
Abstract
Background:
Proton pump inhibitors (PPIs) are highly effective in treating gastroesophageal reflux disease (GERD). However, persistent, troublesome reflux symptoms despite PPI use are common, and a proportion of individuals with these persistent symptoms is considered to have refractory GERD (rGERD). There are limited data on patients’ experience with persistent reflux-like symptoms to guide healthcare professionals in managing this troublesome condition.
Methods:
An international, population-based, online survey was conducted among adults who reported persistent reflux-like symptoms; 24 questions were posed regarding the participants’ symptoms, diagnosis, treatment, and comorbid conditions. Descriptive analyses were performed to characterize participants’ experience with diagnosis and their satisfaction with treatment. All data were self-reported.
Results:
Of 565 initial respondents, 283 (51%) answered the question regarding being formally diagnosed by a healthcare professional with GERD and/or rGERD. The 197 (70%) participants who answered “yes” made up the survey population. Heartburn (65%) and acid regurgitation (62%) were the most common troublesome symptoms. PPI use was reported by 145 (74%) respondents, but only 30% were satisfied with PPI therapy. The most common alternative therapies included antacid/alginates (63%), histamine H2-receptor antagonists (33%), mucosal protectants (25%), and lifestyle modifications (84%).
Conclusions:
In this population-based survey, nearly one-third of participants with persistent reflux-like symptoms had not received a formal diagnosis of GERD or rGERD. Although most participants diagnosed with GERD/rGERD had received PPI therapy, persistent symptoms, dissatisfaction with PPI therapy, and concerns about long-term PPI use were common. These data emphasize the need for patient input when developing management strategies for GERD and persistent reflux-like symptoms or rGERD.
Keywords
Key Learning Points
Approximately 30% of survey respondents with persistent reflux symptoms had not received a formal diagnosis of GERD or rGERD
Few respondents were satisfied with PPI therapy, as persistent symptoms and concerns relating to long-term use were prevalent
Inadequate response to PPI therapy and opportunities for dose optimization may be under-recognized in clinical practice
Introduction
Gastroesophageal reflux disease (GERD) is highly prevalent, affecting 10% to 12% of the population, 1 and persistent symptoms have been reported by as many as half of patients taking a daily proton pump inhibitor (PPI). 2 In the US, it is estimated that gastrointestinal diseases result in millions of healthcare visits, hospitalizations and procedures, costing billions of dollars annually. 3
In clinical practice there is some confusion around the definition of refractory GERD (rGERD) in terms of symptom frequency and severity or the dose and duration of PPI therapy among patients who have persistent symptoms. 4 A survey of 113 practising clinicians found that both gastroenterologists (GIs) and non-GIs use very imprecise definitions of rGERD, with GIs being more consistent than non-GIs. 4 Further complicating the diagnosis is the fact that reflux-like symptoms have limited specificity for the diagnosis of GERD, thus escalation of reflux therapy may not necessarily improve symptoms. 5 Treatment is also a challenge, in terms of defining the optimal treatment for symptoms of rGERD in patients with or without evidence of persistent reflux, and those with non-acid reflux.
Guidelines (Canadian Association of Gastroenterology [CAG], American College of Gastroenterology [ACG] and the European Society for Neurogastroenterology and Motility [ESNM]/American Neurogastroenterology and Motility Society [ANMS]) recommend that PPI therapy for typical reflux symptoms be initiated with once daily PPI therapy for 8 weeks and, in the absence of alarm features, escalated to twice daily (BID) PPI therapy for a further 8 weeks.6-8 A pragmatic definition of rGERD is, then, the persistence of typical reflux-like symptoms despite at least 16 weeks of PPI therapy, including at least 8 weeks of BID PPI therapy. However, the most recent guidance from the ACG 7 proposes that investigations be considered in individuals whose symptoms have not resolved after once daily PPI therapy for 8 weeks. There is some question of whether investigations are warranted before a trial of twice-daily PPI therapy. A study comparing optimized medical therapy against anti-reflux surgery for rGERD reported low recruitment numbers, in part because many patients did, in fact, improve when their treatment regimen was optimized. 9 This leads to confusion regarding the definition and implications of rGERD on the part of health care providers.
There is little information on the experiences and attitudes of patients with persistent reflux symptoms regarding whether or not they may be considered to have rGERD or how their symptoms have been managed. There is, therefore, a need to understand persistent reflux-like symptoms, regardless of whether the patient is considered to have rGERD, when developing evidence-based management strategies for rGERD. Because there are limited, high quality studies in this area, GRADE-based recommendations on the management of rGERD are, necessarily, “weak” or “conditional” 10 and it is, therefore, critical that the discussions of consensus groups account for patient experiences and preferences.
Regardless, persistent reflux-like symptoms despite PPI therapy have a substantial impact on patient quality of life. 11 Because symptoms are a subjective and personal experience, data on patient perspectives are esssential to help guide management.
The International Working Group for the Classification of Oesophagitis (IWGCO) and the International Foundation for Gastrointestinal Disorders (IFFGD) conducted an international survey to evaluate the experiences and attitudes of adults with GERD or rGERD. The purpose of this survey was to understand the experiences of patients with respect to the nature and duration of their persistent GERD or reflux-like symptoms symptoms in relation to other GI diagnoses, investigations and treatments, and to explore their concerns regarding treatment options. Such data can help increase awareness around the needs of these patients and help identify relevant topics that should be addressed in a consensus guideline on the management of rGERD.
Methods
The initial survey questions were developed by DA, PSi, and PSh with the help of IFFGD staff members. The survey questions were developed based on a literature search conducted for an evidence based consensus process on the management of rGERD to elucidate patient perceptions and experiences with regard to the diagnosis and treatment of persistent reflux-like symptoms to inform the consensus process.
The home page of the survey (https://aboutgerd.org/research-news/refractory-gastroesophageal-reflux-disease-rgerd-survey) provided a description of GERD (most common symptoms are heartburn and/or regurgitation) and rGERD (persistent symptoms despite lifestyle changes and PPI treatment) (Online supplemental 1). The questionnaire included 24 questions and was designed to assess all stages of the journey of patients with a GERD or rGERD diagnosis who reported persistence of reflux-like symptoms despite therapy, including their symptoms and diagnosis, use of PPI and other therapies, comorbid conditions, and testing. All data were self-reported and no diagnostic testing was performed for this survey. Consent to use de-identified information was obtained.
Surveys were included in this analysis if the participant answered, “Have you been formally diagnosed by a healthcare professional with GERD and/or rGERD?” The numbers and percentages of participants who responded affirmatively to each question or sub-question were tabulated for descriptive analyses.
Results
Between June 30, 2021 and November 15, 2021, 565 individuals responded to the survey invitation. Of these 283 responded to the question, “Have you been formally diagnosed by a healthcare professional with GERD and/or rGERD?” and provided informed consent. This included 197 respondents who indicated “yes,” 68 who indicated “no,” and 18 who indicated “do not recall.” The group of 197 (69.6%) who indicated that they had a formal diagnosis of GERD and/or rGERD from a healthcare professional constituted the overall study population for this survey. Most of the respondents were from North America (63%), with a further 15% from Asia, 13% from Europe, 5% from Australia/New Zealand, and 4% from Africa. Data on age and gender were not collected.
Respondents had received their diagnosis either within the previous 3 years (37%), 3 to 10 years ago (32%), or more than 10 years ago (31%). Only 21% had been diagnosed with GERD/rGERD within the previous year. Most respondents were receiving treatment from a gastroenterologist (62%) or a primary care physician (PCP; 63%), including 32% of respondents who were being treated by multiple professionals. Only 9% reported self-managing their symptoms “with over-the-counter (OTC) medication without help from a healthcare professional.”
When asked to choose their 3 most troublesome symptoms, heartburn (65%), and acid regurgitation (62%) were the most common selections, but patients also frequently endorsed dysphagia-like symptoms such as “a feeling of food getting stuck” (37%) or “difficulty swallowing” (26%). Among “any symptoms,” 51% reported dysphagia-like symptoms. Other common symptoms are shown in Figure 1.
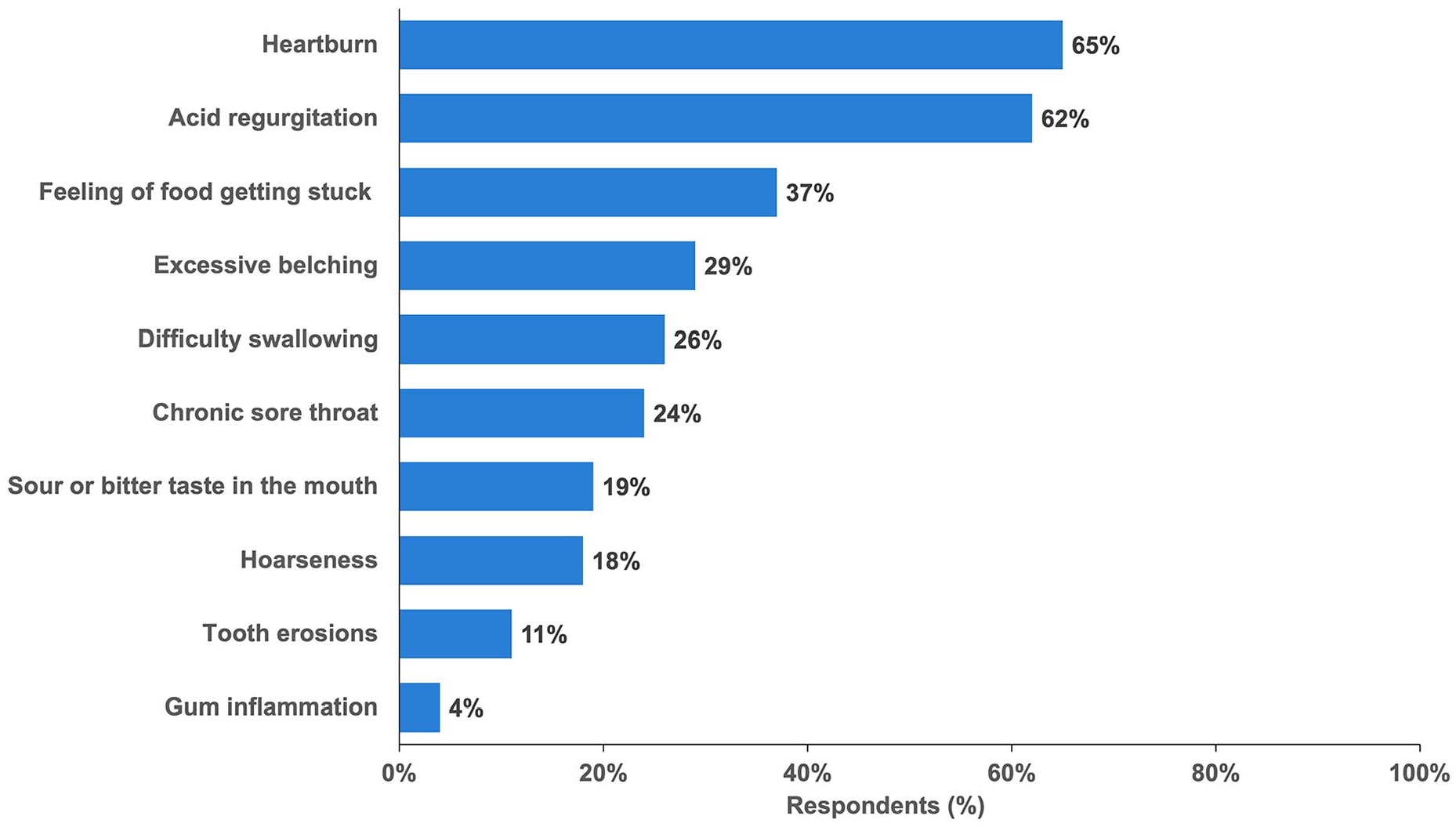
Most common troublesome symptoms reported by respondents (n = 197).
Among those diagnosed with GERD/rGERD, 145 (74%) reported using a PPI for their symptoms. Among 36 respondents who stated that they were not using a PPI, the main reasons were that they were never recommended by a healthcare provider (28%), or that they had been tried but discontinued due to side effects (25%) or lack of efficacy (25%).
The dosing frequency among the 145 patients who stated that they currently use a PPI is shown in Figure 2. Most respondents were taking prescribed PPIs (119/145, 82%), either alone or in combination with an OTC PPI, while 17% of respondents stated they were taking only an OTC PPI (Figure 3).
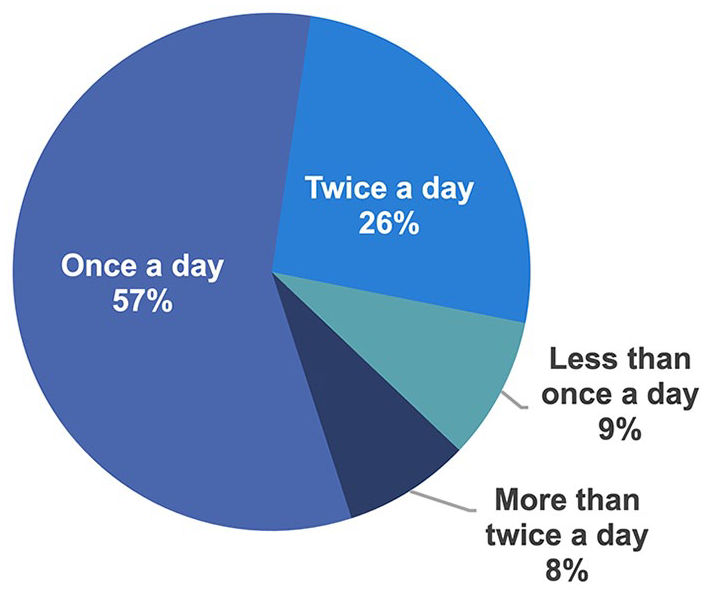
Frequency of PPI use among respondents stating they use a PPI for rGERD symptom control (n = 145).
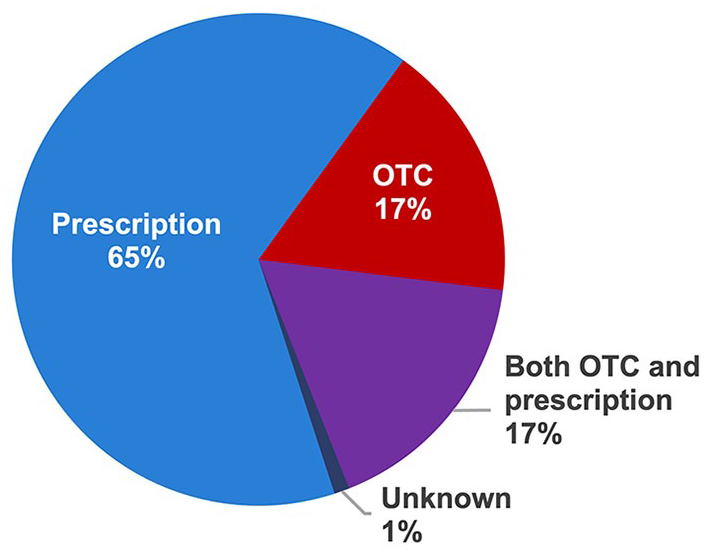
PPI source among respondents stating they use a PPI for rGERD symptoms (n = 145).
Less than 30% of respondents stated that they were satisfied with how well their PPI treats their troublesome refractory reflux symptoms, irrespective of dosing frequency (Figure 4).
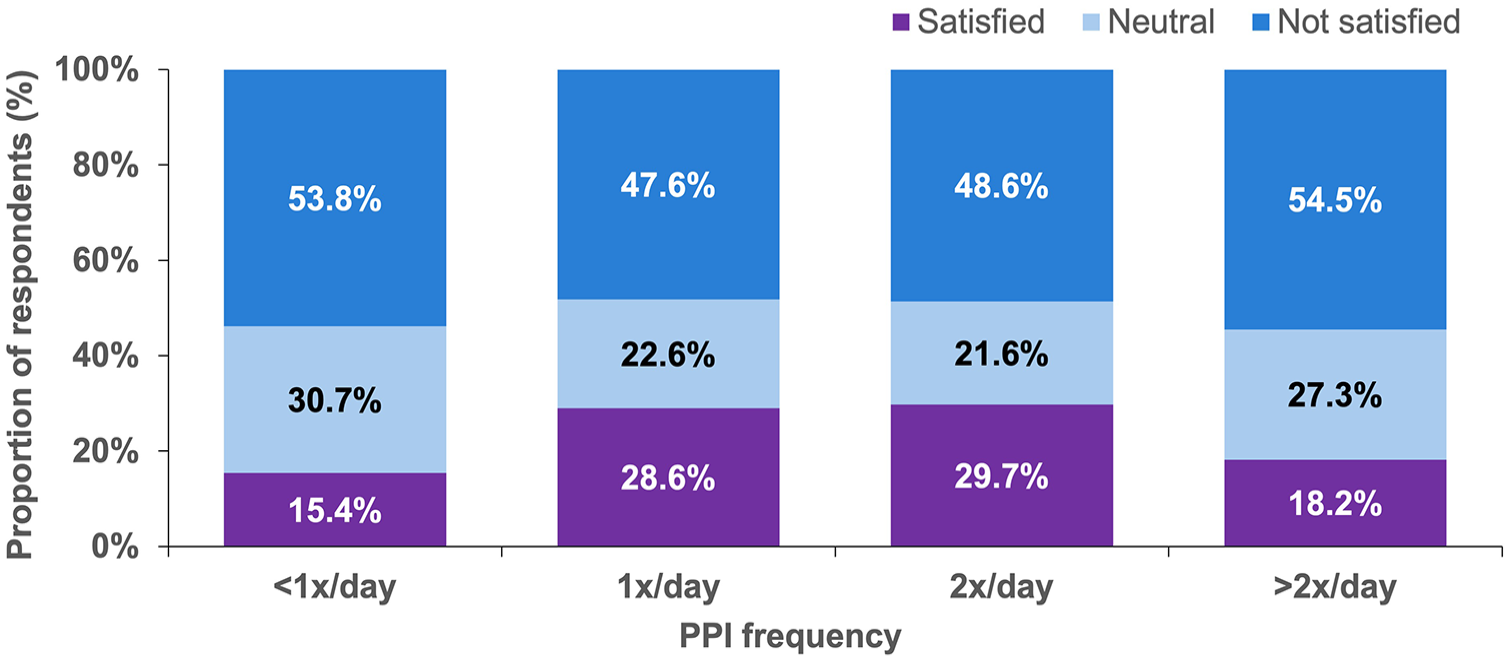
PPI satisfaction with how well their PPI treats their troublesome refractory reflux symptoms among respondents stating they use a PPI for rGERD symptoms (n = 145).
When respondents with a diagnosis of GERD/rGERD (n = 197) were asked about their concerns relating to rGERD and its treatment, 3 of 4 respondents agreed that they were concerned with leaving their symptoms untreated. Many respondents were also concerned with the potential long–term effects of PPI use (70%), side effects of their rGERD medication (63%), and risks of undergoing a surgical treatment (63%).
Among respondents with a diagnosis of GERD/rGERD who were taking a PPI (n = 145), 69% had concerns regarding the potential long-term effects of PPIs, ranging from 80% among those who were not satisfied or neutral regarding the effect of PPI therapy on their troublesome symptoms compared to 67% among those who were satisfied (P > .05). Similarly, concerns about all rGERD medication side effects were reported by 75% of respondents who were not satisfied or neutral regarding their PPI therapy compared to 64% of those who were satisfied (P > .05).
Respondents with a GERD/rGERD diagnosis frequently took alternate medications, including antacid/alginates (63%), histamine H2-receptor antagonists (33%), mucosal protectants (25%), and prokinetics (18%). Most respondents (84%) had also tried various lifestyle modifications, including diet therapy (58%), raising the head of the bed (55%), and adjusting the timing of meals (49%). The use of alternate medications was comparable for respondents using PPIs: antacid/alginates (73%), histamine H2-receptor antagonists (36%), mucosal protectants (26%), and prokinetics (20%).
Comorbidities (as diagnosed by a HCP) were common among the 197 respondents with a GERD/rGERD diagnosis, particularly stress/anxiety (39%), followed by irritable bowel syndrome (29%), and constipation (28%) (Table 1).
Healthcare Provider-Diagnosed Comorbidities Among Respondents With a GERD/rGERD Diagnosis (n = 197).
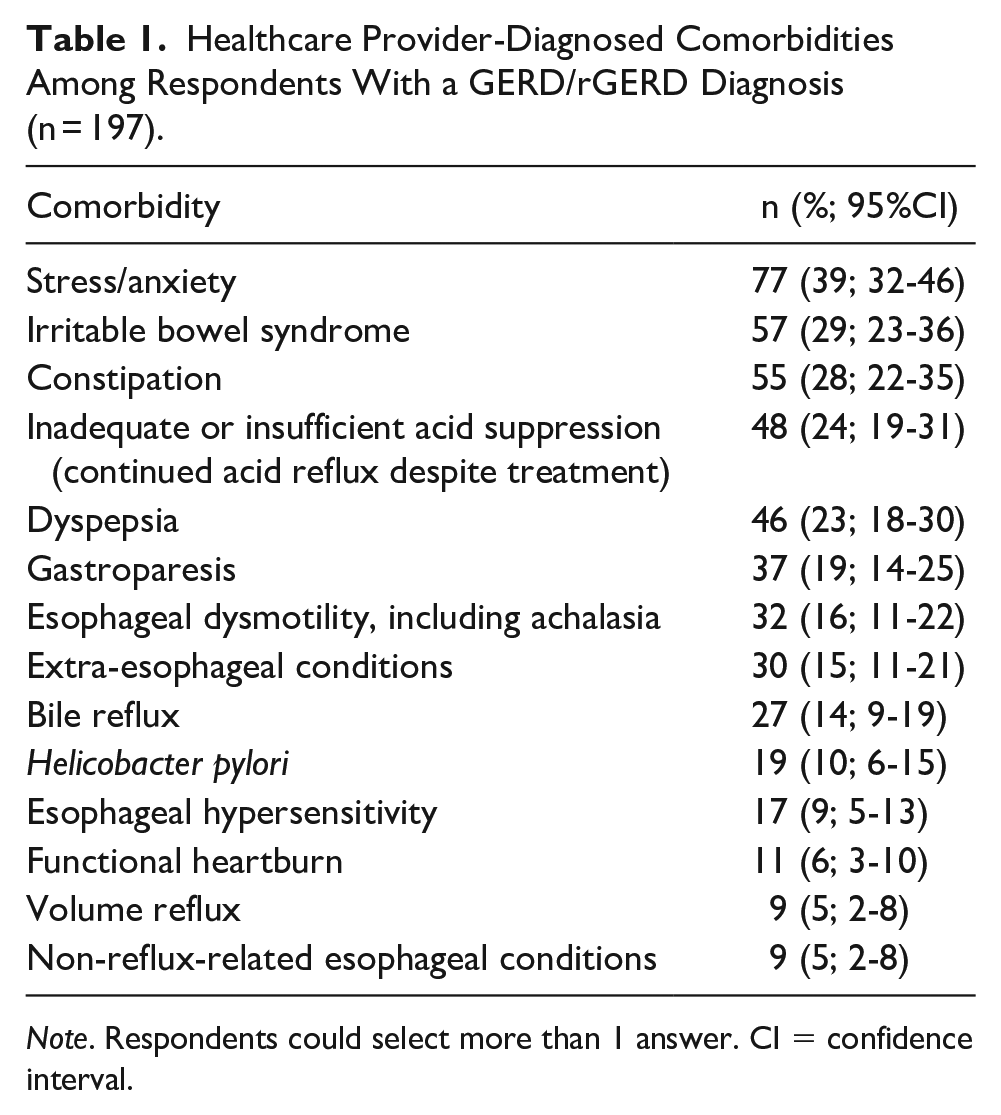
Note. Respondents could select more than 1 answer. CI = confidence interval.
Of respondents with a GERD/rGERD diagnosis, 74% indicated that they had undergone some testing. The most common test was an upper endoscopy (67%) (Figure 5). Esophageal manometry was used infrequently with only 17% of patients reporting this test. Similarly, only 13% of respondents indicated they had undergone esophageal pH testing on PPI, off PPI or both. Over half of respondents reported having had multiple tests.
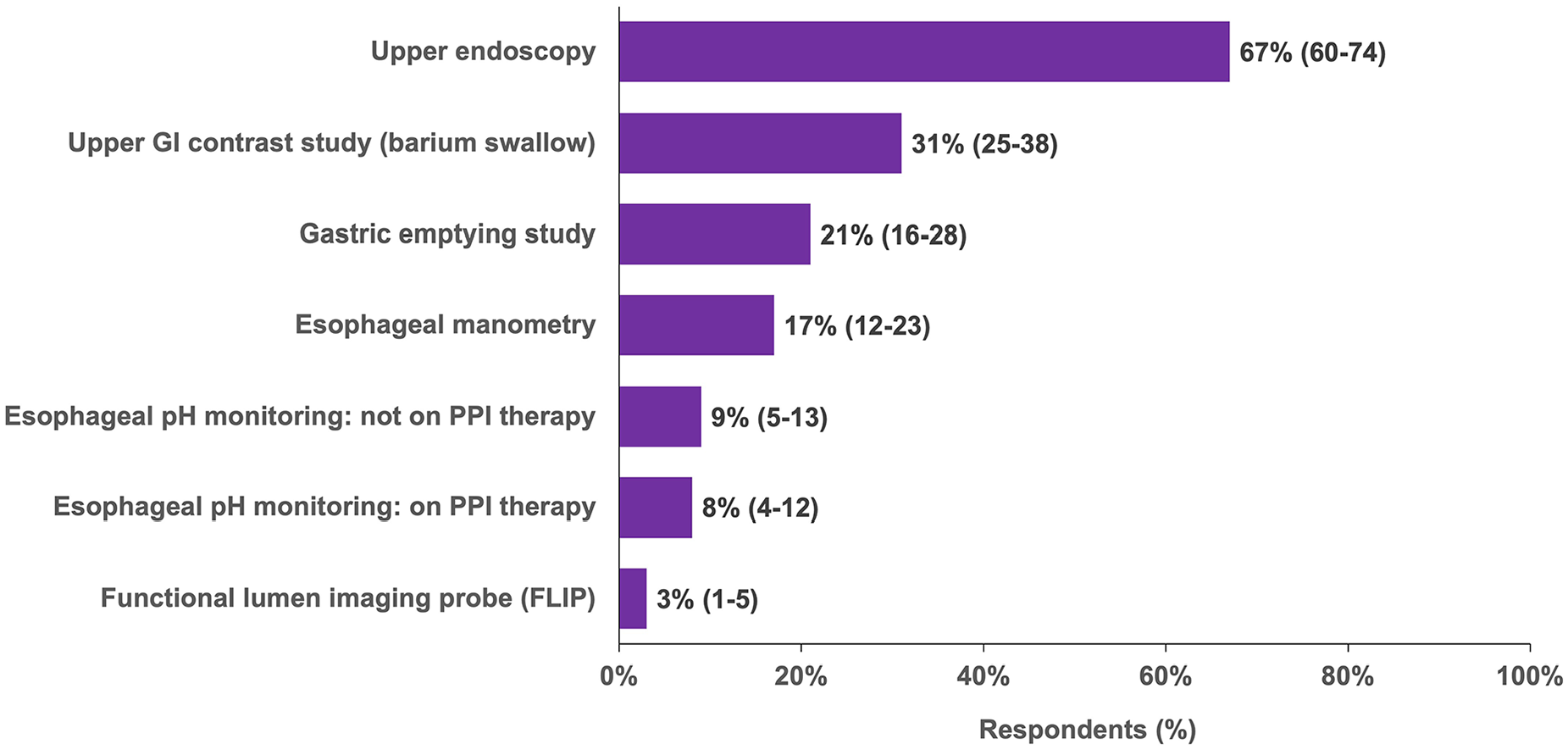
Prior testing undergone by survey respondents with an rGERD diagnosis (n = 197) (%, 95% CI).
Discussion
This survey of 197 respondents who self-reported being diagnosed with GERD or rGERD included 145 (74%) patients treated with a PPI. Most of these respondents were taking prescribed PPIs (82%), and despite a low rate of patient satisfaction (30%) with how well their PPI treated their troublesome refractory reflux symptoms, only one-third of patients were taking a PPI more than once daily. A prior international survey of patients with GERD conducted in 2005 found similarly low rates of satisfaction with prescribed therapy, with only 36% of patients reporting being asymptomatic. 12
The low rate of patient satisfaction, and low rates of dose escalation, coincide with surveys which suggest that clinicians may under-recognize an inadequate response to PPI therapy in real-world clinical practice. 4 It is also possible that the clinicians may under-appreciate the fact that a once-daily PPI does not produce adequate acid suppression in all individuals, 13 attributable, in part, to interindividual differences in efficacy among PPIs.14,15 The low rates of dose escalation cannot be explained by the duration of GERD, since almost 80% of respondents had been diagnosed with GERD/rGERD more than 1 year prior. Indeed, a previous patient survey found that patients had already suffered GERD symptoms for a mean of more than 1.5 years before consulting a physician. 11 In this survey, even many of those who were on BID PPI or higher were not satisfied, so satisfaction rates did not appear to be related to the dosing of PPI. This raises the issue of whether the diagnosis of GERD/rGERD was accurate, as well as questions around whether patients were instructed in the appropriate use of PPIs and their level of adherence.
Although the majority of respondents reported undergoing diagnostic testing, manometry and pH studies were infrequently endorsed. This may be due in part to patient unfamiliarity with the type of testing they are undergoing. However, it is of concern because these tests may be helpful in identifying other diagnoses such as rumination syndrome, functional esophageal disorders, and motility disorders.6,7 In fact, respondents frequently chose dysphagia-like symptoms, and excessive belching among their top 3 most troublesome symptoms suggesting that additional testing might have been informative.
In this survey, respondents with a diagnosis of GERD/rGERD taking a PPI had high rates of concern around the potential long-term effects of PPI use (69%) and the side effects of their rGERD medication (77%). The rates of concern were higher among respondents using PPIs who were not satisfied or neutral regarding how well their PPI treated their troublesome symptoms compared with those who were satisfied. A US survey also found that patients with GERD who were highly satisfied were less likely to worry about long-term medication use. 16 Other surveys have also reported high rates of concern among PPI users. In one survey, almost 80% of GERD patients were at least slightly concerned about adverse effects, and 46% were somewhat or extremely concerned, 17 while another survey found that 16% were “extremely concerned” about adverse events. 17 This is important because concerns about PPIs have been associated with attempts at discontinuation without a physician’s recommendation, and discontinuations increased in association with increasing levels of patient concern.17,18 In one survey, patients with concerns about long-term side effects were more than twice as likely to make changes to their PPI use, often without physician input, compared to patients who did not express concerns. 19
This survey found that respondents with GERD/rGERD using PPIs had frequently tried other medications, including antacid/alginates (73%), histamine H2-receptor antagonists (36%), mucosal protectants (26%), and prokinetics (20%). Similarly, other surveys have found that 50% to 60% of patients with GERD required multiple GERD-related medications to manage their symptoms.20,21
Some limitations of this survey include the fact that all data were self-reported and no diagnostic testing was performed for this survey. Respondents were asked initially if they had ever been diagnosed with GERD or rGERD, with no separation of the 2 diagnoses. However, the invitation to complete the survey did ask potential participants if they suffered from rGERD, and a simple definition was given. Because we restricted our report to the respondents who indicated that they had been diagnosed by a healthcare professional, these patients should reflect the variable definitions used by the medical community for rGERD. In addition, the high rates of dissatisfaction with PPI therapy, despite continued use, would suggest many respondents did in fact have rGERD. The survey, intentionally, did not examine the effects of different PPIs; data on the type and dose of individual PPIs were not collected as this would have complicated the survey and respondent numbers would have been insufficient for meaningful interpretation. Finally, the survey did not ask for patient age or gender, which can affect the response to PPI therapy, and PPI-associated adverse effects may be of more concern in some patient groups.22,23 This was an oversight, but does not invalidate the observation of marked variability in the management strategies reported in this study.
Summary
Many patients with self-reported GERD receiving PPI therapy do not have fully controlled symptoms and are not satisfied with their therapy. Patients have high levels of concern about the long-term use of PPIs and the side effects of GERD medications. This concern often leads to patients changing or stopping their therapy without discussions with their physicians. Surveys have found that patients often report that their healthcare providers had not discussed the potential risk of adverse events of PPIs before initiation of therapy.18,19
This survey confirms the ongoing dissatisfaction with PPIs and GERD therapies, dissatisfaction being reported by 70% of patients who had a self-reported formal diagnosis of GERD or rGERD and were taking a PPI. Patients continued to report troublesome reflux symptoms (70%) and concerns around long-term PPI use (69%) and side effects (77%). This underscores the need for better management strategies, patient education, and the importance of the physician-patient alliance in managing GERD and rGERD.
Supplemental Material
sj-pdf-1-gut-10.1177_26345161231173643 – Supplemental material for Symptom Profile, Proton Pump Inhibitor Therapy, and Diagnostic Testing in Patients With Persistent Reflux-Like Symptoms: Results From a Population-Based Survey
Supplemental material, sj-pdf-1-gut-10.1177_26345161231173643 for Symptom Profile, Proton Pump Inhibitor Therapy, and Diagnostic Testing in Patients With Persistent Reflux-Like Symptoms: Results From a Population-Based Survey by David Armstrong, Sachin Srinivasan, Ceciel Rooker, Paul Sinclair, Emily Taylor and Prateek Sharma in Foregut
Supplemental Material
sj-pptx-2-gut-10.1177_26345161231173643 – Supplemental material for Symptom Profile, Proton Pump Inhibitor Therapy, and Diagnostic Testing in Patients With Persistent Reflux-Like Symptoms: Results From a Population-Based Survey
Supplemental material, sj-pptx-2-gut-10.1177_26345161231173643 for Symptom Profile, Proton Pump Inhibitor Therapy, and Diagnostic Testing in Patients With Persistent Reflux-Like Symptoms: Results From a Population-Based Survey by David Armstrong, Sachin Srinivasan, Ceciel Rooker, Paul Sinclair, Emily Taylor and Prateek Sharma in Foregut
Footnotes
Acknowledgements
The authors would like to thank Pauline Lavigne and Steven Portelance (unaffiliated) for contributions to writing, and editing the manuscript.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Armstrong: Institutional research grants from Nestlé Health Sciences, Canadian Association of Gastroenterology, and Weston Family Foundation; consultant fees from Canadian Partnership Against Cancer; payment or honoraria for lectures from Vitaris and Takeda; support for meeting attendance from the European Commission Initiative on Colorectal Cancer; patents for AI VALI Inc.; advisory board participation for Cinclus Pharma, Phathom Pharma, and Takeda Canada; and served as President of the Canadian Association of Gastroenterology, Treasurer of the International Working Group Classification Esophagitis, and board member of the Canadian Digestive Health Foundation.
Srinivasan: None
Rooker: None
Sinclair: None.
Taylor: None
Sharma: Grants or contracts from Cosmo Pharmaceuticals, Covidien, Salix, Fujifilm Holdings America Corporation, Medtronic USA, Inc. Docbot, ERBE USA, Inc., Olympus, US Endoscopy Ironwood Pharmaceuticals, Inc.; and consulting fees from Bausch, Boston Scientific Corporation, Exact Sciences, Lucid, Lumendi, Medtronic, CDx Labs, Covidien LP, Fujifilm Medical Systems USA, Inc.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Institutional Review Board approval was not required.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.