and lift-off micromotion [5]. A computational study investigating whether stems are required to augment metaphyseal cones (3 scenarios: No stem, 50 mm stem, and 100 mm stem) concluded that stem use may not be necessary to manage uncontained posterior or medial defects of up to 10 mm depth [218]. These authors reported small micromotion (mean < 12 µm) at the bone-implant interface for all loading cases, with or without a stem. Short and long stems had a reduction in micromotion of only 3.3 and 6.7% respectively, which may not be clinically significant. This study may corroborate other reports that showed a reduction in micromotion with stem usage [9,42,153].
A recent retrospective clinical study of 49 revision TKAs reported 100% survival (free of revision for aseptic loosening) of metaphyseal cones with short cemented stems at short-term follow-up of 39 months [21]. One study reported that the use of cementless stems with a cone resulted in higher odds of hip-knee-ankle malalignment compared with cemented stems. This may be due to the difficulty of using offset couplers with central cones [7].
Question 8. The Role of Bone Grafting in Revision TKA: Does Impaction Grafting and Structural Allograft Still Play a Role?
Impaction grafts with morselized cancellous bone with or without mesh were traditionally considered for moderate-sized contained defects. However, the results of this technique in isolation for massive osseous defects in revision TKA have been mixed at best and not as successful as we have seen in total hip arthroplasty [88,125,127,128]. Success is predicated on excellent surgical technique; if not done routinely, it should be referred to an expert in the technique.
There are 3 possible scenarios in which this technique may be utilized with reported success demonstrated using contemporary techniques.
The first scenario is in younger patients undergoing revision TKA with an increased chance of undergoing re-revision later in life. In this setting, this technique allows preservation of bone stock, obviating the need for large metal augments or custom prostheses, which often necessitate removal of more bone.
The second scenario in which to consider impaction grafting is when the technique is combined with metaphyseal cones for severe bone loss involving both the metaphysis and diaphysis. In cases of previously instrumented canals with failed stemmed implant, the resultant sclerotic canal impairs fixation using a cemented stem. In this setting, the impaction grafting technique becomes useful as it optimizes cement fixation in the diaphysis while the metaphyseal defect is addressed with a porous cone. Bedard et al [20] demonstrated 100% survivorship free of aseptic loosening and significant success regarding incorporation of the bone graft using this technique.
The third scenario is the use of impaction grafting in developing nations where advanced technology and highly porous metaphyseal fixation may not be readily available and may further be hindered by a patient’s inability to pay for the device.
At present, the use of bulk/structural allografts is very limited, due to problems with availability, cost, possibility of disease transmission, and high risk of reoperation.
Question 9. The Biomechanics of Cones: Material Properties, Size, Shapes, Zones of Engagement, Cone-Implant Compatibility?
Ultra-porous metaphyseal cones are 3-dimensional metal structures with interconnected pores, with a modulus of elasticity between cancellous and cortical bone. They are highly biocompatible and osteoconductive, and thus provide a porous surface for biologic implant fixation. Pore sizes of 500 um to 600 um and porosity of 60 to 65% optimizes biologic fixation. The increased contact area helps offload stresses and loads imparted on the implant articular surface and stem extensions, decreasing micromotion (goal <150 um) and allowing a stable metaphyseal platform for osseointegration.
Compared with older porous materials, ultra-porous metals manufactured from tantalum and titanium have enriched characteristics with improved osseointegration ability and reduced bacterial adherence [189]. Tantalum (Trabecular Metal, Zimmer Biomet) has corrosion resistance, high coefficient of friction (0.88–0.98), and modulus of elasticity (2–20 GPa) lower than titanium and cobalt/chromium, and thus creates a more physiologic stress transfer [143]. Titanium cones serve as an osteoconductive scaffold and encourage osteoblast migration for osseointegration [189], with several currently on the market including Tritanium (Stryker), StikTite (Smith & Nephew), and Porocoat (DePuy), 3DMetal (Medacta), and InteGrip (Exactech). Unlike tantalum, which is manufactured using a thermal deposition process, contemporary titanium cones are manufactured using 3D-printing.
In contrast to first-generation cones that had limited sizes and geometry relative to the bony anatomy and required freehand host bone-preparation (ie, burring), newer-generation designs allow for easier and more reproducible host bone-preparation with ream and broach systems available, depending on the manufacturer. These systems allow a more efficient preparation and consistent bed for the cone. Unlike when using sleeves, cone preparation and implantation are independent of the knee implant choice and choice of stem fixation. However, the cone must have an appropriate inner diameter to allow for passage of the selected stem diameter and offset adapter if needed in the reconstruction (Table 3). Depending on the cone size, the maximum stem diameter ranges anywhere from 16 to 30 mm, but this is vendor-specific. Newer generation cones have also minimized the outer diameter to reduce bone removal during preparation. While most defects can be managed with symmetric, central cones, asymmetric and bilobed cone designs have been developed to further address larger segmental defects with both central and peripheral metaphyseal bone loss (as seen in AORI IIB and III type defects).
Comparison of cones versus sleeves.
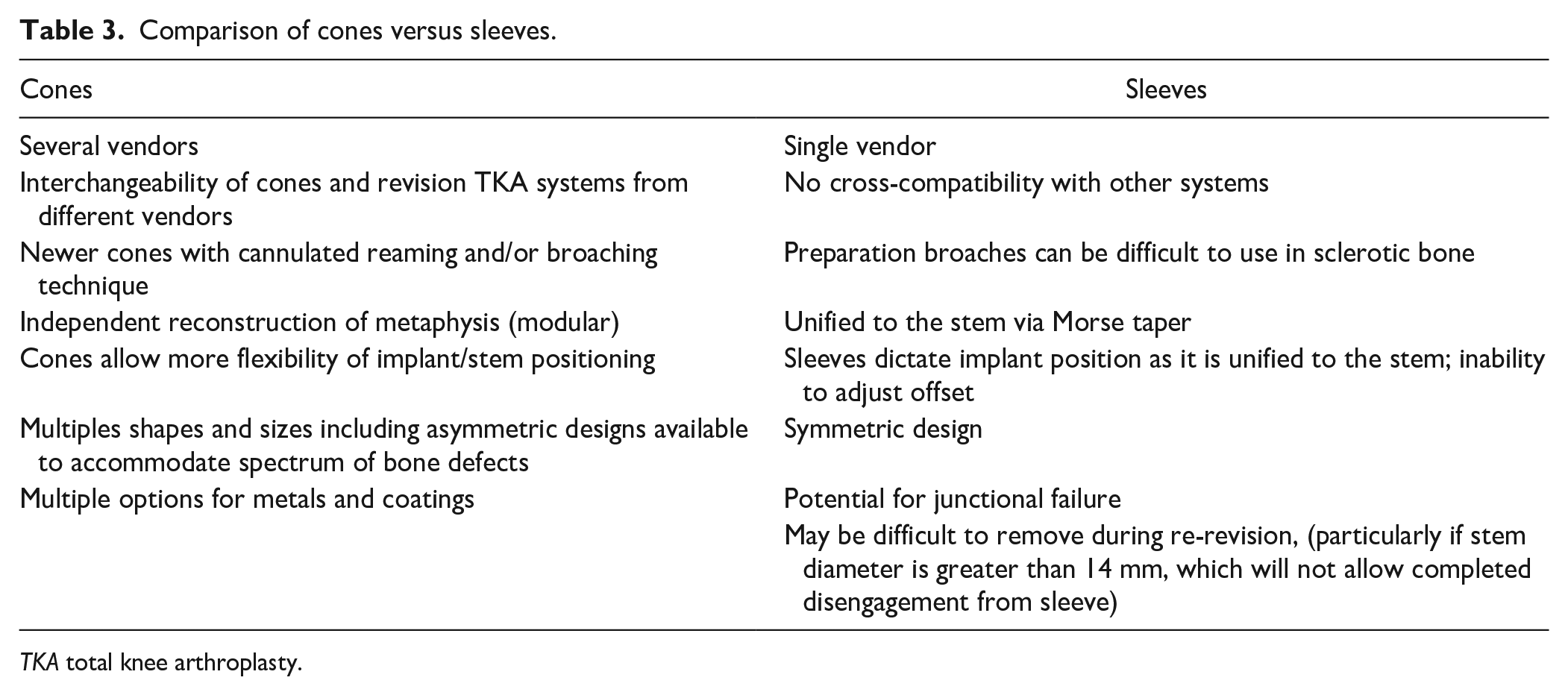
TKA total knee arthroplasty.
Finally, while the independent preparation of cones and revision TKA has allowed for seamless interchangeability from different manufacturers, it is important for surgeons to be mindful of each manufacturer’s cone specifications and sizes as highlighted above. It is imperative that the geometry of the planned stem and cone are in harmony to avoid conflict between the components, and that the cone’s inner diameter is in alignment with the intramedullary canal of the femur or tibia.
Question 10. What Imaging Modality Is Best to Evaluate Cone/Sleeve Ingrowth?
Despite the various imaging modalities available for evaluating cone and sleeve ingrowth, there is a relative lack of standardization. Weight-bearing biplanar plain radiography of the knee including the femur and tibia should serve as initial screening tools as they are easily available and accessible with low costs. Serial radiographs are helpful to ensure no progressive movement between bone and the metaphyseal cone/sleeve as evidenced by partial or circumferential radiolucencies, which may suggest loosening. Implant ingrowth is generally suggested by circumferential apposition of the bone-implant interface and “spot welds,” which represent cancellous hypertrophy between the cone/sleeve and the endosteal surface [56,123].
Criteria described by Engh et al [57] may be used to evaluate for osseointegration at the bone-implant interface and scoring systems accommodating metaphyseal augment constructs have been described [61,63].
Alternative modalities include CT, MARS-MRI, bone scintigraphy (“bone scan”), and single-photon emission CT (SPECT), all providing more detailed views of the bone and implant, which is especially important in patients with normal radiographs. These modalities may also give better insight to loosening and any concomitant osteolysis, which is often underestimated by plain radiography. Bone scintigraphy is a good technique for evaluation of osseous uptake at the cone/sleeve-bone interface after >1 year postoperatively. Lastly, in vivo bone remodeling can be evaluated with SPECT imaging, with studies suggesting osseointegration around 3 months for total joint prostheses [27]. However, this modality is time-consuming, accessibility is limited, and it has not been widely accepted.
Panel 3: Managing Patellar Bone Loss and the Extensor Mechanism Complications in Revision Knee Arthroplasty
Patellofemoral complications have been reported to occur in up to 10% of TKAs; they represent one of the most common reasons for reoperation after TKA [133]. In addition, various conditions including patellofemoral instability, component dissociation or loosening, patellar fracture, residual anterior knee pain, component wear, osteonecrosis, patellar “clunk,” and patellar tendon rupture have been responsible for up to 50% of additional surgical procedures after TKA [30,124,130,133]. The functional role of patella is to provide a mechanical advantage for knee extension power by increasing the moment arm of the knee extensor tendon [111]. Subsequently, during TKA, preserving patellar height relative to the joint line is very important in restoring knee extension power and function while adequate reconstruction of patellar thickness is critical for optimal patellofemoral (PF) tracking and lever arm strength [22,32,98,103,197].
Patellar reconstruction in rTKA or re-revision TKA creates treatment challenges as reconstruction of a failed patellar implant is associated with unique issues, particularly a limited amount of residual bone stock, poor biology and blood supply, and high mechanical loads across the PF joint. Even though the number of rTKAs and re-revision TKAs are increasing [180], the literature provides limited guidance regarding optimal management of the patella and patella bone loss in the revision setting. Unfortunately, the literature contains few prospective and comparative studies on patellar reconstruction techniques in revision TKA [139]. As such, treatment recommendation is often based on case series and expert opinion. To provide assistance in decision-making surrounding patellar bone loss and present adequate ways of managing it, the consensus group answered answer targeted questions on this topic. Because the literature does not have a clear answer to these questions, a group of experts were recruited to provide opinions gleaned from high volume revision practices and extensive experiences managing these types of complex cases.
Question 1: What Are the Best Imaging Modalities for Assessing Patella Component Fixation and Patellar Bone Loss?
Several differential diagnostic algorithms have been developed for complicated TKA, including imaging studies [65,92,177]. Obtaining plain radiographs is the first step in evaluating painful TKAs, patellar component fixation, and presence of patella bone loss (Fig. 5). Although several more advanced imaging modalities such as CT, MRI, SPECT-CT and stress radiographs may be useful, the consensus group did not believe that they should be routinely ordered for evaluation of patella component fixation or patellar bone stock. However, assessment with advanced imaging may be beneficial in special cases.

Standard radiographs for patellar bone loss in anteroposterior (AP), lateral, and merchant views.
The radiographic examination evaluates for presence of periprosthetic patella fractures, osteolysis, radiolucent lines around the button, malposition and patellar maltracking [65,92]. A standard panel of radiographs should include weight-bearing AP, PA 30 degree flexed view, and lateral view, as well as a merchant view to assess the patellofemoral joint [13,65,90,137,149]. The AP view is the least instructive on the status of the PF articulation and rarely has diagnostic value. On the lateral view, the position of the patella can be assessed for either patella baja or alta. In addition, the lateral view provides an estimation of the cement bone interface around the pegs of a cemented component. Avulsion of the proximal pole can also be assessed [90,137,149]. The merchant or skyline view provides an assessment for patella tracking in the unloaded, flexed knee position. It also allows for additional assessment of the cement-bone interface [13,90,149]. The authors believe that when evaluating patellar bone loss, standard radiographs alone suffice as the necessary imaging modality [149]
A CT scan has a high sensitivity and specificity for the diagnosis of osteolysis around TKA [144,172,186,208]. Furthermore, CT can be useful in evaluating implant malrotation [24,65]. Since it was first introduced, CT has undergone major technological improvements and it has become a mainstay in imaging osteolytic lesions following TKA. With the use of various techniques and protocol modifications, artifacts that may compromise visualization of bone and soft tissues close to metal implants have been dramatically reduced [45]. It has been reported that CT scans with metal artifact suppression improve the sensitivity of detecting osteolysis around TKA to greater than 70% [112]. Although there have been notable advances in technological matters and the available protocol adjustments, the presence of some metal artifact is inevitable.
There are various studies that report CT has superior results than plain X-rays in detecting osteolysis around TKA implants [45,112,144,167,172,186,194], and there is increasing support for the use of CT for assessment of periprosthetic bone around TKRs. It is believed that CT may provide a quick, technically simple, highly accurate and reliable form for volume measurement of osteolysis [112]. If surgeons are unsure of the status of patellar bone loss after standard imaging, we advocate the utilization of a CT scan as the subsequent step as this modality offers better bone detail.
However advanced imaging, including CT, is not recommended for routine evaluation because of cost and increased exposure to radiation [186]. The radiation dose of CT can be 80 times as large as that of any plain radiography and comes with a significantly higher cost [144,194]. In addition, the techniques that reduce artifacts through modification of CT parameters require an additional increase in the radiation dose above standardized CT [167,211]. Furthermore, while CT has been documented to produce significantly higher sensitivity and specificity for the detection of osteolytic defects than plain X-rays, the sensitivity of CT for larger bone defects was higher than its sensitivity for small bone defects [194]. A CT scan, which allows for assessment in 3 planes, offers an greater evaluation of the cement bone interface, and allows for the identification of additional areas of osteolysis [90,137]. However, there is minimal data available in the literature on the use of CT in the systematic assessment of patella fixation and bone loss, as well as its relation to intraoperative management.
MRI is the preferred method for evaluating the joint and the surrounding tissues in the native knee [48,177]. However, after TKA, its diagnostic value might be limited due to artifacts caused by the metallic implants [193]. Nevertheless, compared with radiographs, MRI is considered a highly effective method for evaluating osteolysis in patients with superior sensitivity and accuracy [45,172]. There are several studies that support MRI with metal artifact reduction sequences being useful for evaluation of the periprosthetic soft tissues and the component-bone interface for osteolysis in TKA [55,67,87,148,190,194,208]. Metal suppression MRI has been an excellent advancement that allows for bone and soft tissue assessment around titanium and even cobalt chrome implants [167].
Regarding loosening of the patella component, Endo et al [55] showed that sensitivity and specificity of MRI were 84 and 85%, respectively, while for radiography they were 31% and 96%, respectively. The higher sensitivity of MRI compared with radiography is supported by the documented poor sensitivity of radiography for osteolysis [172,194]. It is important to note that MRI may overestimate loosening of the patellar component, because it can show radiolucent lines at the bone-cement interface of the patellar button, which may not necessarily mean that the component is loose. MRI is considered an advanced imaging and is not recommended for routine evaluation because of its cost and the lack of need for its level of imaging [112,186,200].
However, MRI is uniquely suited for assessment of patella fixation for multiple reasons [67,90,193]. First, the cement-bone interface and the cement-patella component interface are separated from adjacent metal thanks to the thickness of the patella component. This allows for minimal to no artifact impact from the cobalt chrome femoral component. It also enables MRI to provide optimal clarity of the fixation interface [67,90].
Second, regarding patellar component fixation, usually a loose patella component has debonded from the underlying cement mantle. When assessing for fixation of a patella component intraoperatively, the consensus opinion was to assess the patellar component/cement interface with either the tip of the diathermy or the tip of a knife and determine whether the interface is sealed.
Nuclear studies have been proven to be sensitive, but nonspecific, regarding TKA pathology. Technetium-99m (99mTc)-, gallium-67 (67Ga)-, and indium-111 (111In)-labeled bone scans are used to investigate problematic TKAs, but these have low specificity. Furthermore, nuclear studies can yield false-positive results because they may detect a normal inflammatory physiology for up to 2 years after undergoing TKA [65,137,161]. As a result, routine use of nuclear studies in the evaluation of painful TKA is not recommended and the authors do not believe it useful for evaluating patella fixation.
There are other imaging techniques such as scintigraphy, single-photon emission computed tomography (SPECT), or positron emission tomography (PET)/CT that may be used for further diagnostics; but the literature exploring whether or not these can establish the correct diagnosis is limited. Combined single-photon emission computerized tomography and conventional CT (SPECT/CT) has been increasingly used in patients with pain after TKA. Although there are studies that advocate its beneficial clinical use in patients after TKA by accurately determining periprosthetic bone tracer uptake and the position of TKA components, there is still a debate regarding if SPECT/CT really leads to improved diagnostic accuracy [151].
In the majority of cases, X-rays are considered to be adequate for the assessment of patella bone loss. Advanced imaging such as MRI and CT is not recommended for routine evaluation of problematic TKA and thus is not indicated for evaluation of the patella bone loss or patellar button fixation alone. Standard imaging for patella bone loss is recommended to be X-rays alone, which should include weight-bearing AP, lateral views, and a merchant view. If the surgeon feels it is necessary to accurately define remaining patellar bone for planning purposes, CT is the best imaging modality.
Question 2. Is There a Satisfactory Patellar Bone Loss Classification? If Not, Should There Be?
Although the number of rTKAs is increasing, there remains inadequate data to guide best treatment options for management of patellar bone loss. For example, the Anderson Orthopedic Research Institute (AORI) classification [59] which is commonly used to describe bone loss in revision TKA is focused to femoral and tibial bone loss, and does not have a patellar section [182].
In 2015 an updated radiographic assessment and evaluation system was developed approved by the Knee Society membership [142]. This Modern Knee Society Radiographic Evaluation System provides radiographic assessment of coronal and sagittal implant fixation focusing on the implant-bone interface with respect to radiolucent lines and osteolysis. It also includes a zonal classification system to describe locations of bone deficiency. This modernized system is more descriptive and more detailed, compared with the previous version, and offers a simplified and standardized method of describing the locations of radiolucent lines and osteolytic regions. This system has included the patella and its implant into its methods of identifying zones of radiolucency and bone thickness (Fig. 6).
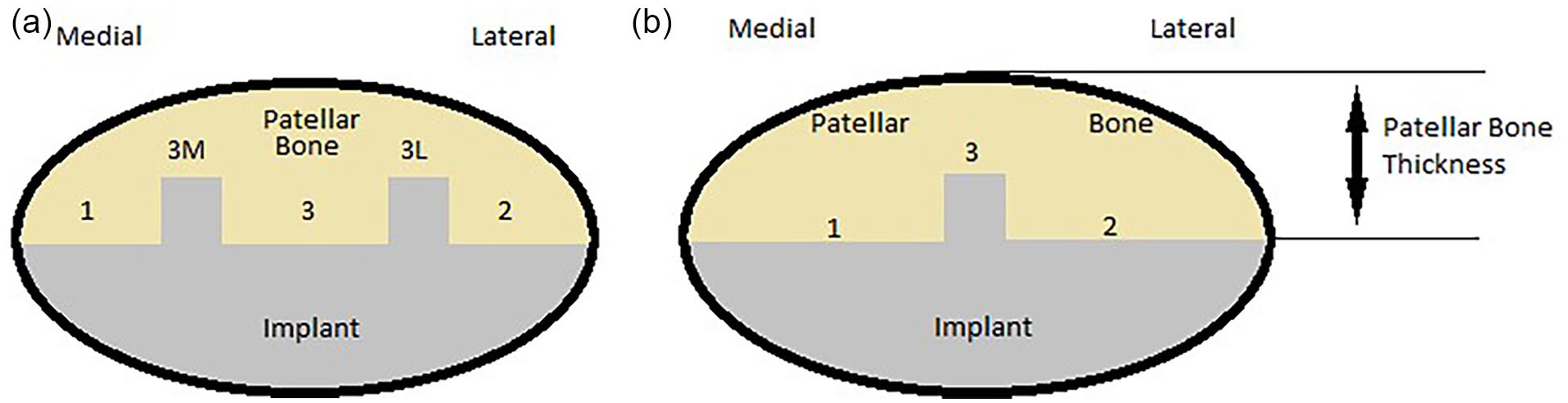
Bone thickness measurement of multi-peg (a) single-Peg (b) in patellofemoral view.
The patellar implant is divided into 3 general zones on the various radiographs. Zones 1 and 2 are on the periphery (medial/lateral), while zone 3 is designated to the central region which encompasses the pegs and the central region between them (Fig. 6a). Also, patellar bone thickness is measured in mm and noted [142] (Fig. 6b).
Patella component patellofemoral view:
Zone 1: medial.
Zone 2: lateral.
Zone 3: central peg/baseplate region (“M” and “L” designate the respective regions on the merchant view, whereas “S” and “I” designate the superior and inferior regions on the lateral view).
However, this is a descriptive evaluation system without much predictive or prognostic potential, with its focus on the uniformity of assessment and documentation.
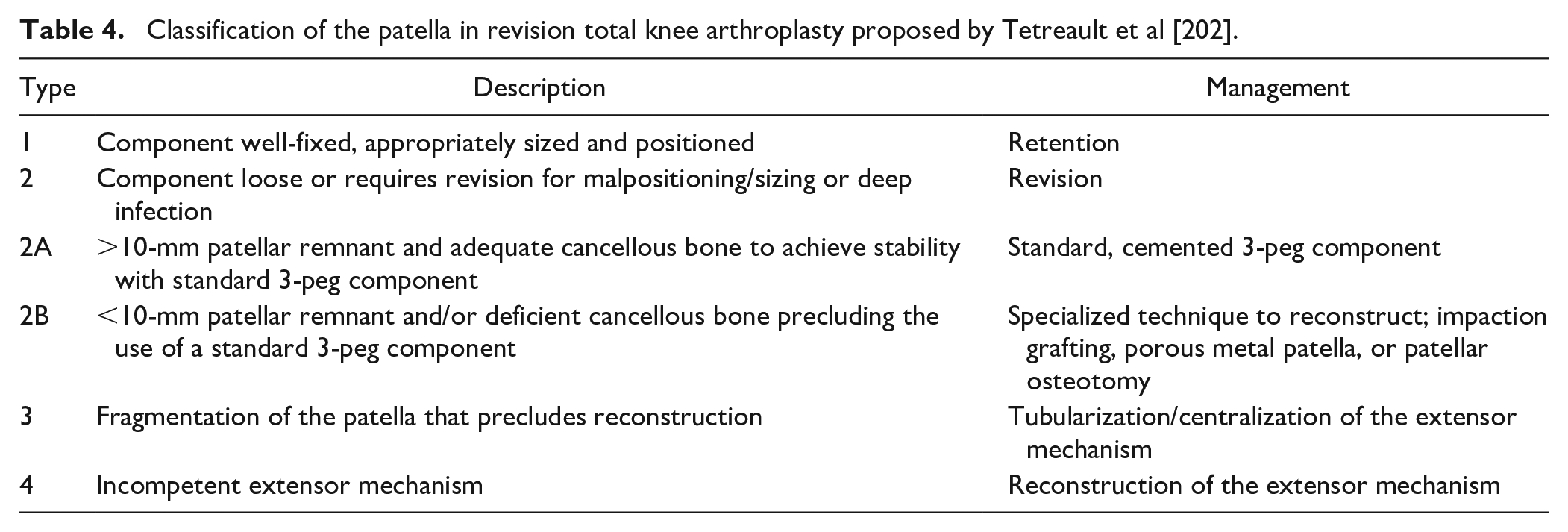
Tetreault et al [202] proposed a classification system that takes into account stability, size, and position of the patellar component; thickness and quality of remaining bone stock; and the extensor mechanism’s competence (Table 4). According to this classification system, type 1 describes a component with an appropriate size well-fixed in good position and suggests retention. Type 2 describes a component that requires revision because it is loose or due to malpositioning/sizing or deep infection. Type 2 is divided into 2A and 2B. Type 2A refers to a >10-mm patellar remnant with adequate cancellous bone, capable to achieve stability with a standard 3-peg component. Type 2A suggests the use of a standard, cemented 3-peg component for revision. Type 2B refers to a <10-mm patellar remnant and/or deficient cancellous bone that precludes the use of a standard 3-peg component. Type 2B suggests the use of a specialized technique to reconstruct like impaction grafting, porous metal patella, or patellar osteotomy. Type 3 describes a patella with fragmentation that precludes reconstruction and suggests tubularization/centralization of the extensor mechanism. Type 4 describes an incompetent extensor mechanism and suggests its reconstruction.
Classification of the patella in revision total knee arthroplasty proposed by Tetreault et al [202].
In a paper describing patellar rebar augmentation, McPherson et al [139] proposed a modified classification system (Table 5) that was used to guide treatment. This system combines both the condition of the cortical rim of the patella and the cavitary bone loss to describe the patellar defects. There are 3 types (1, 2, 3) in this classification and each is divided into 3 more (A, B, C). Type 1 describes an intact cortical rim. Type 2 describes a rim with deficiency
McPherson et al Classification System of Patellar Defects in Revision Total Knee Arthroplasty [139].
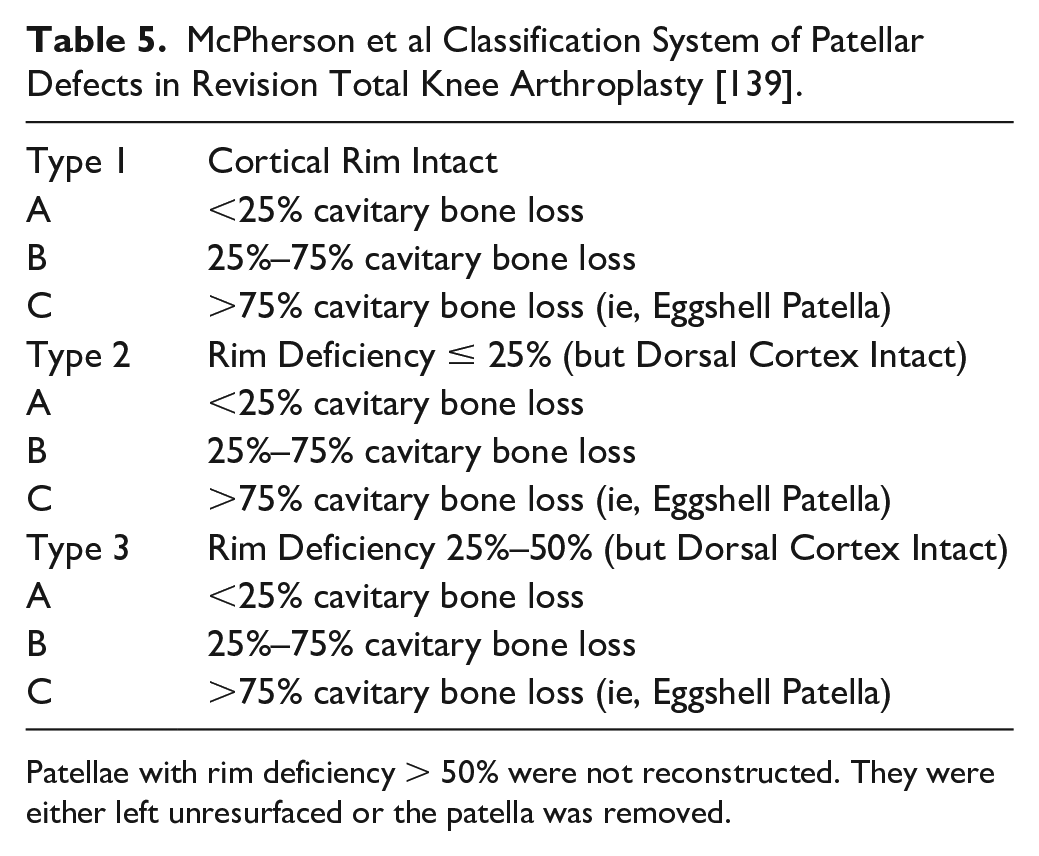
Patellae with rim deficiency > 50% were not reconstructed. They were either left unresurfaced or the patella was removed.
The classification systems currently available to assess patella bone loss do not seem to be adequate. They are either complicated with a multitude of possible options, or too simple in that they do not actually direct treatment. A classification system that would simply classify the status of the patella before the revision surgery and suggest the appropriate reconstruction technique should be available.
This classification system (Table 6) aims to guide surgeons with a simplified assessment of the patella status and assist them in selecting an appropriate surgical treatment. Also, the consensus panel members feel that the surface of the remaining patella has been underestimated in the past and that it should be part of the classification system. If the patella implant is not loose and appears to be stable while even presenting some wear, (type 0), then it the suggestion is to retain it and proceed to other steps of the rTKA process. Especially in a case with a well-fixed, problematic patellar polyethylene in a thin patella, leaving the implant as is should be considered. If the patella remnant appears to have adequate surface and bone stock for reimplantation of a button (thickness >10 mm) then reimplantation of a button is strongly recommended (type 1). In the case that the patella has a thickness of less than 10 mm, then the surgical options depend on the bone stock left. If the thickness of the patella is 5 to 10 mm (type 2), then options include patelloplasty, bone grafting of the remaining patella, or implantation of a bi-convex patella. If the patella has a thickness less than 5 mm (type 3), the options include patelloplasty, bone grafting, use of tantalum, or use of the rebar technique. However, we must note that most of the consensus panel members stated that they would prefer leaving the patellar remnant as is or to performing a patelloplasty. In addition, if during a rTKA the patella presents with avascular necrosis or fragmentation (type 4) (Fig. 7), it is suggested to retain the patella remnant as is or to perform a patellectomy if fragmentation is symptomatic.
New classification system proposed by the consensus group.
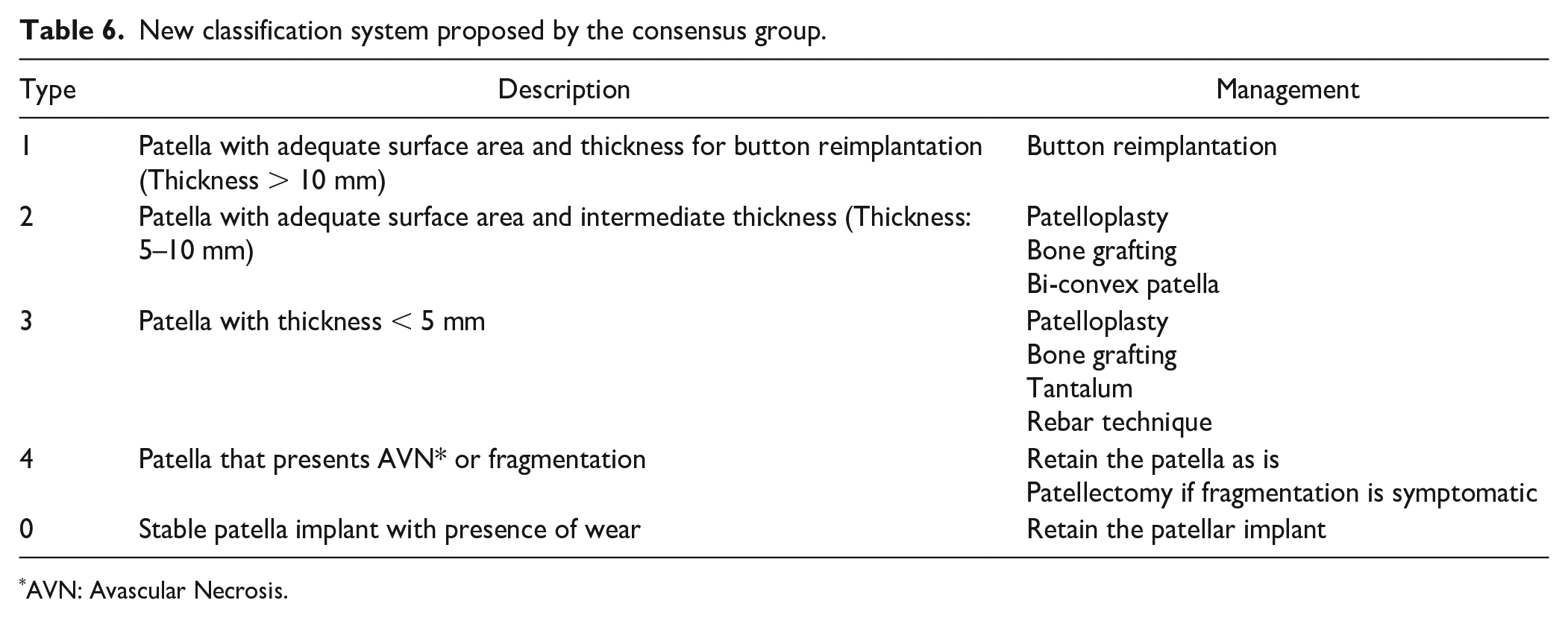
AVN: Avascular Necrosis.
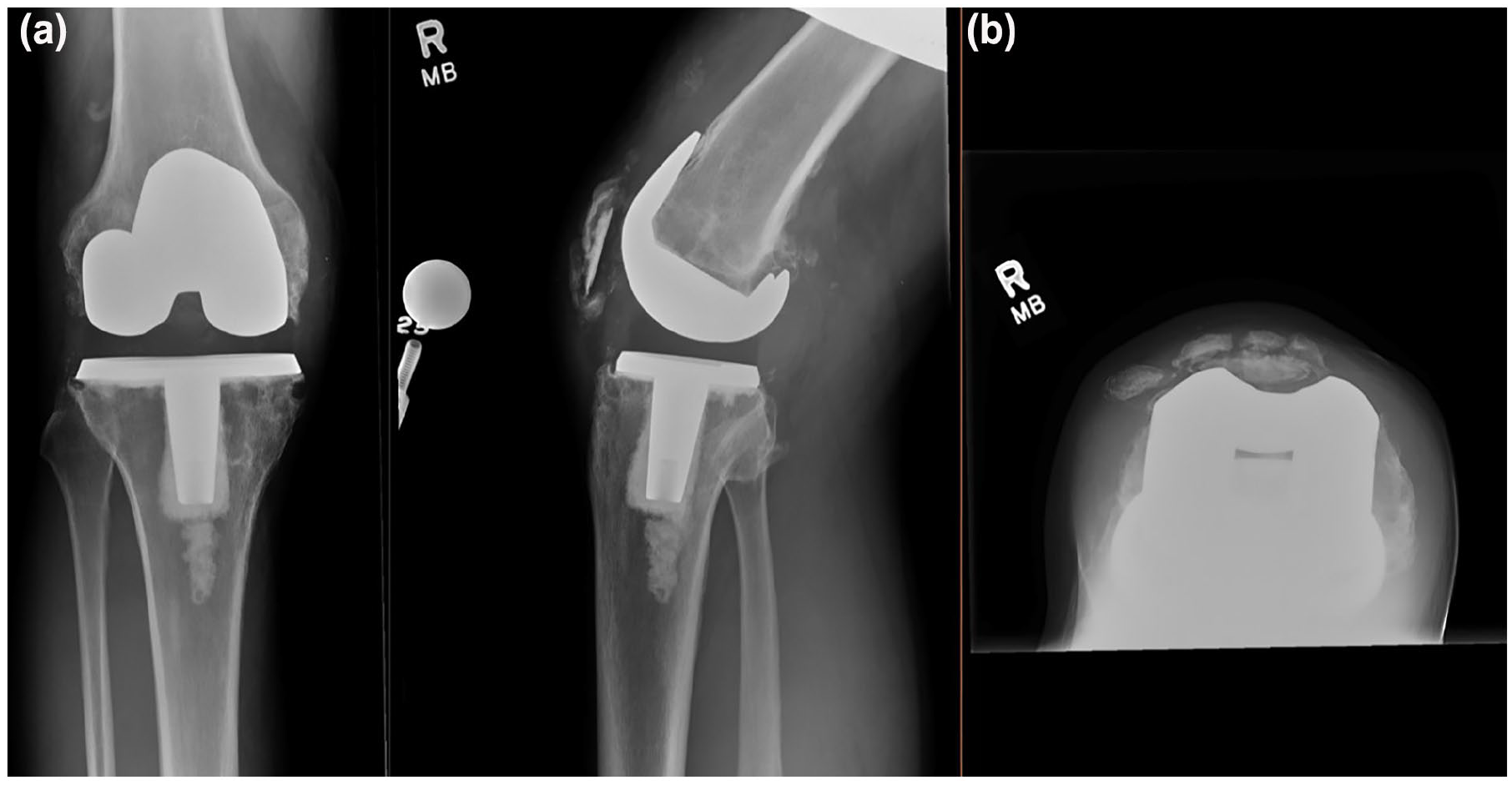
Patella with signs of fragmentation: (a) lateral view and (b) merchant view.
Question 3. What Are the Surgical Options for Reconstruction of the Patella in the Setting of Severe Bone Loss (Patelloplasty, Bone Grafting, Rebar Technique)?
The role of the patella is crucial for the good function of a TKA and proper reconstruction is required. Adequate reconstruction of patellar size and positioning is also critical to patellofemoral tracking [139,159,163]. The issues that may occur during a reconstruction procedure may vary since the patella bone is small (relative to the resurfaced femur and tibia) and has tenuous blood supply [6,201]. In addition, aggressive bone resection may leave little bone remaining, which can be dangerous since patellar bone thickness of less than 10 to 12 mm is considered a risk for fracture when resurfaced with a pegged implant [187]. There is always the possibility the bone holes drilled for the pegs exit the dorsal cortex and create stress points for fracture. Another issue is that the remaining patellar bone is often of poor quality for cement fixation. The remaining cancellous bone can be sclerotic or filled with fibrous tissue, while sometimes the remaining patella is just a cortical eggshell [68,81]. Furthermore, the inherent stability of the component is affected by the size of the cancellous defects, the number of holes with a defect, and the capacity of cement to interdigitate with the cancellous bone [19]. Finally, polymethyl methacrylate (PMMA) is weak in tension and shear forces. The bending forces that are applied on the patellar bone impart tension and shear forces onto PMMA which are amplified in the revision setting when the patella bone is thin and weak. This situation can lead to early cement fatigue and implant loosening [115,133,198,210].
The matter of the optimal revision remains debatable and a major choice must be made by the surgeon. Based on the previous classification and the practice principles it establishes, the surgical options available are: retention of a well-fixed component, reimplantation of a patellar button, patelloplasty, the gull-wing osteotomy, impaction bone grafting, use of a biconvex all-polyethylene component, use of tantalum, the rebar technique, and patellectomy.
Retention of a well-fixed component
When the inspection of the patella during a rTKA reveals a well-fixed patellar implant that may have some degree of wear (type 0), retention of this patellar implant should be considered. This approach is not only obviously easy, but also helps the surgeon avoid additional complications by preserving the bone stock unharmed [126,133]. It is important to confirm intraoperatively that the implant is not loose and has adequate fixation, because there might be a discrepancy with the imaging results [82]. In previous studies a high percentage of patella retention has been noted in revision TKA; in a study by Tetreault et al [201] patella retention was up to 69% [16,17,133]. This approach seems to become common in contemporary practice and is characterized by rather low rate of failure [17,126,135,164,188,201]. Furthermore, in cases when the removal of a well-fixed patella leaves a remaining host bone less than 10 mm in thickness, retention of the implant should be considered. Identifying the amount of wear and deciding if it is acceptable could be a difficult task. Lonner et al [126] recommended retaining the implant only if there is mild deformation due to cold flow and no pitting or delamination. Indications for removal in these cases should be: severe wear or the patella component is metal backed with visible wear; the implanted component is seriously malpositioned or incorrectly sized; the patellar composite is overly thick [68,175,201]. Shield et al [188], in a 2019 study with a minimum 5-year follow-up, report no subsequent failures of the patella in 130 rTKAs where the patella component was not revised despite the presence of mild patella polyethylene wear and mismatched shapes in several cases. In general it believed that in the majority of rTKAs the risks of patellar component retention are outweighed by the benefits [17,126,188,201].
Revision using a standard component
During TKA revision, the surgeon first must decide if there is a need for the patellar component to be revised and then whether or not a new patellar component should be placed. While the patellar revision can optimize the patellofemoral congruency, it may compromise the bone stock and subsequently increase the possibility of further complications [19,133]. The most common reasons for revising a patellar component include loose component or significant wear, malpositioning, maltracking, instability, or even anterior knee pain [133]. After removal of the patellar component, the patella thickness is measured. It has been reported that revision and reconstruction of the patellar compartment should be based on assessment of remaining patellar bone stock, while severe patellar bone loss may preclude adequate fixation for patellar prosthesis [82]. Previous studies have reported that a minimum 10 to 12 mm of bone stock must be present to resurface the patella. This bone stock would allow extensor mechanism to function and not drill through the anterior cortex of the patella [19,68,170,175].
After the implant removal, if the remaining patellar bone remains reconstructable with adequate surface area and bone thickness > 10 mm (type 1) the type of patellar component is the next consideration. A standard 3-pegged all-polyethylene component has been described as a successful choice [202] and is suggested for type 1 patellar bone defects with a concomitant lateral facetectomy. Also, it is recommended to downsize the patella to optimize tracking if needed. Reimplantation of a standard 3-pegged all-polyethylene component is a simple technique, familiar to most surgeons. It requires adequate remaining cancellous bone to provide some inherent stability and to accept cement for interdigitation for long-term fixation [15,17,133,202]. There are no data to support implantation of an uncemented primary patella in a revision TKA, and future studies could provide more information regarding this option. Currently, the members of the consensus group do not support it and are in favor of cementing the patella in revision cases.
Isolated patellar revision is associated with high complication rates and recurrent failure, usually when poor patellar tracking, incongruent designs, and malalignment of the femoral and tibial components exist [82,133,175]. Also, patellae with severe bone deficiencies that do not allow adequate fixation of another patellar implant, occur in approximately 10% of revision knee replacements and this is seen more commonly in septic revision cases [75,115,139]. However, in the setting of 2-stage revision for infected TKA, Tetreault et al [202] found that 75% of patellae could be resurfaced with a standard all-polyethylene component. This result is in accordance with a previous study by Glynn et al [75], who reported resurfacing the patella with a new implant in 78% of cases, leaving the patella unresurfaced 12.9% of the time. Septic rTKA requires a lateral retinacular release more frequently than aseptic rTKA according to Tetreault et al [202] (38% vs 14.5%).
Patelloplasty
Retention of a patellar bony shell, or patelloplasty, is an option suggested for patella Types 2 and 3, when the thickness of the patella is less than 10 mm. After the patellar component has been removed, all the surrounding soft tissues must also be removed to provide adequate exposure of the patella. In this way, a complete assessment of the reconstructability of the patella can be conducted. Afterward, if patelloplasty is decided, all loose bone and cement must be removed from the patella and trimming all overhanging bony structures should be done [46] along with a lateral facetectomy.
This technique appears to be a simple, inexpensive solution with decreased operative time. However, it can lead to complications like maltracking, osteonecrosis, fracture, persisting stiffness, extensor lag, and knee pain [133,159]. Pagnano et al [159] reported an improvement of Knee Society score (KSS) for knee and function on 31 patients who underwent patelloplasty with a mean follow-up of 3.5 years. They also reported complications in 1/6 patients and mild to moderate knee pain persisting in 1/3 of the patients. Laskin et al [115] reported similar results in patients with patelloplasty with 2 years of follow-up. However, they also reported that the patelloplasty group in their study had a mean flexion of 120° compared with 105° in the reimplantation group [115]. Masri et al [135] in a retrospective study, found no difference between 49 patients who had a patellar component after revision TKA when compared with a matched cohort of 45 patients without a patellar component (including 3 patellectomies). The study found no differences regarding knee scores and patient satisfaction score, and the authors supported the need of further prospective randomized trials. Patil et al [164] reported an increase in outcome scores in those patients who had the patella retained without this finding being statistically significant when compared with the patelloplasty group or revision patella group. However, there were limitations with this study as it included patients undergoing revision for any reason, including infection, and a relatively small study group. In a retrospective review of 422 rTKAs performed by Tetreault et al [202], patients who had the patella component retained or revised at the time of revision (282 patients) had significantly improved functional scores compared with those who underwent patelloplasty alone (10 patients).
Although none of the reconstruction techniques have demonstrated superiority, retention of the original patella or reimplantation in the revision setting are preferable when possible. However, when the patella has to be removed during revision TKA and the remaining patella bone is inadequate for reimplantation, patelloplasty should considered as an option. If the patella tracks well in the new trochlea, this option can be well tolerated by the patients and the complications that follow the other techniques can be avoided [46].
Bone grafting
When revising a patellar component, the amount of remaining bone stock is of major importance. In general, the reconstructed patella should have a total height of 24 to 26 mm [1]. Patellae with severe bone deficiency that does not allow patellar implant can be found in about 10% of revision TKAs [81,133]. These patellae are included in Types 2 and 3 with less than 10 mm of thickness; patellar bone-grafting is among the proposed options for treatment. Hanssen presented this method for restoring severe patellar bone loss [81]. According to the procedure, a local synovially based tissue flap is created and is secured to the patellar rim, to contain cancellous bone graft inserted into the defect. Abdel et al [1] reported good clinical outcomes with a long-term follow-up, reduction of anterior knee pain, and improvement in patellofemoral mechanics with this technique. They reported a survivorship free of patellar revision of 96% at 10 years as well. The indications to perform patellar bone- grafting included: severe cavitary or segmental defects; an unsupportive rim of bone; bone stock of <10 mm measured with a caliper. The mean thickness measured intraoperative prior to patellar bone-grafting was 7.4 mm. A modification to this bone grafting method has been presented by Boettner and Bou Monsef [28] using an Achilles tendon allograft to contain a bone graft in 3 failed TKAs for patellar bone loss. Also, they reported an improvement in the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) score from 53 to 89 points.
The main principles regarding the patellar bone-grafting technique are as follows: First, it must be ensured that the femoral and tibial components have adequate rotation to optimize patellofemoral tracking. If not, revision should be considered. Second, a contained shell of punctate bleeding bone is needed. The retropatellar surface should be prepared with a high-speed burr to increase the chance of bone incorporation. Third, the use of autologous bone as graft is preferred. Any autogenous bone harvested during component revision should be retained. In case of autologous bone is not available, cancellous allograft should be considered. Fourth, the use of native tissue should be preferred to close over the envelope such as retinacular tissue, fat pad, part of the iliotibial band. Fifth, the aim of thickness should be 30 mm as there is graft resorption. Sixth, postoperatively, limited weight-bearing and motion should be applied (Fig. 8).

The patella bone grafting technique.
Biconvex all-polyethylene component
The use of standard patellar components may be precluded in patients with a remaining patellar bone thickness of 8 to 10 mm [89,170,175]. In cases where the patella has too much cavitary bone loss to provide fixation for a standard patellar component, a biconvex inlay component may be used [133]. This technique is an available option for patellae type 2, with a bone thickness of 5 to 10 mm. Ikezawa and Gustilo have reported implantation of a biconvex patellar component in patellar shells of 5-mm thickness with no fractures at 2 years follow-up [96]. In addition, Maheshwer et al [134] reported on the use of a biconvex component in patients with average patellar thickness at time of surgery of 6.5 mm (4.5–10 mm). Postoperatively, the mean composite thickness was 14.5 mm (12.5–18 mm). There was a significant increase in the mean postoperative KSS from 47 to 65 and from 45 to 89 for function and pain respectively with no patellar fractures or revision surgeries. Hines et al [89] in a study with a cohort of 262 revision TKAs using a biconvex patellar component, reported a 10-year survivorship free of revision due to aseptic loosening or due to any reason of 96% and 87%, respectively. The use of a cemented biconvex patellar prosthesis is generally best suited to central cavitary defects of the patella with an intact rim [60,175]. This is also due to the fact that the inlay design of the biconvex patellar component allows restoration of central patellar osseous defects, preserving an intact peripheral residual rim [89].
Revision using a porous metal component
The use of trabecular metal is gaining popularity and becomes more common in all aspects of revision and primary arthroplasty procedures [119]. Regarding patellar reconstruction, PT components have been designed to allow patellar resurfacing in the setting of severe patella bone loss [68,82,99,175]. Porous tantalum patellar components can be used in cases in which patellar bone loss precludes the use of a traditional component [68]. The patellar component allows for implantation of a polyethylene patellar component to articulate with the femoral trochlea. However, the use of a trabecular metal as patellar shell requires sufficient blood supply to the residual patellar bone shell to allow for incorporation of the tantalum shell to the bone stock and surrounding soft tissues. Kamath et al [99] reported a survivorship was of 83% in 23 patients. Failures were associated with avascular residual bone and fixation of components to the extensor mechanism. The use of a PT patellar component is suggested as an option for patellae type 3, with a residual bone thickness less than 5 mm.
Gull-wing osteotomy
The gull-wing osteotomy was first presented by Vince et al in 1999 as technique to restore more normal convexity to a thin patellar remnant. This would be achieved with a longitudinal osteotomy which allows the patella to resume a V-shaped appearance, more suitable for patellar tracking [73,105,133]. The use of this technique remains limited. One study demonstrated 100% healing and centrally tracking patellae after the procedure with improved outcomes both clinically and radiographically in 4 patients [73,105]. In a series of 12 patients, Klein et al [105] also reported that the gull-wing osteotomy was an effective method for salvaging the deficient patella with 100% bony union, 100% central tracking, and statistically improved pain scores. Gililland et al [73] reported good function and no patellofemoral complications or re-revisions in 17 patients treated with a gull-wing osteotomy for an avascular or unacceptably thin (<12 mm) patella at the time of revision TKA.
Due to the limited use of the gull-wing osteotomy through the years, the consensus group believes there is limited indication for this procedure. In a case with a concave patella that is avascular or extremely thin and subluxed laterally on the lateral condyle, the gull-wing osteotomy could be considered.
Patellar rebar augmentation technique
The rebar technique is based on the industrial construction concept of metal reinforcement bars (“rebar”) into concrete. In the method presented by McPherson et al in 2021 [139], 2-mm titanium cortical screws are inserted into the dorsal cortex of the patella to augment polymethyl methacrylate (PMMA) cement anchoring to the host patella. The authors prospectively review the rebar technique to determine outcomes in revision TKA with a mean follow-up of 37 months. They report 4 patellar-related complications (3.1%) with no implant failures. The retrieval analysis revealed rigid fixation of the reconstructed patellar component in all cases. The authors progressively expanded the use of the technique to support segmental rim deficiencies up to 25% as well as larger cavitary deficiencies of up to 15 mm. The findings support that patellar rebar screw augmentation is a promising method to support PMMA in cases where the patella presents significant cavitary deficiencies and limited segmental rim deficiencies (up to 25%). The consensus group suggests the rebar augmentation technique should be considered in cases with a patella type 3, with thickness less than 5 mm.
Patellectomy
Patellectomy has been associated with significantly inferior functional results, difficulties with weakness and delayed disruption of the extensor mechanism (possibly due to abnormal knee biomechanics), diminished quadriceps torque and strength, and ligament instability. Subsequently, patellectomy is not routinely recommended and should be considered a last resort option, since it has been associated with a higher complication rate and lower functional score [133]. In 1998, Laskin noted that a total patellectomy with removal of all the bone can result in an extremely weak extensor retinaculum and lead to a secondary rupture [115]. The consensus group recommends patellectomy as an option in cases with patella type 4, when the fragmented patella is symptomatic.
Question 4. What Is the Best Way to Reconstruct the Extensor Mechanism in the Setting of Severe Tibial Bone Loss (Mesh, Allograft)?
Extensor mechanism disruption after TKA is an uncommon but devastating complication that results in significant functional impairment for patients [18,53,132]. Historical treatments for this complication include primary repair, autograft augmentation, and reconstruction with allograft or synthetic material. Nonsurgical treatment and primary repair have demonstrated poor functional outcomes and have largely been abandoned in the chronic rupture setting [31,53,215]. Because the disruption of the extensor mechanism is accompanied by a compromised vascularity that may inhibit healing potential, tissue augmentation is recommended to assist in healing. However, local tissue can be often compromised due to previous surgeries, and autograft augmentation in the chronic setting has also yielded poor results [35,53]. The current mainstay of treatment for chronic extensor mechanism disruptions is reconstruction, with either an allograft (Fig. 9) or a knitted monofilament polypropylene mesh (Marlex; C.R. Bard) (Fig. 10). These techniques have resulted in better outcomes—a recent systematic review demonstrated success of approximately 75% with each technique—as well as similar improvements in patient-reported outcome scores and postoperative extensor lag [184].
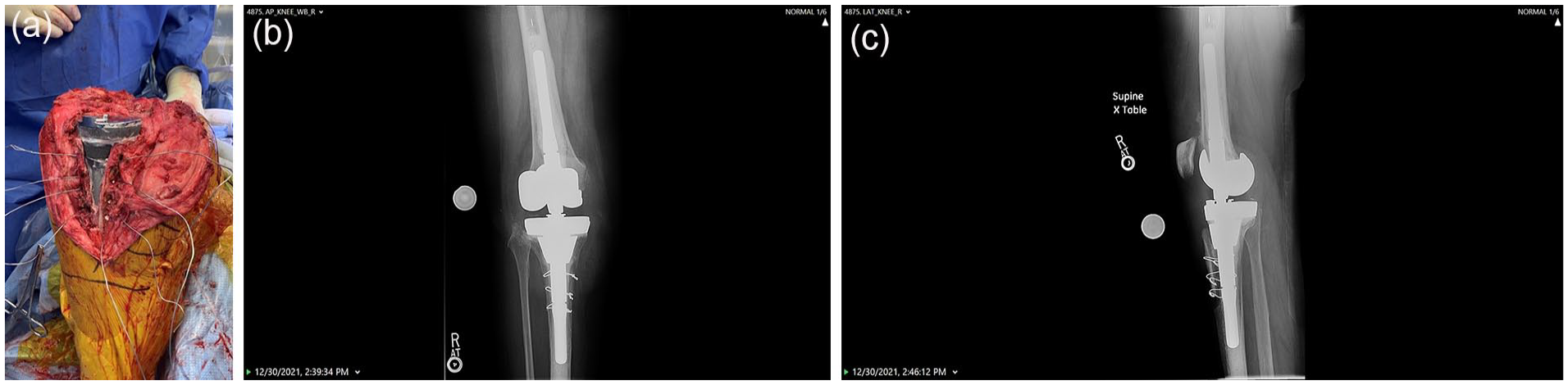
Extensor Mechanism Reonstruction with Allograft. (a) Intraoperative image. (b) AP postoperative X-ray (c) Lateral postoperative X-ray.
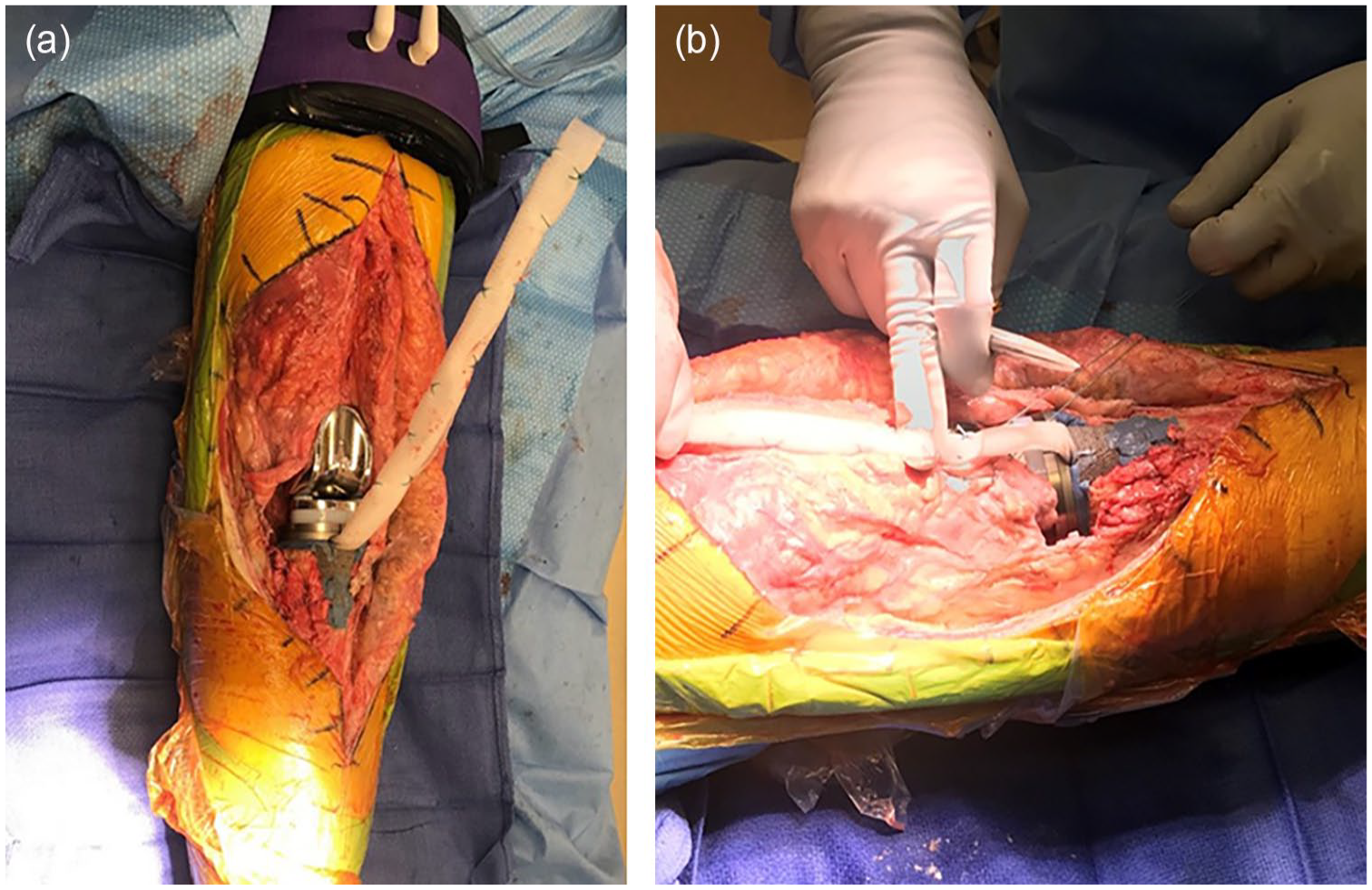
Extensor Mechanism Reconstruction with Mesh. (a) Tibial side fixation of the Mesh. (b) Mesh is incorporated into proximal soft tissue.
Regarding allograft augmentation, there have been many studies showing improved function, decreased dependence on walking aids, and maintained range of motion [18,35,51,195]. With these results, some surgeons considered allograft augmentation to be the benchmark in extension mechanism reconstruction. However, the concerns regarding this method include tissue availability, high direct costs, potential for disease transmission, attenuation of the graft over time, mechanical failure, symptomatic lengthening, and infection [18,34,117,215]. Furthermore, a considerable revision surgery rate due to graft failure (30%–60%) and infection remains [31,35,51,215]. In a cohort of 26 knees that underwent extensor mechanism reconstruction using a fresh-frozen extensor mechanism allograft tensioned in full extension, Ricciardi et al [173] reported that 69% of knees retained their initial allograft reconstruction despite reoperation rates of 58%. The mean follow-up of this study was 68 months (22–113). They found that younger age was significantly associated with failure of the initial allograft reconstruction, calling into question the durability of these reconstructions.
Compared with allografts, synthetic grafts have overall lower cost, improved availability, and no risk of disease transmission. The mesh provides a scaffold for autogenous tissue ingrowth and with direct suture fixation augments compromised host tissue and facilitates collagen formation. The synthetic material maintains tensile strength and does not elongate with time [18,32,215]. In a study of 33 cases that underwent a Marlex mesh reconstruction, Buller et al [34] reported 58% functioning reconstructions at a mean follow-up of 25 months. The 6-year survivorship was 69%; results were not influenced by immobilization type. Outcomes have continued to improve with further refinements in the mesh reconstruction technique. A more recent study reported 2-year survivorship free of mesh revision of 89% [2].
Both the allograft and mesh techniques are highly valuable and come with distinct advantages and disadvantages, making them more preferable in certain situations. In the setting of severe tibial bone loss, the authors’ consensus is that mesh is superior to allograft. When there is an uncontained anterior tibial bone defect, mesh is superior as it can be docked into the implant construct through an intramedullary technique as previously described [2,32]. Allograft is less ideal in this situation as there is poor bone in the anterior tibia to dock the allograft tubercle into, and fixation of the allograft bone block into host bone is tenuous. Furthermore, the cost and availability of mesh are superior and play a role in the setting of a revision when costs and case complexity can already be quite high. However, there are a few important considerations when using a mesh reconstruction in the setting of severe tibial bone loss. First, if one plans to use a cone and place the mesh intramedullary, then you must have a sufficient cone diameter to fit the entire construct (ie, stem, mesh, and cement). In cases like these, preoperative planning plays a crucial role, particularly when assessing the patient’s size and determining the appropriate size of the likely implanted cone. Similarly, if one is planning to use sleeves, then the intramedullary technique requires modification as you will not be cementing the mesh into the sleeve construct.
Question 5. Should Tibial Tubercle Bone Loss Be Managed Differently With Regard to Reconstruction Technique?
When performing revision surgery on a knee with significant tibial tubercle bone loss, surgeons should take additional factors into account to prevent the disruption of the tubercle or patellar tendon. Surgeons should minimize stress on the extensor mechanism during the approach as much as possible. Minimizing retraction of the extensor mechanism as much as possible is the first key principle, and if this does not allow for adequate exposure then other techniques, such as the quadriceps snip and the femoral peel, can be instituted [8,70,116,213]. Similarly, with regard to the reconstruction there are different techniques that can be employed to minimize stress on the tibial tubercle. Surgeons should consider not broaching a sclerotic proximal tibia with tubercle bone loss. This can be accomplished using a ream-only cone, or using a burr or other instrument to create the cavity for a sleeve or cone that usually requires broaching. There are several options if the tubercle breaks intraoperatively. In general, fixing the tubercle is unlikely to work in this setting as there will be poor bone stock, which does not allow for the necessary biology and fixation to obtain healing. If one is revising the tibial component, then mesh may be indicated and can be docked into the construct using the intramedullary technique. Augmentation of the patellar tendon with a hamstring can also be considered.
In addition to demanding careful attention to the extensor mechanism, tubercle bone loss indicates that there is metaphyseal bone loss, which must be considered when planning for the reconstruction. The concept of zonal fixation to determine where fixation must be obtained during revision TKA has gained popularity in recent years [147]. In this framework, there are 3 zones; zone 1 is the epiphysis, zone 2 is the metaphysis and zone 3 is the diaphysis [147]. The tibial tubercle is in zone 2, so if there is tubercle bone loss this raises 2 issues. First, there is likely compromise of both zone 1 and zone 2. This means that surgeons should achieve solid zone 3 fixation in the diaphysis. Secondly, if there is tubercle bone loss then this makes achieving zone 2 fixation with a cone or sleeve more difficult. Surgeons must be very careful with a cone or sleeve to not disrupt the tubercle in situations where there is bone loss, as this is a catastrophic complication. Surgeons should be wary of the size of cones and sleeves and should minimize broaching if possible.
Question 6. Management of Tibial Tubercle Osteotomy (TTO) in Conjunction With Significant Metaphyseal Bone Loss: How Does a TTO Affect Zonal Fixation Recommendations?
Significant metaphyseal bone loss also complicates reconstruction in settings where a tibial tubercle osteotomy (TTO) is required. Zone 2 is often where the best long-term fixation is obtained in the revision setting, and a TTO can compromise this fixation in certain situations. Although the rates of TTO in revision TKA have decreased over time, with the authors believing that TTO is generally not required during revision TKA, there are still cases where it may be necessary. The authors believe that TTO should generally be reserved in cases where it is needed for implant removal. This may be necessary with long cemented stems as well as cone and sleeve constructs. A TTO may also be indicated in situations where it is required to achieve patella baja correction, although this is rare. When reconstructing beyond a TTO, the authors recommend bypassing the TTO with either a cemented or cementless stem. If one is using a fully cemented stem, then the TTO should be closed prior to implantation of the construct to allow for pressurization of cement. If one is using hybrid fixation with a cementless stem, then the TTO can be closed following reconstruction. The authors believe that closing it after the reconstruction is generally preferred as it allows for minimal stress on the TTO closure during tibial implant insertion. In regard to metaphyseal fixation, cones may be preferred to sleeves in the setting of a TTO so no broaching is required, which can put the proximal tibia at risk with severe bone loss.
Panel 4: Considerations Regarding Complex Modular Replacement Systems: Condylar Hinges, Distal Femoral Replacements, and Proximal Tibial Replacements
Regarding the following questions, we aim to discuss principles of complex modular replacement systems including condylar and segmental hinges (distal femoral replacement [DFR] and proximal tibial replacement [PTR]), to delineate areas where data are lacking, and to provide expert opinion. In general, revisions using segmental replacements are complex, with high morbidity and complication rates compared with primary TKA. As such, these procedures should be performed by experienced arthroplasty surgeons at centers with expertise in complex revision knee surgery.
Question 1. While Addressing Bone Loss During Revision TKA, What Are the Indications to Use a DFR and/or a PTR?
In cases of severe bone loss during revision TKA, segmental reconstructions (DFR or PTR) should be used as a last option, considering the high perioperative complication rates and mixed mid- and long-term survivorship [23,38,40,50,66,93,136,179,191,217]. On the femoral side, conventional, nonsegmental implants such as condylar revision nonhinged components should be used, provided that the medial and lateral femoral condyles are present, bone defects are contained, and rotational stability can be achieved through augmented metaphyseal support in zone 2 with the use of cones or sleeves [147]. In cases in which collateral ligaments are severely compromised, but the remaining bone can accommodate zone 2 fixation, a condylar hinge prosthesis should be used with the goals of preserving bone and providing stable motion. Fig. 11 demonstrates such a scenario, in which a hinge TKA was utilized along with femoral and tibial cones and short cemented stems.
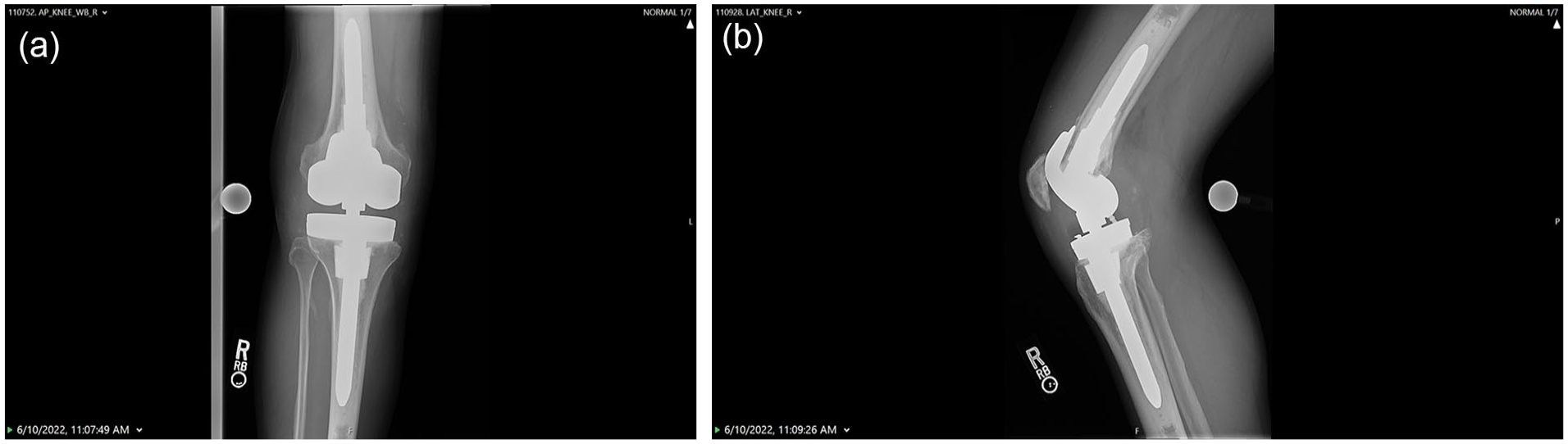
Hinge construct with femoral and tibial cones and cemented stems. (a) AP X-ray. (b) Lateral X-ray.
Regarding periprosthetic joint infection (PJI), the failure rate of DFR is relatively higher than that of nonsegmental reconstructions. A recent study by Theil et al included 97 patients treated for PJI, of which 41 received a DFR during second stage reimplantation. The 5-year reinfection rate for DFRs was 50% (34%–66%) compared with a 7% (0%–14%) 5-year reinfection rate for rotating-hinge revision TKAs [204]. This data suggests that the primary indication for a DFR is as a salvage procedure for massive femoral bone loss where only zone 3 is available for fixation.
In the setting of periprosthetic fracture, certain patterns are amenable to open reduction and internal fixation (ORIF); however, revision to a cemented DFR would be the preferred approach for highly comminuted and distal fracture patterns where adequate fixation is not possible and for situations in which the prior femoral TKA component is no longer supported due to the fracture pattern. The decision between performing a revision with a DFR or ORIF should be made on a case-by-case basis. Given the morbidity of ORIF in the elderly, frail population, DFR may be used to treat comminuted periprosthetic fractures to allow for early mobilization and full weight-bearing [49,74,120,146]. Surgeons should be familiar with the minimal bone resection required for implantation of the different segmental replacements of the knee and use the one that preserves the maximum amount of bone.
In most cases of severe tibial bone loss in revision TKA, reconstruction can be achieved with conventional revision implants that offer varied levels of constraint, often combined with augments, cones, or sleeves to achieve fixation in the metaphyseal region. Outside of oncologic reconstructions, the indications to use a PTR are limited. In cases with insufficient support for reconstruction in zone 2, a PTR should be used as a last resort, given that outcomes and survivorship are worse when PTRs are used [26,77,83,93]. It should be noted that cases with complex and massive tibial bone loss may also have insufficient soft tissue coverage, and a muscle flap may be required for coverage in this area of a reconstruction to decrease the chances of failure secondary to wound breakdown. It is the authors’ opinion that while some extreme bone loss scenarios involve an absent tibial tubercle, in less severe patterns preservation of the anterior tibial column and tibial tubercle is paramount and possible in some cases of PTR.
Question 2. What Are the Indications to Use Hybrid Stem Fixation vs Fully Cemented Stem Fixation vs Uncemented Porous Stem Fixation in Complex Modular Replacements?
Stems in segmental modular reconstructions transmit loads seen at the implant interface to zone 3, aid in alignment of components, provide temporary fixation prior to biologic ingrowth of cones or sleeves, and ultimately decrease rates of aseptic loosening. Several philosophies of stem fixation exist, including hybrid (uncemented without potential for osseointegration), fully cemented, and biologic uncemented (with potential for osseointegration). In addition, stems can be used with or without a cone or sleeve. A rarely used fixation strategy in nononcologic indications for DFR, it achieves fixation through controlled axial compression and ingrowth at the distal implant bone interface (Compress, Zimmer Biomet) [221]. A complete discussion of each of these philosophies for condylar hinge constructs, DFR, and PTR is included in Table 7.
Comparison of stem fixation options for condylar hinge components, DFR, and PTR.
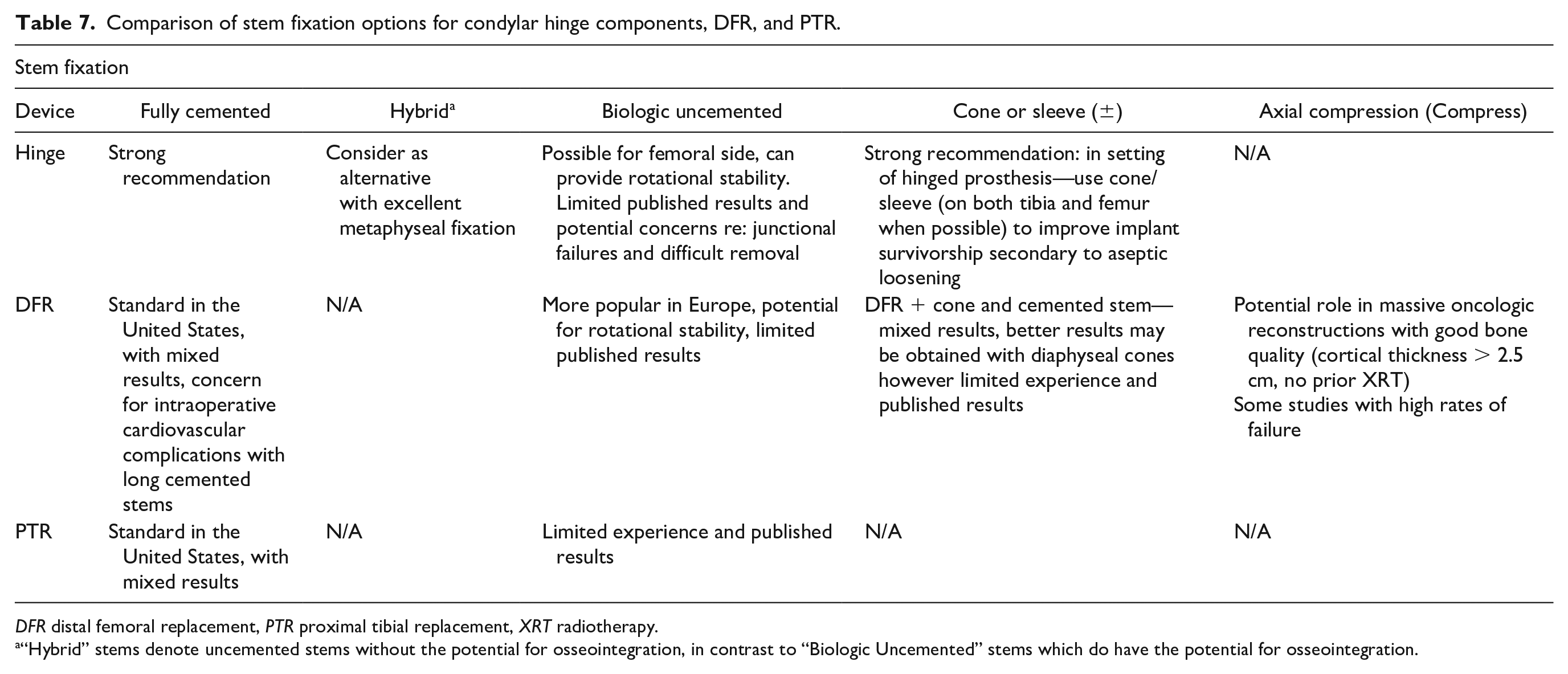
DFR distal femoral replacement, PTR proximal tibial replacement, XRT radiotherapy.
“Hybrid” stems denote uncemented stems without the potential for osseointegration, in contrast to “Biologic Uncemented” stems which do have the potential for osseointegration.
The authors strongly recommend that a cone or sleeve be used, when possible, to enhance stem fixation in hinge prostheses. In the setting of DFR, adjunctive cones have been used; however, clinical outcome and survivorship data are lacking [107]. Currently, cones are designed for augmentation of metaphyseal or metadiaphyseal fixation, rather than for diaphyseal fixation. Consideration should be given to the development of cones or sleeves for use in the diaphysis.
While fully cemented stems for condylar hinge, DFR, and PTR constructs are commonly employed in North America, published results have been varied as to their success. Much of the survivorship data regarding cemented DFRs and PTRs come from the oncologic literature, with aseptic loosening rates of 4% to 10% at 4 to 12 years and higher rates approaching 30% at 15 years in some studies [41,80,94,152,160,178]. Regarding contemporary cemented DFR for nononcologic reasons, the available literature suggests all-cause revision rates range from approximately 18% to 24% at 5 years, with one recent study demonstrating rates of 17 and 27.5% for aseptic loosening and all-cause revision, respectively, at 10 years [191,199,217]. Previously instrumented canals, which may be sclerotic in nature, can perform worse with fully cemented stems in the revision complex modular knee replacement scenario, as cement needs a more porous or cancellous surface for interdigitation and durable fixation. Hybrid stem fixation in conjunction with metaphyseal cone or sleeve augmentation is an alternative option [110,207,185]. Uncemented stems that allow for biologic fixation hold the potential for rotational stability and improved long-term fixation. One example is seen in Figs. 12 and 13, in which a tapered biologic uncemented femoral stem is employed in a DFR, in conjunction with a cone and cemented tibial stem. While there is significant interest in this uncemented biologic stem fixation in this setting, currently, published results for this approach are limited. Concerns remain regarding the potential bone loss associated with removing well-fixed noncemented stems in case of failure of the reconstruction, as well as potential bone loss associated with stress shielding.
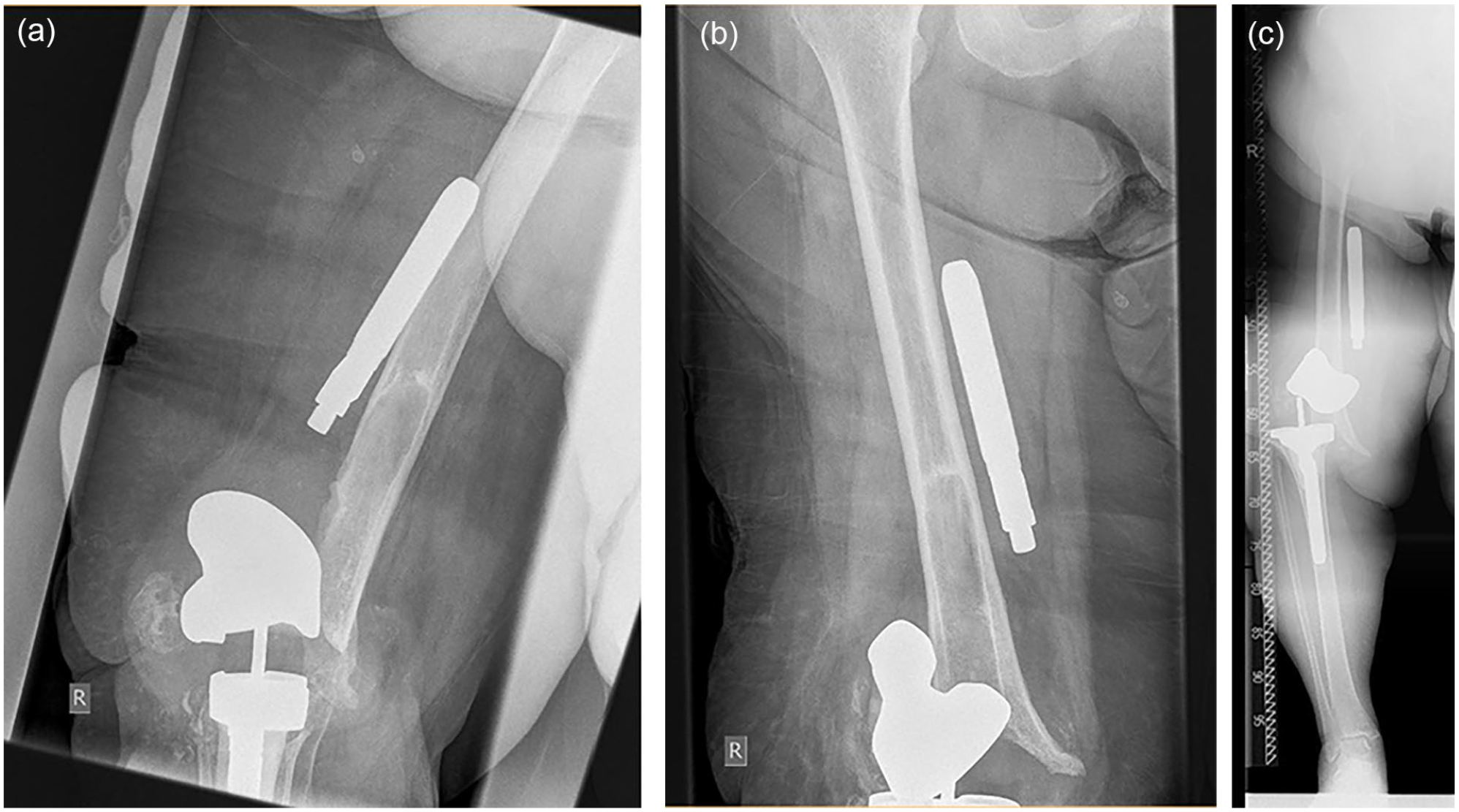
Preoperative images of a failed revision total knee arthroplasty (TKA) with massive femoral bone loss. This patient had 6 previous knee operations including multiple failed 2-stage surgeries for recurrent polymicrobial periprosthetic joint infection (PJI). (a) Lateral X-ray. (b) AP X-ray, (c) AP long standing X-ray.
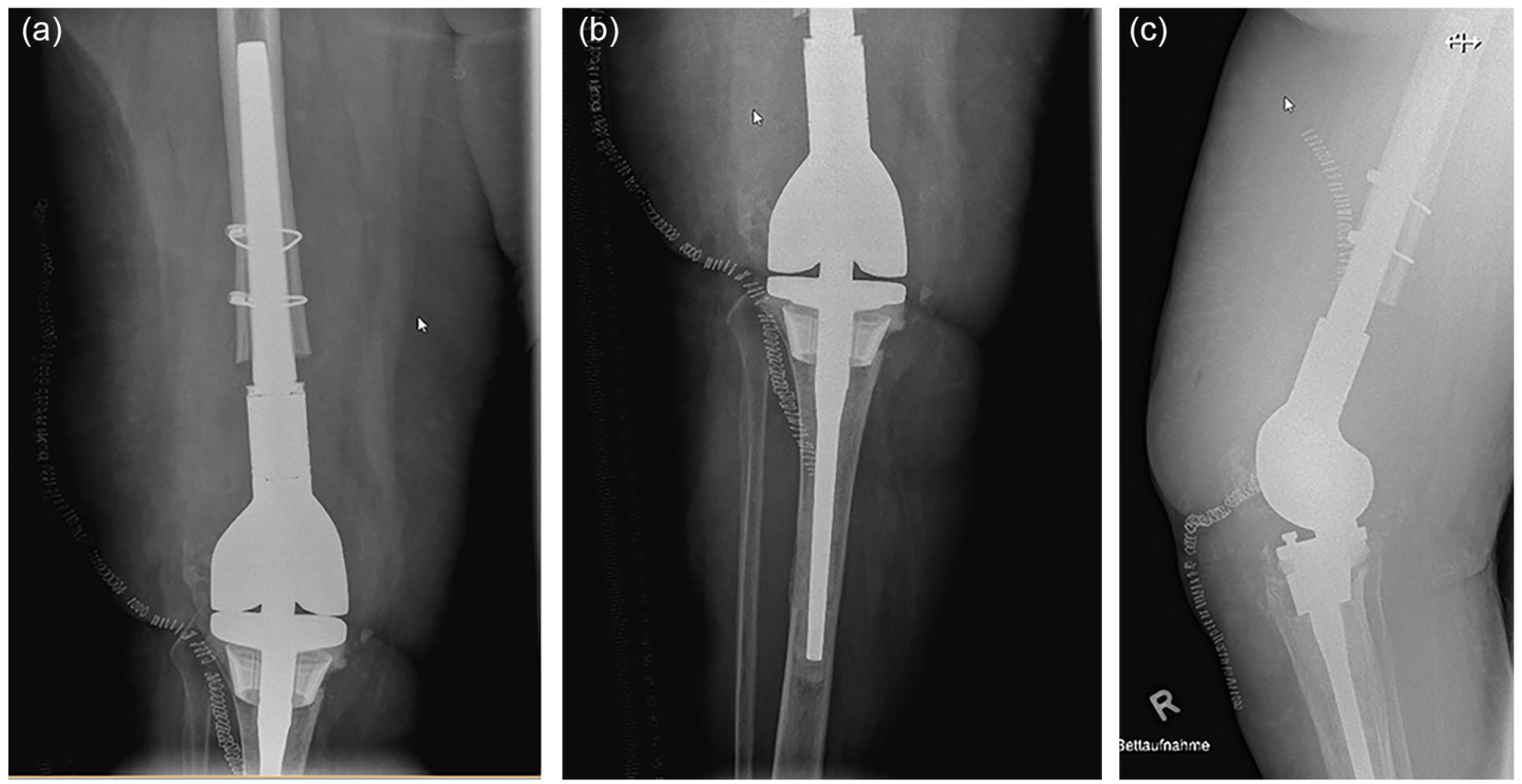
After irrigation debridement, use of a nonarticulating antibiotic spacer, as well as prolonged antibiotic therapy, the patient underwent reimplantation with a distal femoral replacement (DFR) and tapered biologic uncemented femoral stem, as well as a cone and cemented tibial stem. (a, b) AP X-rays. (c) Lateral X-ray.
Axial compression type stems in DFR have a role in massive oncologic revisions in patients with sufficient bone quality (cortical thickness > 2.5 mm), no prior radiation, and not enough diaphysis to support a conventional DFR stem. Conversely, utilizing this implant design in nononcologic revision arthroplasty that frequently affects an elderly population with poor bone stock has fared far worse than in oncologic reconstructions of younger patients [40,196,221]. It is the authors’ opinion that most complex modular revision knee cases requiring a DFR would thus be not well suited for an axial compression ingrowth femoral device.
Question 3. How Long Should the Stem Be in Complex Modular Replacement Systems?
To determine the appropriate stem length for use in segmental hinge replacements and standard condylar hinges without segmental replacement, implant-related factors should be considered, including the ratio of stem length to implant body length (including any segments added in a segmental reconstruction), stem fixation method, and use of a cone or sleeve [3,25,50,72,79,107,141,162]. Patient factors that may be considered include bone quality and body weight or body mass index (BMI). In this section, we discuss optimal stem length separately for segmental hinge replacements and condylar hinges without segmental replacement given the unique characteristics and literature relevant to each implant.
Stem length in segmental hinge replacements—DFR and PTR
In segmental reconstructions, the ratio between stem length and construct length required for adequate fixation is still unclear. The available literature suggests that outcomes are worse if a short stem and long implant body length (including segments) are present. Dhawan et al [50] found that DFRs implanted for revision arthroplasty or tumor surgery with longer bodies (>45 mm) had significantly lower survivorship than DFRs with shorter bodies (≤45 mm) when cemented stem length was kept constant. In the oncology literature, several groups reported higher rates of aseptic loosening in DFRs that replaced ≥40% of the femur compared with those that replaced <40% of the femur when either cemented or uncemented stems were used [102,157,206]. In PTRs with cemented stems, the probability of aseptic loosening increased in a stepwise fashion with percentage of tibia replaced when <40%, 40% to 60%, and >60% tibial bone loss were compared [206].
A relative paucity of literature exists evaluating stem length in segmental replacements when fixation is enhanced with the use of a cone or sleeve. The femoral diaphyseal cone fixation method described in detail by Koech et al [107] for proximal femoral replacement is equivalent to implantation of a diaphyseal cone in the context of DFR. A cone is implanted at the junction between the femoral diaphysis and the body (or segment, if present) of a segmental replacement with the goals of creating a base for the segmental replacement body (or segment, if present) to sit within a short segment of remaining femur. This achieves greater contact between the implant and bone and provides a porous surface for bony ingrowth to offload stress from the bone-cement interface [107]. This technique has been used in DFRs by the authors of the current manuscript (Fig. 14) Implant-specific sleeves are available that play a similar role in segmental reconstructions. One example is the porous metal augment—which pairs in an uncemented fashion with 3 and 5 cm DFRs—that provides augmented intramedullary fixation in the metaphysis or metadiaphysis of the distal femur (Orthopedic Salvage System [OSS], Zimmer Biomet). This system also has a porous augment that pairs with the PTR and provides augmented intramedullary fixation in the tibial diaphysis.
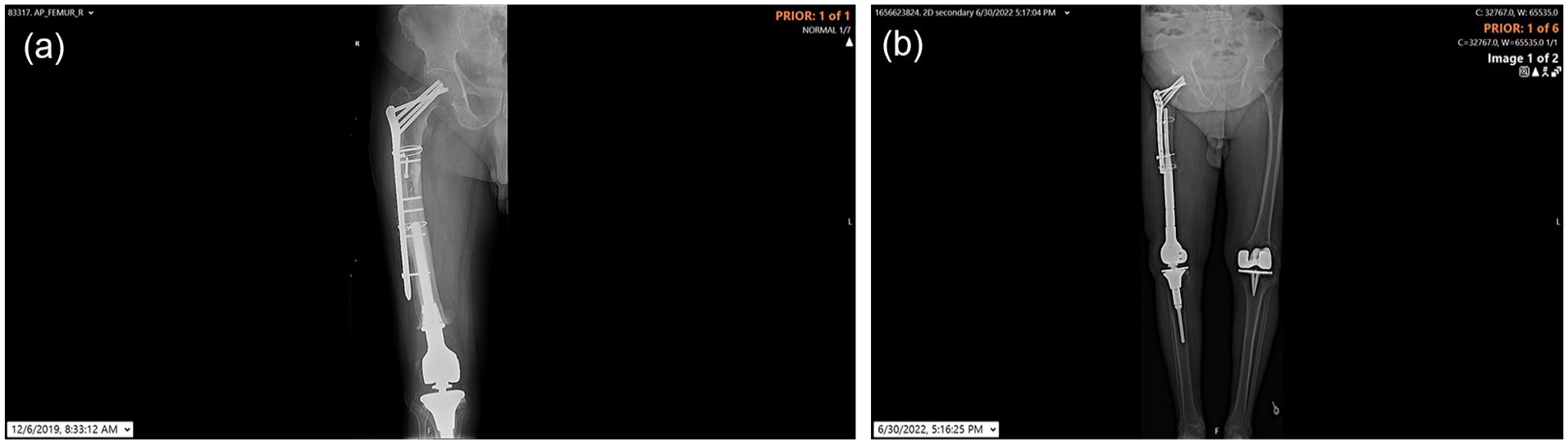
The femoral diaphyseal cone fixation method: Use of a cone and long segment distal femoral replacement (DFR), with partial hardware removal and limited proximal bone available for a cemented stem, in the setting of nonunion and bone void following previous open reduction and internal fixation (ORIF) of a periprosthetic fracture above a prior DFR.
The authors’ opinion is that in the context of segmental hinge replacements with cemented stems, the ratio of stem length to implant body and segment length should be 1:1 or greater. This is particularly relevant in patients with reduced bone quality. When the replaced segment is short, a metadiaphyseal cone can be used to augment fixation. When the replaced segment is long and there is significantly reduced femoral bone available for fixation, a diaphyseal cone can be used to augment fixation. This may allow for a shorter cemented stem to be used. The longer the segment replaced, the shorter length of native bone available for fixation [107]. In the context of uncemented stems that allow for biologic fixation [157], it is believed that use of a relatively long stem is advantageous, although stem length should be modulated to match the bowed femoral anatomy and avoid 3-point fixation, if possible. In general, both cemented and uncemented stems should be implanted with adequate fill of the canal to achieve a bone-stem ratio of ≤2.5 [25,62,157].
Stem length in condylar hinges
Fixation of standard nonsegmental condylar hinges can be attained in several zones [147]. In addition to stem fixation in the diaphysis (zone 3), fixation is created through femoral condylar capture and engagement of the box in the epiphysis (zone 1), and by cement fixation, cones, or sleeves in the metaphysis (zone 2) [147].
Limited biomechanical studies have been performed to determine the effect of stem length on outcome in hinges. Guttowski et al [79] evaluated different lengths of cemented and uncemented stems in a rotating-hinge knee model in a cadaveric biomechanical study. In an AORI 2a model, cemented stems that were 100 and 160 mm in length had similar pull-out forces and these were superior to a 160 mm hybrid stem [79].
To our knowledge, no clinical studies have been reported to date that have directly compared different lengths of stems in hinge knees. Several large clinical series evaluating outcomes following revision TKA with hinges included different implant systems with varying characteristics, including stem fixation and length [3,44,162,212]. Differences noted in survivorship and the rate of aseptic loosening across these studies could in part be due to differences in stem characteristics, although further study with direct comparison of stem length is required. Other studies compared different stem fixation methods with some variability in stem length present in patients treated with revision TKA, although only small numbers of hinges were included in these studies relative to other levels of constraint [72,165]. Gililland et al [72] evaluated revision implants with cemented stems that ranged in length from metaphyseal cemented stems to longer stems and compared these with uncemented stems that varied in length but were implanted to provide 4 cm of press-fit contact. Regardless of stem length, they found relatively low rates of aseptic loosening (3%–4%) in all patients treated with cemented and uncemented stems in revision TKA.
Cones and sleeves are commonly used to optimize metaphyseal fixation in hinges, and the use of shorter stems may be considered when concomitant cones or sleeves are used. Several recently published series evaluating hinges described the use of cones or sleeves in some or all of the patients included [3,44,118,162]. In the biomechanical study by Guttowski et al [79], in the context of an AORI 3 defect, a cemented 100-mm stem with metaphyseal cone led to improved pull-out force compared with a 160-mm hybrid stem without cone. Further study is required to elucidate the interplay between cone use and stem length in achieving zonal fixation that results in maximal survivorship.
The authors have general consensus on the ideal stem length to use in hinges. Given the potential for fixation of hinge implants in the epiphysis and metaphysis, there is less reliance on stem fixation alone than required in segmental replacements. Therefore, the use of relatively shorter stems can be considered in hinges compared with segmental constructs. Cemented stems with at least a 100-mm length should be used when possible. No clear benefit exists in using longer stems. However, short stems can be considered, especially when concomitant cones or sleeves are used. For uncemented stems, adequate stem length is required for diaphyseal engagement. The literature suggests that 4 cm of diaphyseal engagement results in adequate fixation [72].
Question 4. How Should a Previously Instrumented Canal Be Handled in Case of a Re-Revision TKA? When Should You: (a) Increase Stem Length; (b) change Stem Fixation Mode; (c) Add a Cone or Sleeve; (d) Use Impaction Grafting?
Re-revision TKA with a complex modular replacement system after a failed stemmed TKA in which the intramedullary canal has been previously violated creates a challenging situation involving bone loss and the presence of sclerotic bone that is less amenable to fixation. The authors provide a consensus opinion on how to optimize several variables related to fixation.
Stem length in re-revision
The standard practice in re-revision after failure of a previously stemmed TKA is to increase stem length. This allows for stem fixation within the native femoral medullary canal in a region that the previous construct did not contact. In addition to the adjustment of stem length, re-revision should also involve addressing bone loss, optimizing fixation with cones or sleeves, and obtaining adequate fixation in other zones, if available [147], given that the optimization of stem length alone is possibly inadequate. In general, the same recommendations pertaining to stem length should be followed as outlined in question 3 of the previous section. However, when bone loss has been addressed and fixation optimized with other methods such as cones or sleeves, the stem of the re-revision implant could be shorter than the previous implant; this might be particularly relevant if the previous stem was quite long.
Stem fixation mode in re-revision
Previously instrumented canals can pose several difficulties regarding stem fixation. If cement was used for fixation of a previously stemmed implant, it is paramount to remove all cement and pseudomembrane in the canal, which could affect new stem preparation, alignment and fixation in a re-revision scenario. In addition, in cases of PJI, retained cement could harbor infection, so all cement should be meticulously removed to remove this potential nidus of persistent infection. In general, cemented stems are the workhorse fixation method in re-revision scenarios. It is possible, however, that after removing previous implants, a sclerotic canal may be encountered. In these cases, it is the authors’ opinion that cementing into a sclerotic canal that was previously stemmed is suboptimal and may lead to increased rates of stem fixation failure. In this setting, there may be a greater role for uncemented biologic stems, hybrid fixation, or impaction grafting; this is an area for which additional research is needed.
Cones and sleeves in re-revision
Biological fixation in the metaphysis or diaphysis provided through a cone or sleeve should be used to augment fixation, when possible, during re-revision TKA. The results of several studies suggest that improved longevity and/or a reduced rate of aseptic loosening in revision TKA occurs when cones or sleeves are used in the femur and tibia [44,141,156,162]. The fixation provided via cones or sleeves is even more important when the intramedullary canal has been previously instrumented compared with those in which it has not. If a segmental replacement is used, in addition to implanting a longer stem, consideration should be given for placement of a cone at the junction between the body/segments and diaphyseal or metadiaphyseal bone (question 3) [107]. If a nonsegmental hinge is used, a cone or sleeve should be used to obtain metaphyseal fixation.
Role of impaction grafting in re-revision
Impaction grafting refers to the use of particulate bone graft, typically cancellous chips, to restore bone stock in a revision setting when minimal cancellous bone is present after removing a stem. In these cases, impaction grafting can create a medullary canal into which a new stem can be cemented with durable fixation. It is a technically demanding and time-consuming procedure but has been used for up to 4 decades with series from various institutions familiar with the technique demonstrating excellent long-term survivorship beyond 10 years [47,176]. Concerns of impaction grafting are stem subsidence and femoral fracture, in addition to poor incorporation of graft into host bone. Several studies described the process of particulate allograft incorporation and replacement with new host bone within the year after initial operation [54,122,205,216]. Several specialized centers and surgeons experienced in this technique with reported excellent outcomes; however, widespread use of impaction grafting has fallen out of favor in North America secondary to the aforementioned concerns and the availability of other stem fixation modes to address massive bone loss in revision TKA. It is the authors’ consensus that impaction grafting is technique dependent, and familiarity with this technique should be established prior to employing this strategy clinically. Current instrumentation used for impaction grafting includes a central guide wire to help in positioning of bone allograft for subsequent central insertion of a new cemented stem and appropriate bone stock restoration circumferentially around the new stem. There is certainly room for improvement in instrumentation related to this procedure, and the authors’ preferred use of this technique is in scenarios in which use of impaction grafting can restore bone stock in severe diaphyseal bone loss to avoid the use of a segmental prosthesis. Fig. 15 demonstrates a case of impaction grafting and the technique of central pin placement, graft impaction, and stem trial insertion.
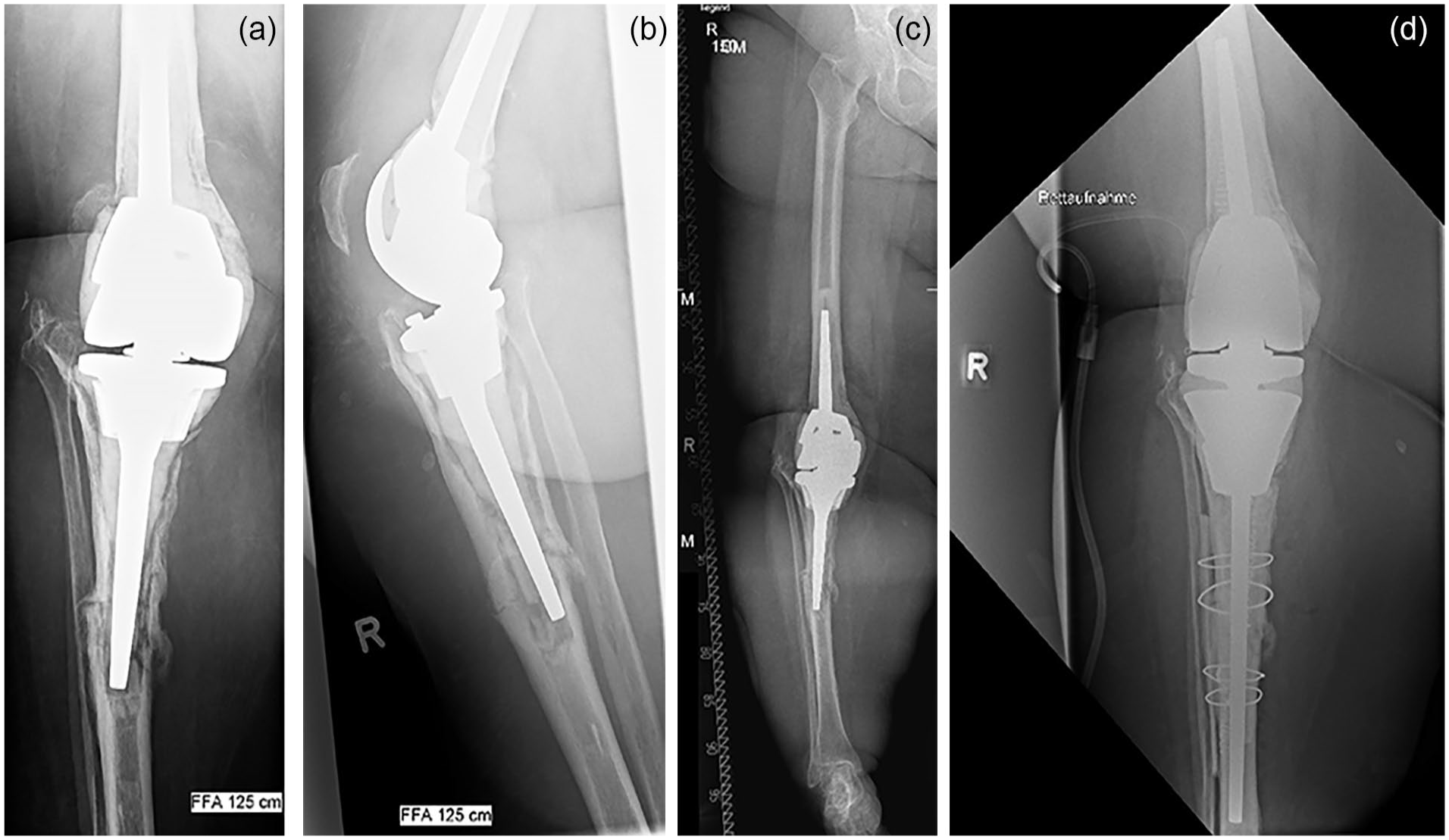
Failed hinge total knee arthroplasty with severe tibial bone loss, aseptic loosening, and periprosthetic fracture, addressed by impaction grafting, a longer cemented stem, cortical strut grafting, and tibial cone fixation: (a, b, c) preoperative images and (d) postoperative image.
Question 5. How Do You Deal With Extra-Articular Deformity, Retained Hardware, a Nonpatent Intramedullary Canal, or Adjacent Total Hip Replacement When Performing a Complex Modular Replacement?
Several unique scenarios exist that warrant special considerations when performing a complex modular replacement of the knee. The authors provide a consensus opinion on how to approach these unique scenarios.
Extra-articular deformity
The location, direction, and magnitude of an extra-articular deformity affects surgical planning [183,214]. The basic considerations regarding their management in primary arthroplasty can be extrapolated to the revision scenario. Multiplanar radiographs and/or computed tomography (CT) scan of the affected bone are often required to determine the precise extent of the deformity, which is often multiplanar. As a rule, the closer the deformity is to the knee joint, the greater the compensatory bone resection will be needed for an intra-articular correction [214]. Conversely, a mild deformity located far from the knee joint can often be addressed with compensatory bone resections. Severe deformity may need a staged correction before revision arthroplasty is performed. The authors strongly recommend against addressing severe deformity with a large resection to remove the deformity, and reconstruction with a segmental replacement. Every attempt should be made to correct the deformity and preserve bone and ligament attachments in the knee.
While performing revision TKA in a patient with extra-articular deformity, computer-assisted navigation or robotics can aid the surgeon in achieving adequate mechanical alignment, while preserving bone and achieving a stable reconstruction without the need for segmental replacement. If canals are not patent, appropriate measures should be taken (see the subsequent section on this topic).
Customization of implants is sometimes needed to accommodate for extra-articular deformity. Patient-specific implants, with stems of different shapes and sizes, can be manufactured to accommodate restrictions of host bone. Intraoperative customization of implants using metal-cutting burrs to modify off-the-shelf implants can be considered on a case-by-case basis.
Retained hardware and nonpatent medullary canals
The consensus approach to hardware present at the time of revision TKA involves removal of hardware that may interfere with component placement and fixation and retention of hardware that does not impact the reconstruction. In some cases, limited hardware removal is sufficient (Fig. 15). It is our preference to accomplish removal of hardware and reconstruction during a 1-stage procedure. However, if the hardware removal will be extensive or if concerns exist regarding multiple incisions and/or soft tissue coverage, a 2-stage procedure should be strongly considered. In cases in which infection is suspected, all hardware should be removed, if possible, and a 2-stage procedure should be performed. Specialized equipment should be available for hardware removal, including metal-cutting tools, screwdrivers, and broken screw removal sets, among others.
The medullary canal can be obstructed by bone or have altered geometry after fracture healing, osteotomy, or another lesion. Advanced preoperative imaging (CT) should be obtained, or a templating software using plain radiographs utilized, to characterize the dimensions of the bone and canal. Standing long-leg radiographs help evaluate limb alignment. These modalities will aid the surgeon to determine which implants should be used, identify and instrument the canal intraoperatively, fill any bony defects, and achieve appropriate fixation. Intraoperative fluoroscopy may be used to visualize appropriate re-establishment of the canal in an appropriate position. Specialized equipment including burrs, guide wires, and flexible reamers should be considered. Given the presence of altered and/or sclerotic bone in nonpatent canals, the surgeon should select components that optimize fixation within and outside of the zone that was not patent.
Adjacent total hip arthroplasty
When revision TKA is performed in patients with an ipsilateral primary or revision hip arthroplasty, the distance between the stems must be considered. Previously, based on finite-element modeling, 110 mm was reported as the minimal distance between stems to reduce the risk of interprosthetic fracture [192]. Given that interprosthetic fractures can be catastrophic, necessitating use of a total femur replacement, the surgeon should consider the distance and bone quality carefully and proceed with an approach that protects the bone. The authors recommend use of the shortest possible stem for the revision TKA and consideration of concomitant enhanced fixation with a sleeve or cone. If this is impostsible, the short gap between the 2 constructs may be reinforced with a plate, strut allograft, or both. As a last resort, consideration can be given to the use of a custom coupling device between the 2 stems [78] or conversion to an intramedullary or conventional total femur replacement [91]. In a multiply revised complex reconstruction, the benefits and risks of amputation or fusion should be considered on a case-by-case basis.
Supplemental Material
sj-docx-1-hss-10.1177_15563316231202750 – Supplemental material for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium
Supplemental material, sj-docx-1-hss-10.1177_15563316231202750 for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium by Peter Keyes Sculco, Dimitrios A. Flevas, Seth A. Jerabek, William A. Jiranek, Mathias P. Bostrom, Fares S. Haddad, Thomas K. Fehring, Alejandro Gonzalez Della Valle, Daniel J. Berry, Marco Brenneis, Troy D. Bornes, Carolena E. Rojas Marcos, Timothy M. Wright and Thomas P. Sculco in HSS Journal®
Supplemental Material
sj-docx-10-hss-10.1177_15563316231202750 – Supplemental material for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium
Supplemental material, sj-docx-10-hss-10.1177_15563316231202750 for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium by Peter Keyes Sculco, Dimitrios A. Flevas, Seth A. Jerabek, William A. Jiranek, Mathias P. Bostrom, Fares S. Haddad, Thomas K. Fehring, Alejandro Gonzalez Della Valle, Daniel J. Berry, Marco Brenneis, Troy D. Bornes, Carolena E. Rojas Marcos, Timothy M. Wright and Thomas P. Sculco in HSS Journal®
Supplemental Material
sj-docx-11-hss-10.1177_15563316231202750 – Supplemental material for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium
Supplemental material, sj-docx-11-hss-10.1177_15563316231202750 for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium by Peter Keyes Sculco, Dimitrios A. Flevas, Seth A. Jerabek, William A. Jiranek, Mathias P. Bostrom, Fares S. Haddad, Thomas K. Fehring, Alejandro Gonzalez Della Valle, Daniel J. Berry, Marco Brenneis, Troy D. Bornes, Carolena E. Rojas Marcos, Timothy M. Wright and Thomas P. Sculco in HSS Journal®
Supplemental Material
sj-docx-12-hss-10.1177_15563316231202750 – Supplemental material for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium
Supplemental material, sj-docx-12-hss-10.1177_15563316231202750 for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium by Peter Keyes Sculco, Dimitrios A. Flevas, Seth A. Jerabek, William A. Jiranek, Mathias P. Bostrom, Fares S. Haddad, Thomas K. Fehring, Alejandro Gonzalez Della Valle, Daniel J. Berry, Marco Brenneis, Troy D. Bornes, Carolena E. Rojas Marcos, Timothy M. Wright and Thomas P. Sculco in HSS Journal®
Supplemental Material
sj-docx-13-hss-10.1177_15563316231202750 – Supplemental material for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium
Supplemental material, sj-docx-13-hss-10.1177_15563316231202750 for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium by Peter Keyes Sculco, Dimitrios A. Flevas, Seth A. Jerabek, William A. Jiranek, Mathias P. Bostrom, Fares S. Haddad, Thomas K. Fehring, Alejandro Gonzalez Della Valle, Daniel J. Berry, Marco Brenneis, Troy D. Bornes, Carolena E. Rojas Marcos, Timothy M. Wright and Thomas P. Sculco in HSS Journal®
Supplemental Material
sj-docx-14-hss-10.1177_15563316231202750 – Supplemental material for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium
Supplemental material, sj-docx-14-hss-10.1177_15563316231202750 for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium by Peter Keyes Sculco, Dimitrios A. Flevas, Seth A. Jerabek, William A. Jiranek, Mathias P. Bostrom, Fares S. Haddad, Thomas K. Fehring, Alejandro Gonzalez Della Valle, Daniel J. Berry, Marco Brenneis, Troy D. Bornes, Carolena E. Rojas Marcos, Timothy M. Wright and Thomas P. Sculco in HSS Journal®
Supplemental Material
sj-docx-15-hss-10.1177_15563316231202750 – Supplemental material for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium
Supplemental material, sj-docx-15-hss-10.1177_15563316231202750 for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium by Peter Keyes Sculco, Dimitrios A. Flevas, Seth A. Jerabek, William A. Jiranek, Mathias P. Bostrom, Fares S. Haddad, Thomas K. Fehring, Alejandro Gonzalez Della Valle, Daniel J. Berry, Marco Brenneis, Troy D. Bornes, Carolena E. Rojas Marcos, Timothy M. Wright and Thomas P. Sculco in HSS Journal®
Supplemental Material
sj-docx-16-hss-10.1177_15563316231202750 – Supplemental material for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium
Supplemental material, sj-docx-16-hss-10.1177_15563316231202750 for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium by Peter Keyes Sculco, Dimitrios A. Flevas, Seth A. Jerabek, William A. Jiranek, Mathias P. Bostrom, Fares S. Haddad, Thomas K. Fehring, Alejandro Gonzalez Della Valle, Daniel J. Berry, Marco Brenneis, Troy D. Bornes, Carolena E. Rojas Marcos, Timothy M. Wright and Thomas P. Sculco in HSS Journal®
Supplemental Material
sj-docx-17-hss-10.1177_15563316231202750 – Supplemental material for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium
Supplemental material, sj-docx-17-hss-10.1177_15563316231202750 for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium by Peter Keyes Sculco, Dimitrios A. Flevas, Seth A. Jerabek, William A. Jiranek, Mathias P. Bostrom, Fares S. Haddad, Thomas K. Fehring, Alejandro Gonzalez Della Valle, Daniel J. Berry, Marco Brenneis, Troy D. Bornes, Carolena E. Rojas Marcos, Timothy M. Wright and Thomas P. Sculco in HSS Journal®
Supplemental Material
sj-docx-18-hss-10.1177_15563316231202750 – Supplemental material for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium
Supplemental material, sj-docx-18-hss-10.1177_15563316231202750 for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium by Peter Keyes Sculco, Dimitrios A. Flevas, Seth A. Jerabek, William A. Jiranek, Mathias P. Bostrom, Fares S. Haddad, Thomas K. Fehring, Alejandro Gonzalez Della Valle, Daniel J. Berry, Marco Brenneis, Troy D. Bornes, Carolena E. Rojas Marcos, Timothy M. Wright and Thomas P. Sculco in HSS Journal®
Supplemental Material
sj-docx-19-hss-10.1177_15563316231202750 – Supplemental material for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium
Supplemental material, sj-docx-19-hss-10.1177_15563316231202750 for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium by Peter Keyes Sculco, Dimitrios A. Flevas, Seth A. Jerabek, William A. Jiranek, Mathias P. Bostrom, Fares S. Haddad, Thomas K. Fehring, Alejandro Gonzalez Della Valle, Daniel J. Berry, Marco Brenneis, Troy D. Bornes, Carolena E. Rojas Marcos, Timothy M. Wright and Thomas P. Sculco in HSS Journal®
Supplemental Material
sj-docx-2-hss-10.1177_15563316231202750 – Supplemental material for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium
Supplemental material, sj-docx-2-hss-10.1177_15563316231202750 for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium by Peter Keyes Sculco, Dimitrios A. Flevas, Seth A. Jerabek, William A. Jiranek, Mathias P. Bostrom, Fares S. Haddad, Thomas K. Fehring, Alejandro Gonzalez Della Valle, Daniel J. Berry, Marco Brenneis, Troy D. Bornes, Carolena E. Rojas Marcos, Timothy M. Wright and Thomas P. Sculco in HSS Journal®
Supplemental Material
sj-docx-20-hss-10.1177_15563316231202750 – Supplemental material for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium
Supplemental material, sj-docx-20-hss-10.1177_15563316231202750 for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium by Peter Keyes Sculco, Dimitrios A. Flevas, Seth A. Jerabek, William A. Jiranek, Mathias P. Bostrom, Fares S. Haddad, Thomas K. Fehring, Alejandro Gonzalez Della Valle, Daniel J. Berry, Marco Brenneis, Troy D. Bornes, Carolena E. Rojas Marcos, Timothy M. Wright and Thomas P. Sculco in HSS Journal®
Supplemental Material
sj-docx-21-hss-10.1177_15563316231202750 – Supplemental material for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium
Supplemental material, sj-docx-21-hss-10.1177_15563316231202750 for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium by Peter Keyes Sculco, Dimitrios A. Flevas, Seth A. Jerabek, William A. Jiranek, Mathias P. Bostrom, Fares S. Haddad, Thomas K. Fehring, Alejandro Gonzalez Della Valle, Daniel J. Berry, Marco Brenneis, Troy D. Bornes, Carolena E. Rojas Marcos, Timothy M. Wright and Thomas P. Sculco in HSS Journal®
Supplemental Material
sj-docx-22-hss-10.1177_15563316231202750 – Supplemental material for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium
Supplemental material, sj-docx-22-hss-10.1177_15563316231202750 for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium by Peter Keyes Sculco, Dimitrios A. Flevas, Seth A. Jerabek, William A. Jiranek, Mathias P. Bostrom, Fares S. Haddad, Thomas K. Fehring, Alejandro Gonzalez Della Valle, Daniel J. Berry, Marco Brenneis, Troy D. Bornes, Carolena E. Rojas Marcos, Timothy M. Wright and Thomas P. Sculco in HSS Journal®
Supplemental Material
sj-docx-23-hss-10.1177_15563316231202750 – Supplemental material for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium
Supplemental material, sj-docx-23-hss-10.1177_15563316231202750 for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium by Peter Keyes Sculco, Dimitrios A. Flevas, Seth A. Jerabek, William A. Jiranek, Mathias P. Bostrom, Fares S. Haddad, Thomas K. Fehring, Alejandro Gonzalez Della Valle, Daniel J. Berry, Marco Brenneis, Troy D. Bornes, Carolena E. Rojas Marcos, Timothy M. Wright and Thomas P. Sculco in HSS Journal®
Supplemental Material
sj-docx-24-hss-10.1177_15563316231202750 – Supplemental material for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium
Supplemental material, sj-docx-24-hss-10.1177_15563316231202750 for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium by Peter Keyes Sculco, Dimitrios A. Flevas, Seth A. Jerabek, William A. Jiranek, Mathias P. Bostrom, Fares S. Haddad, Thomas K. Fehring, Alejandro Gonzalez Della Valle, Daniel J. Berry, Marco Brenneis, Troy D. Bornes, Carolena E. Rojas Marcos, Timothy M. Wright and Thomas P. Sculco in HSS Journal®
Supplemental Material
sj-docx-25-hss-10.1177_15563316231202750 – Supplemental material for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium
Supplemental material, sj-docx-25-hss-10.1177_15563316231202750 for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium by Peter Keyes Sculco, Dimitrios A. Flevas, Seth A. Jerabek, William A. Jiranek, Mathias P. Bostrom, Fares S. Haddad, Thomas K. Fehring, Alejandro Gonzalez Della Valle, Daniel J. Berry, Marco Brenneis, Troy D. Bornes, Carolena E. Rojas Marcos, Timothy M. Wright and Thomas P. Sculco in HSS Journal®
Supplemental Material
sj-docx-26-hss-10.1177_15563316231202750 – Supplemental material for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium
Supplemental material, sj-docx-26-hss-10.1177_15563316231202750 for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium by Peter Keyes Sculco, Dimitrios A. Flevas, Seth A. Jerabek, William A. Jiranek, Mathias P. Bostrom, Fares S. Haddad, Thomas K. Fehring, Alejandro Gonzalez Della Valle, Daniel J. Berry, Marco Brenneis, Troy D. Bornes, Carolena E. Rojas Marcos, Timothy M. Wright and Thomas P. Sculco in HSS Journal®
Supplemental Material
sj-docx-27-hss-10.1177_15563316231202750 – Supplemental material for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium
Supplemental material, sj-docx-27-hss-10.1177_15563316231202750 for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium by Peter Keyes Sculco, Dimitrios A. Flevas, Seth A. Jerabek, William A. Jiranek, Mathias P. Bostrom, Fares S. Haddad, Thomas K. Fehring, Alejandro Gonzalez Della Valle, Daniel J. Berry, Marco Brenneis, Troy D. Bornes, Carolena E. Rojas Marcos, Timothy M. Wright and Thomas P. Sculco in HSS Journal®
Supplemental Material
sj-docx-28-hss-10.1177_15563316231202750 – Supplemental material for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium
Supplemental material, sj-docx-28-hss-10.1177_15563316231202750 for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium by Peter Keyes Sculco, Dimitrios A. Flevas, Seth A. Jerabek, William A. Jiranek, Mathias P. Bostrom, Fares S. Haddad, Thomas K. Fehring, Alejandro Gonzalez Della Valle, Daniel J. Berry, Marco Brenneis, Troy D. Bornes, Carolena E. Rojas Marcos, Timothy M. Wright and Thomas P. Sculco in HSS Journal®
Supplemental Material
sj-docx-29-hss-10.1177_15563316231202750 – Supplemental material for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium
Supplemental material, sj-docx-29-hss-10.1177_15563316231202750 for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium by Peter Keyes Sculco, Dimitrios A. Flevas, Seth A. Jerabek, William A. Jiranek, Mathias P. Bostrom, Fares S. Haddad, Thomas K. Fehring, Alejandro Gonzalez Della Valle, Daniel J. Berry, Marco Brenneis, Troy D. Bornes, Carolena E. Rojas Marcos, Timothy M. Wright and Thomas P. Sculco in HSS Journal®
Supplemental Material
sj-docx-3-hss-10.1177_15563316231202750 – Supplemental material for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium
Supplemental material, sj-docx-3-hss-10.1177_15563316231202750 for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium by Peter Keyes Sculco, Dimitrios A. Flevas, Seth A. Jerabek, William A. Jiranek, Mathias P. Bostrom, Fares S. Haddad, Thomas K. Fehring, Alejandro Gonzalez Della Valle, Daniel J. Berry, Marco Brenneis, Troy D. Bornes, Carolena E. Rojas Marcos, Timothy M. Wright and Thomas P. Sculco in HSS Journal®
Supplemental Material
sj-docx-30-hss-10.1177_15563316231202750 – Supplemental material for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium
Supplemental material, sj-docx-30-hss-10.1177_15563316231202750 for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium by Peter Keyes Sculco, Dimitrios A. Flevas, Seth A. Jerabek, William A. Jiranek, Mathias P. Bostrom, Fares S. Haddad, Thomas K. Fehring, Alejandro Gonzalez Della Valle, Daniel J. Berry, Marco Brenneis, Troy D. Bornes, Carolena E. Rojas Marcos, Timothy M. Wright and Thomas P. Sculco in HSS Journal®
Supplemental Material
sj-docx-31-hss-10.1177_15563316231202750 – Supplemental material for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium
Supplemental material, sj-docx-31-hss-10.1177_15563316231202750 for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium by Peter Keyes Sculco, Dimitrios A. Flevas, Seth A. Jerabek, William A. Jiranek, Mathias P. Bostrom, Fares S. Haddad, Thomas K. Fehring, Alejandro Gonzalez Della Valle, Daniel J. Berry, Marco Brenneis, Troy D. Bornes, Carolena E. Rojas Marcos, Timothy M. Wright and Thomas P. Sculco in HSS Journal®
Supplemental Material
sj-docx-32-hss-10.1177_15563316231202750 – Supplemental material for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium
Supplemental material, sj-docx-32-hss-10.1177_15563316231202750 for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium by Peter Keyes Sculco, Dimitrios A. Flevas, Seth A. Jerabek, William A. Jiranek, Mathias P. Bostrom, Fares S. Haddad, Thomas K. Fehring, Alejandro Gonzalez Della Valle, Daniel J. Berry, Marco Brenneis, Troy D. Bornes, Carolena E. Rojas Marcos, Timothy M. Wright and Thomas P. Sculco in HSS Journal®
Supplemental Material
sj-docx-33-hss-10.1177_15563316231202750 – Supplemental material for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium
Supplemental material, sj-docx-33-hss-10.1177_15563316231202750 for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium by Peter Keyes Sculco, Dimitrios A. Flevas, Seth A. Jerabek, William A. Jiranek, Mathias P. Bostrom, Fares S. Haddad, Thomas K. Fehring, Alejandro Gonzalez Della Valle, Daniel J. Berry, Marco Brenneis, Troy D. Bornes, Carolena E. Rojas Marcos, Timothy M. Wright and Thomas P. Sculco in HSS Journal®
Supplemental Material
sj-docx-34-hss-10.1177_15563316231202750 – Supplemental material for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium
Supplemental material, sj-docx-34-hss-10.1177_15563316231202750 for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium by Peter Keyes Sculco, Dimitrios A. Flevas, Seth A. Jerabek, William A. Jiranek, Mathias P. Bostrom, Fares S. Haddad, Thomas K. Fehring, Alejandro Gonzalez Della Valle, Daniel J. Berry, Marco Brenneis, Troy D. Bornes, Carolena E. Rojas Marcos, Timothy M. Wright and Thomas P. Sculco in HSS Journal®
Supplemental Material
sj-docx-35-hss-10.1177_15563316231202750 – Supplemental material for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium
Supplemental material, sj-docx-35-hss-10.1177_15563316231202750 for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium by Peter Keyes Sculco, Dimitrios A. Flevas, Seth A. Jerabek, William A. Jiranek, Mathias P. Bostrom, Fares S. Haddad, Thomas K. Fehring, Alejandro Gonzalez Della Valle, Daniel J. Berry, Marco Brenneis, Troy D. Bornes, Carolena E. Rojas Marcos, Timothy M. Wright and Thomas P. Sculco in HSS Journal®
Supplemental Material
sj-docx-36-hss-10.1177_15563316231202750 – Supplemental material for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium
Supplemental material, sj-docx-36-hss-10.1177_15563316231202750 for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium by Peter Keyes Sculco, Dimitrios A. Flevas, Seth A. Jerabek, William A. Jiranek, Mathias P. Bostrom, Fares S. Haddad, Thomas K. Fehring, Alejandro Gonzalez Della Valle, Daniel J. Berry, Marco Brenneis, Troy D. Bornes, Carolena E. Rojas Marcos, Timothy M. Wright and Thomas P. Sculco in HSS Journal®
Supplemental Material
sj-docx-37-hss-10.1177_15563316231202750 – Supplemental material for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium
Supplemental material, sj-docx-37-hss-10.1177_15563316231202750 for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium by Peter Keyes Sculco, Dimitrios A. Flevas, Seth A. Jerabek, William A. Jiranek, Mathias P. Bostrom, Fares S. Haddad, Thomas K. Fehring, Alejandro Gonzalez Della Valle, Daniel J. Berry, Marco Brenneis, Troy D. Bornes, Carolena E. Rojas Marcos, Timothy M. Wright and Thomas P. Sculco in HSS Journal®
Supplemental Material
sj-docx-38-hss-10.1177_15563316231202750 – Supplemental material for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium
Supplemental material, sj-docx-38-hss-10.1177_15563316231202750 for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium by Peter Keyes Sculco, Dimitrios A. Flevas, Seth A. Jerabek, William A. Jiranek, Mathias P. Bostrom, Fares S. Haddad, Thomas K. Fehring, Alejandro Gonzalez Della Valle, Daniel J. Berry, Marco Brenneis, Troy D. Bornes, Carolena E. Rojas Marcos, Timothy M. Wright and Thomas P. Sculco in HSS Journal®
Supplemental Material
sj-docx-39-hss-10.1177_15563316231202750 – Supplemental material for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium
Supplemental material, sj-docx-39-hss-10.1177_15563316231202750 for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium by Peter Keyes Sculco, Dimitrios A. Flevas, Seth A. Jerabek, William A. Jiranek, Mathias P. Bostrom, Fares S. Haddad, Thomas K. Fehring, Alejandro Gonzalez Della Valle, Daniel J. Berry, Marco Brenneis, Troy D. Bornes, Carolena E. Rojas Marcos, Timothy M. Wright and Thomas P. Sculco in HSS Journal®
Supplemental Material
sj-docx-4-hss-10.1177_15563316231202750 – Supplemental material for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium
Supplemental material, sj-docx-4-hss-10.1177_15563316231202750 for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium by Peter Keyes Sculco, Dimitrios A. Flevas, Seth A. Jerabek, William A. Jiranek, Mathias P. Bostrom, Fares S. Haddad, Thomas K. Fehring, Alejandro Gonzalez Della Valle, Daniel J. Berry, Marco Brenneis, Troy D. Bornes, Carolena E. Rojas Marcos, Timothy M. Wright and Thomas P. Sculco in HSS Journal®
Supplemental Material
sj-docx-40-hss-10.1177_15563316231202750 – Supplemental material for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium
Supplemental material, sj-docx-40-hss-10.1177_15563316231202750 for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium by Peter Keyes Sculco, Dimitrios A. Flevas, Seth A. Jerabek, William A. Jiranek, Mathias P. Bostrom, Fares S. Haddad, Thomas K. Fehring, Alejandro Gonzalez Della Valle, Daniel J. Berry, Marco Brenneis, Troy D. Bornes, Carolena E. Rojas Marcos, Timothy M. Wright and Thomas P. Sculco in HSS Journal®
Supplemental Material
sj-docx-5-hss-10.1177_15563316231202750 – Supplemental material for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium
Supplemental material, sj-docx-5-hss-10.1177_15563316231202750 for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium by Peter Keyes Sculco, Dimitrios A. Flevas, Seth A. Jerabek, William A. Jiranek, Mathias P. Bostrom, Fares S. Haddad, Thomas K. Fehring, Alejandro Gonzalez Della Valle, Daniel J. Berry, Marco Brenneis, Troy D. Bornes, Carolena E. Rojas Marcos, Timothy M. Wright and Thomas P. Sculco in HSS Journal®
Supplemental Material
sj-docx-6-hss-10.1177_15563316231202750 – Supplemental material for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium
Supplemental material, sj-docx-6-hss-10.1177_15563316231202750 for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium by Peter Keyes Sculco, Dimitrios A. Flevas, Seth A. Jerabek, William A. Jiranek, Mathias P. Bostrom, Fares S. Haddad, Thomas K. Fehring, Alejandro Gonzalez Della Valle, Daniel J. Berry, Marco Brenneis, Troy D. Bornes, Carolena E. Rojas Marcos, Timothy M. Wright and Thomas P. Sculco in HSS Journal®
Supplemental Material
sj-docx-7-hss-10.1177_15563316231202750 – Supplemental material for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium
Supplemental material, sj-docx-7-hss-10.1177_15563316231202750 for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium by Peter Keyes Sculco, Dimitrios A. Flevas, Seth A. Jerabek, William A. Jiranek, Mathias P. Bostrom, Fares S. Haddad, Thomas K. Fehring, Alejandro Gonzalez Della Valle, Daniel J. Berry, Marco Brenneis, Troy D. Bornes, Carolena E. Rojas Marcos, Timothy M. Wright and Thomas P. Sculco in HSS Journal®
Supplemental Material
sj-docx-8-hss-10.1177_15563316231202750 – Supplemental material for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium
Supplemental material, sj-docx-8-hss-10.1177_15563316231202750 for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium by Peter Keyes Sculco, Dimitrios A. Flevas, Seth A. Jerabek, William A. Jiranek, Mathias P. Bostrom, Fares S. Haddad, Thomas K. Fehring, Alejandro Gonzalez Della Valle, Daniel J. Berry, Marco Brenneis, Troy D. Bornes, Carolena E. Rojas Marcos, Timothy M. Wright and Thomas P. Sculco in HSS Journal®
Supplemental Material
sj-docx-9-hss-10.1177_15563316231202750 – Supplemental material for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium
Supplemental material, sj-docx-9-hss-10.1177_15563316231202750 for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium by Peter Keyes Sculco, Dimitrios A. Flevas, Seth A. Jerabek, William A. Jiranek, Mathias P. Bostrom, Fares S. Haddad, Thomas K. Fehring, Alejandro Gonzalez Della Valle, Daniel J. Berry, Marco Brenneis, Troy D. Bornes, Carolena E. Rojas Marcos, Timothy M. Wright and Thomas P. Sculco in HSS Journal®
Supplemental Material
sj-pdf-41-hss-10.1177_15563316231202750 – Supplemental material for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium
Supplemental material, sj-pdf-41-hss-10.1177_15563316231202750 for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium by Peter Keyes Sculco, Dimitrios A. Flevas, Seth A. Jerabek, William A. Jiranek, Mathias P. Bostrom, Fares S. Haddad, Thomas K. Fehring, Alejandro Gonzalez Della Valle, Daniel J. Berry, Marco Brenneis, Troy D. Bornes, Carolena E. Rojas Marcos, Timothy M. Wright and Thomas P. Sculco in HSS Journal®
Supplemental Material
sj-pdf-42-hss-10.1177_15563316231202750 – Supplemental material for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium
Supplemental material, sj-pdf-42-hss-10.1177_15563316231202750 for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium by Peter Keyes Sculco, Dimitrios A. Flevas, Seth A. Jerabek, William A. Jiranek, Mathias P. Bostrom, Fares S. Haddad, Thomas K. Fehring, Alejandro Gonzalez Della Valle, Daniel J. Berry, Marco Brenneis, Troy D. Bornes, Carolena E. Rojas Marcos, Timothy M. Wright and Thomas P. Sculco in HSS Journal®
Supplemental Material
sj-pdf-43-hss-10.1177_15563316231202750 – Supplemental material for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium
Supplemental material, sj-pdf-43-hss-10.1177_15563316231202750 for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium by Peter Keyes Sculco, Dimitrios A. Flevas, Seth A. Jerabek, William A. Jiranek, Mathias P. Bostrom, Fares S. Haddad, Thomas K. Fehring, Alejandro Gonzalez Della Valle, Daniel J. Berry, Marco Brenneis, Troy D. Bornes, Carolena E. Rojas Marcos, Timothy M. Wright and Thomas P. Sculco in HSS Journal®
Supplemental Material
sj-pdf-44-hss-10.1177_15563316231202750 – Supplemental material for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium
Supplemental material, sj-pdf-44-hss-10.1177_15563316231202750 for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium by Peter Keyes Sculco, Dimitrios A. Flevas, Seth A. Jerabek, William A. Jiranek, Mathias P. Bostrom, Fares S. Haddad, Thomas K. Fehring, Alejandro Gonzalez Della Valle, Daniel J. Berry, Marco Brenneis, Troy D. Bornes, Carolena E. Rojas Marcos, Timothy M. Wright and Thomas P. Sculco in HSS Journal®
Supplemental Material
sj-pdf-45-hss-10.1177_15563316231202750 – Supplemental material for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium
Supplemental material, sj-pdf-45-hss-10.1177_15563316231202750 for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium by Peter Keyes Sculco, Dimitrios A. Flevas, Seth A. Jerabek, William A. Jiranek, Mathias P. Bostrom, Fares S. Haddad, Thomas K. Fehring, Alejandro Gonzalez Della Valle, Daniel J. Berry, Marco Brenneis, Troy D. Bornes, Carolena E. Rojas Marcos, Timothy M. Wright and Thomas P. Sculco in HSS Journal®
Supplemental Material
sj-pdf-46-hss-10.1177_15563316231202750 – Supplemental material for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium
Supplemental material, sj-pdf-46-hss-10.1177_15563316231202750 for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium by Peter Keyes Sculco, Dimitrios A. Flevas, Seth A. Jerabek, William A. Jiranek, Mathias P. Bostrom, Fares S. Haddad, Thomas K. Fehring, Alejandro Gonzalez Della Valle, Daniel J. Berry, Marco Brenneis, Troy D. Bornes, Carolena E. Rojas Marcos, Timothy M. Wright and Thomas P. Sculco in HSS Journal®
Supplemental Material
sj-pdf-47-hss-10.1177_15563316231202750 – Supplemental material for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium
Supplemental material, sj-pdf-47-hss-10.1177_15563316231202750 for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium by Peter Keyes Sculco, Dimitrios A. Flevas, Seth A. Jerabek, William A. Jiranek, Mathias P. Bostrom, Fares S. Haddad, Thomas K. Fehring, Alejandro Gonzalez Della Valle, Daniel J. Berry, Marco Brenneis, Troy D. Bornes, Carolena E. Rojas Marcos, Timothy M. Wright and Thomas P. Sculco in HSS Journal®
Supplemental Material
sj-pdf-48-hss-10.1177_15563316231202750 – Supplemental material for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium
Supplemental material, sj-pdf-48-hss-10.1177_15563316231202750 for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium by Peter Keyes Sculco, Dimitrios A. Flevas, Seth A. Jerabek, William A. Jiranek, Mathias P. Bostrom, Fares S. Haddad, Thomas K. Fehring, Alejandro Gonzalez Della Valle, Daniel J. Berry, Marco Brenneis, Troy D. Bornes, Carolena E. Rojas Marcos, Timothy M. Wright and Thomas P. Sculco in HSS Journal®
Supplemental Material
sj-pdf-49-hss-10.1177_15563316231202750 – Supplemental material for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium
Supplemental material, sj-pdf-49-hss-10.1177_15563316231202750 for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium by Peter Keyes Sculco, Dimitrios A. Flevas, Seth A. Jerabek, William A. Jiranek, Mathias P. Bostrom, Fares S. Haddad, Thomas K. Fehring, Alejandro Gonzalez Della Valle, Daniel J. Berry, Marco Brenneis, Troy D. Bornes, Carolena E. Rojas Marcos, Timothy M. Wright and Thomas P. Sculco in HSS Journal®
Supplemental Material
sj-pdf-50-hss-10.1177_15563316231202750 – Supplemental material for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium
Supplemental material, sj-pdf-50-hss-10.1177_15563316231202750 for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium by Peter Keyes Sculco, Dimitrios A. Flevas, Seth A. Jerabek, William A. Jiranek, Mathias P. Bostrom, Fares S. Haddad, Thomas K. Fehring, Alejandro Gonzalez Della Valle, Daniel J. Berry, Marco Brenneis, Troy D. Bornes, Carolena E. Rojas Marcos, Timothy M. Wright and Thomas P. Sculco in HSS Journal®
Supplemental Material
sj-pdf-51-hss-10.1177_15563316231202750 – Supplemental material for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium
Supplemental material, sj-pdf-51-hss-10.1177_15563316231202750 for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium by Peter Keyes Sculco, Dimitrios A. Flevas, Seth A. Jerabek, William A. Jiranek, Mathias P. Bostrom, Fares S. Haddad, Thomas K. Fehring, Alejandro Gonzalez Della Valle, Daniel J. Berry, Marco Brenneis, Troy D. Bornes, Carolena E. Rojas Marcos, Timothy M. Wright and Thomas P. Sculco in HSS Journal®
Supplemental Material
sj-pdf-52-hss-10.1177_15563316231202750 – Supplemental material for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium
Supplemental material, sj-pdf-52-hss-10.1177_15563316231202750 for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium by Peter Keyes Sculco, Dimitrios A. Flevas, Seth A. Jerabek, William A. Jiranek, Mathias P. Bostrom, Fares S. Haddad, Thomas K. Fehring, Alejandro Gonzalez Della Valle, Daniel J. Berry, Marco Brenneis, Troy D. Bornes, Carolena E. Rojas Marcos, Timothy M. Wright and Thomas P. Sculco in HSS Journal®
Supplemental Material
sj-pdf-53-hss-10.1177_15563316231202750 – Supplemental material for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium
Supplemental material, sj-pdf-53-hss-10.1177_15563316231202750 for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium by Peter Keyes Sculco, Dimitrios A. Flevas, Seth A. Jerabek, William A. Jiranek, Mathias P. Bostrom, Fares S. Haddad, Thomas K. Fehring, Alejandro Gonzalez Della Valle, Daniel J. Berry, Marco Brenneis, Troy D. Bornes, Carolena E. Rojas Marcos, Timothy M. Wright and Thomas P. Sculco in HSS Journal®
Supplemental Material
sj-pdf-54-hss-10.1177_15563316231202750 – Supplemental material for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium
Supplemental material, sj-pdf-54-hss-10.1177_15563316231202750 for Management of Bone Loss in Revision Total Knee Arthroplasty: An International Consensus Symposium by Peter Keyes Sculco, Dimitrios A. Flevas, Seth A. Jerabek, William A. Jiranek, Mathias P. Bostrom, Fares S. Haddad, Thomas K. Fehring, Alejandro Gonzalez Della Valle, Daniel J. Berry, Marco Brenneis, Troy D. Bornes, Carolena E. Rojas Marcos, Timothy M. Wright and Thomas P. Sculco in HSS Journal®
Footnotes
Acknowledgements
The authors thank Donald Garbuz, MD, for his contributions to the consensus statement.
Authors’ Note
The Management of Bone Loss in Revision TKR Work Group consists of:
Matthew S. Austin, MD1, Andrea Baldini, MD, PhD2, Fabio Catani, MD3, Antonia F. Chen, MD4,5, Martin Pietsch, MD6, Bryan D Springer, MD7,8, Jonathan M. Vigdorchik, MD9, Geoffrey H. Westrich, MD9, Friedrich Boettner, MD9, Fernando J. Quevedo González, PhD9, Erik Hansen, MD10, Gijs Van Hellemondt, MD11, Paul F. Lachiewicz, MD12, Arun Mullaji, MD13, Neil P. Sheth, MD14, Mark Taylor, PhD15, Matthew P. Abdel, MD16, Michael Bolognesi, MD12, Alberto V. Carli, MD9, Steven B. Haas, MD9, Gwo-Chin Lee, MD9, David G. Lewallen, MD16, Roberto Rossi, MD17, William Walter, MD18,19, Derek F. Amanatullah, MD20, Brian P. Chalmers, MD9, Kevin B. Fricka, MD21,22, Thorsten Gehrke, MD, PhD23, Carlos A. Higuera-Rueda, MD24, Brett R. Levine, MD25, Joseph D. Lipman, MS9, Giles R. Scuderi, MD26, Amar S. Ranawat, MD9, Ajay Premkumar, MD9, John Steele, MD9, Nana O. Sarpong, MD9, Michael Kheir, MD9, Elizabeth Davis, MD9, Ioannis Gkiatas, MD27,28, Cynthia A Kahlenberg, MD9
1Department of Orthopaedic Surgery, Thomas Jefferson University Hospital, Philadelphia, PA, USA
2Institute for Complex Arthroplasty and Revisions, Villa Ulivella Clinic, Florence, Italy
3Department of Orthopaedic Surgery, University Hospital Policlinico di Modena, University of Modena and Reggio Emilia, Modena, Italy
4Department of Orthopaedic Surgery, Brigham and Women’s Hospital, Boston, MA, USA
5Harvard Medical School, Boston, MA, USA
6Department of Orthopaedic Surgery, Orthopaedic Hospital Stolzalpe (LKH Murtal), Stolzalpe, Austria
7Hip & Knee Center, OrthoCarolina, Charlotte, NC, USA
8Musculoskeletal Institute, Atrium Health, Charlotte, NC, USA
9Hospital for Special Surgery, New York, NY, USA
10Department of Orthopaedic Surgery, University of California, San Francisco, San Francisco, CA, USA
11Sint Maartenskliniek, Nijmegen, The Netherlands
12Department of Orthopaedics, Duke University Medical Center, Durham, NC, USA
13Department of Orthopaedics, Breach Candy Hospital, Mumbai, India
14Department of Orthopaedic Surgery, Pennsylvania Hospital, Philadelphia, PA, USA
15Medical Device Research Institute, College of Science and Engineering, Flinders University, Adelaide, SA, Australia
16Department of Orthopedic Surgery, Mayo Clinic, Rochester, MN, USA
17Orthopaedics and Traumatology Department, AO Ordine Mauriziano, Turin, Italy
18The University of Sydney, Sydney, NSW, Australia
19Department of Orthopaedic and Trauma Surgery, Royal North Shore Hospital, St. Leonards, NSW, Australia
20Orthopaedic Surgery, Stanford University Medical Center, Stanford, CA, USA
21Anderson Orthopaedic Research Institute, Alexandria, VA, USA
22Joint Replacement Center, Inova Mount Vernon Hospital, Alexandria, VA, USA
23Department of Orthopaedic Surgery, ENDO-Klinik Hamburg, Hamburg, Germany
24Department of Orthopaedic Surgery, Cleveland Clinic Foundation, Weston, FL, USA
25Department of Orthopaedic Surgery, RUSH University Medical Center, Chicago, IL, USA
26Department of Orthopedic Surgery, Northwell Health Orthopaedic Institute, Garden City, NY, USA
27Department of Orthopaedic Surgery, University of Ioannina, Ioannina, Greece
28Stavros Niarchos Foundation Complex Joint Reconstruction Center, Hospital for Special Surgery, New York, NY, USA
Declaration of Conflicting Interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: PKS, MD, reports relationships with Atec, Depuy Synthesis, Lima Corporate, and Zimmer Biomet. SAJ, MD, reports relationships with Stryker, Imagen Technologies, and Wolters Kluwer Health-Lippincott Williams and Wilkins. WAJ, MD, reports relationships with Biomech, Depuy Orthopedics, The Hip Society, and Moximed. MPB, MD, reports relationships with AAOS, American Austrian Foundation, Hip Society, and Smith & Nephew. FSH, MBBS, MD, reports relationships with Corin, Bone & Joint Journal, Institute of Sport, Exercise and Health, MatOrtho Limited, Smith & Nephew, Stryker, and University College London Hospitals. TKF, MD, reports a relationship with Depuy Synthesis. AGDV, MD, reports relationships with Hip Society, Johnson & Johnson, Link, Naviswiss, and Wishbone. DJB, MD, reports relationships with AO Recon, Bodycad, Current Concepts in Joint Replacement, Depuy, International Hip Society and Wolters Kluwer Health-Lippincott Williams & Wilkins. TPS, MD, reports relationships with Exactech and OREF. The Management of Bone Loss in Revision TKR Work Group declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Matthew S. Austin, MD, declares relationships with Corin, Depuy Synthesis, Link, Zimmer Biomet, AAHKS, AAOS, Knee Society, and American College of Rheumatology. Andrea Baldini, MD, PhD, declares relationships with Convatec, Ethicon, Permedica, Zimmer Biomet, and European Knee Society. Fabio Catani, MD, declares a relationship with Stryker. Antonia F. Chen, MD, declares relationships with Adaptive Phage Therapeutics, BICMD, Convatec, Ethicon, GLG, Guidepoint, Hyalex, Heraeus, IrriMax, IlluminOss Osteal Therapeutics, Peptilogics, Stryker, SLACK, Smith & Nephew, Sonoran, UpToDate, AAOS, AJRR, AAHKS, and European Knee Association. Martin Pietsch, MD, declares a relationship with Zimmer Biomet. Bryan D. Springer, MD, declares relationships with Convatec, Osteoremedies, Stryker, AAHKS, and IOEN. Jonathan Vigdorchik, MD, declares a relationship with Corin, Depuy Synthesis, Intellijoint, and Ortho AI, and Stryker. Geoffrey Westrich, MD, reports relationships with Ethicon, Exactech, Hospital for Special Surgery, Stryker, and Eastern Orthopaedic Association. Friedrich Boettner, MD, reports relationships with OrthoDevelopment and Smith & Nephew. Fernando J Quevedo González, PhD, reports a relationship with Lima Corporate. Erik Hansen, MD, reports relationships with Corin and Medico. Gijs Van Hellemondt, MD, reports relationships with Zimmer Biomet, Smith & Nephew, Materialize, European Knee Society, AO Foundation, MO Journal/JOINTS Journal. Paul F. Lachiewicz, MD, reports relationships with Guidepoint Global Advisors, Gerson Lehrman Group, Innacoll, Heron Therapeutics, AO Foundation, Southern Orthopaedic Association, J Arthroplasty, and JSOA. Arun Mullaji, MD, reports relationships with Depuy, Springer, ISTA, and Indian Society for Hip and Knee Surgery. Neil P. Sheth, MD, declared relationships with Medacta, OrthoInfo, Zimmer Biomet AAOS Now, and Eastern Orthopaedic Association. Mark Taylor, PhD, declares relationships with 360 MedCare, DePuy Synthes, and Synopsys. Matthew P. Abdel, MD, declares relationships with Stryker, OsteoRemedies, Springer, AAHKS, and IOEN. Michael Bolognesi, MD, declares relationships with Smith & Nephew, Total Joint Orthopedics, Zimmer Biomet, EOA, SOA, OREF, and BOS (AAOS). Steven B. Haas, MD, declares relationships with Smith & Nephew, OrthAlign, Health Grades, and Knee Society. Gwo-Chin Lee, MD, declares relationships with Conformis, Corin, and Heron Therapeutics. David G. Lewallen, MD, declares relationships with Accuitive Technologies, Corin USA, Ketai Medical Devices, Zimmer Biomet, Mid-America Orthopaedic Association, and Orthopaedic Research and Education Foundation. Roberto Rossi, MD, declares relationships with Arthrex, Angelini Farmaceutical, Lima Corporate, and Zimmer Biomet. William Walter, MD, declares relationships with Depuy, Johnson & Johnson, Matortho, Microport, Navbit, Smith & Nephew, and Arthroplasty Society of Australia. Derek F. Amanatullah, MD, declares relationships with Exactech, Expert Institute, Knible Designs, Medacta, nSight Surgicak, QT Ultrasound, Recoup Fitness, Stryker, United Orthopedics, OREF, and NCATS. Brian P. Chalmers, MD, declares relationships with Orthodevelopment and DJO. Kevin B. Fricka, MD, declares relationships with Anderson Orthopaedic Research Institute, Operation Walk VA, Orthalign, Smith & Nephew, and Zimmer Biomet. Thorsten Gehrke, MD, PhD declares relationships with Waldeman and Zimmer Biomet. Carlos A. Higuera-Rueda, MD, declares relationships with Stryker, Zimmer Biomet, 3M, Osteal, Microgen Dx, OREF, KCI(3M), AAOS International Committee, AAHKS International Committee. Brett R. Levine, MD, declares relationships with Link, Zimmer Biomet, Smith & Nephew, Exactech, MAOA, AAOS, AAHKS. Joseph D. Lipman, MS, declares relationships with Exactech and John Insall Estate. Giles R. Scuderi, MD, declares relationships with Zimmer Biomet, 3M KCI, Canary, ROM Tech, KAT Robotics, Enhanced Medical Nutrition. Amar S Ranawat, MD, declares relationships with Depuy and India ROC. Ajay Premkumar, MD, declares relationships with Accujoint, Azra Care, and Osgenic. The other authors declare no potential conflicts of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Management of Bone Loss in Revision TKR Work Group and HSS Journal received financial support for the research, writing, and publication of this article from the Stavros Niarchos Foundation Complex Joint Reconstruction Center at Hospital for Special Surgery.
Human/Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2013.
Informed Consent
Informed consent was not required for this consensus statement.
Required Author Forms
Disclosure forms provided by the authors are available with the online version of this article as supplemental material.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.