
Abstract
Objective:
We aimed to compare the outcomes of laparoscopic type IV hiatal hernia repairs in elective and emergent settings and assess the feasibility of same-day surgery (SDS) in elective repairs.
Methods:
SDS was defined as discharge on the day of the procedure. The feasibility of SDS in elective repairs was assessed.
Results:
There were 265 primary type IV hernia repairs: 208/265 (78.5%) elective versus 57/265 (21.5%) in emergent settings, age:70.0 (64.0-75.0) versus 73.0 (60.8-82.0), P = .059, BMI: 30.1 (26.6-33.8) versus 27.5 (24.4-32.4), P = .025, ASA IV: 5/208 (2.4%) versus 11/57 (19.3%), P < .001, LOS:1 (0-2) versus 2 (1-4), P < .001, 30-day mortality: 0/208 (0.0%) versus 2/57 (3.5%), P = .046. SDS was planned in 83/208 (39.9%) elective procedures and performed in 65/83 (78.3%); 18/83 (21.7%) were transitioned from SDS to observation/inpatient. NGT was attempted in 18/57 (31.6%) in emergent setting and was successful in 5/5 at the bedside and 11/13 (84.6%) endoscopically. Ischemia was seen in 4/57 (7.0%) in emergent settings and perforation in 1/4. Time from surgical consultation to arrival to the OR in patients without ischemia/perforation/obstructive gastric volvulus (n = 50) was 57.9 hours (44.0-79.7) versus 5.5 hours (4.1-8.9) in those with, (n = 7).
Conclusion:
Type IV hiatal hernia can be repaired laparoscopically with good outcomes in elective and emergent settings and as SDS in elective repairs. Emergent presentations can occur in about 20% of type IV hernias in older patients with lower BMI and higher ASA. Ischemia/perforation are rare. Emergent presentations without ischemia/perforation can be treated with gastric decompression and urgent repair during the same admission.
Learning Points
Our study compares outcomes of laparoscopic type IV hiatal hernia repairs in elective and emergent settings in a single center and shows that type IV hiatal hernia repairs can be performed laparoscopically and with good outcomes in elective and emergent settings and as same-day surgery in elective repairs.
Introduction
The outcomes of large hiatal hernia repairs in elective settings via a laparoscopic approach1,2 and in emergent settings via an open approach3,4 have been previously reported. A population-based analysis of a nationwide database of repairs of all types of paraesophageal hiatal hernias, including 7950 patients (24.6 % urgent/emergent repairs, 70 % completed laparoscopically vs 75.4% elective repairs, 90% performed laparoscopically), focused on assessing the feasibility of the laparoscopic approach and the need for fundoplication in emergent setting and identified laparoscopy as the standard approach in elective repairs. 5
Overall, the length of hospitalization for paraesophageal hiatal hernias repairs, including type IVs, has improved over time, from 7 days via a transthoracic approach in 1967, 6 4.5 days via an intrabdominal approach in 2004, 3 2 to 3 days via a laparoscopic approach in 2010, 2 to outpatient laparoscopic repairs in 2020 to 2023, as we previously reported.7,8 In a recent study of 518 primary and reoperative laparoscopic procedures which included 184/518 (35.5%) type IV hiatal hernias (elective and emergent repairs assessed as a group), we showed an increasing number of same-day surgeries with 77 primary elective type IV hiatal hernia repairs planned as same-day surgery and 68/77 (88.3%) performed as same-day surgery. 9
In the present study, we aimed to compare the outcomes of laparoscopic type IV hiatal hernia repairs in the elective and emergent settings in a single center and with the same surgical and anesthesia team. We assessed the clinical presentation, complications, treatment modalities in emergent settings, outcomes of repairs in patients with and without ischemia, the rate of symptomatic recurrence, and feasibility of same-day surgery in elective repairs. To our knowledge, no previous study has compared laparoscopic type IV hiatal hernias repairs in elective and emergent settings in a single center and assessed the feasibility of same-day surgery in elective repairs in a large cohort of type IV hiatal hernias.
Materials and Methods
A retrospective study of prospectively collected data of patients who underwent type IV hiatal hernia repair in elective setting versus emergent settings (presentation to the emergency department) from 01/20/2014 to 09/30/2022 at the McGovern Medical School at UTHealth, Esophageal Disease Center at Memorial Hermann Southeast, in Houston, Texas, was conducted. Type IV hiatal hernia was identified on imaging or intraoperatively when, in addition to the stomach, other organs such as the greater omentum, colon, small bowel, 10 and the tail of the pancreas herniated in the chest. Intrathoracic stomach was defined as 100% herniation of the stomach into the chest. GI radiologists measured the size of the hiatal hernia on the esophagram in the prone oblique position view.
Crural closure was performed in all patients and was reinforced by a biologic mesh in those with atrophic right curs or if the right or left crus were denuded of the peritoneal lining as the result of the excision of the hernia sac.
Fundopexy was performed by placing interrupted stitches, starting right below the gastroesophageal junction, on the entire fundus at the level of the divided short gastric vessels. The stitches were placed between the stomach and the left lower-lateral hemidiaphragm and the left upper-lateral abdominal wall to maintain the longest intra-abdominal esophageal length in place and to anchor the entire fundus and the upper body of the stomach into the abdomen to prevent recurrence. At present, we perform fundopexy in all type IV hiatal hernias. The outcomes of Toupet fundoplication versus fundopexy in primary laparoscopic hiatal hernia repair at our center were previously reported. 11
A single surgical and anesthesia team performed all procedures, and a trained team of thoracic nurses provided postoperative care.
Same-day surgery was defined as discharge on the day of surgery, observation as <24-hour hospital stay (1-night hospitalization), and inpatient as ≥2-night hospitalization. An ERAS protocol with a series of measures in perioperative phases, as previously reported,7,8 was applied to achieve same-day-surgery in elective repairs.
The clinical characteristics and outcomes of patients who underwent elective type IV hernia repairs (elective setting) were compared to type IV hiatal hernia repairs in patients who presented to the emergency department (emergent setting). Outcomes were assessed by perioperative complications, length of stay, same-day surgeries in the elective setting, 30-day mortality, and postoperative emergency department (ED) visits and readmissions. Patients with ischemia were compared to patients without ischemia.
Patients’ characteristics and perioperative data were extracted from electronic health records. The study was approved by the institutional review board at UTHealth and Memorial Hermann system.
Statistical Analysis
Clinical data and outcomes were entered into the Microsoft Office Excel program. Descriptive statistics were provided in all the tables. Frequencies and percentages were used to describe the categorical variables, while median and interquartile range (IQR) were used to describe the continuous variables. Categorical variables are compared between groups using a Chi-square test or Fisher’s exact test for smaller-sized samples. Continuous variables are compared between groups by either an independent t-test or a Wilcoxon Rank Sum test based on normality assumptions. The level of significance was set at P < .050. Statistical analyses were performed using MATLAB (The MathWorks Inc. 2022. MATLAB version: 9.13.0 [R2022b], Natick, Massachusetts: The MathWorks Inc).
Results
From 01/20/2014 to 9/30/2022, there were 776 hiatal hernia repairs at our center. The reoperative repairs (n = 166) and hernia types I-III (n = 345) were excluded, and 265/776 (34.1%) patients who underwent primary type IV hernia repairs were included in the study.
Herniation of the stomach and the greater omentum in the chest was seen in all patients. Herniation of the stomach and only the greater omentum was seen in 249/265 (94.0%), and herniation of the stomach, the greater omentum, and solid organs were seen in 16/265 (6.0%): herniated colon in 16/16 (100.0%), small bowel in 6/16 (37.5%), and the tail of the pancreas in 1/16 (6.3%).
Comparing patients with herniation of the stomach and only the greater omentum to those with herniation of the stomach, the greater omentum and other organs showed, age: 70.0 (63.8-76.0) versus 72.0 (65.5-91.0), P = .218, sex: female: 191/249 (76.7%) versus 13/16 (81.2%), P = 1.000, male: 58/249 (23.3%) versus 3/16 (18.8%), P = 1.000, BMI: 29.9 (26.2-33.4) versus 25.9 (24.8-33.0), P = .304, ASA: III (II-III) versus III (III-III), P = .039, duration of operation: 124.0 (103.0-147.0) versus 191.0 (149.5-221.0), P < .001, elective procedures: 201/249 (80.7%) versus 7/16 (43.8%), P = .002, emergent setting: 48/249 (19.3%) versus 9/16 (56.2%), P = .002, length of stay: 1.0 (0.0-2.0) versus 2.5 (1.5-8.0), P = .003, SDS number in elective procedures: 63/201 (31.3%) versus 1/7 (14.3%), P = .442, need for ED visits after discharge : 31/249 (12.4%) versus 1/16 (6.3%), P = .702, readmission: 17/249 (6.8%) versus 1/16 (6.3%), P = 1.000, mortality: 1/249 (0.4%) versus 1/16 (6.3%), P = .117.
Overall, there were 208/265 (78.5%) elective repairs and 57/265 (21.5%) repairs following presentation to the emergency department (emergent setting).
Comparing repairs in elective versus emergent settings showed that patients in emergent settings tend to be older: 70.0 (64.0-75.0) versus 73.0 (60.8-82.0), P = .059, had lower BMI: 30.1 (26.6-33.8) versus 27.5 (24.4-32.4), P = .025 and higher ASA IV: 5/208 (2.4%) versus 11/57 (19.3%), P < .001. The most common presenting symptoms in the elective setting were regurgitation in 159/208 (76.4%), dysphagia in 157/208 (75.5%), and heartburn in 109/208 (52.4%) versus upper GI bleeding in 33/57 (57.9%), abdominal pain in 25/57 (43.9%), and nausea/vomiting in 18/57 (31.6%) in the emergent setting. Demographics, hiatal hernia characteristics, presenting symptoms, and endoscopic findings are shown in Table 1.
Demographics, Hiatal Hernia Characteristics, Presenting Symptoms, and Endoscopic Findings in Elective Versus Emergent Setting.
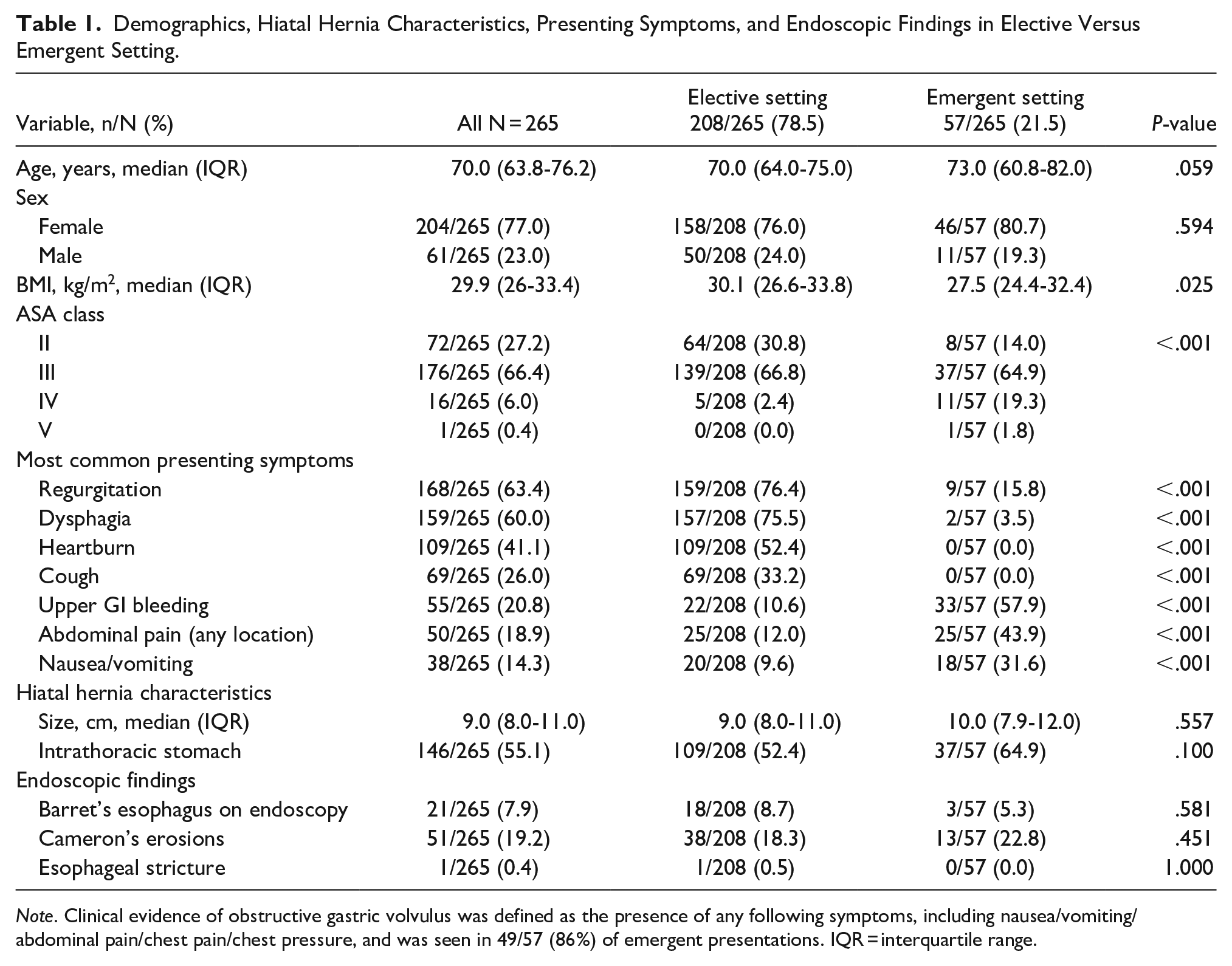
Note. Clinical evidence of obstructive gastric volvulus was defined as the presence of any following symptoms, including nausea/vomiting/ abdominal pain/chest pain/chest pressure, and was seen in 49/57 (86%) of emergent presentations. IQR = interquartile range.
All elective and 55/57 (96.5%) repairs in an emergent setting were performed laparoscopically. Tension-free intra-abdominal esophageal length was achieved in all without the need for Collis gastroplasty.
Two procedures that were not performed laparoscopically had herniation of the stomach and the greater omentum only. One was a conversion in the emergent setting in a patient who had previously undergone a left thoracotomy and excision of a distal esophageal leiomyoma. There were extensive upper abdominal and mediastinal adhesions that required conversion to laparotomy. The other one was performed via laparotomy in the emergent setting in a hemodynamically unstable patient with suspicion of ischemia, which was confirmed intraoperatively.
The type of procedures, operative data, type of anesthesia, and type of hospitalization in patients who underwent repairs in elective versus emergent settings are shown in Table 2.
Procedures, Operative Data, Type of Anesthesia, and Hospitalization in Elective Versus Emergent Setting.
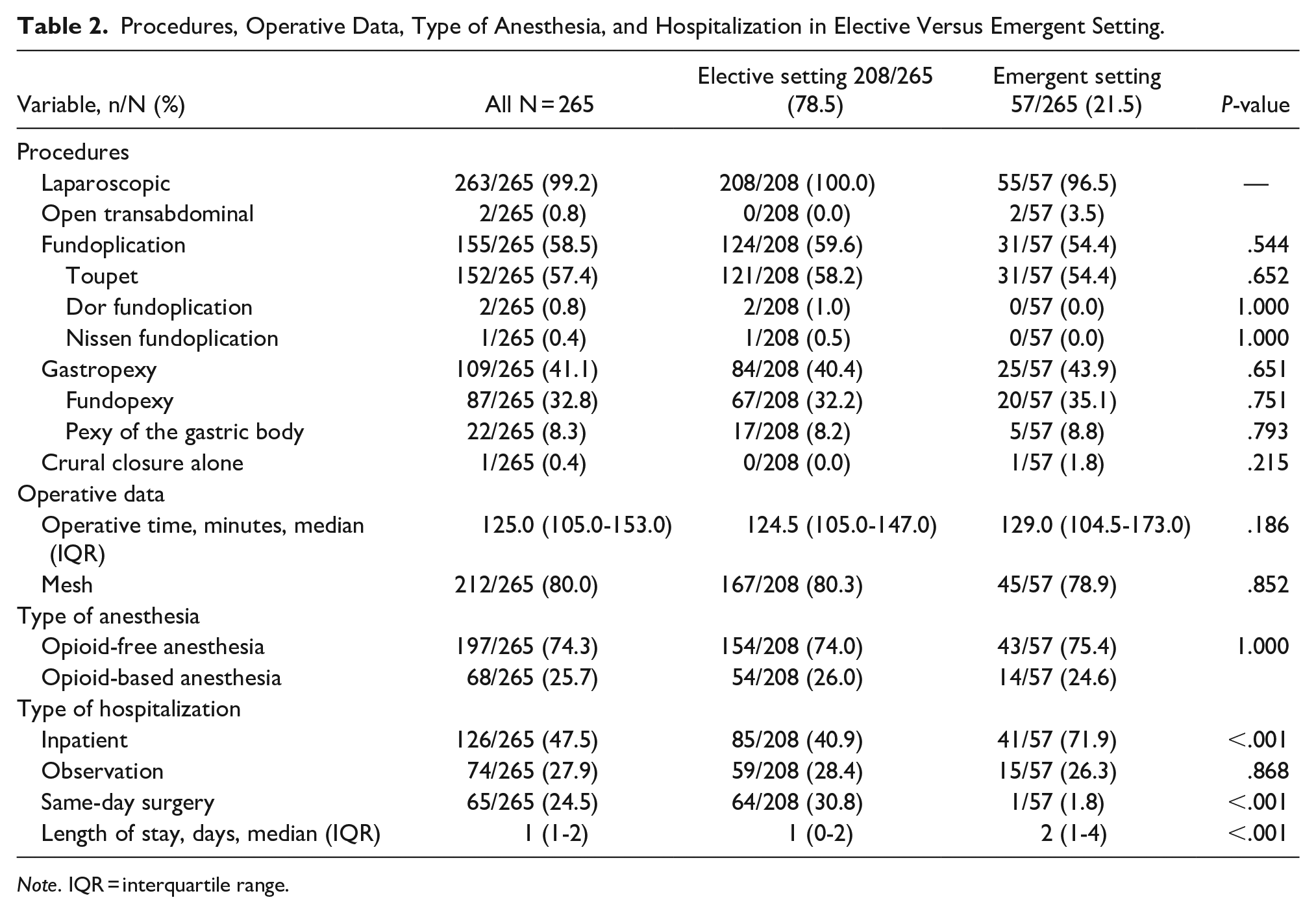
Note. IQR = interquartile range.
Same-day surgery was planned in 83/208 (39.9%) elective repairs and was performed in 65/83 (78.3%). Demographics, hiatal hernia characteristics, procedures, operative data, and type of anesthesia in patients who underwent elective procedures planned as same-day surgery and were performed versus not performed as same-day surgery are shown in Table 3.
Demographics, Hiatal Hernia Characteristics, Procedures, and Operative Data and Types of Anesthesia in Patients Who Underwent Elective Procedures Planned as Same-Day Surgery (SDS) and Performed Versus Not Performed as SDS.
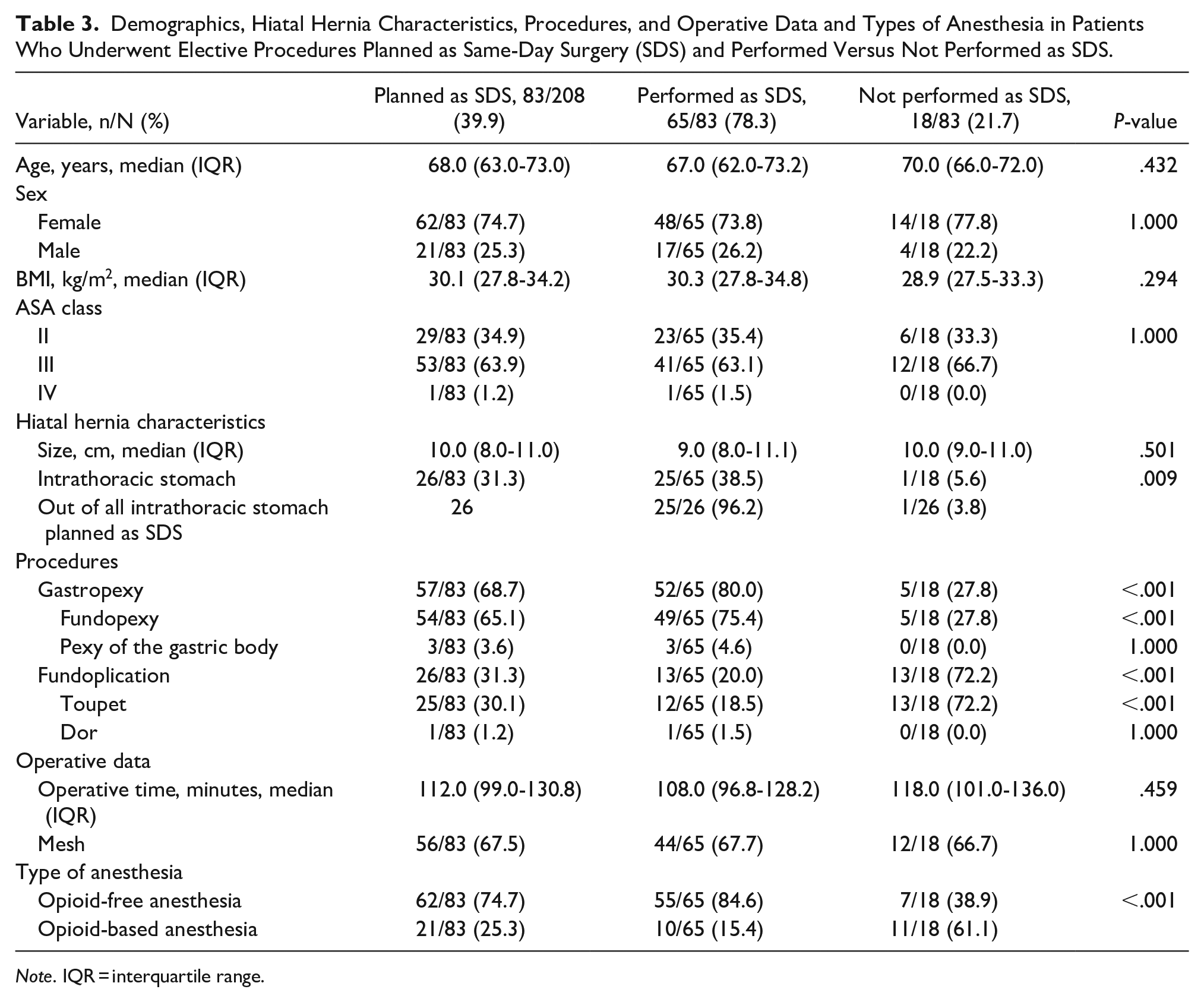
Note. IQR = interquartile range.
Overall, in-hospital complications were comparable between the procedures in elective and emergent settings. There was 1 gastric leak in an 80-year-old female with an intrathoracic stomach who underwent an elective laparoscopic Toupet fundoplication and required take back for laparoscopic repair of gastric leak on POD 7. She was discharged on POD 6 after the second procedure. In-hospital reoperation was required in 4/265 (1.5%) patients and included 2 laparoscopic removals of retained Penrose, 1 VATS evacuation of hematoma, and 1 laparoscopic repair of gastric leak.
One patient who underwent a laparoscopic repair with fundopexy in the emergent setting and was discharged on POD 1 presented with post-operative dysphagia and underwent EGD with dilation on POD 20. Following dilation, she presented with severe abdominal pain. CT scan showed a large left-sided intrabdominal hematoma. She underwent laparoscopic evacuation of hematoma and was discharged on POD 3.
Thirty-day mortality was seen in 2/57 (3.5%) in emergent setting: 1 in a 90-year-old female who developed fulminant Heparin-induced thrombocytopenia and died on POD 10 despite emergent thrombectomy and 1 in an 85-year-old female who was readmitted with hypotension and ground level fall on POD 5 following hernia repair and died on POD 6. The second mortality did not seem to be directly related to our procedure, but her ultimate cause of death was declared as myocardial infarction.
Symptomatic recurrence requiring reoperation occurred in 13/265 (4.9%) at a median time of 24.0 months (11.8-35.8), 1/13 who underwent elective repair with Toupet fundoplication and mesh, was discharged on POD 2, and was readmitted on POD 3 with acute onset of chest pain and shortness of breath. She was found to have a recurrent hiatal hernia with an intrathoracic stomach. She underwent laparoscopic repair of a torn crura with primary closure and mesh reinforcement. She was discharged on POD 5 after the reoperative repair.
There was no difference in symptomatic recurrence in elective and emergent settings. In patients with Toupet fundoplication, symptomatic recurrence requiring reoperation was seen in 10/152 (6.6%) versus 1/87 (1.1%) in patients with fundopexy, P = .060.
Postoperative in-hospital complications and symptomatic recurrence requiring reoperation in elective versus emergent settings are shown in Table 4.
Postoperative In-Hospital Complications and Symptomatic Recurrence Requiring Reoperation in Patients in Elective Versus Emergent Setting.
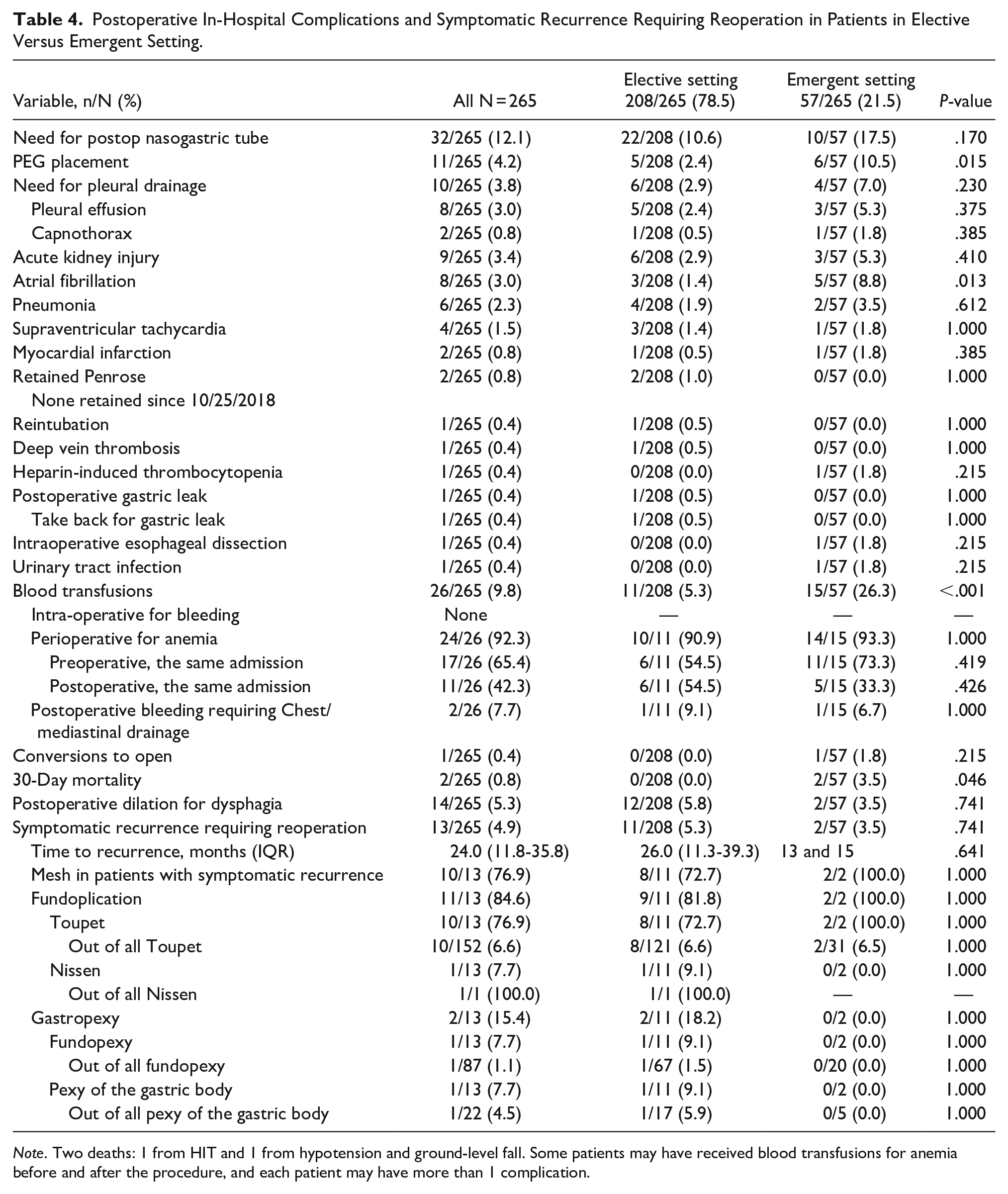
Note. Two deaths: 1 from HIT and 1 from hypotension and ground-level fall. Some patients may have received blood transfusions for anemia before and after the procedure, and each patient may have more than 1 complication.
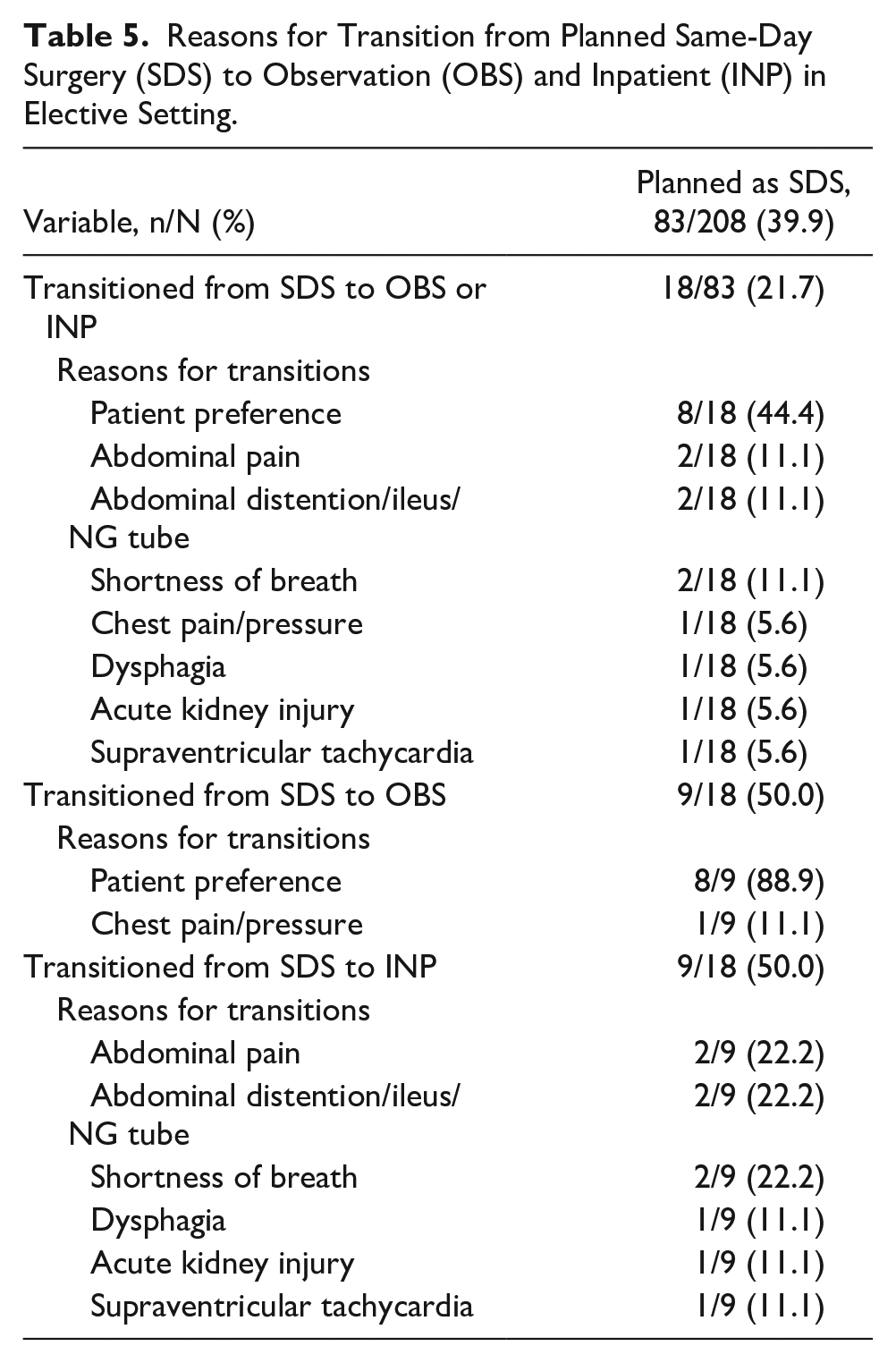
Transitions from same-day surgery to observation or inpatient occurred in 18/83 (21.7%) patients who were planned as same-day surgery. Reasons for the transition from planned same-day surgery to observation/inpatient status in patients who underwent elective repairs are shown in Table 5.
Reasons for Transition from Planned Same-Day Surgery (SDS) to Observation (OBS) and Inpatient (INP) in Elective Setting.
Emergency department visits after discharge were required in 7/65 (10.8%) of patients in the elective setting who had their procedures performed as same-day surgery. Reasons for emergency department visits after discharge in patients who had their procedures as same-day surgery versus those who did not are shown in Table 6. In the same-day surgery group, there was no difference in demographics, symptoms, hiatal hernia characteristics, type of procedures, and operative data between patients who had emergency department visits post-discharge versus those who did not (data not shown).
Emergency Department (ED) Visits Following Discharge and Readmissions in Patients in Elective Setting Whose Procedures Were Performed as Same-Day Surgery (SDS) Versus Not Performed as Same-Day Surgery.
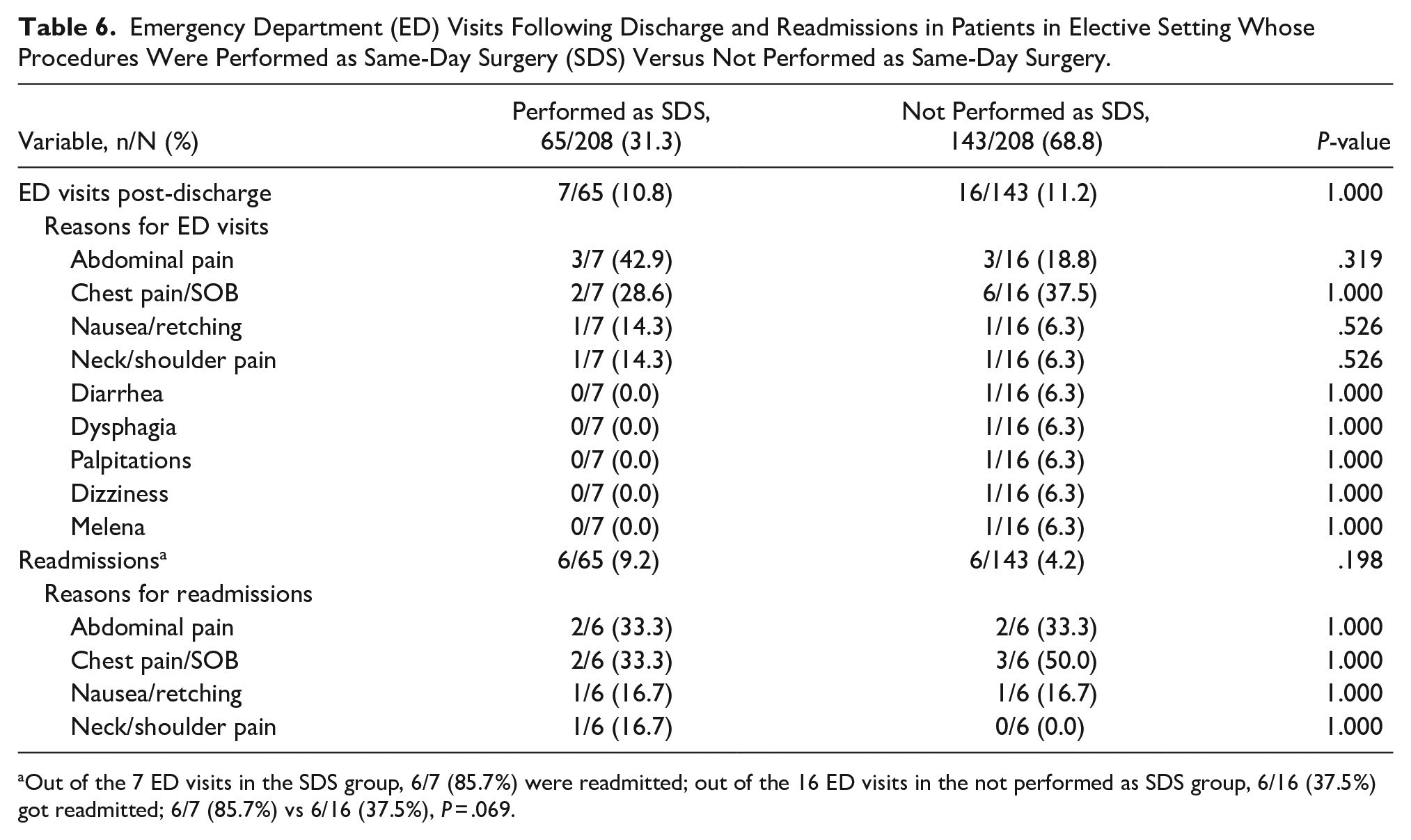
Out of the 7 ED visits in the SDS group, 6/7 (85.7%) were readmitted; out of the 16 ED visits in the not performed as SDS group, 6/16 (37.5%) got readmitted; 6/7 (85.7%) vs 6/16 (37.5%), P = .069.
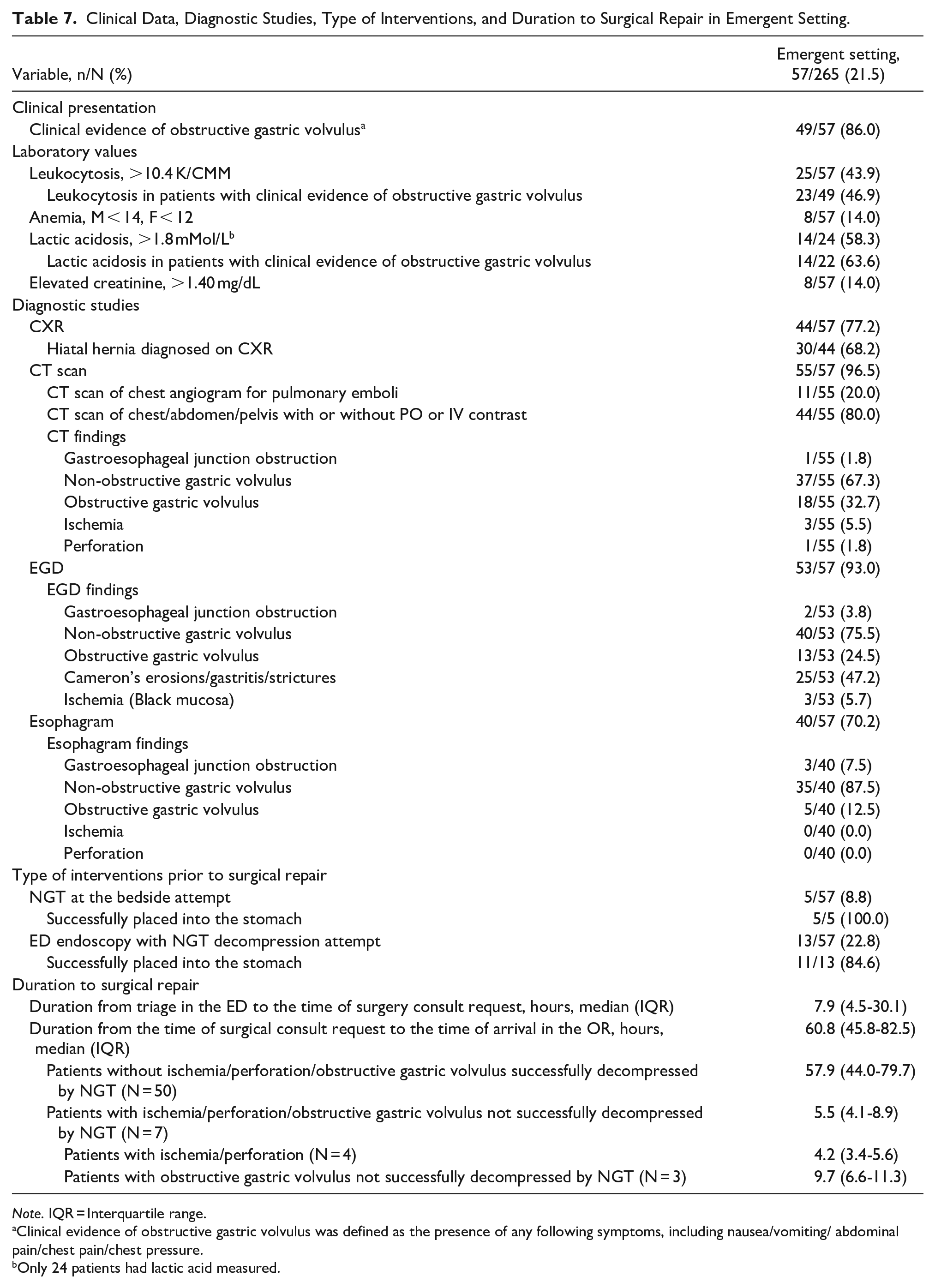
Ischemia was seen in 4/57 (7.0%) of emergent procedures and perforation in 1/57 (1.8%). All patients with ischemia had focal gastric ischemia treated with debridement and primary repair. The gastric perforation was repaired primarily. None required partial gastrectomy. The mean WBC level in patients with ischemia was 18 500 K/CMM, range (11 600-26 000), and the mean lactic acid level in patients with ischemia was 3.1 mMol/L, range (1.8-5.2).
Clinical data, diagnostic studies, and types of interventions in patients with type IV hiatal hernia repairs performed in emergent settings are shown in Table 7.
Clinical Data, Diagnostic Studies, Type of Interventions, and Duration to Surgical Repair in Emergent Setting.
Note. IQR = Interquartile range.
Clinical evidence of obstructive gastric volvulus was defined as the presence of any following symptoms, including nausea/vomiting/ abdominal pain/chest pain/chest pressure.
Only 24 patients had lactic acid measured.
Comparing repairs in an emergent setting without ischemia, 53/57 (93.0%) versus those with ischemia, 4/57 (7.0%) showed comparable demographic and clinical presentation. Patients with ischemia had a lower prevalence of ASA of II: 8/53 (15.1) versus 0/4 (0.0) and had higher ASA of IV: 10/53 (18.9) versus ¼ (25.0), P < .003. The operative time was 127.5 minutes (102.5-161.0) versus177.0 (137.5-233.0), P = .166. The 30-day mortality was 2/53 (3.8%) versus 0/4 (0%), P = 1.000. Leukocytosis was higher in the group with ischemia: 21/53 (39.6%) versus 4/4 (100%), P = .027, lactic acidosis was 11/21 (52.4%) (of patients who had lactic acid measured) versus 3/3 (100%), P = .239. The length of stay was 2 days (1-4) versus 6 days (3-8), P = .165.
Discussion
Clinical Manifestations
Our study shows that the clinical manifestations of type IV hiatal hernias differ in elective and emergent settings. The most common presenting symptoms in the elective setting in our study were regurgitation and dysphagia versus obstructive symptoms and upper gastrointestinal bleeding in the emergent setting. Previous reports have shown similar clinical manifestations.2,12 The physical exam in patients with obstructive symptoms can be misleading as patients may have a soft and non-tender abdomen because the primary pathology is intrathoracic. In those patients, the surgical plan may be based on presenting symptoms such as nausea and vomiting, laboratory values, and radiographic and endoscopic findings rather than the abdominal exam. Our study showed that about 20% of patients with type IV hiatal hernia can present in the emergent setting. Therefore, patients with type IV hiatal hernia must be informed of the risks related to their condition and its associated complications. None of the 57 patients in the emergency setting in our study were previously seen in our clinic, as we routinely suggest urgent repair in all symptomatic type IV hiatal hernias.
Ischemia and Perforation in the Emergent Setting
We showed that ischemia and perforation are rare complications of type IV hiatal hernias.
Other studies with repairs via an open approach have reported a rate of ischemia of 0% to 2.0%.12,13
Leukocytosis (WBC > 10.4 K/CMM) in our study was seen in 25/57 (43.9%) patients in the emergent setting and ischemia in only 4/25 (16.0%). This finding indicates that leukocytosis may have a higher specificity than sensitivity, possibly until it reaches higher levels; the same may apply to lactic acidosis >1.8 mMol/L, which was seen in 14/24 (58.3%) and ischemia in only 3/14 (21.4%).
Prompt intervention to reduce the hernia and restore gastric blood flow can prevent the progression of an obstructive volvulus to ischemia and perforation. All 4 patients with ischemia, including ¼ with perforation, had good outcomes, emphasizing the importance of prompt surgical intervention in those patients. Three out of 4 patients with ischemia, including the 1 with perforation, underwent laparoscopic repair, highlighting the feasibility of a laparoscopic approach in the emergency setting.
Emergent Versus Urgent Repair
We showed that patients with emergent presentations can be treated differently based on their clinical manifestations and disease severity. In the absence of ischemia or perforation and in patients with obstructive gastric volvulus responding to gastric decompression with a nasogastric tube or endoscopy, as seen in 50/57 (87.7%) in our series, patients can be treated with delayed repair during the same admission.
Delayed repair, when possible, allows adequate fluid resuscitation and a cardiac evaluation to assess the operative risk. In patients with clinical and radiographic evidence of obstructive gastric volvulus, gastric decompression has significant clinical advantages prior to surgical repair. First, it decreases the risk of aspiration during intubation; second, it prevents the adverse hemodynamic effects of a distended intrathoracic stomach on the heart and lungs; and lastly, it decreases the intraoperative risk of gastric perforation. Mobilizing a distended stomach is more challenging and the thin wall of a distended stomach increases the risk of gastric perforation when manipulated by instruments such as Babcock.
Perioperative Complications
Our results show that laparoscopic IV hiatal hernia repair can be performed with minimal perioperative complications in elective versus emergency settings.
In-hospital blood transfusion for anemia was higher in the emergent setting than in the elective setting in our study, which seems to be related to a higher number of patients with anemia as the presenting symptom in the emergent group. All procedures were performed with minimal blood loss, emphasizing the feasibility of laparoscopic repair in elective and emergent settings. Previous studies have reported minimal intraoperative and postoperative bleeding in large hiatal hernia repairs in both transthoracic (0.5%) 3 and laparoscopic approach (0.3%). 2
Atrial fibrillation was higher in the emergent setting in our study; this finding may be related to the older age of patients in the emergent setting, the stress associated with the effect of an obstructive gastric volvulus and gastric distension on the heart, fluid shifts, and the need for more aggressive fluid resuscitation in the emergent group. Other studies have shown a variable rate of atrial fibrillation, with 0.5% in the transthoracic approach, 3 8.3% in the transabdominal approach, 4 and none in the laparoscopic approach. 2
We had 2/265 (0.8%) devastating complication of retained Penrose that was placed around the gastroesophageal junction for esophageal retraction; both underwent reoperation and laparoscopic removal. Therefore, we changed our policy from the use of Penrose to a rolled Surgicel for esophageal retraction.
We had no esophageal leak in our study. Gastric leak was seen in 1 elective repair. In our previous report of 131 large hiatal hernias from 2009 to 2015 that included 54 (41.2%) type IV hiatal hernias, 1 we had 2/131 (1.5%) esophageal leaks, ½ had a type IV hiatal hernia with an intrathoracic stomach, and both had undergone a Toupet fundoplication. The lower rate of esophageal leak in our present study is related to the experience of the surgical team, maybe the fact that we did not use a Collis gastroplasty, and possibly related to the fact that we have changed our approach from Toupet to fundopexy, which does not require placing stitches in the esophagus.
We believe that placing stitches in the esophagus following extensive mediastinal esophageal mobilization, esophageal devascularization, and hernia sac excision in patients with type IV hiatal hernia, who are generally older, may increase the risk of a leak; the risk may be lower in patients with type I hiatal hernia, who are generally younger and in whom less extensive esophageal mediastinal mobilization is required.
Prior studies have reported no esophageal leaks in transabdominal repairs, 4 0.8% in transthoracic repairs, 3 and 2.4% 2 to 6.8% 14 in laparoscopic repairs. Overall, it seems that perioperative complications of type IV hiatal hernia repairs are related more to institutional experience and volumes than the surgical approach, emphasizing that type IV hiatal hernias in elective and emergent settings should be performed in high volumes institutions.
Same-Day Surgery
The outcomes of type IV hiatal hernia repairs have improved over time, from a length of stay of 7 days via a transthoracic approach reported in 1967, 6 4.5 days via an intrabdominal approach in 2004, 3 2 to 3 days via a laparoscopic approach in 2010, 2 to outpatient laparoscopic repairs in the 2020s, as we previously reported.7 -9
Same-day surgery was planned in 83/208 (39.9%) elective repairs in our study and was performed in 65/83 (78.3%). As previously reported, we have implemented an ERAS protocol with a series of measures in perioperative phases 7 including the use of an opioid-free anesthesia 8 to achieve same-day surgery. The present study confirms that there were more same-day surgeries with opioid-free anesthesia versus opioid-based anesthesia. Presently, we plan same-day surgery in all elective procedures, and the 2 exclusion criteria for planning same-day surgery are admission via the emergency department and ASA of IV. The most common reason for the transition to observation was patient preference. Ultimately, the final decision on when to discharge a patient is made on the day of surgery based on the patient’s comorbidities, duration of operation, and clinical condition in the recovery room rather than the patient’s age and preference.
30-Day-Mortality
While the length of stay for large hiatal hernia repairs has significantly decreased over time, the 30-day mortality seems to be comparable with all types of surgical approaches and throughout the previous decades, with 1.2% via a left thoracotomy in 1967 6 and 1.7% in 2004, 3 0% in the open transabdominal in 2005, 4 and 1.7% in laparoscopic repairs in 2011. 2
We had 2/265 (0.8%) 30-day mortalities in the emergent setting: one 90-year-old female from fulminant HIT and one 85-year-old female from MI. The findings of our study and others confirm that hiatal hernia repair of large hiatal hernias can be performed with low mortality, and the cause of death is mainly related to overall patient condition and patient selection rather than surgical approach or direct consequence of the operation such as leak or bleeding.
Symptomatic Recurrence
In a study of 131 patients with large hiatal hernia, with a follow-up in 99 patients, we showed a symptomatic recurrence requiring reoperation in 8/99 (8.1%), 2 in the perioperative period, and 6 at 25 months (8-31). 1 We further compared outcomes of Toupet fundoplication versus fundopexy in all types of hiatal hernias and showed that at a follow-up of 38.4 months (29.0-44.6) versus 19.7 months (14.2-23.5), symptomatic recurrence requiring reoperation was seen in 15/133 (11.3%) in the Toupet fundoplication group versus none in the fundopexy group.
In the present study, symptomatic recurrent hiatal hernia requiring reoperation was seen in 13/265 (4.9%) at a median time of 24.0 months (11.8-35.8) in 10/152 (6.6%) with Toupet fundoplication versus 1/87 (1.1%) with fundopexy, P = .060. One explanation for the lower rate of symptomatic recurrence requiring reoperation in the Toupet group in the present study compared to the Toupet group in our previous study that included type I hiatal hernias may be related to the fact that patients with type IV hiatal hernias are older and perform fewer activities such as heavy lifting that may result in recurrence, compared to patients with type I hiatal hernia who are mostly younger and more active.
We perform esophageal mediastinal mobilization from the aorta and bilateral pleura to the level of the pericardium to achieve tension-free intrabdominal esophageal length in all patients with type IV hiatal hernia. We believe mediastinal esophageal mobilization can be achieved more easily and under direct vision with a laparoscopic approach compared to an open transabdominal. The transthoracic approach provides a clear dissection plane and allows extensive esophageal mobilization, however, is more morbid compared to a laparoscopic approach.
With an aging population, type IV hiatal hernias will remain a relevant healthcare problem. Patients and healthcare providers should be aware of clinical manifestations, the possibility of emergent presentation, and complications associated with type IV hiatal hernias.
All procedures in our study were performed by the same surgical team in a single center. Consistency creates a learning environment with continuous improvement in knowledge and competency. Clear protocols set a culture of safety, result in better outcomes, and gradually increase the number of same-day surgeries in elective repairs so that same-day surgery becomes a rule rather than an exception.
Conclusion
Laparoscopic type IV hiatal hernia repair with good outcomes is possible in elective and emergent settings. Same-day surgery can be achieved in elective repairs. About 20% of patients experience an emergent presentation, which is more common in older patients with lower BMI and higher ASA. In rare cases, ischemia and perforation may occur; however, prompt intervention can lead to good outcomes. Presentations without ischemia or perforation can be treated with nasogastric placement, endoscopic decompression, and urgent repair during the same hospital stay.
Limitations
We acknowledge the limitations of our study, including its retrospective nature, lack of longitudinal follow-up prior to emergent repairs, heterogeneous assessment of patients who presented to the emergency department with different types of CT scans and interventions, such as bedside versus endoscopic nasogastric tube placement, lack of homogeneous laboratory values, such as lactic acid levels in all patients, and lack of radiographic follow-up post-discharge to assess for recurrence in all. Patients may have presented to other centers with post-operative complications and symptomatic recurrence requiring reoperation that we are unaware of.
Footnotes
Acknowledgements
We want to acknowledge Dr. Justin Tholany, Chief of Staff, Memorial Hermann Southeast and Pearland, Chairman of the Esophageal Disease Radiology at Memorial Hermann Southeast, for performing and interpreting the majority of videoesophagrams in this study and leading our radiology department to deliver excellence in gastrointestinal radiology at our center, Tuan Murray, MBA, imaging educator, Eleanor Garcia-Rogers, lead diagnostic imaging technologist for her leadership and availability, Lisa Araguz, lead diagnostic imaging technologist, Magen Halewyne, diagnostic imaging technologist, Chea’ Williams, diagnostic imaging technologist, A. Jim Harville, surgery/diagnostic imaging technologist, and Joseph K. Thomas, surgery/diagnostic imaging technologist at Memorial Hermann Southeast, for their great attitude, hard work, and dedication to patient care.
Author Contributions
S.P.: study design; acquisition of data; revision manuscript. R.T.: study design; acquisition of data; revision manuscript. C.H.: acquisition of data; revision manuscript; statistical analysis. M.M.: acquisition of data; revision manuscript; statistical analysis. F.B.: study design; acquisition of data; writing and revision manuscript.
Data Availability
Data is available for review as per the editor’s request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The study was approved by the institutional review board at UTHealth and Memorial Hermann system.
Use of Artificial Intelligence
Not applicable.