
Abstract
Background:
Gastroesophageal reflux disease (GERD) is usually associated with disruption of the esophagogastric junction (EGJ). The endoscopic Hill classification has proven to be inadequate to assess EGJ integrity. Recently, the American Foregut Society (AFS) developed an endoscopic classification focused on hiatal hernia (L), hiatal opening (D), and the flap valve (F). While pH-monitoring remains the gold standard for the diagnosis of GERD, high-resolution manometry (HRM) can assess EGJ anatomy and competency. Aim of this study is to validate the AFS classification in patients with suspected GERD assessing its accuracy in predicting EGJ disruption and pathologic reflux.
Methods:
We prospectively enrolled patients with suspected GERD who underwent upper endoscopy, HRM and pH-study between November 2022 and March 2023. Demographic and clinical data were analyzed. The efficacy of the AFS classification in predicting GERD (acid exposure time, AET > 6%) was assessed. Each component of the classification was compared with the corresponding HRM variable.
Results:
Among 56 patients (48% men, BMI 23.5 kg/m2, age 43 years), an AET > 6% was found in 22 (39%), and in 0% of patients with AFS grade I, 5.9% with grade II, 52% with grade III and 77.8% with grade IV (P < .001). The L component effectively predicted the EGJ type, the D the EGJ-Contractile Integral, while the absence of the flap valve was related to a positive Straight Leg Raise maneuver.
Conclusions:
The new grading system is able to stratify patients with pathologic GERD. Moreover, the single components of the AFS classification are associated with manometric markers of EGJ disruption.
Keywords
Key Learning Point
● The American Foregut Society endoscopic classification for EGJ integrity can effectively stratify patients with pathologic GERD.
● The single components of the classification correlates with HRM parameters that represent different mechanism of EGJ disruption.
● Higher AFS grades are associated with a more profound degree of EGJ disruption.
Introduction
Gastroesophageal reflux disease (GERD) symptoms reach the prevalence of 18% in Western Countries. 1 However, as defined by the Rome IV Conference, there are several functional syndromes that can mimic GERD, 2 making diagnostic tests mandatory to obtain a definitive diagnosis. According to Lyon 2.0 criteria, an acid exposure time (AET) >6% at multichannel intraluminal impedance pH-study (MII-pH) or pH study alone, a Los Angeles grade B, C, or D esophagitis or Barrett’s esophagus at upper endoscopy are needed to diagnose an “actionable GERD.” 3 However, these criteria do not describe the mechanisms involved in the pathophysiology of the disease, the understanding of which could help physicians to provide a tailored treatment. Traditionally, the Hill classification, introduced in 1996, has been used to assess esophago-gastric junction (EGJ) integrity during upper endoscopy. 4 Nevertheless, its clinical significance has been limited by the lack of standardization and reproducibility and by an unclear distinction between the grades. Moreover, the role of length of hiatal hernia measurement is uncertain and not included in the classification. Recently, the American Foregut Society (AFS) developed a new endoscopic classification system focused on 3 components: axial length of hiatal hernia (L component), wideness of hiatal opening (D component) and presence of the flap valve (F component). 5 Since this classification was built using a Delphi method, it needs validation with objective clinical data. While pH-monitoring remains the gold standard for the diagnosis of pathologic acid reflux, high-resolution manometry (HRM) can assess the EGJ anatomy and competency by means of the EGJ type, the EGJ-contractile integral (EGJ-CI), and the straight leg raise (SLR) maneuver. Aim of this study is to validate the AFS classification in patients with suspected GERD and to assess its accuracy in predicting pathologic reflux and EGJ disruption.
Methods
A prospective study was conducted at our referral center for esophageal diseases. After Institutional Review Board, consecutive patients with GERD symptoms who underwent upper endoscopy, HRM and pH-study were enrolled between November 2022 and March 2023.
Inclusion criteria were age between 18 and 75 years, upper endoscopy performed off-proton pump inhibitors (PPI) for at least 2 weeks, HRM and reflux study performed within 1 month from the endoscopy. Patients with eosinophilic esophagitis, scleroderma, achalasia, prior esophageal surgery, and pregnancy were excluded.
All the patients were referred at our center after the 8-week PPI trial. After clinical evaluation, the patients underwent upper endoscopy, HRM and MII-pH study off-PPI, regardless of response to antisecretory medications. The endoscopy was performed by 2 expert physicians (AL and PM) who had carefully reviewed the AFS classification prior to the beginning of the study. During endoscopy, Hill and ASF classification were recorded and classified.
The function tests were performed by expert physicians (SS and MS) who were blinded from the classifications. According to the Lyon Consensus 2.0, an AET > 6% on MII-Ph study or 2 days of AET > 6% on wireless pH-study defined pathologic GERD. 3
The study was conducted in accordance with the Helsinki Declaration. All authors had access to the study data; each author reviewed and approved the final manuscript.
Clinical Evaluation
Demographic and clinical data including age, body mass index (BMI), use and response to PPI and time from symptoms onset were collected during endoscopy. Symptoms burden was evaluated using validated questionnaires. GERD-Q 6 was used to assess the overall impact of GERD symptoms; GERD Health Related Quality of Life (GERD-HRQL) 7 to assess heartburn and Reflux Symptom Index (RSI) 8 for extra-esophageal symptoms.
Upper GI-Endoscopy
Endoscopy was performed with the patient in left lateral decubitus and on conscious sedation. All the abnormalities of the esophagus, stomach and duodenum were recorded in the final report.
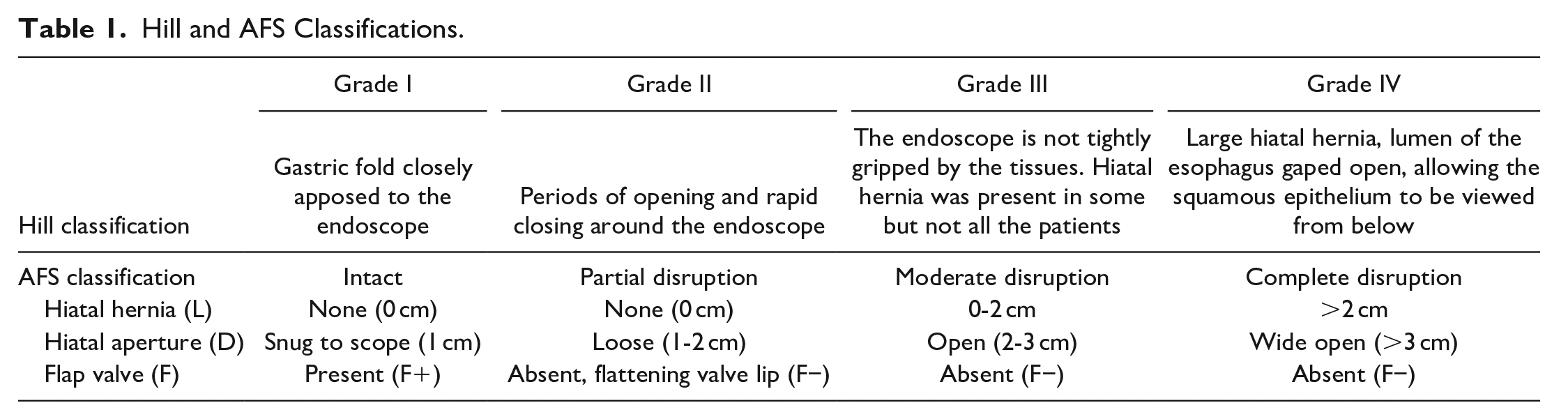
The Z-line was evaluated and the presence of esophagitis was classified according to the Los Angeles classification. Upon entering the stomach, the EGJ was evaluated in retroflexed view. Insufflation was kept for approximately 30 to 45 seconds or until the rugal folds of the gastric fundus were flattened. The hiatal aperture was measured using the standard scope of 1 cm as reference (D component). The presence of the flap valve was therefore evaluated (F component). A provocative maneuver consisting in a gentle pull of the endoscope toward the lesser curvature was performed in order to induce potential hiatal hernia. After the maneuver, the forward view was restored to record hiatal hernia axial length, defined as the distance between the end of the gastric folds and diaphragmatic indentation (L component). Each component of the AFS classification was recorded in a dedicated case report form. The final AFS grade is determined by the component with the worse grade. Hill classification was recorded according to the original paper. AFS and Hill grading systems are fully detailed in Table 1.
Hill and AFS Classifications.
High-resolution Esophageal Manometry
High-resolution manometry was performed using a solid-state catheter with 36 circumferentially incorporated sensors spaced at 1-cm intervals, following the Chicago Classification 4.0 (CCv4.0) standard protocol. 9 After an overnight fast, ten swallows of 5 mL room temperature water were performed in the semi-recumbent position. Failed, weak or intact swallows were defined according to CCv4.0, based on distal contractile integral (DCI) values (≤100 mmHg•cm•s, 100-450 mmHg•cm•s and ≥450 mmHg•cm•s). Patients with >70% weak swallows or ≥50% failed swallows were categorized as ineffective esophageal motility (IEM). The assessment of EGJ competency was performed using the EGJ-CI, total and intra-abdominal LES length, and EGJ morphology. EGJ-CI was calculated during the reference period for 3 respiratory cycles at the isobaric contour of gastric pressure plus 2 mmHg using the DCI software tool over the EGJ. 10 The EGJ type was classified according to CCv4.0 as type 1 (superimposed LES and CD), type 2 (LES-CD separation <3 cm) and type 3 (LES-CD separation ≥3 cm). Multiple rapid swallows (MRS) were performed at the end of the protocol and consisted of 5 swallows of 2 mL of water administered at <3 seconds intervals. Contraction reserve was present when the ratio between MRS DCI and mean single swallow DCI was >1.
The SLR maneuver was performed after the MRS as previously described. 11 The patient was asked to raise 1 leg in supine position for 5 seconds. Double leg raise consisted in the elevation of both legs and it was performed if abdominal pressure did not increase with the single leg raise. HRM operator was allowed to help the patient if he was not able to elevate both legs. The SLR maneuver was considered effective if the intra-abdominal pressure increased by 50% during SLR. Intra-esophageal peak pressure 5 cm above the LES was analyzed both during baseline and SLR maneuver, and an increase of 11 mmHg was considered abnormal.
Esophageal pH and pH-Impedance Study
All pH studies were performed after at least 2 weeks of PPI withdrawal. Wireless 96-hour pH-study or catheter-based 24-hour pH-impedance study were both allowed. The wireless pH-study capsule (BRAVOTM) was positioned 6 cm above the cardia during endoscopy. According to Lyon consensus 2.0, 3 the cut-off for a positive wireless pH-study was an AET > 6% for at least 2 days. The multichannel intraluminal impedance-pH (MII-pH) studies were performed using catheters with 8 impedance and 2 pH electrodes. After calibration, the catheter was inserted trans-nasally with the pH electrode positioned 5 cm above the LES. Symptoms, duration of meal and time spent in the recumbent position were recorded on a diary.
Total, upright and recumbent AET, number of acid, weakly acid, and weakly alkaline reflux episodes, DeMeester score, symptom index (SI) and symptom association probability (SAP) were recorded. Mean nocturnal basal impedance (MNBI) and post-reflux swallow-induced peristaltic wave (PSPW) index were also collected from all pH-impedance studies. 12
Data Collection and Statistical Analysis
Categorical variables are reported as count and percentage, while numerical variables as median and interquartile range (IQR). The normality of continuous variables was assessed using the Shapiro–Wilk test. Continuous values were compared between the groups using the nonparametric Mann-Whitney U test or Kruskal–Wallis H test, while Chi Square or Fisher test were used as appropriate for categorical values. The population was stratified according to AFS and Hill grade and the endoscopic grades were compared with the outcome variable (AET > 6% on MII-pH, 2 days of AET > 6% for wireless pH-study). The different component of the AFS classification were compared with objective HRM parameters: the L component with the EGJ type, the D component with the EGJ-CI and the F component with the SLR response. A sub-analysis of patients with AFS grade III and IV was performed to identify the single component that most influenced the final grade.
A two-tailed P-value .05 was considered significant for all statistical test. Statistical analyses were performed using Statistical Package for the Social Sciences Software (SPSS 25.0®). 13
Results
A total of 56 patients met the study criteria and were included. The median age was 42.6 years, BMI 23.5 kg/m2, and symptom duration 36 months. A total of 22 patients (39%) presented a positive pH-study. The GERD group had a significant higher rate of patients with EGJ type 3 (13.6% vs 0%, P = .030) and with SLR maneuver >11 mmHg (70% vs 21.9%, P < .001), and a lower median EGJ-CI (26.7 vs 32.6 mmHg * cm, P = .048), as detailed in Table 2.
Demographic, Clinical, High-Resolution Manometry and pH Characteristics of the Overall Patient Population According to Acid Exposure Time (AET).
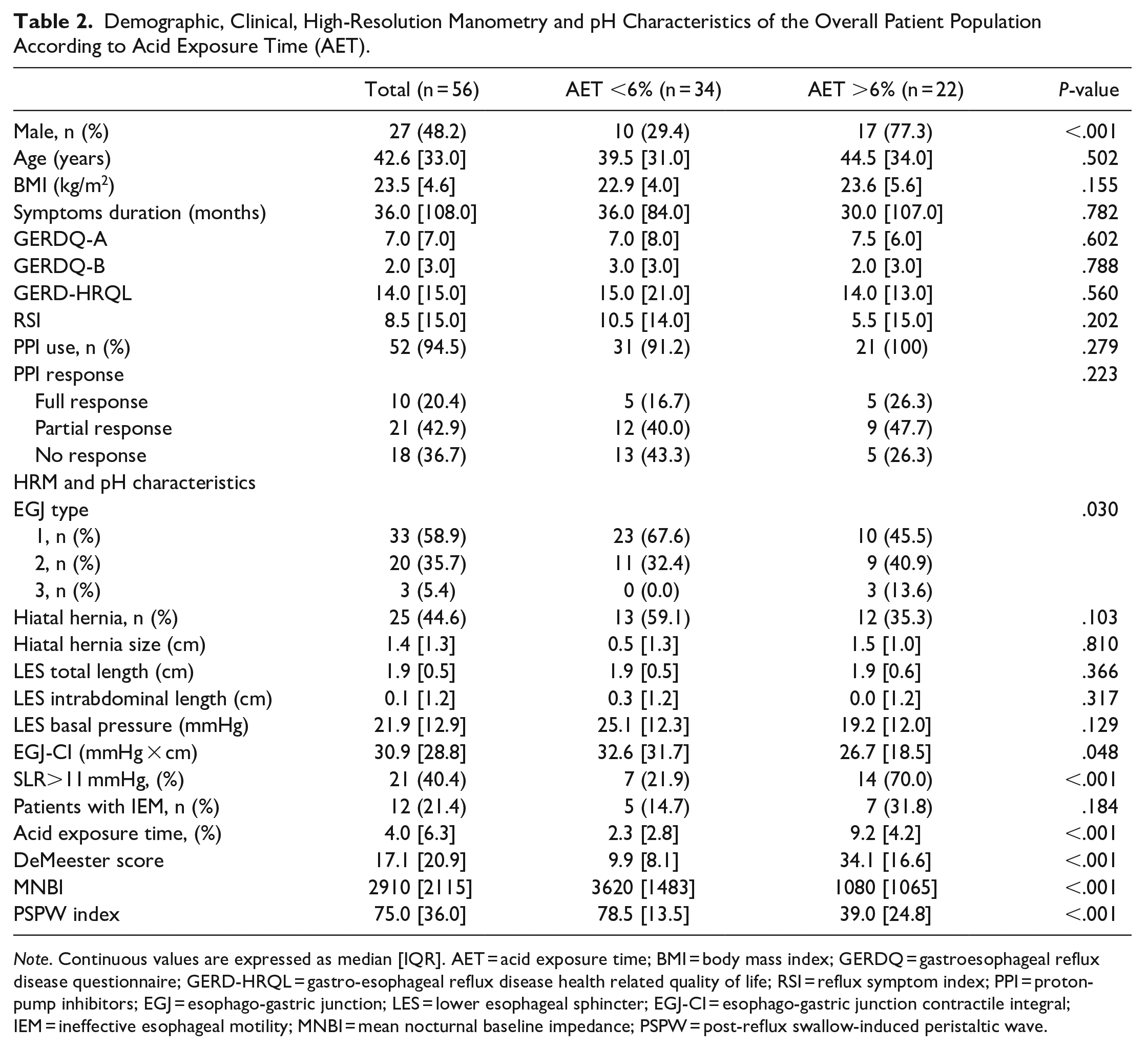
Note. Continuous values are expressed as median [IQR]. AET = acid exposure time; BMI = body mass index; GERDQ = gastroesophageal reflux disease questionnaire; GERD-HRQL = gastro-esophageal reflux disease health related quality of life; RSI = reflux symptom index; PPI = proton-pump inhibitors; EGJ = esophago-gastric junction; LES = lower esophageal sphincter; EGJ-CI = esophago-gastric junction contractile integral; IEM = ineffective esophageal motility; MNBI = mean nocturnal baseline impedance; PSPW = post-reflux swallow-induced peristaltic wave.
Figure 1 shows the differences in terms of positive pH-study in the study population when stratified for Hill and AFS classification. In the AFS classification a stepwise increase of patients with AET > 6% was found (0% in grade I, 5.9% in grade II, 52% in grade III, and 78% in grade IV, P < .001).

Rate of patients with acid exposure time >6% in the study population stratified by Hill and AFS classification.
Considering AFS grade 3 and 4 as positive test, sensitivity was 90.9%, specificity 58.8%, positive predictive value was 58.8% and negative predicted value was 90.9%.
Patients with higher grades of AFS classification showed worse HRM parameters related with GERD, such as intra-abdominal LES length, EGJ-CI and positive SLR maneuver, as detailed in Table 3.
High-Resolution Manometry Characteristics of the Study Population Stratified for AFS Grade.
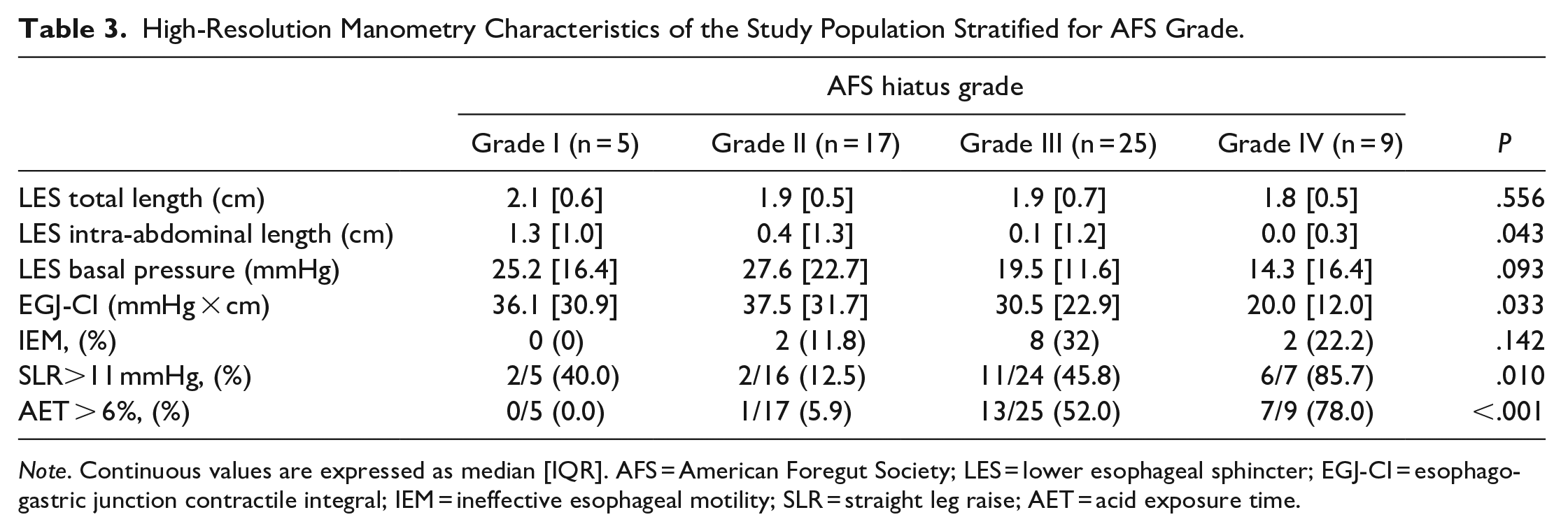
Note. Continuous values are expressed as median [IQR]. AFS = American Foregut Society; LES = lower esophageal sphincter; EGJ-CI = esophago-gastric junction contractile integral; IEM = ineffective esophageal motility; SLR = straight leg raise; AET = acid exposure time.
With regard to the analysis of the single components of the AFS classification, the L component was significantly associated with EGJ type and LES intra-abdominal length. A manometric EGJ type I was present in 70% of the patients with L grade I or II, in 44.4% with grade III and in 14.3% with grade IV (P < .001). The median EGJ-CI gradually decreased as the D grade increased, as well as LES basal pressure, as shown in Table 4. Only 2 patients with a positive SLR maneuver were found in the F+ group (15.4%), compared with 48.7% in the F- (P = .033).
High-Resolution Manometry Parameters Associated With the Components of the AFS Classification.
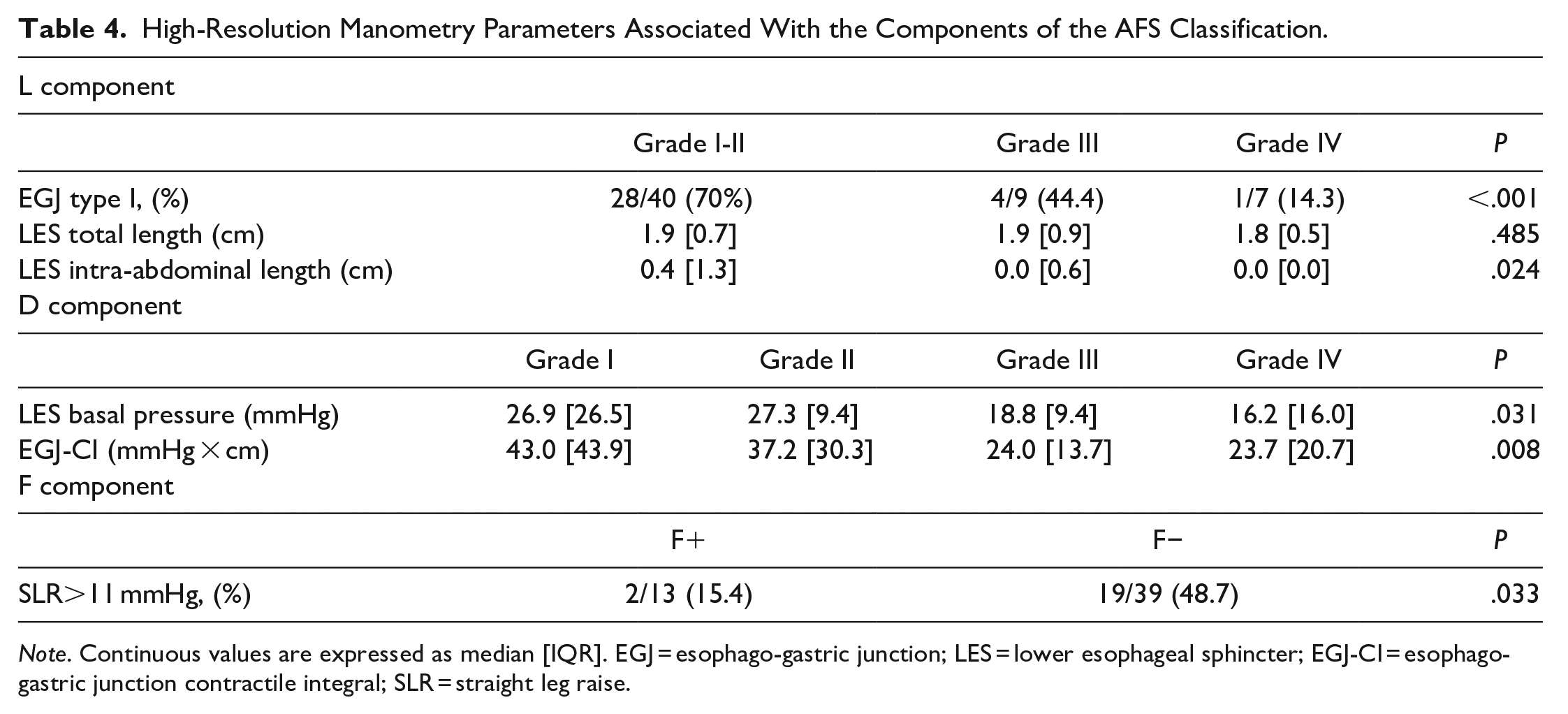
Note. Continuous values are expressed as median [IQR]. EGJ = esophago-gastric junction; LES = lower esophageal sphincter; EGJ-CI = esophago-gastric junction contractile integral; SLR = straight leg raise.
A sub-analysis of patients with AFS grades III and IV showed that in 26/34 patients (76%) a single component was worse than the others and therefore determined the final grade. The L component drove the classification in 6 patients (17.6%), the D component in 14 patients (41.2%) and the F component in 6 patients (17.6%).
Discussion
In this prospective study evaluating patients with GERD symptoms with endoscopy, HRM and pH study, we validated the endoscopic AFS classification for EGJ disruption. Furthermore, we demonstrated the ability of the single components of the classification to identify the pathophysiologic mechanism underlying GERD.
The AFS classification is proposed as an alternative to the old Hill classification. One of the main differences between the two grading systems is the main role that the presence of hiatal hernia has in the AFS compared to the Hill. In our study, the L component, that represents hiatal hernia axial length, correlates with the EGJ type at HRM, considered the gold standard in the evaluation of hiatal hernia. 14 In AFS L grade I and II, including patients without endoscopic evidence of hiatal hernia, an HRM EGJ type I was found in 70% of the cases, compared with 44.4% in grade III and 14.3% in grade IV (P < .001). Also, the intra-abdominal LES length, a crucial variable for EGJ competency, 15 was significantly different among the groups. A previous study by Oberg et al. evaluated the efficacy of Hill classification to determine the intra-abdominal length of LES when compared with conventional manometry, and found that Hill classification was able to find a significant difference in terms of intra-abdominal LES length only comparing the outer grades, I and IV. 16 In this study, we demonstrated that L grade in AFS classification is superior to Hill classification in the identification of hiatal hernia and LES position.
Hiatal aperture is described by the AFS D component. Based on the assumption that the wider is the hiatus the lesser would be the pressure of the EGJ, we evaluated the D component comparing it with pressure parameters at HRM. The LES basal pressure has been traditionally used to evaluate EGJ competency in the conventional manometry era. In the previously cited paper by Oberg et al., Hill grade IV presented with a significant lower LES pressure when compared with the other grades, but grade II and III were similar. EGJ-CI is a novel HRM parameter that encompass pressure and length of the LES and the crura diaphragm, providing a more realistic evaluation of the EGJ complex competency. 10 In our study, the EGJ-CI showed a stepwise decrease across the AFS grades, with similar values only between grades III and IV. This is probably explained by the fact that in both grades the EGJ is disrupted and too loose to allow a precise measurement of the component itself. Again, we found AFS classification to be superior to Hill in the identification of a hypotensive LES due to EGJ disruption.
The flap valve is a muscolomucosal fold positioned at the angle of His, and it plays a crucial defensive role in protection from reflux. The main hypothesis of his mechanism of action states that this fold provides a mechanical protection from gastro-esophageal reflux, thrusting against the lesser curvature when intragastric pressure increases. 17 The SLR is a novel provocative maneuver that increases intra-abdominal pressure during HRM, evaluating the ability of the EGJ to prevent a consequent increase in intra-esophageal pressure. 11 Although it is still unknown which component of the EGJ is responsible for a positive SLR, we speculated that the ability of the flap valve in preventing a backward pressure could be assessed by this maneuver. In our cohort, only 15.4% of the patients with a positive SLR were present in the F+ group, compared with 48.7% in the F- group, demonstrating a significant association between SLR maneuver and flap valve.
Among the patients with AFS grade III and IV, the D component determined the final grade in the classification in 41.2% of the subjects. Since this component reflects the degree of crura separation, these data support the importance of the extrinsic sphincter as anti-reflux mechanism. 18
As shown in Figure 1, Hill grade II and III present similar rates of patients with AET > 6% (42.1% vs 37.9%), demonstrating the inability of this grading system to stratify patients with GERD. In 1999, Oberg et al. found that 75% of patients with Hill IV presented with a pathologic AET, but this indicator had a lower impact when compared to other endoscopic criteria of GERD. 16 We found a stepwise increase in patients with pathologic GERD in AFS classification (0% in grade I, 5.9% in grade II, 52% in grade III, 78% in grade IV), with significant differences between each grade.
These findings could be explained by the fact that the three main HRM variables associated with GERD (LES intra-abdominal length, EGJ-CI and SLR > 11 mmHg) were significantly worse in higher AFS grades, demonstrating a more profound degree of EGJ disruption.
Several factors explain the differences between the Hill and AFS classifications. First, a more standardized protocol allows consistency in the allocation of patients into different grades. Second, the vagueness in the definition of Hill grades has been eliminated by the measurement of objective parameters (ie, hiatal hernia axial length, hiatal diameter). Finally, a more profound awareness of the different components of the anti-reflux barrier (crura diaphragm, flap valve and LES) made the AFS classification more balanced than the Hill, solely based on the flap valve.
The major strengths of this study are the prospective design, a thorough pathophysiologic evaluation and that physicians performing HRM and pH-study were blinded to endoscopic classifications.
This study has also some limitations. First, the single center nature in a tertiary center for esophageal diseases may limit his reproducibility in real world. Second, the learning curve for acquisition of the new classification has not been taken into account, nor the possible variability between the physicians evaluating the AFS grades during endoscopy.
Conclusions
In conclusion, the AFS classification is able to stratify patients with pathologic GERD and to identify different grades of EGJ disruption. Moreover, the single components of the classification are related to different factors participating in the integrity of the anti-reflux barrier.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The study was conducted in accordance with the Helsinki Declaration and was approved by the Istitutinal Review Board.
Use of Artificial Intelligence
The authors did not use artificial intelligence tools in any steps of the production of this article.