
Abstract
The upper esophageal sphincter (UES) is a 3 to 5 cm long multiplicitous high-pressure zone that connects the hypopharynx to the cervical esophagus. Due to its anatomic location between the arbitrary anatomic boundaries of numerous subspecialties, this region has often been referred to as “no man’s land.” Recent evidence confirming that the UES is not round suggests that conventional dilators designed to distend the cylindrical esophagus may be inappropriate to treat disorders of this region. This has led to the development of devices specifically designed to dilate the kidney shaped UES. The purpose of this manuscript is to review the anatomy and physiology of the UES, educate the reader on the most common indications for UES dilation, and describe the contemporary technique of state-of-the-art dilation of the UES with a novel device designed specifically to treat disorders of the pharyngo-esophageal segment.
Keywords
UES Anatomy and Terminology
The upper esophageal sphincter (UES) is a 3 to 5 cm long high-pressure zone that connects the hypopharynx to the cervical esophagus. Due to its anatomic location, this region has also been referred to as the pharyngo-esophageal segment or PES. The UES specifically refers to the intra-luminal high-pressure zone visualized on manometry (Figure 1). The PES refers to the anatomic components that make up the high-pressure zone (Figure 2). A more appropriate term for this region is the upper esophageal high-pressure zone (UEHPZ). Because this high-pressure zone exists between the arbitrary anatomic boundaries of numerous subspecialties, some clinicians have referred to this region of the foregut as “no man’s land.” 1
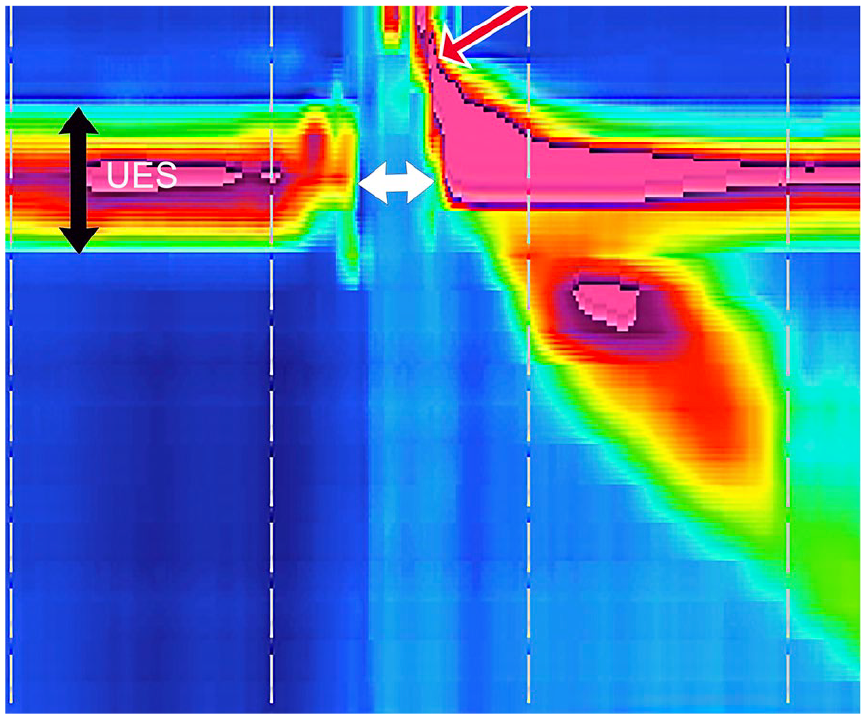
3 to 4 cm upper esophageal sphincter (UES) high-pressure zone visualized on high resolution manometry.
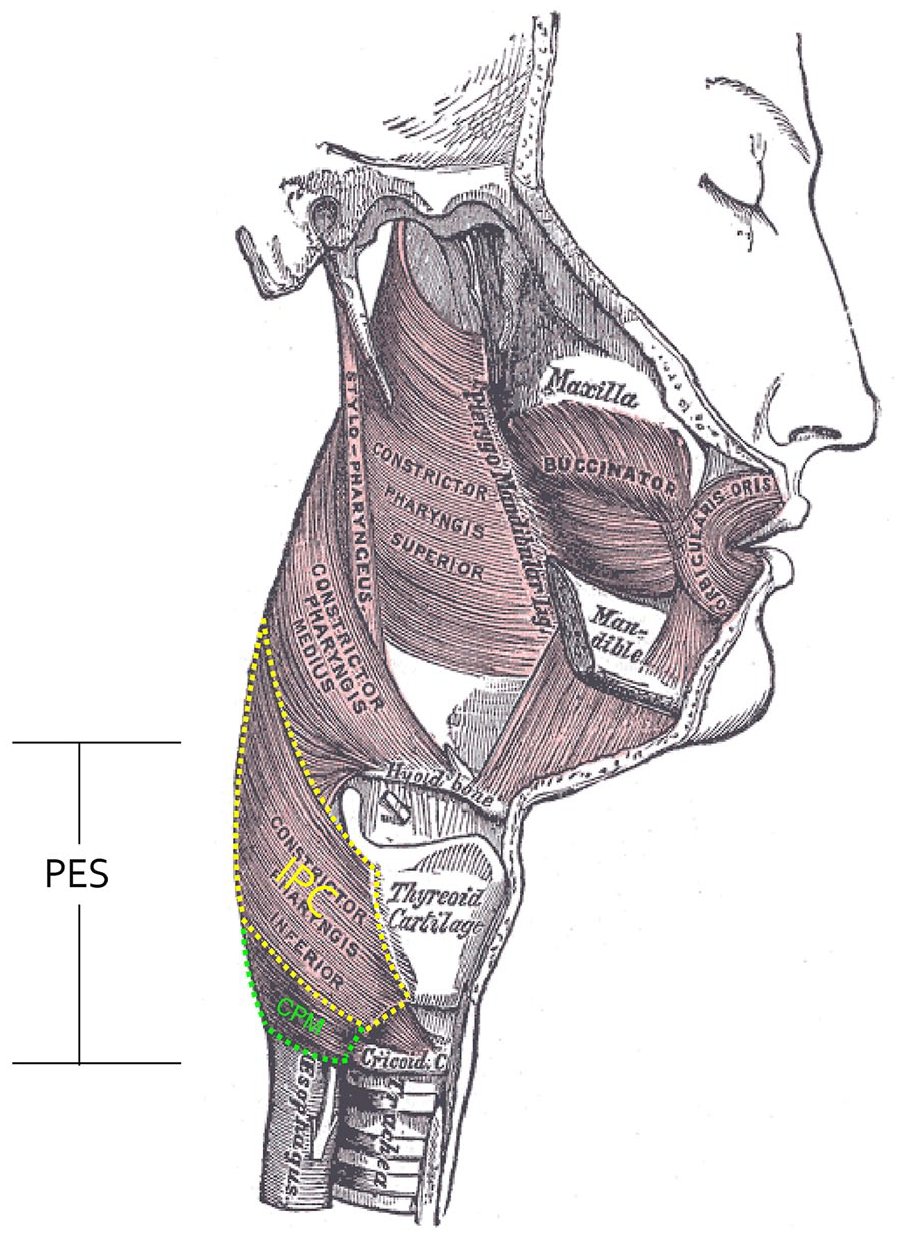
Drawing of the pharyngo-esophageal segment (PES).
The UES, PES, and UEHPZ are synonymous and may be used interchangeably. The cricopharyngeus muscle (CPM), however, makes up only the distal third of the high-pressure zone and is not synonymous with these terms. The 1 cm CPM muscle is the only true PES sphincter which is why UEHPZ is a more appropriate term for this 3 to 5 cm multiplicitous region. Because of its pervasiveness in contemporary medical literature, however, the term UES will be utilized throughout this manuscript. The UES is modifiable with behavioral therapy and surgery.2 -5 It is for this reason that the UES has captured the interest of innumerable dysphagia clinicians and surgeons alike.
The proximal two-thirds of the UES is made up of the elastic recoil of the laryngeal cartilage against the cervical spine. The distal one-third of UES pressure is comprised of the elastic recoil of the cricoid cartilage against the cervical spine and the baseline pressure generated by the cricopharyngeus muscle (CPM) which is tonically contracted at rest (Figure 3). The spacious pyriform recesses, bounded by the thyropharyngeus muscle, transition to the post-cricoid region at the level of the CPM. Recent evidence suggests that the narrowest cross-sectional dimension of the UES is not circular like the lumen of the esophagus but more closely approximates a kidney shape (Figures 4 and 5).6 -8 The shape of esophageal dilators has not deviated from a cylindrical shape since the first description of using a whalebone to dilate the esophagus of a patient with achalasia over 350 years ago. 9 Our contemporary understanding of pharyngo-esophageal anatomy has led to the development of dilators specifically tailored to distend the UES. These innovative UES-specific dilators have nearly twice the cross-sectional dimension of conventional esophageal dilators (38 mm or 114 French).
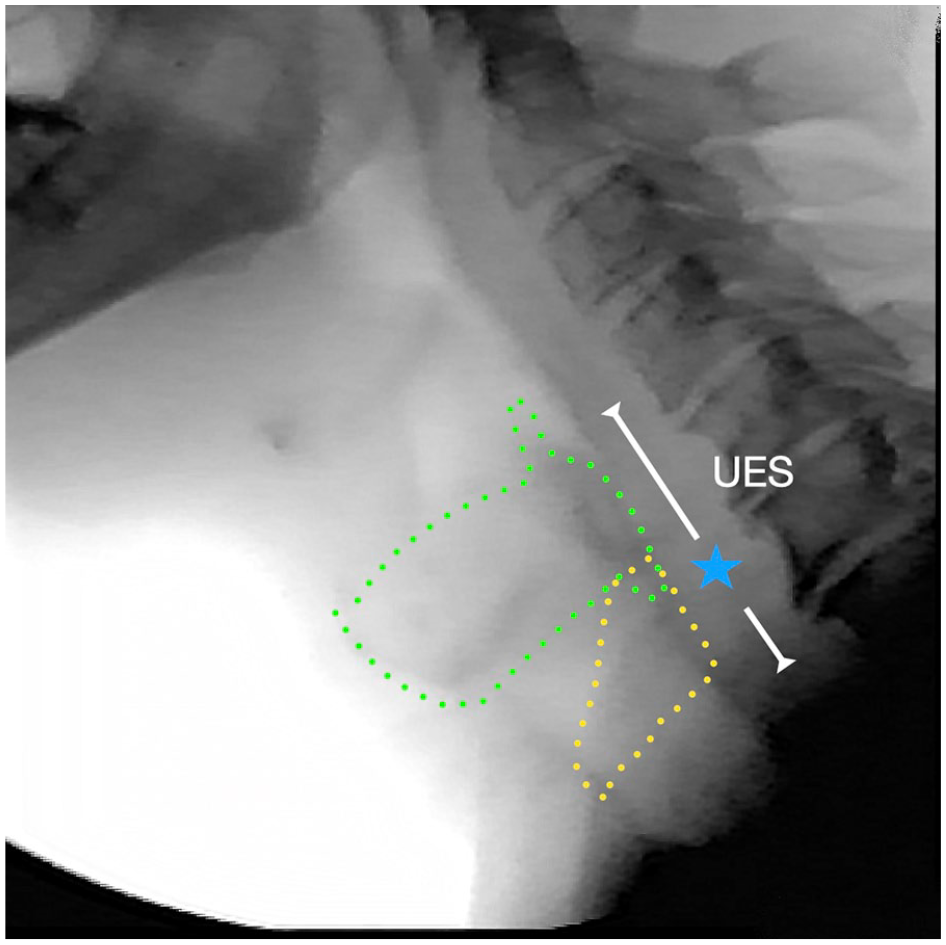
Lateral fluoroscopic image of the upper esophageal sphincter (UES). The proximal two-thirds of the UES is made up of the elastic recoil of the laryngeal cartilage against the spine. The distal one-third of UES pressure is comprised of the elastic recoil of the cricoid cartilage against the spine and the baseline pressure generated by the cricopharyngeus muscle (CPM). Green dots = outline of thyroid cartilage; Yellow dots = outline of cricoid cartilage; White line = upper esophageal sphincter; blue star = location of cricopharyngeus muscle.
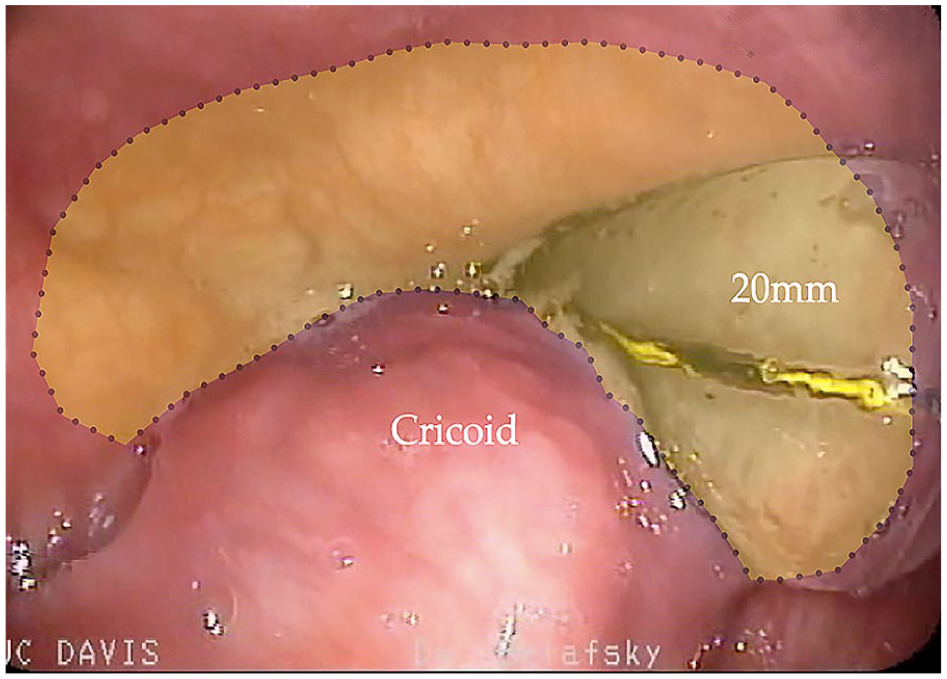
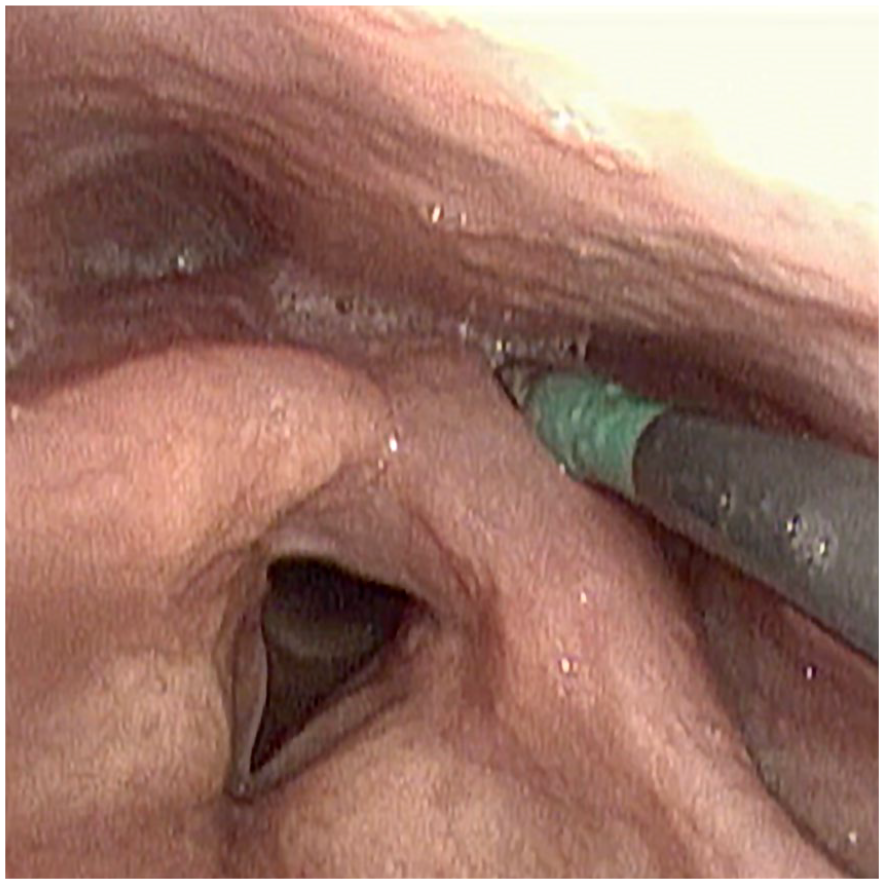
Endoscopic image displaying the kidney shape (yellow outline) of the upper esophageal sphincter (UES). 20 mm = 20 mm conventional controlled radial expansion esophageal dilator distending < half of the UES.
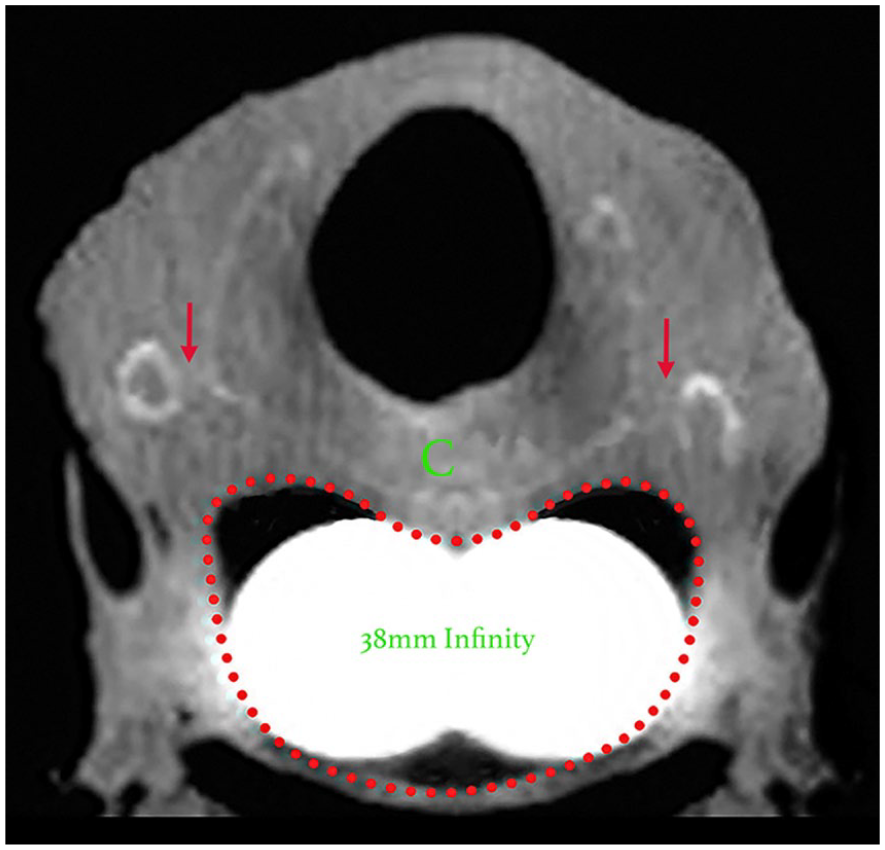
Transverse CT in a human cadaver through the narrowest region of the upper esophageal sphincter (UES) at the level of the crico-thyroid joint (red arrows). There is a 38 mm Infinity UES dilator distending the UES revealing its kidney shape (red dotted line).
UES Opening Mechanism
Opening of the UES depends upon muscular relaxation of the cricopharyngeus muscle, elevation of the laryngeal cartilages off the cervical spine, and intrabolus pressure generated by lingual and pharyngeal contraction. Cook et al 10 described 5 phases of UES opening (Figure 6). Phase I of UES relaxation involves the inhibition of tonic CPM contraction. During Phase I, the larynx remains low in the neck and the UES is closed (Figure 6I). Intrinsic CPM relaxation is followed by elevation of the hyoid and larynx (Phase II, Figure 6II). Hyolaryngeal excursion does not actually open the UES but primes the high-pressure zone for active distraction in Phase III. The amount of UES relaxation provided by laryngeal elevation appears to be more important to sphincteric opening than muscular inhibition, since the UES can open by active distraction without CPM relaxation, but CPM relaxation without elevation will not open the UES. This has significant clinical implications as swallowing in individuals with good hyolaryngeal elevation and lingual and pharyngeal contraction, but poor CPM relaxation is possible and often encountered (CP bar—Figure 7). Swallowing in individuals who can relax their CPM but cannot elevate their larynx and contract their tongue and pharynx has not been observed.
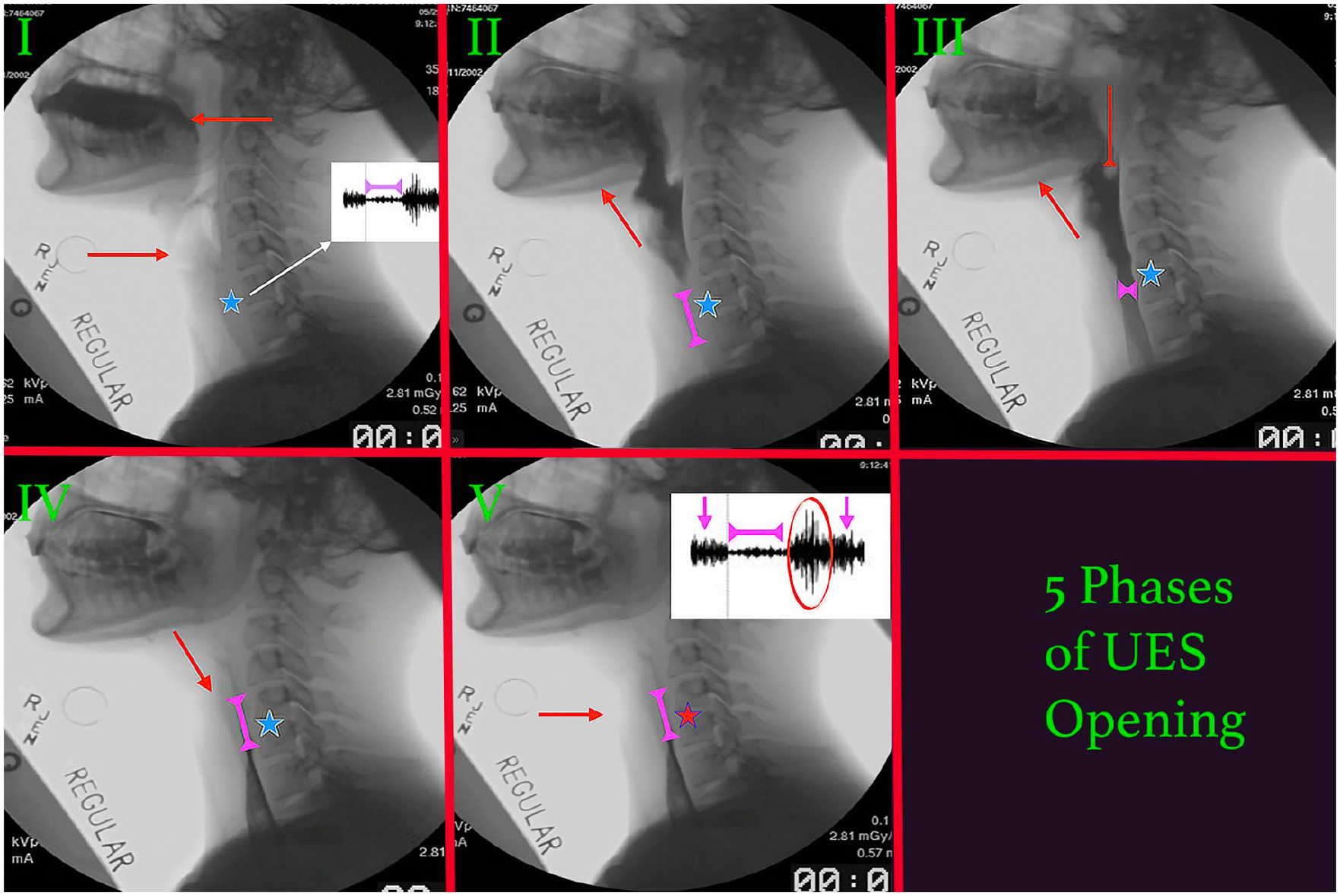
Five Phases of upper esophageal sphincter (UES) opening (I-V). Phase I) There is inhibition of tonic cricopharyngeus muscle (CPM—blue star) relaxation. The head of the bolus traverses the anterior faucial pillar (left facing red arrow). The larynx remains low in the neck (right facing red arrow) and the UES is closed. White inset shows CPM relaxation (magenta double arrow) on CP electromyography. Phase II) The hyoid and laryngeal cartilages elevate towards the mandible (red arrow) as the bolus enters the hypopharynx. The UES is primed but remains closed (double magenta arrow). The CPM remains intrinsically relaxed. Phase III) The laryngeal cartilages remain elevated (up facing red arrow) and the CPM remains intrinsically relaxed (blue star). The tongue and pharynx generate pressure on the bolus (intrabolus pressure; down facing red arrow) which opens the UES (double magenta arrow). Phase IV) The bolus traverses the UES and the laryngeal cartilages descend (red arrow). The CPM (blue star) remains intrinsically relaxed and the elastic recoil closes the UES behind the tail of the advancing bolus (double magenta arrow). Phase V) The laryngeal cartilages have returned to their resting position adjacent to the cervical spine (red arrow). The UES is closed (double magenta arrow). There is compensatory hyper-contraction of the CPM (red star). White inset displays this increased activity on CP EMG (red circle) with the electrical activity returning to baseline (downward facing magenta arrows).
Lateral fluoroscopic view displaying incomplete relaxation of the cricopharyngeus muscle (CP bar– red arrow) in a patient with inclusion body myositis. There is dilation of the hypopharynx above the UES obstruction (blue star).
Phase III of UES opening involves active distension of the laryngeal cartilages off the cervical spine (Figure 6III). This phase relies upon lingual and pharyngeal peristalsis to propel the bolus past the spacious hypopharynx, through the narrowed but expanding UES, and into the cervical esophagus. The elasticity of the UES allows it to be opened by the intrabolus pressure exerted by the advancing bolus. The UES will open as little as necessary to accommodate a bolus. The maximum extent of normal UES opening is dependent on bolus size and is currently uncertain. The herpetology literature contains numerous reports of various species of snakes swallowing whole prey that are greater than their own body weight (eg, a 32lb Burmese Python swallowing a small cattle). 11 Normal human UES opening on lateral fluoroscopic view with a 20cc barium bolus is approximately 1 cm.12,13 Most humans can swallow a 13 mm tablet without difficulty. Similarly, a normal sized Thompson Seedless grape (20 mm) can be swallowed whole by many individuals and competitive eaters have been known to swallow a hotdog (15 cm × 3.8 cm) in its entirety. The best estimate we have on the maximum capability of UES opening in humans is based on our ability to dilate the UES up to 160 French without trauma.14,15 This suggests that normal maximum UES opening in humans may be at least 40 mm and that the normal human UES may be able to accommodate passage of a walnut (3 cm × 2 cm) or even a golf ball (42 mm).
After the bolus passes into the cervical esophagus, the elasticity of the laryngeal cartilages causes a passive collapse of the UES (Phase IV) (Figure 6IV). Phase V involves UES closure through active compensatory hypercontraction of the CPM (Figure 6V).
Most Common Indications for UES Dilation
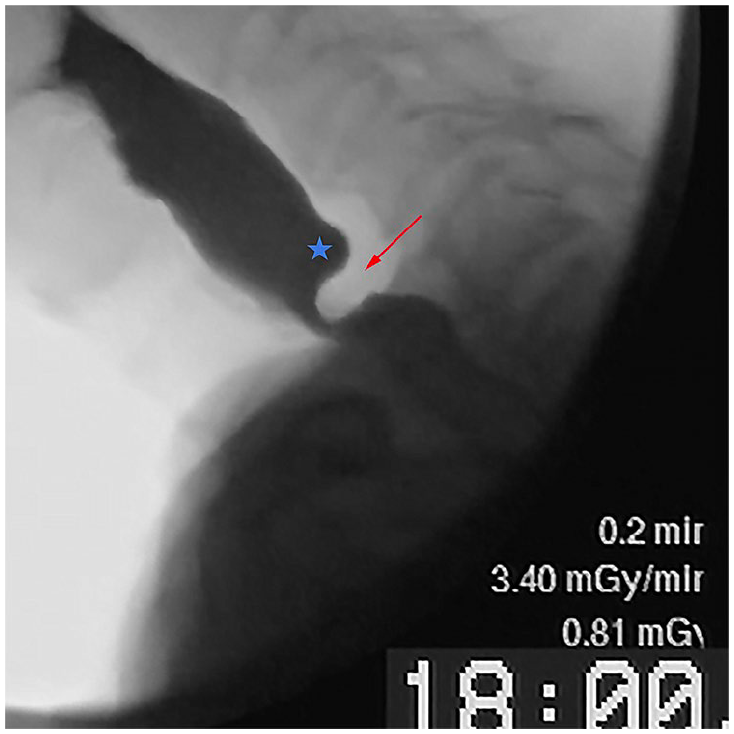
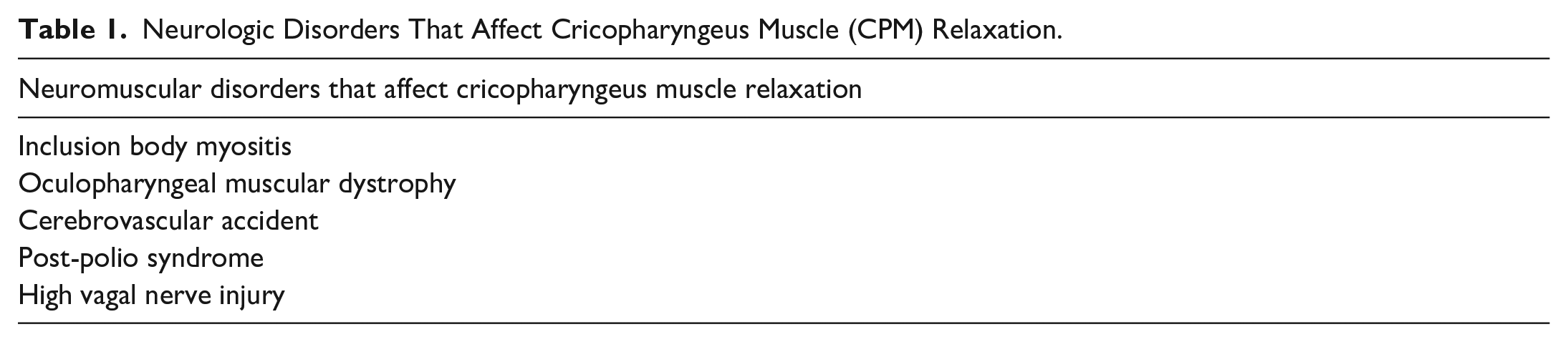
Any disorder that affects sphincter opening can cause UES dysfunction and swallowing impairment. Only disorders that narrow the actual lumen of the UES will respond to dilation. Disorders that predominantly affect laryngo-hyoid elevation (Phase II) and/or lingual and pharyngeal contractility (Phase III) are unlikely to improve with dilation. We refer to UES dysfunction caused by disordered luminal opening as pharyngo-esophageal segment outlet obstruction (PESOO) and differentiate PESOO from UES dysfunction caused by disordered laryngo-hyoid elevation and lingual and pharyngeal contraction. The most common causes of PESOO that improve with dilation are cricopharyngeal webs, neurological disorders of CPM relaxation (Table 1), radiation induced UES stenosis, and small Zenker diverticuli (Figure 8). Cricopharyngeal webs (CPWs) are extremely common and have been identified in nearly 70% of elderly cadavers. 16 These webs can be difficult to visualize on swallowing esophagography and flexible endoscopy. Many feel that the widely used term “non-obstructive dysphagia” is a misnomer, and that many individuals with CPWs are misclassified as having non-obstructive dysphagia (Figure 9).
Neurologic Disorders That Affect Cricopharyngeus Muscle (CPM) Relaxation.
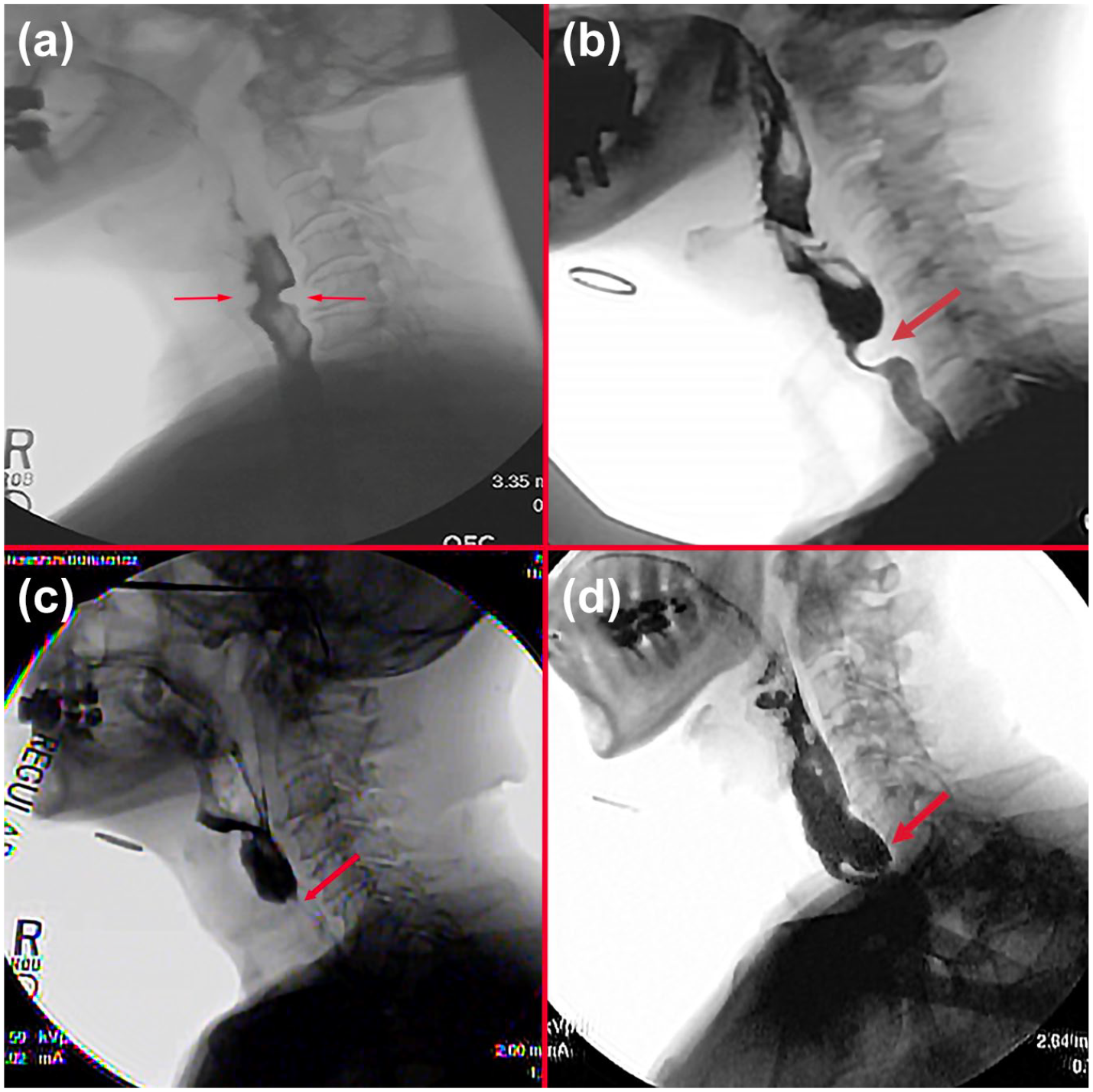
Most common causes of upper esophageal sphincter (UES) dysfunction that improve with dilation: (a) lateral fluoroscopic view of cricopharyngeal web (red arrows), (b) lateral fluoroscopic view showing poor relaxation of the cricopharyngeus muscle (red arrow) in a patient with oculopharyngeal muscular dystrophy, (c) lateral fluoroscopic view of a patient with radiation induced UES stenosis (red arrow), and (d) lateral fluoroscopic view of small (1 cm) Zenker diverticulum.
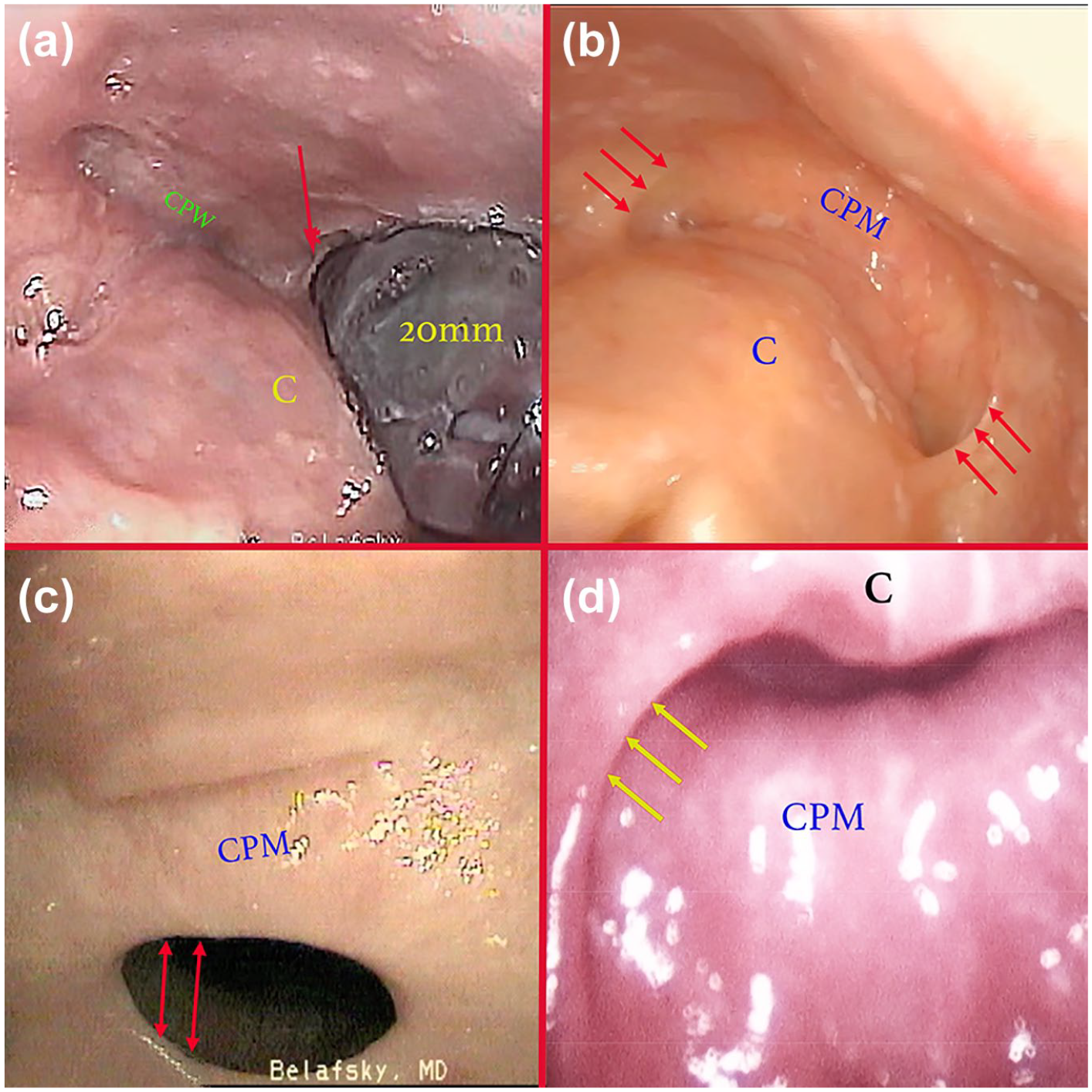
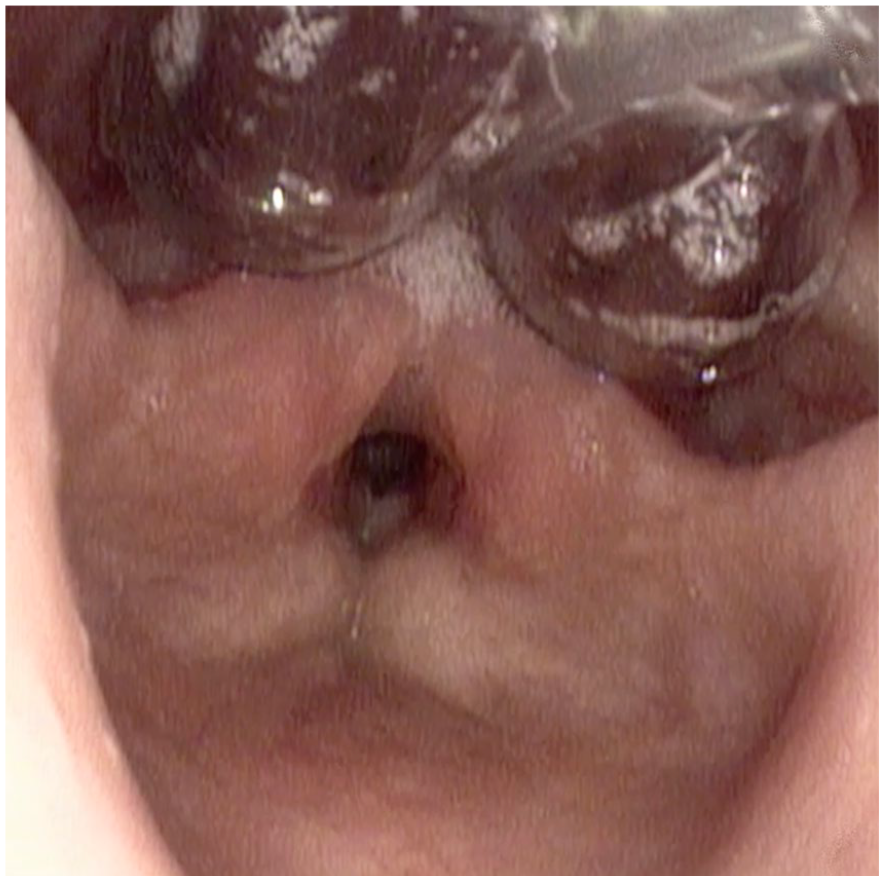
Endoscopic view of cricopharyngeal webs (CPWs). These webs are difficult to visualize on swallowing fluoroscopy and routine endoscopy. They become readily apparent once the upper esophageal sphincter (UES) is distended with a dilator or rigid laryngoscope. (a) Endoscopic image taken at the time of trans-nasal dilation of the UES with a 20 mm esophageal balloon showing a CPW. The web is obscuring nearly 50% of the UES and the 20 mm device is barely distending the UES (red arrow). C = back of cricoid. (b) Endoscopic image of a patient with UES stenosis from oropharynx radiation toxicity. This image was taken at the time of trans-nasal video laryngoscopy during a Valsalva maneuver. There are bilateral CPWs obscuring the lateral hypopharynx (red arrows). CPM = cricopharyngeus muscle; C = posterior lamina of cricoid cartilage. (c) Image of a large CPW taken during a burp at the time of trans-nasal endoscopy. The web is adherent to the cricopharyngeus muscle (CPM) and has reduced the lumen to approximately 8mm (red arrows). Dilation of the hypopharynx is seen posterior to the CPM. (d) Endoscopic image of the distal upper esophageal sphincter at the time of rigid endoscopy. The patient is supine and the laryngeal cartilages are distended anteriorly (C = cricoid cartilage). The cricopharyngeus muscle is in view posteriorly (CPM) and there is a large CPW (yellow arrows).
Technique of UES Dilation
Upper esophageal sphincter dilation is a common procedure which may be performed using a variety of devices and techniques. It may be performed via bougienage or using rigid or pneumatic dilators. It may be performed via trans-nasal or trans-oral routes, and under direct visualization, fluoroscopic guidance, or blind. It may be performed awake, under sedation, or general anesthesia. Maloney dilators have a tapered, weighted end and are passed blindly through the mouth. Savary dilators are similar but are passed through the mouth over a guidewire placed at the time of per oral endoscopy. We have been dilating the esophagus through the nose with controlled radial expansion balloons for nearly 2 decades. 17 The view afforded by the trans-nasal technique is unique and suggested that the UES is not round and that cylindrical dilators designed to dilate the esophageal body and LES are insufficient to distend this region (Figure 4). 14 Subsequent UES casting experiments in large animal and human cadavers confirmed that the narrowest segment through the UES is indeed kidney shape and dissimilar to the circular cross section of the esophagus6,7 (Figures 4 and 5). This led to the development of a UES-specific dilator that has a cross-section dimension that mimics the kidney-shaped UES (Figure 10).

Infinity 32 mm upper esophageal sphincter dilator (Hope Medical, Cincinnati, OH).
The Infinity UES Dilation System became commercially available in the Spring of 2023 (Hope Medical, Cincinnati, OH). Since this time, the majority of UES dilations at our institution have been performed with the Infinity system. The devices were designed to mimic the staged approach to lower esophageal sphincter dilation for achalasia and are available in small (23 mm), medium (32 mm), and large (38 mm) sizes. Evidence suggests that staged dilation with the Infinity system is safe, effective, and achieves dilation dimensions nearly twice that of conventional cylindrical esophageal devices.14,15 Achieving greater UES dimensions, however, does not necessarily equate to better outcomes, and there have been no published randomized trials comparing outcomes with the Infinity device to conventional esophageal dilators and/or surgical therapies (CP myotomy/myectomy). Although there is an ongoing clinical trial evaluating functional outcomes of the Infinity device (Allen et al., personal communication, 2024), there is no contemporary data comparing Infinity treatment efficacy to UES dilation with conventional esophageal dilators and further research is warranted.
Patients with severe UES obstruction typically get scheduled for a “series of 3” dilations separated by 3 to 4 weeks between procedures. Our series of 3 approach has been described previously and is modeled after the technique recommended for LES achalasia that is utilized to minimize perforation risk.14,18 We begin with a 23 mm Infinity balloon and then proceed to the 32 and then 38 mm device over the ensuing procedures (3 to 4 weeks apart). If patients have mild CP dysfunction (eg, small CPW), the initial dilation may be performed with the 32 mm balloon (Figure 14). If patients have profound UES stenosis (eg, severe radiation toxicity), initial dilation may be performed with a 10 to 20 mm maximum diameter conventional controlled radial expansion esophageal balloon (eg, Cook Hercules Esophageal Dilator, Cook Medical, Bloomington, IN) and then advanced to the 23, 32, and then 38 mm Infinity device. Because of the safety of UES dilation performed with radial expansion balloons over a guidewire and the significantly greater diameter that can be achieved with UES-specific devices, we no longer routinely perform UES dilation with rigid Savary-type dilators or flexibly Maloney-type bougies. The Infinity UES dilators are not appropriate for individuals after total laryngectomy. The neo-pharynx in laryngectomees is circular in diameter and only conventional cylindrical singleton dilators should be used in these individuals.
Our technique of UES dilation involves a “sidecar” approach performed via Seldinger technique over a guidewire (Table 2). The Infinity device is too large to fit through the port of a conventional gastroscope. The procedure is performed in the clinic without sedation, in the procedure suite with moderate sedation, or in the operating room under general anesthesia. Most otolaryngologist perform endoscopy and dilation with a small caliber esophagoscope passed through the nose (eg, Pentax EE-1580K 60 cm video esophagoscope, 5.1 mm OD, Pentax Medical, Montvale, NJ). Trans-nasal endoscopic visualization provides an unobstructed view of the UES, affords passage of the endoscope through tight stenoses (<6 mm), and allows the patient to be reclined on a gurney or seated upright in an examination chair in the anatomic position (Figure 10). Most gastroenterologists and general foregut surgeons perform UES dilation through the mouth with a conventional therapeutic gastroscope with the patient in the left lateral decubitus position (eg, Pentax EG29-i10 video endoscope, 9.8 mm OD, Pentax Medical, Montvale, NJ). Some otolaryngologists perform UES dilation under general anesthesia through the mouth with a rigid (Dedo Laryngoscope, Teleflex, Morrisville, NC) or video laryngoscope (GlideScope, Verathon, Bothell, WA) utilized to provide visualization (Figure 11).
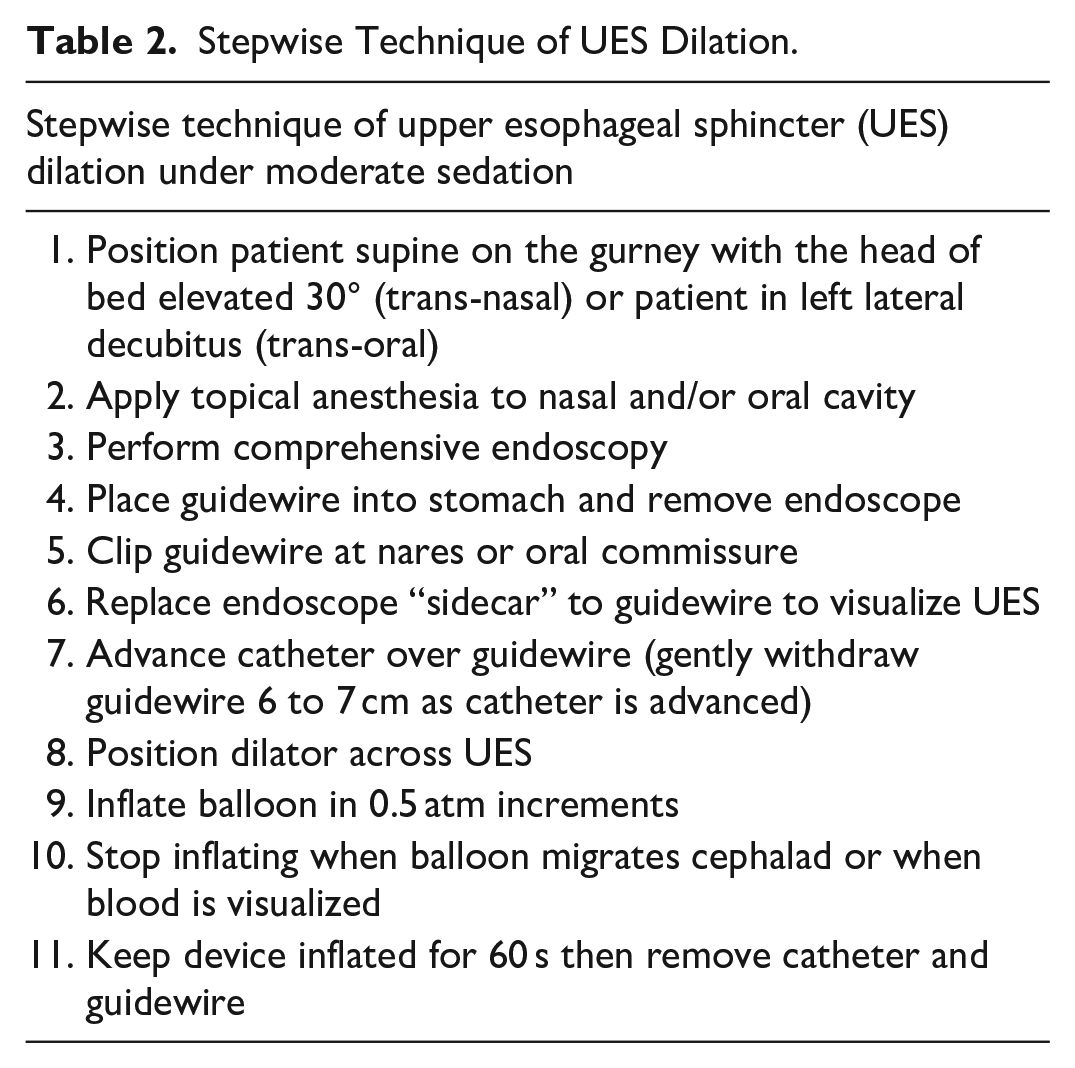
Stepwise Technique of UES Dilation.
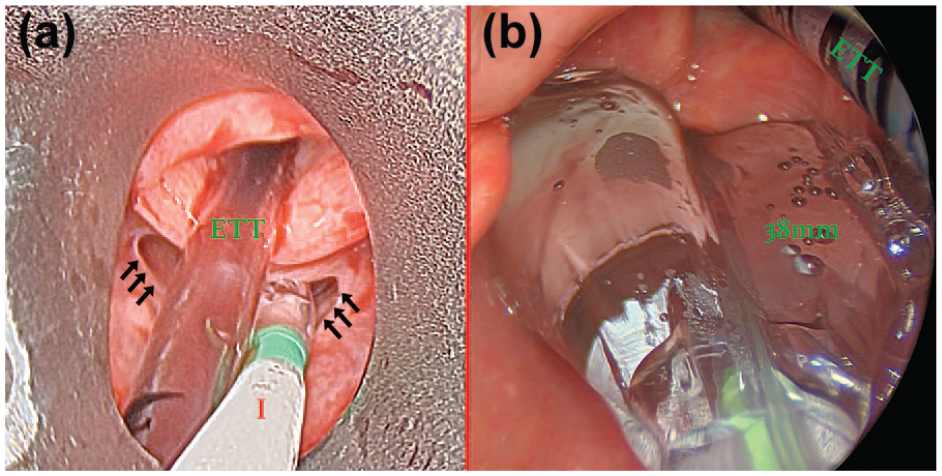
Upper esophageal sphincter (UES) dilation with the 38 mm Infinity UES Balloon through a per-oral rigid laryngoscope. (a) The endotracheal tube (ETT) is seen entering the larynx. The 38 mm Infinity balloon (I) is seen traversing the UES prior to inflation. There is a tight cricopharyngeal web (black arrows). (b) Inflation of the 38 mm Infinity balloon to 4 atm (38 mm).
We perform the majority of UES dilations in an outpatient endoscopy suite under moderate sedation which is achieved using a combination of fentanyl and midazolam. The patient is placed in a 30-degree reclined position on a hospital gurney (Figure 12). The nose is topically anesthetized and decongested. Comprehensive diagnostic esophagoscopy is performed through the more patent nares with a Pentax EE-1580K 60 cm (5.1 mm OD) video esophagoscope (Pentax Medical, Montvale, NJ, USA) or through the mouth with the patient on their side. Comorbid esophageal pathology is common in persons with UES dysfunction and must be evaluated prior to dilation. 19 A guidewire is placed through the endoscope into the stomach and the endoscope is withdrawn. If performed through the nose, the endoscope is then replaced through the contralateral nares and positioned “sidecar” with a view of the larynx and hypopharynx. The balloon is then passed over the guidewire and positioned to span the UES (Figure 13). Slowly withdrawing the guidewire 5 to 6 cm during balloon catheter advancement assists with the ease of device progression through the pharynx and keeps the guidewire from curling.

Patient position on gurney for trans-nasal UES dilation under moderate sedation.
38 mm upper esophageal sphincter (UES) Infinity balloon positioned in the UES prior to inflation.
UES dilation is performed under endoscopic visualization with slow 0.5atm increments on the manometric saline insufflator. If the balloon migrates proximally, the device is completely deflated and repositioned back within the UES. The device should not be advanced into the esophagus while inflated. Proximal migration indicates that maximum UES distension may have been achieved. Patience during dilation gives the device time to safely expand adherent or fibrotic tissue. Maximum inflation pressure is achieved when the balloon consistently migrates proximally (requiring deflation and repositioning), when any blood is visualized on the balloon or in the hypopharynx, or when maximum inflation pressure per manufacturer recommendation for the device is reached (4-5 atm). The balloon is kept at maximum inflation pressure for 60 s (Figure 14). The pressure on the manometer will go down as the tissue of the UES expands and more saline will need to be added to maintain the device at the maximum desired pressure.
Upper esophageal sphincter (UES) dilation of radiation induced UES stenosis with a 38 mm Infinity device performed through the nares.
Post-UES Dilation Care and Complications
Staged balloon dilation of the UES over a guidewire performed under moderate sedation is safe. Minor adverse events may occur in 9% of procedures. 15 They are transient (<3 days) and self-limited and include mild throat discomfort, worsening dysphagia, globus, nasal congestion, nausea or vomiting, and regurgitation. Major complications of esophageal dilation with a UES balloon are rare (<0.2%) and include perforation, hemorrhage, aspiration, and rarely death. In a cohort of 133 UES dilations performed with the Infinity device, there were no major complications. 15 Our recommendation is to withhold anticoagulants prior to UES dilation although we have periodically performed UES dilation and accepted an increased risk of hemorrhage in persons who could not come off these medications. Because of the reported safety of the staged approach, we do not routinely administer peri-operative antibiotics or obtain a post-procedure radiograph. Pain is minimal and typically controlled with liquid acetaminophen administered every 12 hours as needed for 3 days. The patient is discharged after a 30-min observation period from the recovery room. They are advised to have a protein shake or smoothie for their next 2 meals and are then advanced to their pre-procedure diet as tolerated. Each patient is called the following day by a registered nurse to ensure recovery.
If any danger signs of serious complication are noted after the procedure, the patient is kept nil by mouth and admitted for observation. Danger signs include severe throat or chest pain, severe worsening swallow function, bleeding, dyspnea, tachycardia, neck, or chest swelling or crepitation. A chest radiograph and ECG are obtained, and intravenous fluids and antibiotics are initiated. The patient is assumed to have a perforation and admitted for supportive care. Telemetry is considered for all patients and intensive care monitoring is reserved for patients suspected of having a cardiac complication and for those with hemodynamic compromise. Drying agents are considered to reduce saliva flow and infection risk (glycopyrolate 0.2 mg IV and transdermal scopolamine patch). We do not routinely pass a feeding tube or obtain a contrast swallow study or CT scan to confirm perforation. In our experience, these options hasten complication risk and recovery. If the patient has a pre-existing gastrostomy tube, tube feedings may be conservatively initiated if the patient is stable.
The patient is maintained on antibiotics, drying agents, IV fluids, and nil by mouth until all vital signs have normalized and pain and crepitance have resolved. After 3 days of stable symptoms and vital signs, a water-soluble contrast swallow study (eg, Gastrograffin or Visipaque) is obtained. If the water-soluble study is normal, barium is administered to confirm the absence of a leak. If the swallow study suggests a perforation, the patient is kept nil by mouth and the study is repeated every 3 to 5 days. Parenteral nutrition is considered. When this study is normal, the patient is placed on a clear liquid diet for 24 hrs and then discharged home on a puréed diet if doing well the following day. The patient is maintained on a puréed diet for 1 week, a soft diet for the second week, and instructed to return to their pre-procedure diet the following week. In our experience, we have not had to operate on these suspected or confirmed cases of perforation with the proposed observation and medical management strategy described herein.
Conclusions
The shape of esophageal dilators has not changed in over 350 years. Staged dilation of the UES performed over a guidewire with a UES-specific dilation system is safe and provides nearly twice the maximum dilation dimension as UES dilation with a single cylindrical conventional esophageal balloon or bougie.
Footnotes
Author Contributions
Dr. Belafsky conceived, composed, and edited the entire manuscript.
Use of Artificial Intelligence Statement
No artificial intelligence (AI) was utilized for the composition or editing of this manuscript.
Declaration of Conflicting Interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Conflict of Interest for Dr. Belafsky:
Co-founder Reflux Gourmet, LLC
Co-founder Hope Medical, Inc
Research Funding California Institute for Regenerative Medicine and Inovio Pharmaceuticals, Inc.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This was an invited manuscript based on literature review. No data was collected, and no ethics approval was required.