
Abstract
Background
Cirrhosis is associated with an increased frequency of thromboembolic events, particularly in the portal sector. Several hypotheses have been put forward to explain this hypercoagulability state. However, studies assessing the expression of procoagulant microparticles (MP) in cirrhosis are rare.
Aims
To evaluate the expression of procoagulant MP in cirrhosis using thrombin generation (TG) test and to assess the activity of MP according to the clinical and biological status of patients.
Methods
39 cirrhotic patients and 39 control subjects were enrolled in a cross sectional comparative study. The biological explorations were performed at inclusion (The conventional tests of hemostasis, factor VIII (FVIII) and protein C (PC) assay and TG test carried out under sensitive conditions to MP activity and standard conditions).
Results
The mean age of patients was 65 years. Etiologies were dominated by viral infection (64%). The majority of patients were classified as Child-Pugh stage A (49%) and had decompensated cirrhosis (54%). Portal thrombosis was observed in 9 patients and hepatocellular carcinoma (HCC) was documented in 14 patients. Cirrhotic patients had higher FVIII/PC ratio and lower TG under different experimental conditions than controls. However, by expressing the results of MP dependent TG to the results of TG under optimal condition, patients generated as much thrombin as controls. MP dependent TG increased with the severity, decompensated status and complications of the disease.
Conclusion
The MP procoagulant activity in cirrhotic patients is comparable to that in controls and increases with disease severity, decompensation, and complications.
Plain Language Summary
For a long time, cirrhosis with liver failure was traditionally believed to cause bleeding tendency due to coagulation factors deficiency. However, it is now recognized that cirrhosis also increased the risk of blood clots. While several explanations have been proposed, a few studies have investigated the role of procoagulant microparticles (MP), defined as small membrane-derived vesicles released from cells during activation or apoptosis, in cirrhosis, despite their known role in clot formation in other diseases.
Therefore, this study aimed to assess the role of procoagulant MP in cirrhotic patients through thrombin generation (TG) assay, a global test of hypercoagulability. The levels of factor VIII (FVIII) and protein C (PC), representing procoagulant and anticoagulant factors respectively, were measured. the FVIII / PC ratio was calculated as marker of clotting tendency. A total of 39 cirrhotic patients and 39 healthy controls were enrolled. The mean age of patients was 65 years. Etiologies of cirrhosis were dominated by viral infection (64%). Mild cirrhosis was observed in 49% of patients and decompensated cirrhosis in 54%. Portal thrombosis was detected in 9 patients and hepatocellular carcinoma (HCC) was documented in 14 patients. The results showed that cirrhotic patients had higher FVIII/PC ratio and produced less thrombin (lower TG under different experimental conditions) than healthy individuals. However, when comparing MP related TG with TG under optimal conditions, patients generated as much thrombin as controls. MP dependent TG increased with severity, decompensation status and complications of the disease. In summary, MP procoagulant activity in cirrhotic patients is at least as high as in controls and increases further in severe, decompensated or complicated cirrhosis.
Introduction
Cirrhosis is the final stage of all chronic liver diseases. It is associated to hepatocellular insufficiency which is responsible for a decrease in coagulation factor synthesis. This results in a prolongation of coagulation times. Patients with cirrhosis are at high risk of bleeding and were considered for a long time as “naturally anticoagulated”. However, many observational studies have recently reported an increased frequency of thromboembolic events in cirrhotic patients in both portal and peripheral territories, compared to general population.1,2 Indeed, the decrease in procoagulant factors, along with that of anticoagulant factors, lead to a precarious hemostatic balance in cirrhotic patients.
Several studies evaluating hemostatic balance in cirrhosis using the thrombin generation (TG) test have shown an increased TG explained by a resistance to the inhibitory action of protein C (PC).3,4 Other hypotheses proposes that the hypercoagulability state in cirrhotic patients, particularly those with hepatocellular carcinoma (HCC) or portal thrombosis, may be driven by the increased expression of microparticles (MP) and their enhanced tissue factor dependent activity. 5
MP are extracellular vesicles released from cells membranes, including endothelial cells and platelets, by apoptotic or activation process. They can be explored using several quantitative and qualitative assays (TG assay, flow cytometry, and chronometric assays). 6 Circulating MP are endowed with procoagulant activity as they express tissue factor (TF) and phospholipids (PL) on their surface. They are considered as hypercoagulability markers in many diseases. 6
However, studies conducted to evaluate the expression of procoagulant MP during cirrhosis are rare and heterogeneous in methods and results. In this context, we have conducted this study to evaluate the expression of procoagulant MP in cirrhosis and to study the MP procoagulant activity based on their expression of TF and PL according to the clinical and biological status of the patients.
Materials and Methods
Study Population
A cross-sectional comparative study including 39 patients with cirrhosis was conducted in La Rabta University Hospital from 2017 to 2020. The diagnosis of cirrhosis was established on pathological evidence or on a set of clinical, biological, morphological or elastometric data. Non-inclusion criteria were ongoing anticoagulant or antiplatelet treatment, hormonal contraception, antiviral therapy, a known history of hemostatic diseases, extra hepatic malignancy, renal failure, infection, proinflammatory disease. Patients were compared to 39 age and gender matched healthy subjects with no comorbidities or ongoing treatment, selected as controls from outpatients, blood donors and laboratory staff.
Data Collection
The study was approved by the local ethical committee. Written informed consent was obtained from each patient and control. The following clinical and biological data were recorded at enrollment for each patient: gender and age, cardiovascular risk factors (including age, smoking, diabetes, hypertension, dyslipidemia, coronary artery disease and obesity), venous risk factors (including thrombosis history, venous insufficiency, surgery and immobilization), duration, etiology and severity of cirrhosis assessed by the Child-Pugh score, compensated/decompensated disease status, complications (including portal thrombosis and HCC), bilirubin and albumin plasma levels and platelet count.
Blood Sampling and Laboratory Tests
Peripheral venous blood was drawn into plastic tubes containing citrate (3.2%, 9:1). Poor platelet plasma was obtained after a double centrifugation at 2500 g for 10 min at room temperature. Aliquots were stored at −80 °C, in less than two hours, until analysis.
Classical coagulation times (prothrombin time (PT)), activated partial thromboplastin time (APTT) and fibrinogen assay) were measured on STA ® Evolution instrument from Diagnostica Stago, Asnière-France. Factor VIII (FVIII) and PC assays were performed on SysmexCS-2100i instrument from Siemens Health Care Diagnostic, Marbung, Germany. FVIII/PC ratios were calculated and compared between patients and controls.
The MP procoagulant activity was assessed by TG assay according to the calibrated automated thrombogram method as described by Hemker et al 7 The coagulation was triggered under three distinct experimental conditions. First, TF was added without PL using PRP-REAGENT® (Diagnostica Stago, Asnière-France) to evaluate the endogenous procoagulant activity of MP dependent on PL (MP-PL), second, PL was added without TF using MP-REAGENT® (Diagnostica Stago, Asnière-France) to assess the endogenous procoagulant activity of MP dependent on TF (MP-TF) and finally both TF (1 pmol/L) and PL (4 μmol/L) were combined using PPP-REAGENT® low (Diagnostica Stago, Asnière-France) to represent the optimal condition.
Depending on each experimental condition, a triggering reagent was added into a well of 96-well microtiter plate while 20 μL of prewarmed calibrator (thrombin calibrator® (Diagnostica Stago, Asnière-France) was added to another well, followed by 80 μL of plasma to both wells. After incubation at 37 °C for 10 min, coagulation was initiated by adding of CaCL2 and a fluorogenic thrombin substrate at zero time (FLUCA-KIT®; Diagnostica Stago, Asnière-France). The fluorescence arising from the action of the generated thrombin on its substrate was measured using a FLUOROSKANA scent (Diagnostica Stago, Asnière-France). The TG parameters analyzed included : the Lagtime (minutes), the time to peak (Ttpeak, minutes), the peak (nmol/L), the endogenous thrombin potential (ETP, nmol/L × min), and the velocity index (nmol/L/min). Tests were performed in duplicates for each patient by the same researcher.
The results obtained in the absence of PL or TF (MP-PL and MP-TF) were expressed as ratios compared to those obtained in the presence of PL and TF (optimal condition). The expression of the results as ratios makes it possible to better evaluate the own contribution of the MP in the TG and to minimize the inter-individual variations in the TG parameters.8,9
Statistical Analysis
Data analysis was performed with Statistical Package for the Social Sciences (SPSS) software version 20. Data were expressed as mean, standard deviation and percentage.
The comparisons of two means on independent series were carried out by the Student's test and in case of small numbers by the nonparametric test of Mann and Whitney.
The comparisons of several (> 2) means in independent series were performed using the Kruskall-Wallis H test of nonparametric analysis of variance.
The correlation between two quantitative variables was studied by the Pearson correlation coefficient. For all statistical tests, the significance level was set at .05.
The study reporting was guided by Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) recommendations.
Results
Clinical and Biological Data
The main patients’ characteristics are reported in Table 1.
Clinical and Biological Characteristics in Cirrhotic Patients and Controls.

Note: Values are mean ± standard deviation or number (percentage). *P < .05. Abreviations: ALD, alcoholic liver disease; APTT, activated partial thromboplastin time; ETP, endogenous thrombin potential; HCC, hepatocellular carcinoma; MP, microparticles; NAFLD, nonalcoholic fatty liver disease; PBC, primitive biliary cholangitis; PL, phospholipids; PT, prothrombin time; TF, tissue factor; TG, thrombin generation; TtPeak, time to peak.
The bold type indicates significant results.
Portal thrombosis was documented in 9 patients (23%). It was associated to HCC in 5 patients while 9 patients had HCC without thrombosis.
Factor VIII Levels, Protein C Levels and Factor VIII / Protein C Ratios
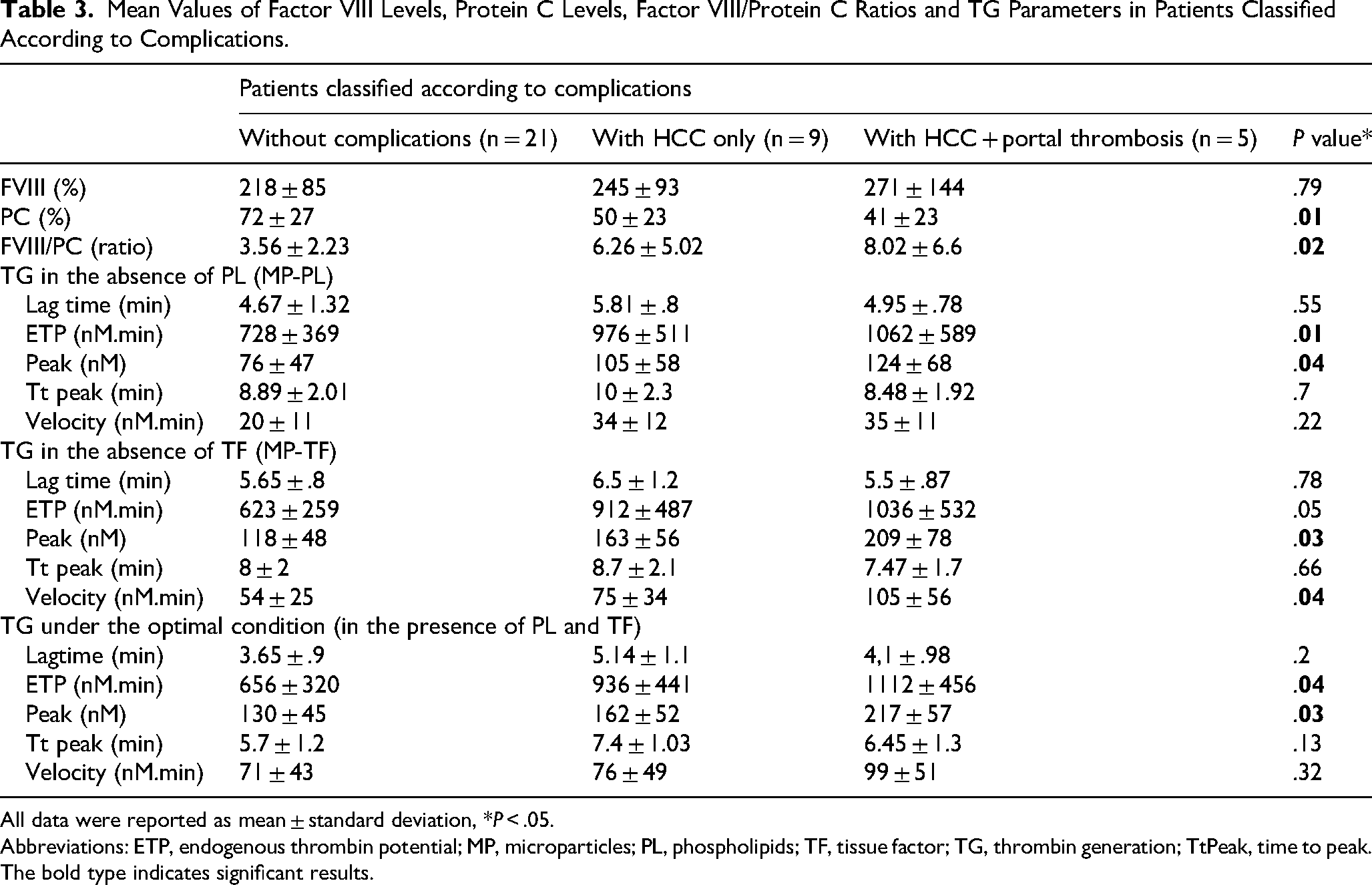
The mean level of FVIII was significantly higher in patients compared to controls (234% vs 152%; P < .0001) (Table 1). Levels of FVIII increased significantly from Child-Pugh stage A to stage B and C (193%, 239% and 325% respectively; P = .01) (Table 2). The mean level of FVIII was higher in patients with decompensated cirrhosis compared to those with compensated cirrhosis with no significant difference (249% vs 210%; P = .24) (Table 2). FVIII was higher in cirrhotic patients with both HCC and portal thrombosis compared to those with HCC only and patients with uncomplicated cirrhosis, with no significant difference (271%, 245% and 218% respectively; P = .79) (Table 3).
Mean Values of Factor VIII Levels, Protein C Levels, Factor VIII / Protein C Ratios and TG Parameters in Patients Classified According to the Severity of the Cirrhosis and the Compensated/Decompensated status.

All data were reported as mean ± standard deviation, *P < .05.
Abreviations: ETP, endogenous thrombin potential; MP, microparticles; PL, phospholipids; TF, tissue factor; TG, thrombin generation; TtPeak, time to peak.
The bold type indicates significant results.
Mean Values of Factor VIII Levels, Protein C Levels, Factor VIII/Protein C Ratios and TG Parameters in Patients Classified According to Complications.
All data were reported as mean ± standard deviation, *P < .05.
Abbreviations: ETP, endogenous thrombin potential; MP, microparticles; PL, phospholipids; TF, tissue factor; TG, thrombin generation; TtPeak, time to peak.
The bold type indicates significant results.
The mean PC level was significantly lower in cirrhotic patients compared to controls (61% vs 103%; P < .0001) (Table 1). PC levels tended to decrease with Child-Pugh stages with no significant difference (69%, 54% and 50% respectively; P = .07) (Table 2). PC levels were significantly lower in patients with decompensated cirrhosis compared to those with compensated cirrhosis (51% vs 76%; P = .03) (Table 2) and in patients with both HCC and portal thrombosis compared to patients with HCC only and patients with uncomplicated cirrhosis (41%, 50% and 72% respectively; P = .01) (Table 3).
FVIII / PC ratio was calculated and compared between cirrhotic patients and controls. The mean FVIII / PC ratio was significantly higher in patients compared to controls (5.01 vs 1.53; P < .0001) (Table 1). The FVIII / PC ratios increased significantly from stage A to stage B and C of Child-Pugh (3.14, 5.03 and 9.42 respectively; P = .004) (Table 2). They were significantly higher in patients with decompensated cirrhosis compared to those with compensated cirrhosis (6.3 vs 2.9; P = .04) (Table 2) and in patients with both HCC and portal thrombosis compared to patients with HCC only and patients without complications (8.02, 6.26 and 3.56 respectively; P = .02) (Table 3).
Evaluation of Microparticle Procoagulant Activity Using Thrombin Generation Test
Patients Versus Controls
TG in the presence of TF and PL (optimal condition) or in the absence of TF or PL demonstrated that the lagtime and the Ttpeak were significantly shorter in cirrhotic patients compared to controls, while the ETP and the peak were significantly lower than inf controls (Table 1).
- The endogenous PL and TF provided by MP were sufficient to accelerate the TG in cirrhotic patients but did not increase the overall amount of generated thrombin compared to controls under the conditions of the study. - The amount of thrombin generated in patients in the absence of exogenous PL or TF and attested by ETP was not different from that generated in the presence of PL and TF (optimal condition). In other words, the endogenous PL and TF derived from MP were capable of maintaining thrombin generation (Figure 1).
TG results expressed as ratios:
By evaluating the contribution of endogenous PL (MP-PL), the ETP and the peak expressed as ratios had become comparable in patients and in controls (ETP ratio = 1.13 vs1.02; P = .12 and peak ratio = .61 vs .07; P = .43). So, the endogenous PL made it possible to generate a quantity of thrombin in cirrhotic patients at least equal to that generated in controls.

Thrombin Generation Under Different Experimental Conditions in Patients and Controls. Abreviations : ETP, endogenous thrombin potential ; MP-PL, thrombin generation in the absence of phospholipids; MP-FT, thrombin generation in the absence of tissue factor ; P, P value. *: thrombin generation in the presence of both phospholipids and tissue factor. The amount of thrombin attested by ETP is lower in patients than in controls under the different experimental conditions. The amount of thrombin generated in the absence of PL or TF and attested by ETP was not different from that generated in the presence of PL and TF (optimal condition).
By evaluating the contribution of endogenous TF (MP-FT): The lagtime and the Ttpeak had become comparable in patients and in controls (Lagtime ratio = 1.44 vs 1.35; P = .55 and Tt peak ratio = 1.3 vs 1.23; P = .48). So, endogenous TF allowed a TG in cirrhotic patients as fast as in controls.
Patients Classified According to Disease Severity and Decompensated/Compensated Disease status
The ETP, the peak and the velocity tended to increase with the severity of the cirrhosis with no significant difference under the three experimental conditions. The ETP and the peak were significantly higher in patients with decompensated cirrhosis compared to those with compensated cirrhosis under the three experimental conditions (Table 2).
Patients with Hepatocellular Carcinoma with and Without Thrombosis
TG in the presence of TF and PL (optimal condition)
The amount of thrombin, assessed by the ETP and the peak, was significantly higher in patients with both HCC and portal thrombosis compared to patients with HCC only. Cirrhotic patients with HCC only had higher amount of thrombin than patients with uncomplicated cirrhosis (Table 3).
TG in the absence of TF or PL
The PL and TF dependent procoagulant activity of MP, as assessed by the ETP and the peak, was significantly higher in patients with both HCC and portal thrombosis compared to patients with HCC only who had a higher PL and TF dependent procoagulant activity of MP compared to patients without complications (Table 3).
Correlation Between Microparticle Procoagulant Activity and Factor VIII / Protein C Ratio
No correlation was found between the FVIII / PC ratio and TG parameters under the three experimental conditions. However, when expressed as ratios, the FVIII / PC ratio showed a negative correlation with both the lagtime and the Ttpeak (P = .008, correlation ratio r = −.42 and P = .004, r = −.45 respectively) and a positive correlation with the peak and the velocity (P < .0001, correlation ratio r = .56 and P < .0001, r = .57 respectively).
Discussion
This cross-sectional comparative study included 39 cirrhotic patients and 39 controls and aimed to evaluate the expression of procoagulant MP during cirrhosis as well as their procoagulant activity according to patients’ clinical and biological status.
Our results showed a higher FVIII/PC ratio in patients compared to healthy subjects and a lower TG in patients than controls under the different experimental conditions. However, by expressing MP dependent TG results as ratios, cirrhotic patients generated as much thrombin as controls.MP procoagulant activity was higher in severe, decompensated and complicated disease forms.
To our knowledge, this is the first study to evaluate the MP procoagulant activity in cirrhosis through the TG test under two different experimental conditions sensitive to MP (MP-PL and MP-FT). However, the study has several limitations that should be acknowledged: the lack of a prior sample size calculation that considered statistical power and the relatively small size of the study population may have reduced conclusions robustness. As recruitment occurred during the post-COVID-19 lockdown period, sampling process may have been affected. Another limitation is the reliance on a single method to explore the MP procoagulant activity, TG test, which did not allow for quantitative characterization of MP. Note that several studies have associated functional and / or quantitative tests (TG test, flow cytometry, chronometric tests…).
Hemostatic Balance in Cirrhotic Patients
FVIII is the most potent limiting factor in the amplification of TG while PC is one of the most important anticoagulant factors that regulate the decline in TG. 10 As a result, the high FVIII / PC ratio has recently been considered as a reflection of the hypercoagulability state by several authors. 11 In our study, the mean FVIII / PC ratio was significantly higher in patients compared to controls.
This was explained by the significant increase of FVIII level (firstly due to the factor VIII extrahepatic synthesis such as glomerular and tubular cells whom functioning is accelerated in hepatocellular deficiency and secondly the reduction of factor VIII clearance)10,12,13 and the significant decrease of PC level in cirrhotic patients (exclusively hepatic synthetic anticoagulant protein).14,15 In addition, this ratio increased significantly from stage A to stage C of Child-Pugh and was significantly higher in decompensated than compensated cases. These results demonstrate a state of hypercoagulability in cirrhotic patients, particularly during the advanced stages of the disease, and agree with those of Tripodi et al and Baccouche et al3,16 Furthermore, the FVIII / PC ratio was higher in cirrhotic patients with HCC and portal thrombosis compared to patients with HCC only who had a higher FVIII/PC ratio than patients with no complications.
Hypercoagulability State Evaluated by Thrombin Generation Test in Cirrhosis
According to our results, TG in optimal condition showed that the lagtime and the Ttpeak were significantly shorter in cirrhotic patients compared to controls. However, the ETP and the peak were significantly lower in cirrhotic patients compared to controls. An accelerated TG could be explained by the excess of endogenous TF in cirrhotic patients (main actor of the initiation phase of coagulation) which reduces the lagtime and therefore the time to peak in the presence of an excess of PL and FVIII (powerful factors of thrombin propagation phase). A decrease in the overall quantity of generated thrombin could be explained by the decrease in procoagulant factors in cirrhotic patients. 17 The action of anticoagulant factors, which is more modest than the action of procoagulant factors, has not been explored under the experimental conditions (in the absence of a PC activator). Studies evaluating TG in cirrhotic patients in the presence of a PC activator have shown that cirrhotic patients have acquired resistance to PC activation. 4 In fact, in the presence of a PC activator, the inhibition of the TG is less important in cirrhotic patients compared to control subjects and consequently the quantity of generated thrombin was comparable or even higher in cirrhotic patients. 16 Similar studies showed that the ETP was lower in cirrhotic patients compared to controls. By adding a PC activator, the ETP became comparable in the two groups.18–20
According to our results, TG study under optimal condition showed that the ETP, the peak and the velocity tended to increase from stage A to stage C of Child-Pugh with no significant difference. The imbalance between pro and anticoagulant factors creates a hypercoagulability state which worsens in advanced stages, being linked to hepatocellular deficiency. The difference was not significant given the small number of patients classified in different Child-Pugh stages. It has been reported in other studies that TG under standard conditions increases with disease severity. 21
Besides, our results showed that in decompensated forms, the ETP and the peak were significantly higher compared to compensated forms. This suggests that in decompensated cases, the fragile hemostatic balance in cirrhotic patients tended to hypercoagulability. 22 Moreover, the quantity of generated thrombin, attested by the peak and the ETP, was significantly higher in patients with HCC and portal thrombosis compared to patients with HCC only. These had higher ETP and peak compared to patients with uncomplicated cirrhosis. It can be deduced that the appearance of HCC worsens the basic hypercoagulability state of the cirrhotic patient, which may increase the risk of portal thrombosis. Indeed, it has been shown that the tumor cell is able to activate coagulation and generate high amounts of thrombin by two mechanisms: a direct mechanism through the expression of procoagulant factors (particularly TF) and indirectly by the release of mediators responsible for the activation of endothelial and blood cells and by the release of procoagulant MP.23–25
Microparticle Procoagulant Activity in Cirrhosis: Application of Thrombin Generation Test
Very few studies have evaluated the expression of procoagulant MP in cirrhosis.5,26 In addition, these studies are very heterogeneous due to the characteristics of the study population, the techniques and the experimental conditions.
Patients Versus Controls
According to this study, in the absence of exogenous PL or TF (MP-PL or MP-TF), the lagtime and the Ttpeak were significantly shorter in cirrhotic patients compared to controls. However, the ETP and the peak were significantly lower in patients compared to controls.
The variation in TG parameters was similar to that found under optimal conditions so this result can be explained by the absence of a PC activator. By adding a PC activator, the amount of generated thrombin in cirrhotic patients,would probably have been at least equal to that generated in controls. A single study involving 72 cirrhotic patients and 30 control subjects evaluating the MP procoagulant activity through the TG assay, in the absence of exogenous PL (MP-PL) showed that the MP procoagulant activity was significantly more important in patients than in controls. 27 TG results obtained in the absence of exogenous PL or TF expressed in ratios to TG results obtained under the optimal condition showed that: by evaluating the contribution of endogenous PL, the ETP and the peak had become comparable in patients and controls. By evaluating the contribution of endogenous TF, the lagtime and the Ttpeak had become comparable in the two groups. Thus, PL were primarily involved in the amount of thrombin while TF was primarily involved in the rate of TG. Moreover, MP procoagulant activity (attested by the ETP and the Peak) expressed as ratio was positively correlated to FVIII/PC ratio. Chronological parameters (the lagtime and the Ttpeak) were negatively correlated to FVIII/PC ratio.
Patients Classified According to Disease Severity, Decompensated/Compensated status and Complications
In our study, MP-dependent TG tended to increase in cirrhotic patients from Child-Pugh A to Child-Pugh C class.MP procoagulant activity in cirrhotic patients has been reported to increase with disease severity.28,29 Campello et al also showed in a recent study conducted in 2021, which included 80 patients with cirrhosis in advanced stages of the disease, that endothelial, platelet and total MP were higher in patients with severe cirrhosis. 30 This study showed significantly higher MP-dependent TG in patients with decompensated cirrhosis. This suggests, considering the procoagulant role of MP, that patients with decompensated cirrhosis have a higher thrombotic risk than patients with compensated cirrhosis. In addition, endothelial cells derived MP are involved in the vascular tone regulation 31 and the vascular permeability. 32 These two factors may be implicated, among others, in the occurrence of ascites in cirrhotic patients. Otherwise, MP dependent TG was significantly higher in patients with HCC only compared to patients without complications. HCC has been reported to be a cancer with high necrotic and apoptotic potential. 33 This may explain the increased release of MP by the tumor cells of HCC. Similarly, the study conducted by Campello et al that included 65 cirrhotic patients (33 patients with HCC and 32 patients without HCC), showed higher levels of MP, evaluated by flow cytometry, in patients with HCC compared to cirrhotic patients without HCC. 26
Besides, our results showed a higher MP dependent TG in patients with HCC and portal thrombosis than patients with HCC only. It has been reported that MP derived from apoptotic, activated or tumor cells contribute to thrombogenesis. 34 This may explain that increased MP procoagulant activity in HCC worsens the risk of portal thrombosis in cirrhotic patients. Campello et al concluded that cirrhotic patients with HCC had a higher risk of portal thrombosis than cirrhotic patients without HCC (24% vs 12% respectively). 26
In view of these findings, several mechanisms are involved in the hypercoagulability state in cirrhotic patients, particularly those with severe and advanced cirrhosis associated with HCC (the imbalance between procoagulant and anticoagulant factors attested by an increased FVIII/PC ratio, resistance to PC activation and increased release of MP). This could probably justify thromboprophylaxis during cirrhosis.
Conclusion
Our study has shown that MP procoagulant activity, expressed as ratio, is as high in cirrhotic patients as in controls. Additionally, MP-dependant TG shows an association with disease severity, complications occurrence and portal thrombosis and HCC association.
Also, MP procoagulant activity rises along with FVIII/PC ratio and may serve as a potential marker for hypercoagulability. However, we only focused on MP procoagulant activity without specifying their cellular derivation. Investigating both MP cellular origin and procoagulant activity could deepen our understanding of thrombogenesis factors.
Footnotes
Acknowledgements
We thank Dr Ben Romdhane N for her invaluable contribution to this work. Even though she is no longer with us, her enduring influence continues to inspire. This article stands as a tribute to her legacy.
Ethics Approval and Consent to Participate
The study was approved by the local ethical committee of La Rabta University Hospital. Written informed consent was obtained from each patient and control.
Consent for Publication
All patients and controls included in this study have given their consent for publication.
Author Contributions
Baccouche H, Belekremi M, Labidi A: designed the study.
Baccouche H, Labidi A, Chakroun A, Boubaker J, Mahjoub S: administered and validated the project.
Baccouche H supervised the project.
Chakroun A, Boubaker J, Mahjoub S: were involved in the project investigation.
Belakremi M, Labidi A: were involved in data collection and curation and specimens collection.
Belakremi M, Hadj Taieb R and Baccouche H: were involved in labratory experiments, analyzed the clinical and experimental data.
Belakremi M, Baccouche H, Labidi A: performed statistical analysis and software analysis
Belakremi M and Hadj Taieb R: wrote the original draft.
Baccouche H, Labidi A, Chakroun A, Boubaker J and Mahjoub S: reviewed and edited the paper.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors thank the Research and Innovation Commission of La Rabta Hospital that financed the purchase of reagents.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.