
Abstract
Voluntary non-remunerated blood donation is well-established in many countries; however, this approach is under pressure to provide sufficient plasma for future needs. In this article we consider various aspects of plasma donation, including donor characteristics, health and safety issues, and motivating factors, including the potential role of incentives. The status of plasma donation in various European countries, and challenges associated with the COVID-19 pandemic are also discussed. Common motivators for plasma donors include the benefit that donated plasma provides for other people, the sense that helping others is in their nature, a sense of pride at undertaking a special task, and the desire to achieve donation goals. Motivations may differ between age groups and gender. Donating plasma is safe and adverse events are infrequent, with the most common being hypotensive/vasovagal events and phlebotomy events. The main reasons plasma donors discontinue are socioeconomic, relating to the time required and conflicts with work and other commitments. When persuading donors to convert from whole blood to plasma donation, face-to-face requests are more successful than leaflets or telephone/email requests, and clear information addressing health and safety concerns is needed. However, telephone/email communication can be helpful for encouraging plasma donors to return for future donations or to donate more frequently. There is ongoing debate about non-remunerated versus remunerated plasma donation. Remuneration may be an incentive for some individuals, whereas it may deter people who have a strong altruistic drive. It has been suggested that a combination of paid and unpaid donation systems could cover a wider range of potential donors. Most European countries currently have non-remunerated donor systems, but a few do allow monetary compensation.
Introduction: Plasmapheresis
Plasmapheresis involves the removal of blood plasma from an individual and the return of cellular components back into the circulation.1,2 For plasma donation, a small volume of plasma (less than 16% of total blood volume according to the European Regulations) is removed, with no need for replacement. 3 The donated plasma is stored as fresh frozen plasma and subsequently used for transfusion and/or in the manufacture of therapeutic products such as albumin, immunoglobulins and coagulation factors4–6 (Figure 1).
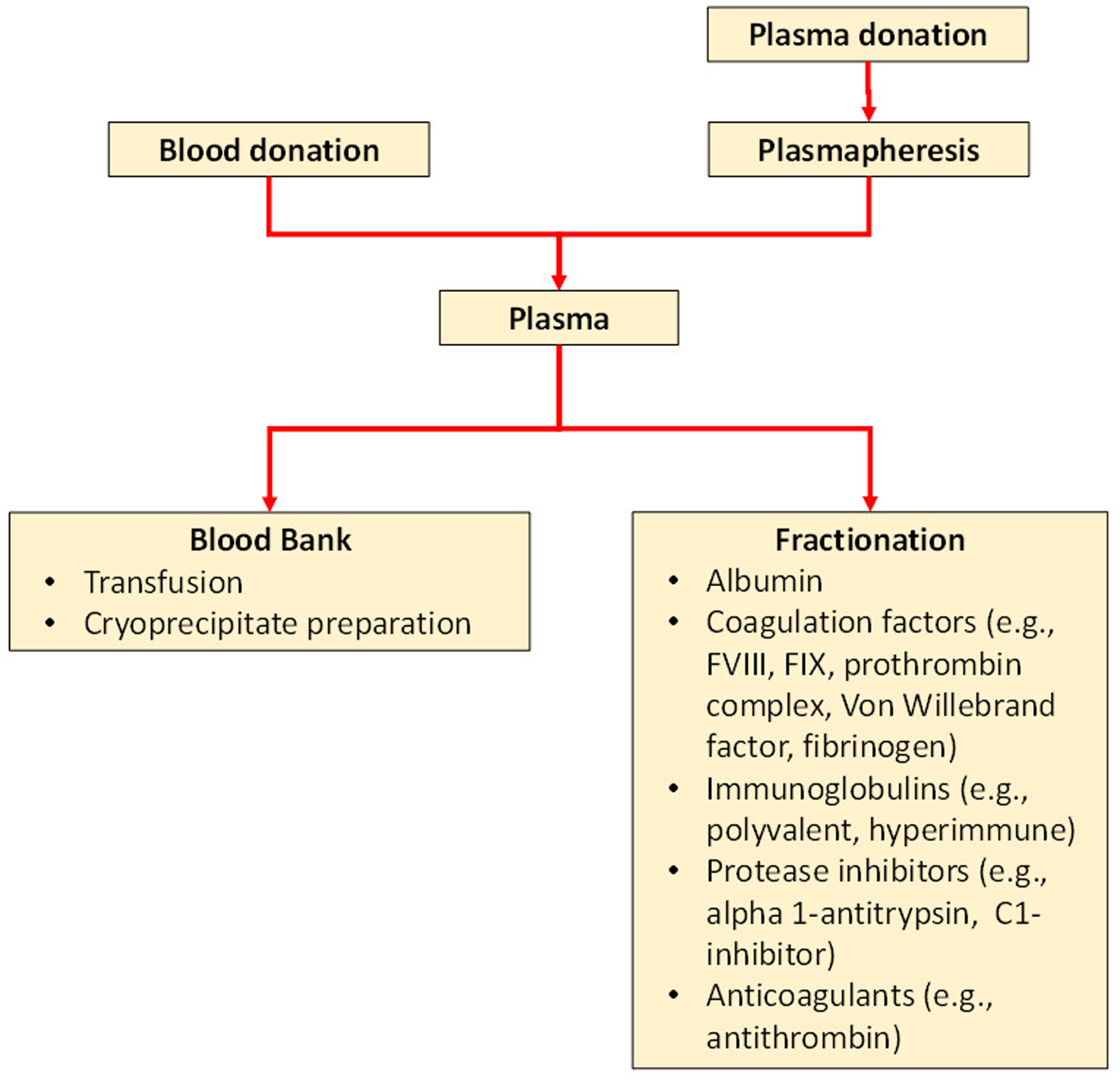
Blood plasma flow chart: from donation through to therapeutic use (plasma exchange) and fractionated products.
Blood donation services play a pivotal role in assuring adequate blood donations and ensuring the safety of donors. Voluntary, non-remunerated whole blood donation is well-established in many countries and is supported by the WHO. 7 However, this approach is under pressure to provide sufficient plasma, and reliance on this strategy alone may not meet the needs of all patients requiring plasma derived medicinal products. 8
Therefore, plasma donation is essential to cover the growing need for plasma-derived medicinal products. This narrative review considers various aspects of plasma donation, including donor characteristics, health and safety issues, methods of encouraging donations and motivating donors, the status of plasma donation in various European countries, and challenges associated with the COVID-19 pandemic. Relevant papers were identified by a search of PubMed up to 21 December 2021 for studies of any design related to plasma donor characteristics and motivators, and also for reports on plasma donation status in selected European countries.
Plasma Donors
general characteristics
Few studies have reported specifically on the characteristics of plasma donors; available data come from different countries. A German study found that 56.8% of donors were male and that the mean age of first-time donors was 29.8 years while that of repeat donors was 43.2 years. 9 The proportion of males and the mean age of plasma donors was lower than among whole-blood donors. Plasma donors made an average of 14.2 donations/year. A large US study of source plasma donors found that 62% of donors were male and the average age of first-time and repeat donors was 30 and 36 years, respectively. 10 A study in the Netherlands found that most plasma donors were in employment (76-79%) and were living with a partner and children (74-86%). Approximately one-third (34-36%) had completed higher education, which was higher than in the general Dutch population. Donors were healthier than the general Dutch population. 11
perceived benefits and drawbacks of plasma donation for the donor
A survey of donors in Australia found that the perceived benefits of plasma donation for themselves included the increased frequency of donation compared with whole-blood donations, which helped them to establish a donation routine, and the increased interaction with centre staff, which made the process more pleasant. The donation procedure was felt to be less taxing than whole-blood donation and they were less likely to be medically deferred. 12 Donors had the idea that plasma donations were particularly helpful to the blood service and reported feeling special compared with whole-blood donors.
Perceived negative aspects of plasma donation included greater inconvenience, particularly in relation to the long donation time, as well as arm discomfort from the prolonged time the needle was in place, increased tiredness, and excessive paperwork and expectations from the collection service. 12
safety
It is noteworthy that plasma donation is a safe process and that donors have a favourable experience. Adverse events are uncommon, occurring in only 0.16–2.3% of plasma donations and affecting 1.74% of the donors.10,13 Adverse events are more common in females and first-time plasma donors. In a recent study, the rate of adverse events was 2.6-fold higher in females than males and 11-fold higher in first-time donors than in repeat donors. 10 One study reported rates of 7.96% in first-time plasma donors and 1.01% in repeat donors. 9
The most common adverse events are hypotensive/vasovagal events and access-site events, which together account for up to 90% of adverse events. 10 Hypotensive/vasovagal events have been reported to affect 0.49% of whole blood donors 9 and 0.16–1.2% of plasma donations,13,14 while phlebotomy adverse events occur in 0.52% of donors. 9 Citrate reactions affect 0.38–0.49% of plasma donations.10,14 Severe or potentially serious events are rare.10,14
Limited data suggest that plasma donation is also safe over the long-term. No significant changes were seen in total serum protein, immunoglobulin G, haemoglobin, ferritin, transferrin or cardiovascular risk markers after 3 years in participants of an intensive plasmapheresis programme. 15
factors leading to discontinuation
The scarce data available from plasma donors suggest that the main reasons for discontinuation are usually socioeconomic, rather than concerns directly related to the donation process (Table 1).15–18 In particular, the relatively long time required for the plasma donation process often conflicts with donor work or family commitments. Other reasons include excessive paperwork or changes in eligibility. Although adverse events are uncommon, they can have a negative effect on donor return, with syncope being a particular concern. The specific populations that were evaluated differed between studies (eg, lapsed donors, returning donors, people switching donation intensity/type); the results of individual studies are described below.
Summary of reasons donors discontinue making plasma donations.

* Donors can be paid in the USA.
Among Americans who ceased donating after having made multiple previous donations, the most common reasons were work conflicts (23%), length of time of the procedure (23%), time and difficulty associated with getting to the site (21% and 10%) and no longer needing remuneration (22%; donors can be paid in the USA). 16 Among experienced German donors who switched from a moderate to an intensive donation programme (median 49 donations/year), the most common reasons for cessation were socioeconomic (47.2%), such as lack of time, work conflicts or moving from the area. 15 Among lapsed plasma donors in Australia, the most common reason (10 of 17) was a life event that made donation inconvenient (eg, moving to a new house, changing jobs, having children). 17 Australian plasma donors who reverted to whole-blood donation most often did so because of the time required for plasma donation, or because of excessive questioning and paperwork. 19
In a large study of Australian plasma donors, rates of return for further donations were significantly (p < 0.01) lower after the occurrence of syncope (46% returned), presyncope (71%), a citrate reaction (87%) or phlebotomy injuries (88%) compared with donors who had an uncomplicated donation (92%). 13 Those who did return took longer to do so, particularly after experiencing a vasovagal reaction (161 days following syncope vs 39 days following an uncomplicated donation) and gave fewer subsequent donations (median 2 after a vasovagal reaction vs 6 after an uncomplicated donation). A significant negative association between vasovagal reactions and the intention to return for future donations was found among first-time plasma donors. 18
Among German donors who had switched from a moderate to an intensive donation programme, 11.1% ceased donating because of medical reasons unrelated to plasma donation (eg, elevated alanine transferase). 15 In the study of lapsed plasma donors in Australia, 5 of 17 individuals indicated that temporary changes in eligibility had disrupted their donation practice. 17
Motivating and Persuading Donors
The main focus of this section is on voluntary non-remunerated donors. Most plasma donors have previously donated whole blood. To be able to encourage more donors, it is important to understand why people switch to plasma donation and what can be done to motivate individuals to continue making donations.
motivators
The reasons donors are motivated to make voluntary donations can be grouped as moral or altruistic, subjective or non-altruistic, and other unspecific reasons (Table 2).20–26 Common motivators for plasma donors include the benefit that donated plasma provides for other people, the sense that helping others is in their nature, a sense of pride at undertaking a special task, and the desire to achieve donation goals.
Summary of reasons donors are motivated to make voluntary plasma donations.
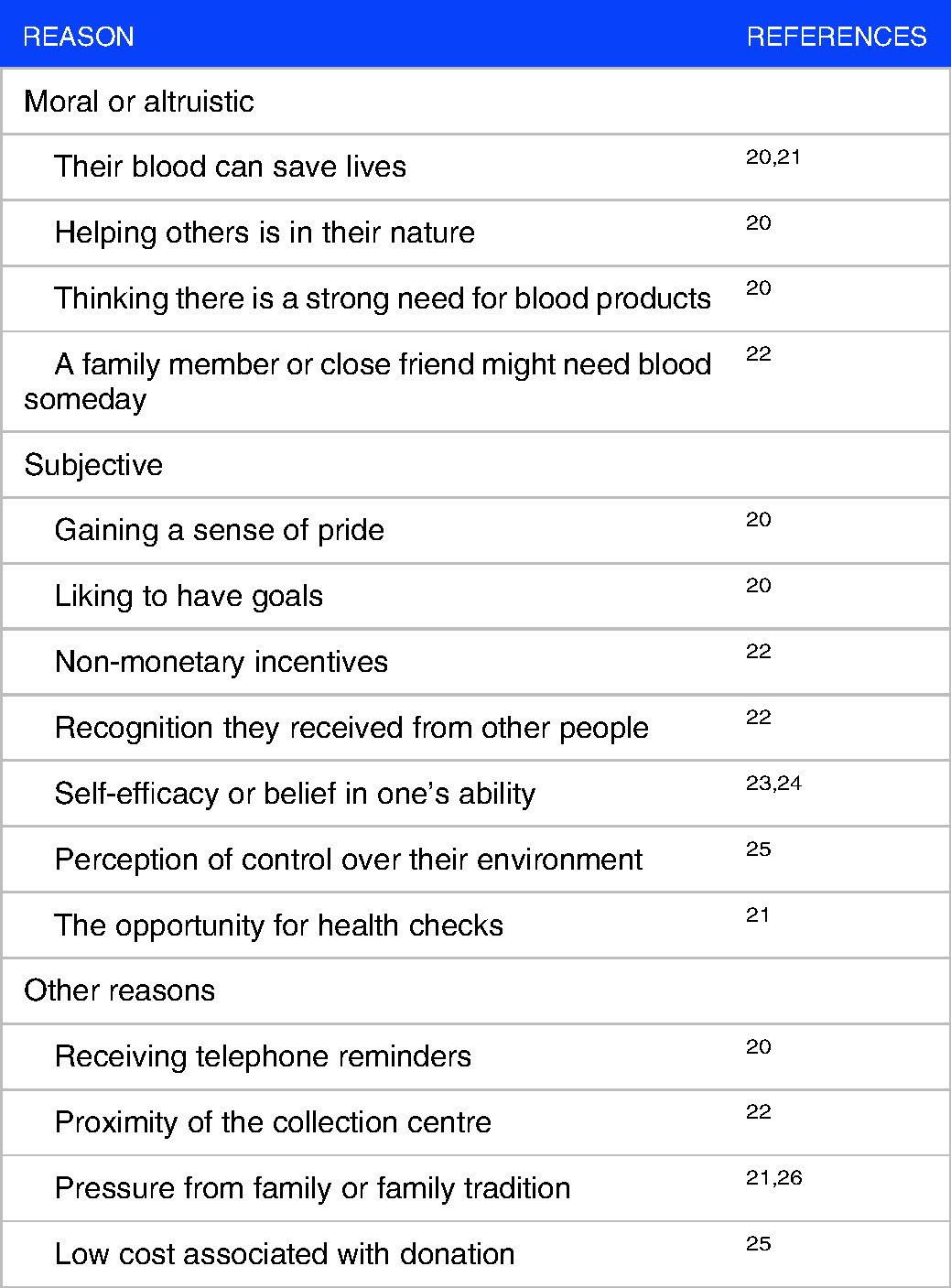
Motivators may differ between plasma and whole-blood donors. A Canadian study found that the greatest motivator for both whole-blood and plasma/platelet donors was that their blood can save lives. 20 The second most common motivator for plasma/platelet donors was that helping others was in their nature, whereas for whole-blood donors, it was that donating was a positive thing to do and required little effort. Other motivators that differentiated plasma/platelet donors from whole-blood donors included thinking there was a strong need for blood products, gaining a sense of pride, liking to have goals, and receiving telephone reminders. This suggests that ongoing support from blood collection agencies is important for motivating plasma donors. 20 However, plasma donors in France expressed no specific motivation other than a favourable attitude to voluntary donation, although a perception of control over their environment and the low cost associated with donation also affected their decision to donate. 25
Different demographic groups may also have slightly different motivations for plasma donation. A small study found that whole-blood donors aged ≥50 years were most likely to later make a plasma donation. 27 In Canada, donors aged >50 years were most likely to be motivated by saving lives or thinking there was a strong need for plasma, whereas donors in their thirties were motivated by the idea that a family member or close friend might need blood someday. 22 A systematic review found that the most common motivators for men to donate blood or undergo apheresis were subjective norms (such as pressure from family), non-monetary incentives, the opportunity for health checks and altruism. 21 One study found that male plasma/platelet donors were most likely to be motivated by donation goal achievement and the recognition they received from other people, whereas the proximity of the collection centre was particularly important to female donors. 22
Family tradition and inherited family values can have a substantial effect on whether people chose to become plasma donors and their commitment to continuing to donate; committed donors under the age of 35 years often have a strong family tradition of donation. 26
Psychological characteristics may also be relevant. A study using a Theory of Planned Behaviour approach found that moral norm and self-efficacy (belief in one's ability) were positively associated with intention to donate plasma, while role identity was negatively associated. 23 Another study found that social or functional labelling had little effect on persuading individuals to convert from whole blood to plasma donation. 28
Motivational differences may exist between future whole-blood and plasma donors even before their first donation. 24 A study found that future plasma donors were more motivated, had higher levels of self-efficacy (ie, felt more able to donate), had more positive attitudes towards donating blood, were less anxious about donating, expressed higher levels of conscientiousness and had a higher level of expected return behaviour.
triggers for first donation
Many people first gain awareness of plasma donation when donating whole blood, either through observation of the process or through the provision of information by staff, while others learn about it from family or friends. 12 The main trigger to convert from whole blood to plasma donation is usually a request by blood centre staff. 12 Face-to-face conversations achieve higher conversion rates than interactions via a call centre. 29 Compared with handing people a leaflet, provision of information by a nurse was found to lead to a higher proportion of new plasma donors, as well as an increased frequency of donation, particularly when the nurse-led information included a self-positive image message. 30 The institutional context is also relevant; a survey of whole-blood donors who had recently made their first plasma donation found that it was important that the request to switch came from the same blood collection organization with which they were already engaged. 31
Key deterrents to converting from whole blood to plasma donations include the time required, and a lack of knowledge about the process and safety. 19 This suggests that provision of clear information about health and safety concerns is important when asking people to convert.
continuing donations
A survey of experienced plasma donors found that the key motivator for continued donation was knowing their donations helped other people. They often adopted a flexible approach to donation frequency in order to continue making donations while fitting it within busy lives. 32
Use of email and telephone communications that provided education about plasma, encouraged first-time plasma donors to view regular donations as being easy, and allowed them to advance book multiple donations was shown to be effective at persuading individuals to return, to donate more frequently and to return more quickly. 33
Fear of blood draw can be associated with greater venepuncture pain, anxiety and vasovagal reactions, and venepuncture pain can be associated with a reduced likelihood of donor return. 34 Provision of a brochure containing tips on relaxation reduced pain and provided donors with a perception of positive support. Whole-blood donors who have had a negative experience (such as deferral or a vasovagal reaction) may respond well to being invited to convert to plasma donation instead. 18
Although it is usual to recruit plasma donors among whole-blood donors, there is evidence that offering new donors the option to donate plasma without a prior whole-blood donation can have a beneficial effect on the donor return rate and donation frequency. 35
flexible donors
To avoid shortages of blood products some blood collection services build a panel of donors that are flexible regarding which product they donate. 36 An exploratory study found that, regardless of their previous donation history, most donors were willing to consider changing their donation as needed by the blood collection service. 36 Donors requested that information about the different products and inventory levels should be available, and that advance warning and practical help with the logistics of switching between products should be provided. Another study found that new donors were more willing than experienced donors to be flexible. 37 Current whole-blood donors were concerned about the time commitment that would be required for plasma, while current plasma donors were concerned about the subsequent longer interval between plasma donations if they also provided whole-blood donations. This suggests that donors should be introduced to the concept of flexible donations early on in their donation history.
Non-Remunerated Versus Remunerated/Incentivized Donation
Although the WHO has set the target that all blood donations should be voluntary and non-remunerated, there is nonetheless considerable interest in offering incentives to increase recruitment and retention of donors. This is especially the case for plasma donation, because of the overall volume of plasma needed to meet current clinical needs, and because of the commitment required by donors in terms of the length of the procedure and the frequency of donations. 38 Whereas whole-blood donations may be made at a mobile unit, workplace or local facility, plasma donations can only take place at designated collection centres. This involves longer travel times and greater costs for many donors, in addition to the longer time needed to complete the donation compared with whole blood.
ethical considerations
Most blood and plasma donors are motivated by altruism (ie, a willingness to give something for the benefit of a stranger, with no benefit to oneself). Altruistic blood donation indicates respect for the need of others and the importance of life, which in turn engenders a sense of social responsibility and benefits the whole community.39,40 It also helps protect the poorest sector of society from exploitation, and may help ensure the safety of blood supplies, since payments could incentivize some people to hide relevant medical information such as infectious diseases.39,40 However, with regard to product safety, in the USA, where remuneration is allowed, there have been no reported cases of infectious diseases transmitted from plasma donors since the modifications of the Code of Federal Regulations requirements and adoption of the Plasma Protein Therapeutics Association IQPP standards. 41 Requirements for mandatory second donation, serology and nucleic acid testing for each donation, and the fractionation process used (which involves solvent detergent, nanofiltration and other processes), ensure plasma products are very safe, which helps to minimize any possible negative effect associated with paying donors. 41
Some countries currently rely in part on imported plasma, often from the USA. Many of these countries follow a non-remunerated policy internally. However, the increasing demand for plasma-derived products means that there is an increasing argument in favour of paid plasma donations, to ensure adequate supplies for the future.38,42
effect of remuneration
Unlike whole-blood donation, comparatively little is known about the effect of monetary incentives on plasma donations. In countries such as Germany and Austria where plasma donors are given financial compensation, it has been found that only 23–56% of donors who are currently paid would be willing to continue donating in the absence of remuneration.43,44 A study in Austria (where payment is made for plasma but not whole-blood donations), found that paid plasma donors had slightly lower altruism scores than non-paid whole-blood donors; however, a subset of plasma donors who expressed willingness to continue donating without compensation had similar altruism scores to the unpaid blood donors. 44
An individual's financial situation may determine their attitude to remuneration for plasma donations. Notably, a substantial increase in Google searches for paid plasma donation was seen in the USA (where donors can be paid) after the global economic crisis in 2007–2008. 45 Young adults may respond positively to payment for donations: when offered a choice between making whole-blood and plasma donations, only 3.9% of US university students expressed a preference for plasma; but, this increased to 47.7% when they were told that plasma donors could be paid. 46
However, while remuneration is an incentive for some donors, it can deter others. Among individuals who have a strong altruistic drive, or those who are motivated by gaining public recognition through being a donor, monetary reward can be perceived to reduce the status of donating, and thus can “crowd out” some potential donors. 40 There is evidence of a difference in attitude between the sexes, at least among whole-blood donors. A study in Sweden (where donations are not remunerated) found that introducing remuneration decreased the willingness of women to continue donating, but not men; however, when offered the option of donating the money to charity, women became more willing to donate again. 47
possible incentive-based strategies
An argument has been made that there is room for both paid and unpaid systems, thus covering a wider range of potential donors, including those motivated by remuneration, altruism, and other factors such as image/reputational concerns.38,48,49 It has also been suggested that an income-restricted system, whereby only those donors whose income falls below a specific threshold would be entitled to compensation for plasma donations, could help those whose economic situation leaves them little option but to seek payment if it is available. 50
A strategy of “double altruism” has also been proposed. In this scenario, payments are made for plasma donations, but people are offered the opportunity to transfer the payment to a charity/nongovernmental organization, thus encouraging donors who may wish to keep the payment as well as those who would prefer to donate the money. 40 A recent study found an increased willingness to donate plasma when “double altruism” was an option. 40
It is also worth noting that incentives need not be cash payments. 51 A common alternative is getting paid time off work. 48 Smaller incentives might include gift tokens or items such as T-shirts.48,51 However, one study found that although token non-cash incentives such as pens or badges were appreciated by plasma donors, many felt the money would be better invested into improving blood service operations. 12
Plasma Donation status Across European Countries
Most countries in Europe rely on voluntary non-remunerated plasma donations systems. Austria, the Czech Republic, Germany and Hungary have both paid and unpaid collection services, and these four countries currently collect >55% of plasma used for manufacturing plasma products in the EU.52,53 Currently, Europe is heavily reliant on imported plasma. In 2017, 38% of the plasma required for fractionation came from European public blood collection services, while 24% came from the private sector (predominantly from the four countries that allow donor payments) and the remaining 38% was imported, largely from the USA, a country that also allows donor payments. 41 Worldwide, 60% of plasma for fractionation originates in the USA. 41
Table 3 summarizes the current or recent status of plasma donation in the most highly populated Western European countries.54–60 In France, Germany, Italy, Spain, and the UK the donation system is voluntary non-remunerated, although monetary compensation is allowed in Germany. Globally the trend is to increase the frequency of donation and the quantity of donated plasma.
Summary of plasma donation status in selected European countries.

In France, Civilian and Armed Forces blood centres provide more than 99% of plasma used for patients in need. 54 Although France has not simplified plasma-related issues (it has several types of therapeutic plasma, with different statuses), the demand for therapeutic plasma at the earliest stages of healthcare intervention is increasing, and it is expected that the regulation will evolve to facilitate access to therapeutic plasma in an emergency. 54
In Germany, between 2006 and 2010, the number of new plasma donors increased by 23%, the number of repeat plasma donors increased by 41%, and the frequency of donations increased, especially among older donors. In 2010, 0.4% of people aged 18–68 years were repeat plasma or platelet donors, and plasma donors made an average of 12.5 donations/year. In 2017, 63.8% of plasma used for fractionation was collected by private centres.55,56
In Italy, the collection of plasma for fractionation increased by 3.8% between 2008 and 2017, and the quantity of plasma sent for fractionation increased by 2.1% in 2017 versus 2016. The plan for 2020 was to increase the quantity of plasma delivered for fractionation to 16–17 kg per 1000 population (compared to 13.7 kg per 1000 population in 2017), increase the plasmapheresis donation rate to 24 per 1000 population (compared to 8 per 1000 population in 2009), and increase the collection rate to 14.1 L per 1000 population.55,56
In contrast, in Spain the quantity of plasma obtained from whole blood donations decreased by 7938 L between 2012 and 2017, mainly due to a drop in whole blood donations. At the beginning of that period, multicomponent donation was more frequent in Spain than plasma donation (45% vs 28%, respectively). 61 However, the overall volume of plasma available to produce plasma derivatives remained stable across 2012–2017, even with an increase in the plasmapheresis programme (with 42,000 procedures performed in 2017). There was a projected need for an additional 117,968 plasmapheresis donations per year compared with 2017 to meet increasing plasma-derived medicinal product needs. 59
In the UK, blood plasma donation to manufacture medicines (immunoglobulin) has been authorized recently (April 2021), to increase the ability of NHS Blood and Transplant (NHSBT) to provide plasma at volume. 60 Prior to then, some plasma was already collected during whole blood donation. However, since 1999, the UK has imported plasma because of a ban on using plasma from UK donors, as a preventative measure against variant Creutzfeldt-Jakob disease. Each year, NHSBT collects around 350,000 L of plasma from blood donations, of which only 100,000 L are used for transfusion. The huge volume of 250 000 L plasma that was discarded will now be available to immunoglobulin manufacturers. 60
Plasma Donation During the COVID-19 Pandemic
Blood donations decreased in the early stages of the COVID-19 pandemic in many countries and have fluctuated since then.62–67 The reduction in donations was mitigated to an extent by a reduction in the demand for blood transfusions because of a decrease in elective surgical procedures, 62 but some shortages were reported. 67 Few data specifically about plasma donations have been published, and the effect on the supply of plasma for fractionation is unclear, although it is possible some centres may have reduced source plasma donations to focus their efforts on whole-blood donations. 62
A survey of seven European countries found that half of blood donors donated less than normal during the first 5 months of the pandemic. 68 Respondents generally perceived the risk of infection while donating to be low; those who perceived the risk as high were much less likely to donate, as were those who were most strongly adherent to COVID guidelines. A survey of German whole-blood donors during the first month of the pandemic found that 56.9% wanted to donate to help contribute to the fight against COVID-19. 69 Associations were found between donors’ intention to return and satisfaction with the donation experience, and how safe they felt. A Dutch study found that peaks in new blood/plasma donor registrations coincided with peaks in media attention about blood donation. 70 People at higher risk of contracting COVID-19, such as older individuals, were over-represented among new registrants; the number of new donors aged ≥55 was more than 7-fold higher in 2020 than in previous years.
Various measures have been implemented to increase the supply of fresh blood components, including public appeals to donate, ensuring people understand that blood donation is a permitted activity during lockdowns, and reassuring donors about the procedures being implemented to keep them safe during the donation process.62,63,71,72 This has involved national media campaigns using traditional or social media, contacting donors directly, or expanding blood drives in military and healthcare settings.62,63,65,71
Finally, COVID-19 convalescent plasma is being investigated as a treatment for the illness. A study of potentially suitable people in the UK found a low level of awareness of convalescent plasma. 73 Factors positively associated with intention to donate included a stronger sense of “altruism through adversity” and moral and civic duty, while generic fears about plasma donation were negatively related.
Conclusions
The increasing demand for plasma-derived medicinal products means that many countries need to recruit additional plasma donors. Understanding the characteristics and motivations of individuals who donate plasma is important, so that these factors can be taken into account when devising strategies to encourage new donors and maintain existing donors.
Available evidence suggests that key motivators for plasma donation include the benefit that donated plasma provides for other people, the sense that helping others is in their nature, a sense of pride at undertaking a special task, and the desire to achieve donation goals. The main reasons plasma donors stop donating are socioeconomic, relating to the time required and conflicts with work and other commitments. When asking donors to convert from whole blood to plasma donation, there is evidence that face-to-face requests may be more successful than leaflets or telephone/email requests, and that donors require clear information addressing health and safety concerns. However, telephone/email communication may be helpful for encouraging existing plasma donors to return for future donations or to donate more frequently.
With respect to safety, plasma donation is generally well tolerated by the donor, although additional long-term safety data would be helpful, particularly as donors could be asked to donate at shorter intervals in the future to help maintain supplies. Regarding the safety of plasma-derived products, current requirements for testing, and the methods used during the fractionation process, ensure plasma products are safe for recipients.
Most of the available data on characteristics and motivators among donors come from cohort studies rather than randomized controlled trials and studies have often been small. Studies also vary in terms of the populations that were enrolled and when and how they were surveyed. In particular, further work is needed to fully understand motivating factors in specific demographic groups. It is also important to bear in mind the cultural contexts in different countries when determining the most appropriate methods to encourage new and ongoing donors.
There is ongoing debate about the role of remunerated versus non-remunerated plasma donation. Many European countries currently rely in part on imported plasma, often from the USA, where payment is allowed, although many of these countries follow a non-remunerated policy internally. The increasing demand for plasma-derived products means that there is an increasing argument in favour of paid plasma donations in other countries, to ensure adequate supplies for the future. While there is evidence that remuneration is an incentive for some individuals, it may deter other people who have a strong altruistic drive. It has been suggested that a combination of paid and unpaid donation systems could cover a wider range of potential donors, and that non-monetary, rather than monetary, incentives may be appropriate for some people. Optimal strategies to support the supply of plasma for the future may need to be country-specific.
Footnotes
Acknowledgements
Writing and editorial assistance was provided by Content Ed Net (Madrid, Spain) with funding from Grifols (Barcelona, Spain).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the funding from Grifols (Barcelona, Spain).