
Abstract
There are multiple potential complications of eosinophilic esophagitis (EoE). These range from symptom-specific to disease-progression related, which result in fibrostenosis. Clinical manifestations of strictures and narrowing are further complicated by esophageal food impaction (EFI) and esophageal perforation, which can be spontaneous or iatrogenic. This life-threatening complication of EoE is rare and risk can be minimized with careful endoscopic technique during procedures to remove food impactions and during esophageal dilation. Complications of progression can be mitigated with effective EoE treatment and structured patient follow-up and monitoring. This paper reviews this spectrum of EoE complications and discusses assessment, management and prevention.
Introduction
Eosinophilic esophagitis (EoE) is an immune/allergic condition diagnosed with symptoms of esophageal dysfunction, eosinophilic infiltration of the esophageal wall of at least 15 eosinophils per high-power field (eos/hpf), and in the absence of competing causes of eosinophilia. 1 The incidence and prevalence have increased dramatically over the past two decades, and the disease is no longer considered to be rare, with an estimated prevalence of 1 in 700 individuals in the United States. 2 EoE is also a chronic disease, and while there are multiple effective therapies across dietary and pharmacology modalities, long-term treatment and monitoring are mandatory. 3 One of the main goals of managing EoE is to assess for and prevent complications. Complications can occur because of symptoms or features of the disease itself. For example quality of life is decreased in EoE, and adaptive eating behaviors, poor growth, malnutrition, and failure to thrive are also seen. 4 The progression of EoE (either before or after diagnosis) from an inflammatory-predominant to a fibrostenotic condition is also a major driver of complications. 5 This results in esophageal strictures and luminal narrowing which frequently require esophageal dilation, which in rare cases may cause esophageal injury or perforation. Fibrostenosis is also a driver of esophageal food bolus impaction (EFI). While this increases resource utilization, including visits to the emergency department and emergent performance of upper endoscopy, EFI can be a cause of Boerhaave’s syndrome as a complication of EoE, and endoscopy performed to treat EFI can also result in procedural complications, though fortunately these severe outcomes are not common. This paper will review this spectrum of EoE complications, and discuss assessment, management and prevention.
Complications Related to EoE Symptoms and Clinical Features
The common symptoms of EoE include dysphagia in adolescents and adults, and less specific symptoms such as abdominal pain, vomiting, and feeding dysfunction in children. However, either prior to or after diagnosis, severe symptoms can cause poor oral intake of food, leading to weight loss, impeded growth or failure to thrive (in children), and in some cases, malnutrition. These more severe symptoms may be seen in 10% to 20% of children, so while not frequent, they still represent a measurable proportion of patients.6-8 Notably, some children with EoE may require a feeding tube for enteral nutrition support or elemental formula treatment. While this can be considered a complication of severe EoE, it is also a procedure that can result in complications for patients with EoE. 9
Issues related to feeding, either food aversion because of symptoms, pain or discomfort with eating, or prior traumatic experiences with food impaction, can lead to avoidant-restrictive food intake disorder (ARFID) in EoE. 10 ARFID is disordered eating not explained by other causes which leads to failure to meet nutritional needs. In the study by Ketchem and colleagues, 4.5% of EoE patients were found to have restrictive eating behaviors consistent with ARFID and out of proportion to what would be expected with EoE. 10 While this is not common, it can complicate treatment assessment because symptoms and eating-related concerns can persist despite biologic disease control. Additionally, there is an increased burden of psychiatric conditions such as anxiety and depression in EoE, seen in up to a third of patients regardless of age. 11 It is possible, though not confirmed, that worry about adverse experiences related to eating may drive anxiety as a complication and comorbidity of EoE. Feeding dysfunction behaviors and overlapping ARFID or anxiety related to eating are important for providers to evaluate for and identify, as treatment will require a multidisciplinary team with expertise outside of gastroenterology and allergy.3,12
Disease Progression
The natural history of EoE is of a chronic, progressive condition. 5 Children with EoE do not “grow out” of EoE, 13 and it is felt to be a late stage of the atopic march. 14 Moreover, most, but not all, patients will progress from an inflammatory-predominant phenotype to a fibrostenotic phenotype (or a phenotype that mixes inflammatory and fibrotic features). This progression is supported by data from multiple centers around the world showing that the longer the symptom duration prior to diagnosis, the higher the proportion of patients with fibrostenosis at the time of diagnosis.15-18 For example, only 10% to 20% of patients with 1 to 2 years of symptoms prior to diagnosis may be found to have strictures whereas 80% or more may have strictures at presentation if they have a diagnostic delay of 20 years. 15 It is also estimated that rate of strictures increase by 9% for each year EoE goes undiagnosed, 17 with a doubling of risk every 10 years. 16 This is particularly notable as the average diagnostic delay for adults with EoE is 5 to 10 years and this does not appear to be decreasing over time. 19 In addition, data show that after diagnosis if patients have gaps in their care, the disease will also progress.20,21
The major clinical consequence of disease progression in EoE is the development of an esophageal stricture (a focal constriction of the esophagus) or more diffuse luminal narrowing (Figures 1A-C) which drive symptoms of dysphagia and adaptive eating behaviors, and result in EFI (as below) and need for esophageal dilation. A detailed discussion of esophageal dilation technique has been covered in recent guidelines from both the American College of Gastroenterology and the American Society for Gastrointestinal Endoscopy.3,12,22 This thoughtful and careful technique for dilation can prevent complications, as discussed below.
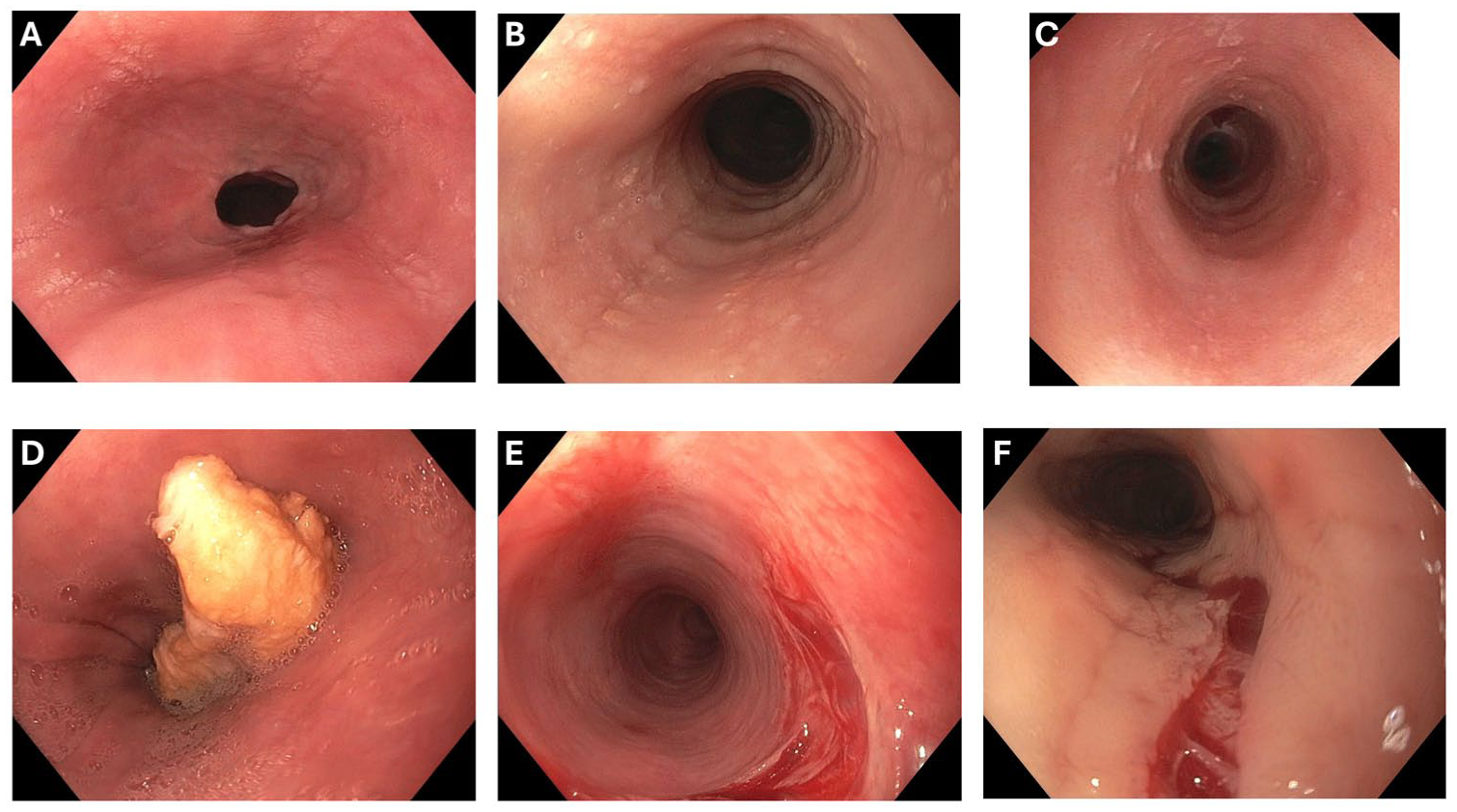
Endoscopic images from patients with EoE. The first three panels show fibrostenotic complications of disease progression: (A) a focal stricture at the gastroesophageal junction, with edema, exudates, and furrows also seen; (B) a narrowed and ringed esophagus (diameter approximately 12 mm), also with edema, exudates, and furrows present; (C) an extremely/severely narrowed esophagus (diameter approximately 6 mm) where the adult upper endoscope would not pass and a neonatal endoscope had to be used; edema, exudates, and rings are also seen; (D) an acute esophageal food impaction in a patient who will be newly diagnosed with EoE. The last two panels show appropriate “dilation effect” that is not a complication of EoE at (E) the level of the upper esophageal sphincter/high proximal esophagus in an area of subtle stricture, and (F) in the mid-esophagus in an area of narrowing.
Though EoE is chronic, to date it has not been associated with the development of esophageal cancer.23,24 This is somewhat counterintuitive as chronic inflammation in most other locations in the body and GI tract lead to the development of malignancy (for example reflux esophagitis leading to Barrett’s esophagus leading to esophageal adenocarcinoma). However, a systematic review the literature found no convincing data that atopic conditions such as eczema or asthma were associated with cancer, a similar finding to EoE, 24 and a case-control study using national claims data in the U.S. found no association between EoE and esophageal cancer, and the odds ratio was potentially in the protective range. 23 Additional studies also show that EoE does not lead to decreased lifespan or increased overall mortality. 25
Food Impaction
Esophageal food impaction is a common complication of EoE, with many patients experiencing short-lived or “transient” impactions that clear quickly, either spontaneously or with some maneuvers like positional changes or swallowing liquid. However, this is also a frequent initial presentation of EoE, with up to a third of patients with EoE being diagnosed in this manner (Figure 1D).26,27 However, food impaction is also the most common setting that EoE will be diagnosed. In fact, EoE is now the most common cause of the food impaction, and will be seen in more than half of patients presenting to the emergency department with EFI. 28 Recent prevalence estimates show that about 41/100 000 people in the U.S., or ~1 in 2400, will have an EFI, more than 134 000 annually. 29
Despite how commonly EoE is seen in patients with food impaction, this is also a time where the diagnosis can be missed. While it is a quality metric, guideline-recommended, and critical clinically to obtain esophageal biopsies to assess for EoE during esophagogastroduodenoscopies (EGDs) performed to treat EFIs, this is done far less than half the time in practice, as demonstraed in multiple studies.3,22,26,30 Not only does this preclude diagnosing EoE, but about half of patients who present with EFI are subsequently lost to follow-up, and the likelihood of this is increased if biopsies are not obtained. 31 Failure to obtain biopsies and loss to follow-up of EFI patients can in some respects be viewed as a complication of EoE, in that it leads to additional diagnostic delay, which increases the risk for disease progression. It has been confirmed, however, that obtaining esophageal biopsies during the EGD to remove a food bolus is safe, 32 and that simple quality-based measures can markedly raise the food impaction biopsy rate. 30 While it is out of the scope of this paper to fully review techniques for EFI removal, below we discuss best practices that can minimize complication risk during these procedures.
Esophageal Perforation
Esophageal perforation is a feared and life-threatening complication related to EoE. Fortunately, these are not common. While single center data have suggested that perforation is seen in ~2% of patients, national claims data finds perforation codes in only 0.5%.2,33 A systematic review found that for almost all patients, perforation was either prior to EoE diagnosis (~67%) or occurred in untreated patients (~18%). 34 There are two main ways for esophageal perforations to happen in EoE: either they are from EFI or they are iatrogenic. For food impaction, Boerhaave’s syndrome can occur due to a patient trying to induce vomiting after food becomes stuck or the food itself might perforate an already inflamed or injured esophagus.33,34 Iatrogenic perforation can occur during the endoscopy to treat EFI (usually during the course of trying to remove the impacted bolus) or it can occur as a result of esophageal dilation.33-36
Complications of dilation in EoE have been the best studied. In the “early years” of EoE, it appeared that esophageal perforation or injury (“rents”; “tears”) was common after dilation, seen in some series at up to 10%, and initial recommendations were to try to avoid dilation if possible. 37 However, as EoE became more recognized and dilation technique evolved, meta-analyses proved to be reassuring with a pooled rate of perforation of 0.033% (95% confidence interval: 0%-0.23%), which is not different from rates quoted for esophageal dilation risk in other non-EoE esophageal conditions.38,39 In addition to perforations, esophageal dissection, hematomas, intramural abscesses, and other injuries have been observed in EoE, but these are mostly confined to case-reports.40-43
Despite the relative rarity of esophageal perforation in EoE, it is still a serious problem that mandates prompt recognition and treatment, though management is similar in EoE to perforations of other causes. Consultation with thoracic surgery and chest imaging should be rapidly performed and a decision about operative vs non-operative management should be determined. For a frank transmural perforation with mediastinal contamination, a surgical approach is typically warranted. For a small leak, intramural injury, or a contained perforation, non-operative management with antibiotics, no oral intake status, and close observation may be considered. In certain cases, particularly with iatrogenic perforation without contamination, esophageal stenting could be considered. 36 However, careful attention must be paid to stent diameter in relation to estimated esophageal diameter. Patients with an extremely narrow caliber esophagus 44 may not be amenable to stenting, or may have additional esophageal injury if a too-large stent is placed. If surgery is performed in patients with esophageal perforation but without a known prior diagnosis of EoE, it would be ideal to obtain esophageal biopsies (either from a surgical approach or during an intraoperative endoscopy) to facilitate the diagnosis of EoE and to institute appropriate treatment in a timely fashion.
Prevention of Complications in EoE
Prevention of Disease Progression with Early Diagnosis and Treatment
There are several ways to prevent disease progression in EoE. First is early diagnosis. Though providers cannot control when a patient presents with symptoms (a patient coming to clinic for the first time with a history of dysphagia for 10 years cannot be diagnosed early), they can have a high suspicion for EoE across a range of patients. 28 EoE should be on the differential diagnosis for all esophageal symptoms across the lifespan, regardless of age, sex, or race/ethnicity.1,3 There are predictive calculators available for use if a provider is unsure of the risk clinically. 45 When endoscopy is performed, as per guidelines recommendations, it is critical to obtain at least six esophageal biopsies from multiple levels of the esophagus regardless of endoscopic appearance in order to maximize diagnostic sensitivity, especially because the esophagus can appear normal in some patients with EoE, especially children.3,12,22,46 Obtaining biopsies during EFI, as noted above, is also critical.
Once EoE is diagnosed, instituting effective treatment and monitoring for treatment response prevents progression to strictures and development of food impaction. Two studies in adults have shown that achieving histologic response decreases the need for future esophageal dilation, suggesting that control of inflammation prevents additional fibrosis.47,48 Two additional studies in children show that achieving initial histologic and endoscopic response also prevent development of newly identified strictures.49,50 Additionally, effective treatment has been shown to improve esophageal distensibility and decrease the occurrence of food impaction itself.51,52 These data, in addition to those from other studies, form the basis of guideline recommendation for maintenance therapy in EoE. 3
Prevention of Complications of Esophageal Dilation
To prevent complications during esophageal dilation, the recommended approach is to “start low and go slow.”22,53 This phrase represents a cautious approach, where the esophageal diameter is estimated, the endoscopist starts with a dilator size below that estimate, and then works upwards with increasing sizes, assessing the esophageal mucosa after each size, to determine if a “dilation effect” has been achieved. A dilation effect is the purposeful stretching of the esophagus, and is the preferred term (rather than “tear,” “laceration,” or “rent”) and goal of dilation (Figures 1E and F). 54 The dilation effect is not a complication, but it is a marker that the dilation session for that endoscopy has reached its goal. Because the esophageal mucosal in EoE is fragile and a tactile sense of resistance may not be present, the usual “rule of 3s” does not apply in EoE. Of note, data show that either balloons or bougies can be used safely in EoE, 38 so a dilator type can be selected based on stricture characteristics and endoscopist preferences. Guidelines recommend a goal dilation range of 16 to 18 mm in EoE in order to resolve dysphagia symptoms and prevent EFI, but this goal may take several EGD sessions to achieve.3,22 These endoscopies can also be used to assess and monitor treatment response.
Despite a careful approach, it is still possible to have an esophageal perforation related to dilation. This should be recognized immediately. One way to do this is to complete the dilation protocol, examine the dilation site, then take biopsies, then clean and re-examine the entire esophagus prior to ending the procedure to ensure no perforation has occurred. If a perforation is identified, management is similar to outlined above. However, this is a situation where stenting can be considered immediately to seal the leak, so it may be prudent to have a variety of stents on hand in units where dilation is performed.
Prevention of Complications During Endoscopy for Food Impaction
In order to prevent complications during endoscopy for EFI, the first step is to realize that this is a high-risk procedure in EoE and to set the stage for success. For the procedure, it is best to intubate patients to protect the airway and have them deeply sedated so they do not retch or vomit during the procedure, an event that has caused perforations. 34 Additionally, use of flexible endoscopes are preferred, as rigid scopes have previously been associated with complications. 35 For bolus removal, the preferred technique is to use a cap and suction. Here, a cap is affixed to the tip of the scope, as much of the bolus as possible is suctioned into the cap, and the entire scope with the bolus fixed in the cap is removed from the patient while holding suction. With this technique, a bolus can often be removed en-bloc. When selecting a cap size, consider the estimated esophageal diameter so as not to risk additional esophageal injury. The cap technique also tends to be more efficient than using forceps to grasp or pick apart the bolus. Nets can be used, but care must be taken to always visualize the tip and not deploy the net in a blind fashion, as this can perforate the esophageal wall. 33 The “push” technique is currently discouraged given how commonly EoE causes EFI. Because EoE will frequently cause strictures and narrowing, and because there is no way to visualize the esophagus distal to a bolus, a blind push could cause esophageal injury. There is a similar consideration with the use of overtubes. Because a patient is typically intubated for the procedure, an overtube is not needed for airway protection. The large caliber of the overtube may also cause esophageal injury, particularly if a decreased esophageal caliber is not recognized during the endoscopy. Finally, if a stricture is identified at the time of the EFI, it is preferred for dilation to be delayed. Because the food has typically been impacted for many hours and removal may be prolonged, the esophagus may be at an increased risk of injury from dilation. The recommended approach is to take biopsies and then bring the patient back at a future time for dilation.
Conclusions
As a chronic allergic disease, multiple complications can be seen in EoE. These range from symptom-specific, such as feeding difficulties leading to slow growth or malnutrition, as well as ARFID or anxiety, and disease-progression related, which are seen with diagnostic delay and untreated EoE. This latter category reflects fibrostenosis in EoE, clinically manifesting as strictures and narrowing, which is further complicated by esophageal food impaction and esophageal perforation, which can be spontaneous or iatrogenic. While this is a severe and life-threatening complication of EoE, it is rare and can be prevented with careful endoscopic technique during procedures performed for EFI and during esophageal dilation. Complications of progression can be mitigated with effective EoE treatment, both initially and maintained over the long-term, and with structured patient follow-up and monitoring. While recognizing complications in EoE is important, it is similarly important to understand what is not a complication. In particular, a purposeful “dilation effect” is not a complication. Additionally, there are yet no data linking EoE to progression to esophageal malignancy or early mortality. This perspective can be reassuring to patients and balance more concerning conversations about EoE chronicity, complications, and need to manage this lifelong disease.
Footnotes
Ethical Considerations
Ethical approval is not required for this manuscript.
Author Contributions
ESD wrote the paper.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported in part by NIH grant T35 DK007386.
Declaration of Conflicting Interests
The author declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr.Dellon reports research funding from: Adare/Ellodi, Allakos, Arena/Pfizer, AstraZeneca, Celldex, Dr. Falk Pharma, Eupraxia, Ferring, GSK, Meritage, Miraca, Nutricia, Celgene/Receptos/BMS, Regeneron, Revolo, Sanofi, Shire/Takeda, Uniquity; consulting fees from: Abbvie, Adare/Ellodi, Alfasigma, ALK, Allakos, Amgen, Anaptysbio, Apogee, Apollo, Aqilion, Arena/Pfizer, AstraZeneca, Bethanamist, Biocryst, Bryn, Calypso, Celgene/Receptos/BMS, Celldex, Cyted, Domain, EsoCap, Eupraxia, Dr. Falk Pharma, Ferring, GI Reviewers, GSK, Holoclara, Invea, Knightpoint, LucidDx, Nexstone Immunology/Uniquity, Nutricia, Parexel/Calyx, Phathom, Regeneron, Revolo, Robarts/Alimentiv, Roivant, Sanofi, Shire/Takeda, Target RWE, Third Harmonic Bio, Upstream Bio; and educational grants from: Allakos, Aqilion, Holoclara, Invea.
Use of Artificial Intelligence
No artificial intelligence (AI) was used in the preparation of this manuscript.