
Abstract
Background
Hepatitis B (HB) is a worldwide public health problem affecting around 250 million people. Only about 10% of people with HB are aware that they are infected. Vaccination is crucial to prophylactically controlling HB and the combination of vaccination and HB immune globulin (HBIG) are essential in preventing disease after exposure to the HB virus.
Objectives
In this article, a caprylate-chromatography process has been used for the production of HBIG (HBIG-C). The previously used solvent-detergent process produced an HBIG (HBIG-S/D) with an excellent safety profile but allowed the retention of some procoagulant plasma proteins. The present studies were conducted to assess the character and purity of HBIG produced by the caprylate-chromatography process.
Design and Methods
Several analytical methods (eg, chromatography, immunoassays, and nephelometry) were used to assess the molecular characteristics, purity and HBIG potency and specific activity of HBIG-C. In addition, testing was conducted to assess the levels of several pro-coagulant factors. HBIG-C was compared with HBIG-S/D and other immunoglobulins manufactured by the S/D process.
Results
The analysis of HBIG-C showed that the product was almost entirely IgG (99.3 ± 0.2% by electrophoresis) and that the residual IgA was less than that found in S/D products. The IgG present in HBIG-C was 99.7 ± 0.6% monomers and dimers as measured by size exclusion chromatography. Aggregates and fragments constituted < 1%. The IgG subclass distribution in HBIG-C was in the normal reference range. Coagulation factor impurities and pro-coagulant activity were reduced in HBIG-C compared to IgG prepared by the S/D method.
Conclusions
HBIG-C takes advantage of long-established donor selection processes combined with recently improved manufacturing processes to produce a safe and effective HBIG-product. HBIG-C combines high purity with reduced pro-coagulant factors in a product used for post-exposure prophylaxis of HB.
Introduction
Recent estimates suggest that 248-292 million people are living with chronic hepatitis B (HB) worldwide.1–4 Prevalence is highest in Asia and Africa with just five countries (China, India, Nigeria, Indonesia, and the Philippines) recording 57% of all HB virus (HBV) infections. 3 It has been estimated that only about 10% of the people living with HB are aware of that they have the infection,2, 3 due to the absence of significant symptoms in many newly infected people and the lack of access to testing in some areas of the world. 5
Some individuals acutely infected with HB will have significant symptoms (abdominal pain, nausea, vomiting, bilirubinemia, icteric sclera, and jaundice) 2 and a small percentage (1%-2%) will develop acute liver failure. 6 Individuals with acute HB can develop chronic HB (characterized by the presence of the HB surface antigen (HBsAg) in their blood for at least six months). Progression to chronic HB is affected by the individual's age at the time of infection. Only 5% of people infected as adults progress, while infected infants have a 20-60% chance of progression.7,8
While vaccination is a crucial factor in controlling the spread of HB infection. Hepatitis B immune globulin (HBIG) is an integral part of prophylactic treatment of individuals exposed to HB. This includes exposure to blood that is HBsAg-positive, infants exposed at birth (born to HBsAg-positive mothers), exposure through sex with an HBsAg-positive partner, and household exposure to a person with acute HB. 9 In addition, HBIG has played a crucial role in facilitating successful liver transplantation in recipients with HB-induced liver failure. In the early days of HB-related liver transplantation, the incidence of post-transplant HB was high which resulted in a lower survival rate for HB-related transplants than that seen in non-HB related transplants. 10 The advent of treatment with nucleotide/nucleoside analogs and HBIG has facilitated liver transplantation11,12 even in areas where the incidence of HB in the population is high. 13
In this paper, a process for purifying HBIG from plasma (caprylate/chromatography) was used and the characteristics of the resulting product (HBIG-C) are described. While the safety profile of HBIG manufactured using the previous solvent detergent purification process is excellent, some procoagulant factors were retained in the products. 14 The caprylate/ chromatography process was developed to reduce the procoagulant activity in the resulting HBIG-C product. This process has been used for the manufacture of polyvalent immunoglobulins15,16 and hyperimmune globulin for SARS-CoV-2. 17
Materials and Methods
Manufacturing Process
The manufacturing process starts with the collection of plasma from vaccinated donors with high titers of anti-HB virus (HBV) antibodies. This plasma was collected by plasmapheresis and was screened for many common blood-borne viruses in compliance with applicable regulatory guidelines and recommendations.18,19
Pooled plasma was treated by alcohol fractionation20,21 and resulting IgG-enriched Cohn Fraction II + II was further purified by caprylate treatment and chromatography.15,16 Figure 1 shows the caprylate/chromatography process in comparison with the solvent/detergent process. 22 The caprylate/chromatography process for HBIG-C is similar to that described for Gamunex™ (IGIV-C), a 10% polyvalent intravenous immunoglobulin produced by the caprylate/chromatography process, 15 with the exception of additional concentration steps to produce a final protein concentration of 16.5%.
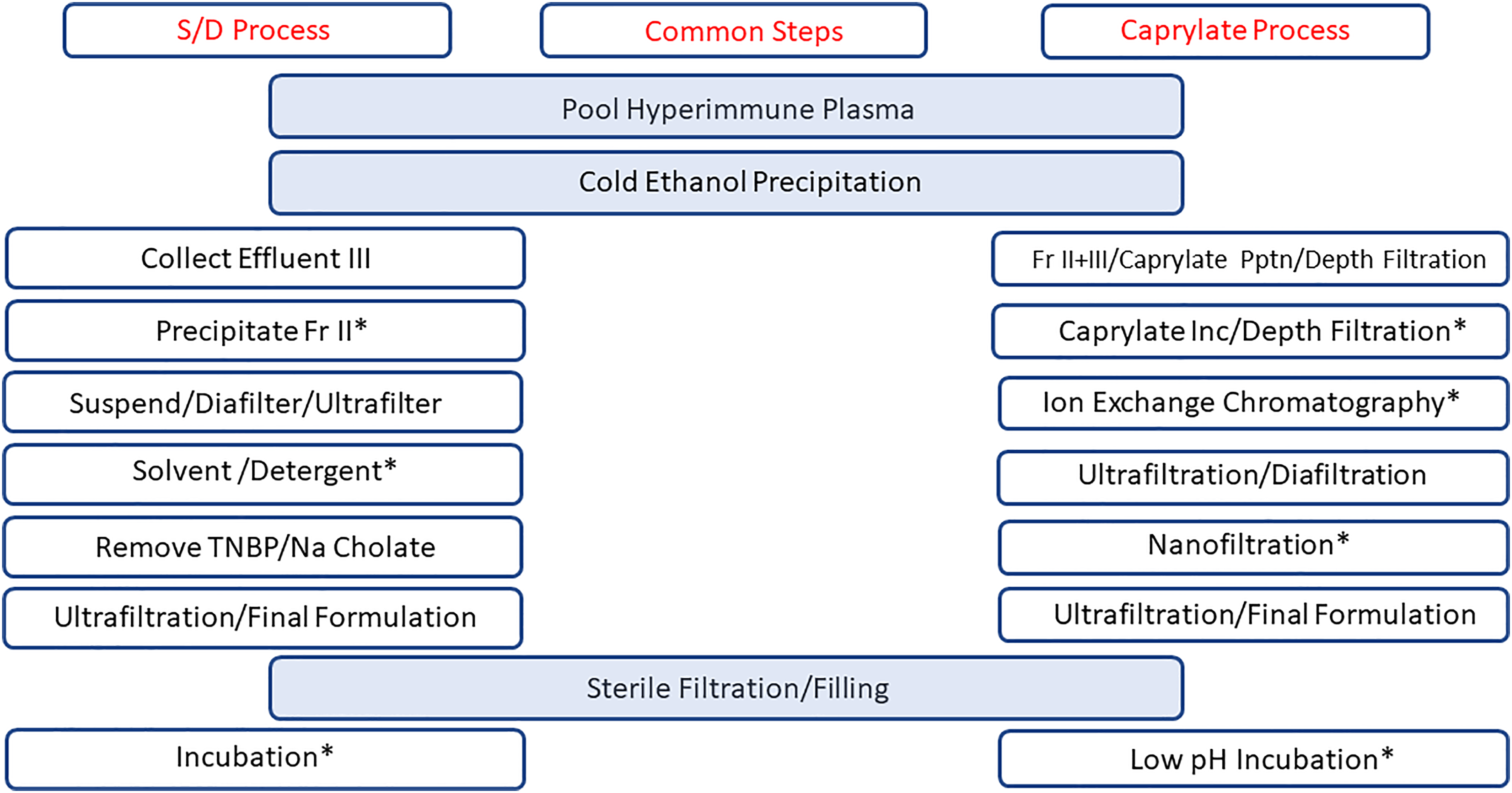
Diagrams representing two manufacturing processes for immune globulins: the solvent detergent (Sy/D) and the caprylate/chromatography process. Steps in the center column (blue) are common to both processes. Steps marked with an asterisk (*) have been shown to deactivate/remove potential infectious agents. Fr = fraction; TNBP = tri-n-butyl phosphate; Pptn = precipitation; Inc = incubation. Figure modified from Woznichak et al 27 .
In the caprylate/chromatography process (Figure 1), Fraction II + III was suspended in water for injection at approximately pH 4.2. Sodium caprylate (20 mM) was added and the pH was adjusted to approximately 5.1. During this step, impurity proteins and some caprylate were precipitated. The precipitate was is removed by filtration. After filtration, the caprylate concentration was readjusted to 20 mM and the solution incubated at pH 5.1. The solution was clarified by filtration. The filtrate was passed through two successive anion exchange chromatography columns (Q Sepharose Fast Flow (Millipore Sigma, Burlington, MA) followed by ANX Sepharose Fast Flow (Cytiva, Marlborough, MA)). The eluate was concentrated by ultrafiltration, diafiltered and nanofiltered. The purified IgG solution was adjusted to pH 4.2, 0.2 M glycine and further concentrated by ultrafiltration to reach 165 mg/mL protein. Bulk IGIV-C solution was sterile filtered, diluted to target potency with IgG manufactured using the same process, but starting with normal plasma, and then filled. The final product is incubated for 14-28 days at 23–27 °C for virus inactivation before storage at 2–8 °C.
The process has also recently been approved for use for manufacture of Xembify™ (IGSC), a 20% polyvalent subcutaneous immunoglobulin product. The caprylate/chromatography process includes several steps that have been validated for the removal or inactivation of blood-borne viruses.15,23–25
Product Characterization
Formulation Characterization
Full characterization of the HBIG-C was conducted to establish design space for manufacture of the product. This characterization also allowed comparison of new product, HBIG-C (HyperHEP B®, Grifols, Research Triangle Park, NC, USA) to immunoglobulin products produced by the prior process (solvent/detergent process: S/D). These products (HyperHEP B S/D®, HyperRAB S/D®; GamaSTAN S/D®, HyperTET S/D®, HyperRHO S/D®: Grifols, Research Triangle Park, NC, USA) are collectively referred to as IGIM-S/D. These S/D products are produced by the same manufacturing processes with the exception of starting with HB-vaccinated donors for HBIG-S/D, rabies-vaccinated donors for rabies immune globulin (RIG-S/D), tetanus vaccinated donors for tetanus immunoglobulin (TET-S/D), and Rho(D) vaccinated donors for Rho(D) S/D. Table 1 shows the formulations for HBIG-C in comparison to HBIG-S/D and IGIV-C 10%.
Product Formulations for Human Hepatitis B Immunoglobulin – Caprylate/Chromatography Process (HBIG-C), Human Hepatitis B Immunoglobulin – Solvent/Detergent Process (HBIG-S/D), and Human Immunoglobulin for Intravenous Injection – Caprylate/Chromatography Process IGIV-C) 10%.

NLT = not less than; NA = not applicable.
Molecular Characteristics
The molecular size distribution in the HBIG-C formulation was determined by size exclusion chromatography using previously described methods. 16 The percentage of monomers, dimers, aggregates and fragments were measured using a Tosoh TSK gel G3000SW column and a guard column consisting of the same packing as the analytical column (Tosoh Bioscience, LLC, King of Prussia, PA, USA) using an isocratic mobile phase of sodium phosphate and sodium chloride. The percent area of the peaks on the chromatogram were calculated relative to the total chromatogram.
Purity
The purity of IgG in HBIG-C was determined by agarose membrane electrophoresis with the Hydrasys-2 AME system (Sebia, Lisses, France). The IgG purity of IGIM-S/D was measured using a Beckman MDQ capillary zone electrophoresis system (Beckman Coulter, Fullerton, CA, USA). These two methods have been validated to give comparable results. Immunonephelometry was used to analyze the content of IgG, IgA, IgM and albumin in HBIG-C, and IGIM-S/D (BNII nephelometric system, Siemens Healthcare Diagnostics, Inc., Tarrytown, NY, USA).
Enzyme-linked immunosorbent assays (ELISA) and activity tests were used to determine the concentration of residual coagulation factors in HBIG-C. Factor XI content was measured by ELISA (Molecular Innovations, Inc., Novi, MI, USA) using the World Health Organization (WHO) second International Standard for Factor XI (Code 15/180) from National Institute for Biological Standards and Control (NIBSC, Hertfordshire, England, UK). Factor XII content was measured using an ELISA from Assaypro, Inc., Saint Charles, MO, USA using a manufacturer provided Factor XII standard. Activity of Factor XIa was measured using a kit (Rossix Rox Factor XIa Kit, Rossix AB, Taljegårdsgatan 3B, SE-431 53 Mölndal, Sweden: American distributor: Diapharma Group, Inc., West Chester, OH, USA) and a standard linked to the WHO first International Standard for Factor Xia (Code 13/100, NISBC). Prekallikrein activator (PKA) was measured using a spectrophotometric assay 14 with a PKA reference preparation (EDQM, Strasbourg, France).
In addition, thrombin generation time (TGT) and non-activated partial thromboplastin time (NAPTT) tests were conducted to measure any residual pro-coagulant activity. The TGT used a Technothrombin TGA Kit (Technoclone GmbH, Vienna, Austria) using a reference linked to the international standard (Code 13/100, NIBSC). NAPTT utilized a Siemens BCS-XP Coagulation Analyzer (Siemens Healthineers, Tarrytown, NY, USA) based on the European Pharmacopeia assay. 26
HBIG Potency and Specific Activity
HBIG potency was measured with the Bio-Rad enzyme immunoassay to detect antibodies to HBsAg (Monolisa Anti-HBs EIA, Bio-Rad Laboratories, Inc., Hercules, CA, USA) using an in house standard with value traceable to the WHO International Standard for WHO second International Standard for Anti-Hepatitis B Surface Antigen Immunoglobulin (NIBSC Code 07/164). HBIG specific activity (International Units (IU)/mg IgG) was calculated by dividing HBIG potency (IU/mL) by IgG concentration (mg/mL).
Results
Product Formulation
As described above, the caprylate/chromatography process for HBIG-C was adapted from the process for IGIV-C 10% and IGSC 20%. HBIG-C was formulated to have the same protein concentration as HBIG-S/D and the same nominal (labeled) HBIG potency (Table 1). The pH profile for HBIG-C was lower than HBIG-S/D but similar to IGIV-C. The glycine content of HBIG-C was similar to the content for HBIG-S/D and IGIV-C, but unlike HBIG-S/D. This new formulation contains no added NaCl.
As shown in Table 2, analysis for protein content showed that the test batches of HBIG-C had a protein content of 17.1 ± 0.3%, similar to that seen for IGIM-S/D (16.5 ± 0.3%). The pH for HBIG-C formulation was lower than IGIM-S/D while the glycine concentration was similar. The osmolality of the caprylate formulation was lower and closer to physiologic than the S/D formulation. The viscosity and turbidity were also lower than the S/D formulation.
Formulation Data for Human Hepatitis B Immunoglobulin – Caprylate/Chromatography Process (HBIG-C) and Human Immunoglobulin – Solvent/Detergent Process (IGIM-S/D.

Data shown are the mean ± SD. cP = centipoise; NTU = nephelometric turbidity unit.
Composition and Purity
Electrophoretic determination of purity IgG purity in HBIG showed that this formulation was almost entirely IgG (99.3 ± 0.2%; Table 3). This purity was similar to that seen with IGIM-S/D. Small amounts of IgA were detected in the final HBIG formulation, but approximately half of similar IG products produced by the S/D process (IGIM-S/D). IgM was detectible in IGIM-S/D, but the levels were below the limits of quantitation in HBIG-C.
Purity and Molecular Composition of Human Hepatitis B Immunoglobulin - Caprylate/Chromatography Process (HBIG-C), Human Immunoglobulin - Solvent Detergent Process (IGIM-S/D).

Samples of HBIG-C were assessed by size exclusion chromatography to determine the molecular distribution of IgG: monomers, dimers, aggregates, and fragments. HBIG-C had an average of 99.7% of monomers plus dimers compared to 99.0% for IGIM-S/D. The IGIM-S/D products had a detectible level of polymers and aggregates, while in HBIG-C polymers and aggregates were below the quantifiable limits of the assay.
Testing was also conducted for residual coagulation factor impurities in the final HBIG formulation. Table 4 shows the amounts of residual coagulation factor impurities measured in the HBIG-C formulation compared to immunoglobulins produced using the S/D process. These data show a substantial reduction in coagulation factor impurities by the caprylate/chromatography process. All the coagulation factor impurities analyzed (Factor XI, Factor XIa, PKA) were reduced by the caprylate/chromatography process with the exception of Factor XII which was already below quantifiable limits in products generated by the solvent/detergent process.
Measurement of Coagulation Factor Impurities in Human Hepatitis B Immunoglobulin - Caprylate/Chromatography Process (HBIG-C) and, Human Immunoglobulin - Solvent Detergent Process (IGIM-S/D).

These data are the mean ± SD. FXI = Factor XI; FXIa = activated Factor IX; FXII = Factor XII; NAPTT = non-activated partial thromboplastin time; TGT = thrombin generation time; PKA = prekallikrein activator.
In addition, non-activated partial thromboplastin times (NAPTT) were measured for HBIG-C and IGIM-S/D. NAPTT is a global assay for coagulation activity in human plasma. The NAPTT assays gave a result > 200 s indicating absence of pro-coagulant substances. NAPPT times <200 s indicate the presence of pro-coagulant substances. TGT was also performed to assess the presence of activated coagulation factor impurities. These tests gave values below the limits of detection for HBIG-C.
IgG Subclass Distribution
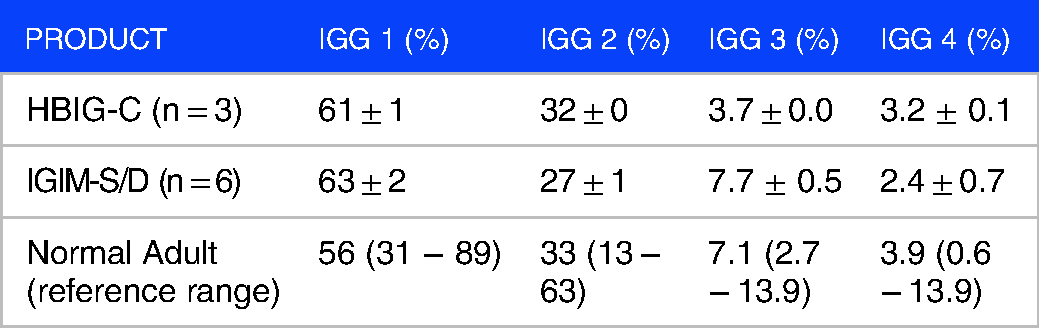
The subclass distribution of IgG in HBIG-C and IGIM-S/D are shown in Table 5. The mean values are within the normal adult range . 27 IgG 1 levels were slightly higher than the normal adult average. IgG2 levels were slightly lower and IgG 3 values were higher than the normal adult average in the IGIM-S/D products. IgG 4 percentages were similar for these products and lower than the normal adult range.
Immunoglobulin G (IgG) Subclass Distribution Comparison of Human Hepatitis B Immunoglobulin - Caprylate/ Chromatography Process (HBIG-C) and Human Immunoglobulin - Solvent/ Detergent Process (IGIM-S/D).
Specific Activity Through Manufacturing Process
HBIG potency and specific activity were measured at various steps during the manufacturing process. At the Fraction II + III paste suspension step, the hepatitis paste was blended with non-HBIG paste to better target final product potency needed. Figure 2 shows that HBIG potency decreased from 75 ± 12 IU/mL in the plasma pool to 24 ± 3 IU/mL at caprylate incubation/filtration step. Then potency increased up to the master bulk stage (1091 ± 127 IU/mL). Master bulk is the purified and concentrated bulk formulated to a target 16.5% IgG concentration. The Master bulk was diluted with polyvalent IgG produced using the same caprylate/chromatography) process before filling in order to meet labeled potency. The labeled potency was set to meet the U.S. Centers for Disease Control and Prevention (CDC)/Advisory Committee on Immunization Practices (ACIP) recommendation of 0.06 mL/kg dosing for post-exposure prophylaxis. 28

Potency (blue bars) and specific activity (orange line) of HBIG through the caprylate/chromatography process. At the Fraction II + III paste suspension step, hepatitis paste was blended with non-HBIG paste. Specific activity values are normalized to Hepatitis paste for Fraction II + III to Master Bulk steps. II + III Paste Suspension = Fraction II and fraction III paste after ethanol precipitation; MIC-1 = caprylate precipitation and filtration; MIC-2 = caprylate incubation and filtration after MIC-1; Conc. Column FT = column flow through concentrated to 10% IgG.
HBIG specific activity, expressed as HBIG activity per mg of IgG, was normalized to the hepatitis paste. (Figure 2). Specific activity was 12 ± 1.9 IU/mg IgG in the plasma pool, increased to 13 ± 0.7 IU/mg IgG for the Master Bulk after the concentration steps. The normalized HBIG specific activity was maintained throughout the fractionation and purification steps.
Discussion
The manufacturing processes described herein were patterned after those used in the production of 20% IG for subcutaneous use (Xembify®, Grifols, Clayton, NC, USA) and 10% IGIV (Gamunex-C®, Grifols).16,29 The low pH, un-buffered glycine formulation has demonstrated suitable tolerability and shelf life stability for these products. The caprylate chromatography process is being utilized not only for development of HBIG-C but also for hyperimmune globulin products to treat several other diseases including COVID-19, 17 rabies 30 and tetanus. 31
Based on the studies presented in this article, the caprylate/chromatography process results in highly purified product that incorporates multiple steps to maintain a high degree of safety with respect to transmission of infectious agents. As a first step, donors with high titers of antibody to the hepatitis B surface antigen are rigorously screened, and their plasma is extensively tested to confirm the absence of infectious diseases. In addition, the caprylate/chromatography process incorporates steps that have been demonstrated to remove or inactivate blood-borne infectious agents. Caprylate forms a precipitate with impurities and any residual infectious agents and this precipitate is removed by depth filtration. 24 Further exposure to caprylate by incubation destroys the envelope of lipid encased viruses and provides inactivation capacity should any residual virions be present.15,23,32 The caprylate treatment provides a robust replacement for the S/D treatments that was used with the earlier S/D process. 15 Other steps in the caprylate/chromatography process that can remove and/or inactivate viruses include column chromatography, nanofiltration and the terminal incubation at low pH. 25
The caprylate/chromatography process also improved the removal of pro-coagulant protein impurities. The tests for Factor XI content and activity showed levels below quantifiable levels in the product of the caprylate/chromatography process. This reflects a decrease of greater than 11,000-fold in Factor XI content from pooled plasma. Similar results were obtained when Factor XII content was measured. The final container had Factor XII content over 850-fold lower than the content in the plasma pool. Similarly, PKA activity was below the limit of quantitation in HBIG-C. This removal of pro-coagulant factors is reflected in the NAPTT and TGT test results. For HBIG-C showed undetectable levels for coagulation activity, confirming the effectiveness of the caprylate/chromatography purification process. It has been shown previously that caprylate precipitation steps in particular provide robust removal of coagulation factor impurities. 29
Analyses also showed that the protein content of HBIG-C was nearly 100% IgG. In addition, the IgG content of HBIG-C was found to be nearly 100% monomer plus dimer. Due to their similar activity, monomer and dimers are grouped together as “monomer plus dimer” for purity with respect to molecular size distribution. 33 Testing of IgG subclasses showed that the distribution of subclasses in HBIG- C was similar to that seen in normal human plasma.
Additionally, the content of IgA in the final HBIG-C formulation was low. The presence of IgA has the potential to produce hypersensitivity reactions in IgA-deficient patients who have been previous exposed to blood products, and therefore lower levels are considered more desirable. However, HBIG-C and other blood-derived products are labeled with warnings about potential hypersensitivity reactions in IgA-deficient patients and extra caution is warranted in these individuals.
The manufacturing process concentrated HBIG activity in addition to removing unwanted plasma proteins. The overall HBIG potency (IU/mL) increased through the purification and concentration steps from the original plasma pool to the master bulk. During purification, at the Fraction II + III suspension step, the HBIG paste was blended with non-HBIG paste also to better target the final product potency. The resulting master bulk was then further diluted with normal immunoglobulin before filling in the final container to provide the correct labeled dosage. 28 The normalized HBIG specific activity (IU/mg IgG) is maintained from the pool to master bulk through the fractionation and purification processes.
In conclusion, the process used to produce HBIG-C utilizes the latest in donor-screening and manufacturing processes to produce a concentrated, HBIG product useful for the post-exposure prophylaxis of HB. The long safety record of the safe use of plasma-derived products has been combined with newly developed purification techniques to produce a product with high purity and minimal levels of coagulation factor impurities.
Declarations
Ethics Approval and Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Author Contribution(s)
Acknowledgements
Michael K. James, PhD (Grifols) is acknowledged for medical writing and Jordi Bozzo, PhD, CMPP is acknowledged for editorial support in the preparation of this article. Bing Robertson, the Grifols QC Biochemistry Lab and Grifols Bioanalytics Lab for performing characterization testing.
Competing Interests
All of the authors are current employees of Grifols or were employed by Grifols at the time these studies were conducted.
Availability of Data and Materials
The underlying data for these studies is available from the corresponding author upon reasonable request.