
Abstract
Introduction:
Per-Oral Endoscopic Myotomy (POEM) is the recommended first-line treatment for all achalasia subtypes due to its minimally invasive nature. We aim to evaluate the trends of utilization, costs, and outcomes (mortality and complications) of POEM versus Heller Myotomy (HM) in U.S. hospitals.
Methods:
This is a retrospective study of individuals admitted with a primary diagnosis of achalasia. Data was obtained from Nationwide Inpatient Sample databases from the years 2016 to 2020 using ICD-10 codes. We assessed the therapeutic procedures employed, the trends and outcomes associated with POEM versus HM in terms of hospital utilization, mortality, morbidity, and the baseline characteristics of our study population.
Results:
A total of 26 880 adult individuals were diagnosed with achalasia. Of these, 11% underwent POEM, while 59% underwent HM. POEM rates increased from 6% to 10% of achalasia admissions, while HM decreased from 49% to 41% during the study period. No significant differences in total hospital charges or length of stay were observed between the 2 procedures. Regarding procedural complications, HM was associated with significantly reduced odds of pneumonia (adjusted Odds Ratio [aOR] = 0.09, 95% CI: 0.02-0.41), pneumoperitoneum (aOR = 0.11, 95% CI: 0.03-0.36), and pneumomediastinum (aOR = 0.21, 95% CI: 0.06-0.68), with no difference in the odds of esophageal perforation (aOR = 1.33, 95% CI: 0.27-6.48) and sepsis (aOR = 2.04, 95% CI: 0.22-18.40).
Conclusion:
While HM rates are currently declining in the U.S., POEM usage appears to be increasing. Despite being a less invasive measure than HM, POEM remains underutilized in the U.S.
Introduction
Achalasia is a rare motility disorder characterized by failure of the lower esophageal sphincter (LES) relaxation and failed peristalsis, resulting from degeneration of ganglion cells of the myenteric plexus. 1 Due to significant technological advances in diagnosis, specifically high-resolution esophageal manometry, the incidence and prevalence of achalasia have been rising with the latest estimates reporting an incidence of 2 to 3 per 100 000 persons/year2,3 and prevalence up to 32.5 per 100 000 persons/year. 3
Chronic achalasia symptoms (eg, dysphagia, regurgitation, and weight loss) have a significant impact on quality of life and are associated with increased morbidity and healthcare utilization.4,5 Therefore, definitive treatments to disrupt the LES for candidate patients are necessary. 6 For decades, definitive treatments included either laparoscopic Heller’s myotomy (HM) or pneumatic dilation (PD). 7 Per-Oral Endoscopic Myotomy (POEM) was first introduced in Japan in 2008 as a treatment modality for achalasia. 8 Offering the benefits of non-surgical minimally invasive intervention, POEM has been found equivalent to HM, 9 superior to pneumatic dilation10,11 with superior outcomes for spastic achalasia12-15 due to the ability to extend the myotomy length.
Major gastroenterology and surgical societies now recommend POEM as a first-line treatment option for achalasia and as the preferred modality in spastic achalasia.1,16-20 Data regarding the utilization of POEM in the treatment of achalasia in the U.S. remain scarce. Therefore, we aimed to assess the utilization, short-term complications, and costs of POEM in comparison with HM in hospitalized patients with achalasia in U.S. hospitals from a nationally-representative database.
Materials and Methods
Study Design and Data Source
Using the National Inpatient Sample (NIS), we conducted a study of individuals hospitalized from 2016 to 2020. The NIS database was developed for the Healthcare Cost Utilization Project (HCUP) to produce U.S. regional and national estimates of inpatient demographic and administrative data on healthcare utilization, cost, quality, and outcomes. 21 It is currently the largest public all-payer database in the U.S, representing a 20% sample of discharges from all non-federal acute care hospitals. 21 The data is selected from a stratified systematic random sample of hospitalizations, and is weighted to provide regional and national estimates for the entire U.S. 22 The International Classification of Diseases, Tenth Revision, Clinical Modification/Procedure Coding System (ICD-10-CM/PCS) codes databases from October 2015 to date. 23 The NIS database provides data on U.S. hospitalizations without patients identifying information, and no Institutional Review Board (IRB) approval was deemed necessary for this study. This study is reported following the “Strengthening the Reporting of Observational Studies in Epidemiology” (STROBE) statement guidelines provided in the Supplemental File).
Study Population and Variables
We studied individuals ≥18 years old with inpatient hospital admissions with a primary diagnosis of achalasia from the years 2016 to 2020. ICD-10 CM/PCS codes were used to identify patients admitted with a principal diagnosis of achalasia (K22.0), and who underwent POEM (0D847ZZ, 0D848ZZ), Heller myotomy (0D840ZZ, 0D843ZZ, 0D844ZZ), esophageal dilation (0D737ZZ, 0D738ZZ, 0D747ZZ, 0D748ZZ, 0D737DZ, 0D738DZ, 0D747DZ, 0D748DZ), or esophagectomy (0DB50ZZ, 0DB53ZZ, 0DT50ZZ, 0DT54ZZ) for the treatment of achalasia. The ICD-10 codes used for this study are provided in the Supplemental Materials and were extracted from a previous study using the NIS. 24
Patient and Hospital Characteristics
We extracted data available and defined within NIS on age, sex (female, male), race (non-Hispanic White, non-Hispanic Black, Hispanic, Other), primary insurance (Medicare, Medicaid, Private Insurance, Self-pay), median income quartile (in quartiles), hospital region (Northeast, Midwest, South, West), teaching status (teaching, non-teaching), and hospital size (small, medium, large). 21 Comorbidities were also captured as part of the Charlson comorbidity index (CCI), and categorized as 0, 1, 2, ≥3.25,26
Outcomes
The primary outcomes explored in this study were the mean length of hospital stay (LOS) and total hospital charges (THC). The secondary outcomes were the complications associated with procedures used for the treatment of achalasia (mortality, gastrointestinal [GI] bleeding, sepsis, pneumonia, esophageal perforation, pneumomediastinum, and pneumoperitoneum). The outcomes were adjusted for confounders which included age, gender, race, insurance status, median annual income, hospital region, hospital teaching status, hospital size, and CCI score.
Statistical Analysis
Baseline characteristics were compared in POEM versus HM using T-test and Chi-Square test. Multivariate linear regression analysis was used to calculate the adjusted mean LOS and THC, and multivariate logistic regression analysis was applied to compare the outcomes (mortality and complications). We assessed the yearly prevalence of procedures used for the treatment of achalasia, the yearly outcomes, and the baseline characteristics of our study population. We used GraphPad Prism 19 for trend lines. We analyzed weighted samples from the NIS database using the Stata/SE® Version 17.0 software (StataCorp, Texas, USA). A P-value of <.05 was set for statistical significance throughout the study.
Results
Baseline Population Characteristics
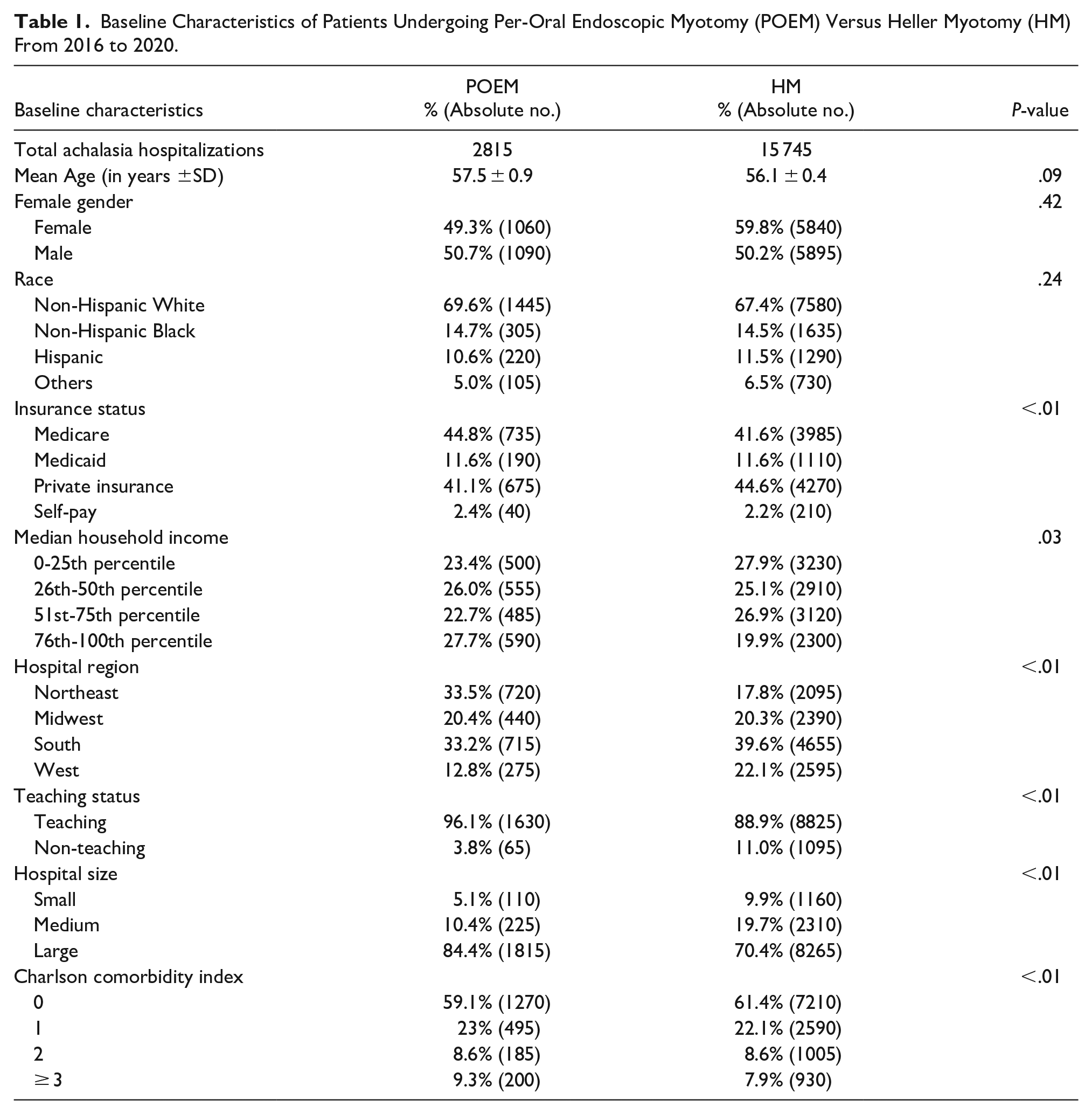
A total of 26 880 patients were discharged with a primary diagnosis of achalasia. Out of these, one-tenth (10.5%, n = 2815) underwent POEM, while more than half (58%, n = 15 745) underwent HM. There was no difference in mean age (P = .094), gender (P = .423), or racial distribution (P = .235) between patients undergoing POEM versus HM (Table 1). A similar distribution in gross yearly income and insurance coverage was noted in our study population, with a majority of Medicare beneficiaries and Private Insurance among individuals undergoing POEM (Medicare 44.8%, Private insurance: 41.1%) and HM (Medicare 41.6% Private insurance 44.6%) (P < .001). While POEM was mainly performed in the Northeast (33.5%) and Southern (33.2%) U.S. regions, HM was predominant in the Southern U.S. regions (39.6%). Both procedures were performed mainly in large-sized (POEM: 96.1%, HM: 88.9%, P < .001) and teaching hospitals (POEM: 84.4%, HM: 70.4%, P < .001). A similar distribution of the comorbid conditions was seen between patients undergoing POEM and HM (Table 1).
Baseline Characteristics of Patients Undergoing Per-Oral Endoscopic Myotomy (POEM) Versus Heller Myotomy (HM) From 2016 to 2020.
Trends in POEM and HM From 2016-2020
From 2016 to 2020, we noted an increase in POEM usage from 6.2% to 10.1% and a decrease in HM from 48.8% to 40.7% (Figure 1) (Supplemental Table 1). Among hospitalizations for achalasia, a 7% increase in discharges from teaching hospitals was observed from 2016 to 2020. From 2016 to 2020, our population was progressively older by 2.1 years, with a 7% increase in patients with CCI of 3 or more (Supplemental Table 2).
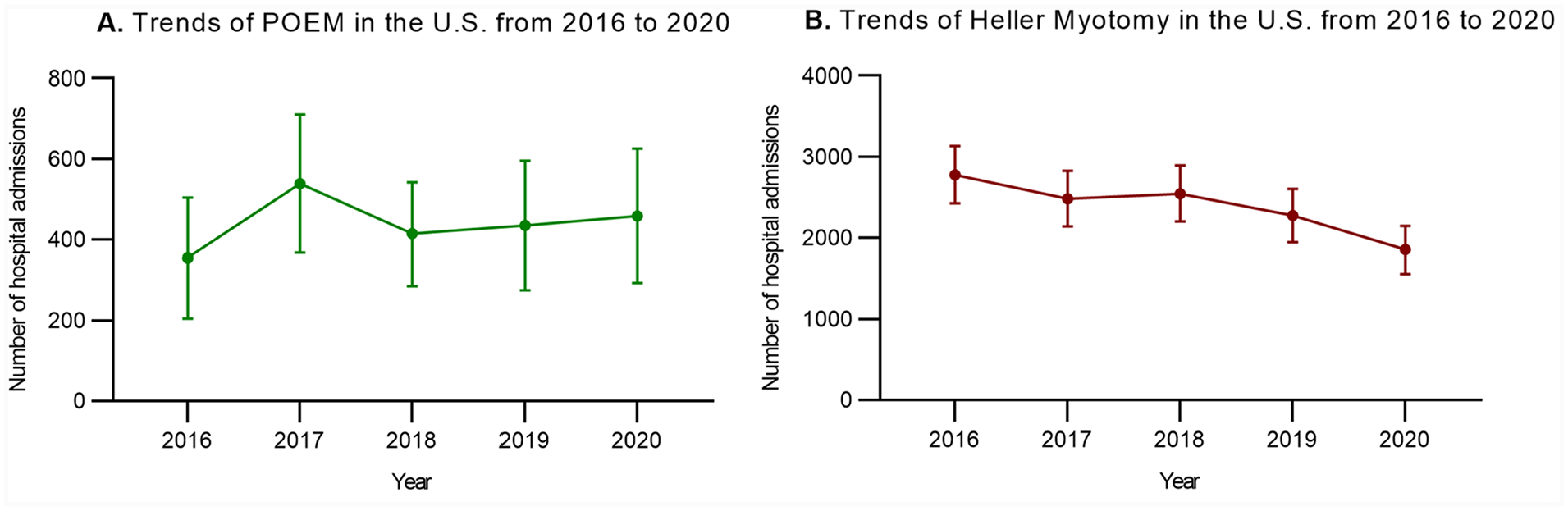
Trends of discharges of patients with a primary diagnosis of achalasia and undergoing Per-Oral Endoscopic Myotomy (POEM) versus Heller Myotomy (HM) from 2016 to 2020. Increased rates of POEM (A) and decreased rates of HM (B) were observed from 2016 to 2020. (A) Trends of POEM in the U. S. from 2016 to 2020. (B) Trends of Heller Myotomy in the U. S. from 2016 to 2020.
Outcomes of POEM Versus HM
When comparing POEM versus HM from 2016 to 2020, our analysis did not show any statistically significant change in the LOS (adjusted Mean difference [aMD] = −0.27 day, 95% CI: −0.79 to 0.24) or THC (aMD = −701 U.S. dollars, 95% CI: −9292 to 7888) (Table 2). Pertaining to procedural complications, when compared to POEM, HM was associated with a statistically significant decrease in the risk of pneumonia (adjusted Odds Ratio [aOR] = 0.09, 95% CI: 0.02-0.41), pneumoperitoneum (aOR = 0.11, 95% CI: 0.03-0.36), pneumomediastinum (aOR = 0.21, 95% CI: 0.06-0.68), with no difference in the risk of esophageal perforation (aOR = 1.33, 95% CI: 0.27-6.48) and sepsis (aOR = 2.04, 95% CI: 0.22-18.40). No cases of mortality or gastrointestinal bleeding were noted in the POEM group (Table 3).
Summary of the Procedures and Outcomes of Patients Admitted With Achalasia From 2016 to 2020.
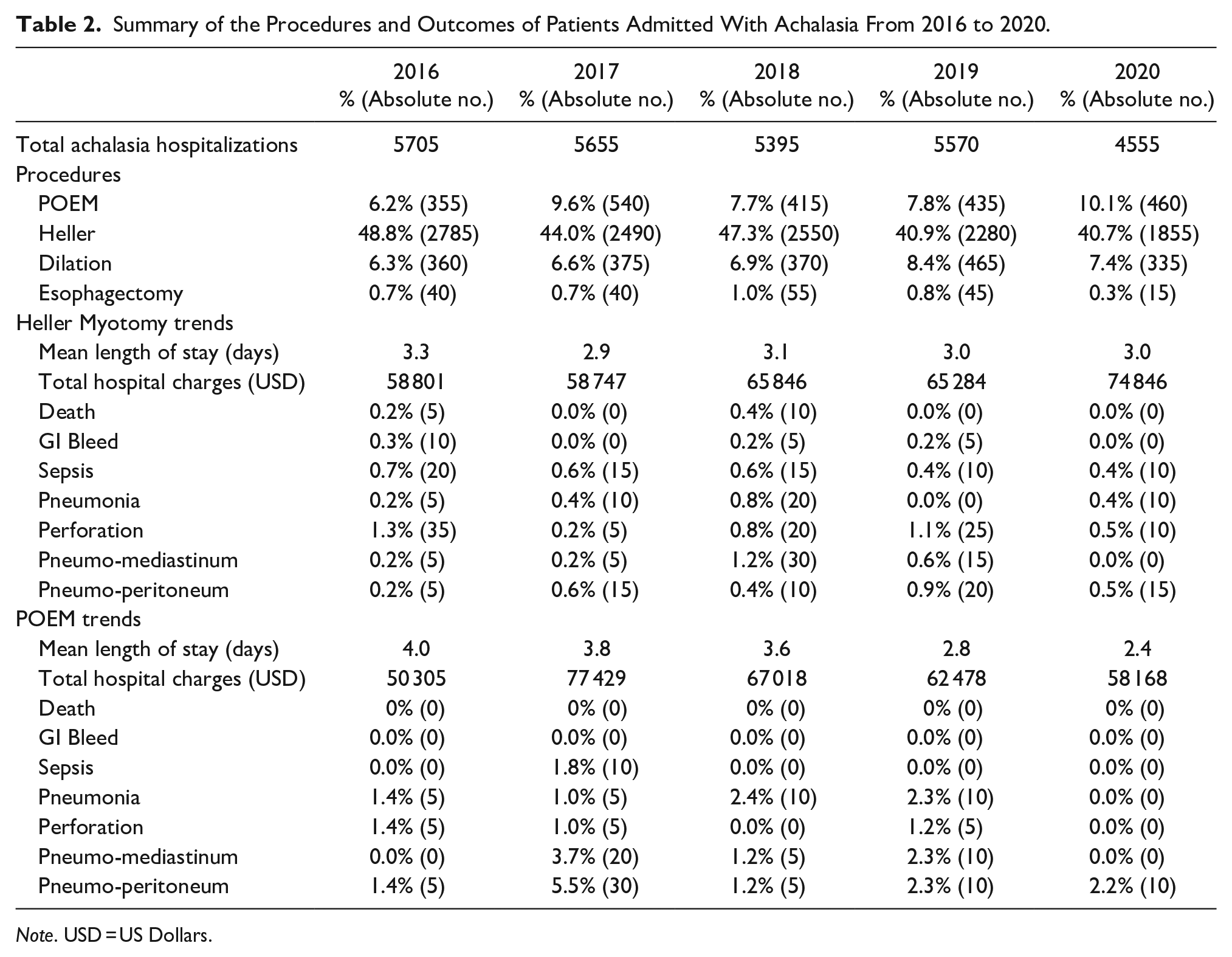
Note. USD = US Dollars.
Comparison of Heller Myotomy (HM) Versus POEM Outcomes From 2016 to 2020.
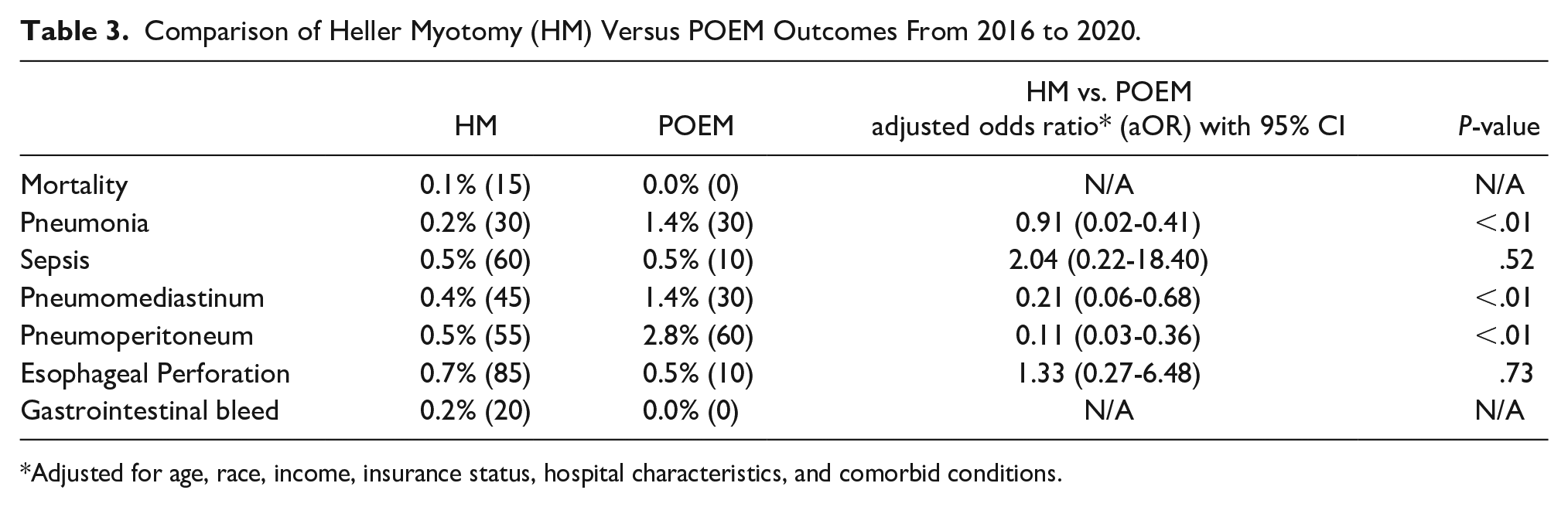
Adjusted for age, race, income, insurance status, hospital characteristics, and comorbid conditions.
Discussion
Our data shows that POEM usage has been increasing and HM usage has been decreasing for the treatment of achalasia. This trend is not surprising since POEM is less invasive than surgical HM, despite being performed mostly laparoscopically. 9 These data also show that both POEM and HM are performed mainly at teaching and large hospitals (96.1% for POEM vs 88.9% for HM, P < .001), which is expected given the complexity of these procedures and the necessary persistent volume for the operators of both procedures to maintain a high level of skills required for these procedures. POEM was mainly performed in the Northeast (33.5%) and Southern (33.2%) U.S. regions while HM was predominantly performed in the Southern U.S. regions (39.6%). A prior nationwide retrospective study from 2013 to 2017 showed that the prevalence of high-resolution esophageal manometry laboratories is the highest in the Northeast, thus explaining the highest percentage of POEMs performed was in the Northeast. 24 However, this study showed that the Southern U.S. region had the fewest centers, which might indicate a recent change in the number of POEM centers in the U.S.
Pertaining to complications, we noted that pneumonia, although uncommon, was seen more with POEM than HM. Achalasia patients are at risk of pneumonia from aspiration, and it is difficult to make a conclusion based on these data if the risk of pneumonia is higher with POEM. Additionally, the incidence of pneumoperitoneum and pneumomediastinum was higher in POEM, which is consistent with previous studies.27-29 Pneumoperitoneum and pneumomediastinum are now considered normal radiological findings post-POEM and as long as there is no evidence of leak or change in clinical status, these findings bear no clinical significance postoperatively and do not require any intervention.27-29 Overall, POEM remains a safe procedure 30 with a safety profile comparable to that of HM. 31
The trend in the number of POEMs increased from 2016 (6%) to 2020 (10%). In contrast, a downward trend was observed in discharges following HM from 2016 (49%) to 2020 (41%). Trieu et al described similar results in a previous nationwide retrospective analysis of achalasia hospitalizations in the U.S. 24 POEM is still considered a new procedure and requires high endoscopic skills and an in-depth understanding and knowledge of the complexity of performing such a procedure including any complication that may arise either during the procedure or postoperatively. This trend is expected to continue as more providers, whether gastroenterologists or surgeons are trained to perform POEM and patients seem to prefer POEM as a non-surgical intervention. Additionally, a same-day discharge appears safe, especially for uncomplicated procedures, and this can lead to significant cost reduction.32,33
Our study has several strengths. Using the NIS, we studied a large population sample of 2815 admissions for POEM and 15 745 admissions for HM, which confers this study adequate power to evaluate the differences in hospital utilization, total healthcare charges, mortality, and complications associated with both procedures. Additionally, the NIS helps to limit the occurrence of reporting bias, which is often found in single-center studies. Further, the validity of our results has been confirmed by previous literature. However, there are some limitations inherent to the study design. The NIS database is an administrative database used to identify diagnoses and procedures with ICD codes. Therefore, a potential over- or under-coding of our variables may have occurred. Moreover, as pointed out earlier, there is a recent trend of same-day discharge of POEM patients postoperatively, which may have underrepresented the total number of POEM procedures performed for achalasia. In addition, the suspension of all elective procedures during the COVID-19 pandemic may have skewed the trends seen in 2020. Last, the NIS does not account for patients but for admissions, therefore one individual can account for multiple admissions.
In conclusion, the use of POEM remains inferior to that of HM, which is likely related to the lack of trained providers to perform such a procedure that requires advanced skills. Additional training of gastroenterologists and surgeons to perform POEM will likely lead to POEM being the main procedure performed to treat achalasia and may significantly decrease the cost associated with achalasia treatment.
Supplemental Material
sj-docx-1-gut-10.1177_26345161231202957 – Supplemental material for Healthcare Utilization, Costs and Other Outcomes of Peroral Endoscopic Myotomy (POEM) Versus Heller Myotomy in the Inpatient Management of Achalasia in The United States: A 2016 to 2020 Nationwide Study
Supplemental material, sj-docx-1-gut-10.1177_26345161231202957 for Healthcare Utilization, Costs and Other Outcomes of Peroral Endoscopic Myotomy (POEM) Versus Heller Myotomy in the Inpatient Management of Achalasia in The United States: A 2016 to 2020 Nationwide Study by Yassine Kilani, Mohammad Aldiabat, Maryam Mubashir, Saqr Alsakarneh, Ammar Arif Vohra, Yazan Aljabiri, Falak Hamo, Fnu Vikash, Vikash Kumar and Salih Samo in Foregut
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Salih Samo: Castle Biosciences-speaker bureau and advisory board. Sanofi-speaker. The rest of the authors: none declared.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.