
Abstract
Introduction
The most recent statistics published by the Office of National Statistics report that 2.1 million people experienced domestic violence and/or abuse (DVA) between 2022 and 2023 (Office of National Statistics, 2023). It is estimated that men in the UK kill one woman every 3 days (Femicide Census, 2021). Reliable data on global trends of DVA is difficult to come by. In a 2018 report, the United Nations (UN) estimated around one in three women globally have experienced DVA (United Nations, 2018). In a later report, the UN estimated that 47,000 women and girls were killed in 2020 by an intimate partner or another family member, equating to a woman or girl being murdered every 11 minutes by a family member. These figures indicate the immense scale of DVA worldwide and its potentially lethal impact.
The potential impacts of DVA are varied and highly specific to each instance. However, there is a range of literature outlining the potential impacts of DVA. There are various potential physical health impacts. There is an increased risk of: traumatic brain injury due to blows to the head (Cimino et al., 2019; Costello and Greenwald, 2022); reproductive health issues from physical or sexual assault (Amel Barez et al., 2022; Sarkar, 2008); death via murder and conditions with high risk of mortality associated with chronic stress such as heart disease (Chandan et al., 2019, 2020; Koenraadt, 2018). Psychological impacts can include increased risk of poor mental health in general but particularly high likelihood of PTSD, anxiety, depression, poor self-esteem, disrupted attachment and increased risk of suicide (Herman, 2015; Humphreys and Thiara, 2003; Munro and Aitken, 2020). Social impacts can include ongoing financial issues, housing issues and social stigma (Conner, 2013; Galántai et al., 2019; Murvartian et al., 2023). In summary, DVA has many potential impacts with life altering or life ending consequences. The researcher will further define and contextualise the usage DVA and other commonly associated language within the ‘Epistemology and Language’ section of this paper. This includes transparency as to the researcher considerations of gendered violence and of how power operates within the UK socio-political context.
Ways of understanding
With DVA so common and the potential impact of DVA appearing so harmful this invites consideration of how we might make sense of the impact of DVA. There are many ways in which those could be conceptualised but perhaps some of the most broadly utilised, particularly by health and social care are attachment theory, intergenerational trauma theory and Adverse Childhood Experience’s (ACE’s) literature.
Attachment theory offers a structure as to how early relationships can influence later relationships. Early attachment theory focussed on parental, particularly maternal, interactions with children and how this influenced their function throughout life. (Ainsworth, 1978; Ainsworth and Bowlby, 1991; Bowlby, 1979). Disruption of this relationship early on was theorised to lead to ‘impairments’ in cognition, self-identity development, emotional regulation and social skills. Critique has emerged of its efficacy for collectivist cultures and its portrayal of how fixed attachment style may be (Fraley and Shaver, 2008; Lee, 2003). Other models of attachment have been suggested, perhaps the most prominent contemporary model is the Dynamic-Maturation Model of Attachment (DMM) which integrates several ideas (Crittenden, 2006). The DMM addresses many of the shortcomings of early attachment theory but has only been introduced to practice comparatively recently but has a growing evidence base (Crittenden, 2011; Crittenden et al., 2021; Spieker and Crittenden, 2018).
Intergenerational trauma highlights that trauma can be transferred through generations of a family whether that is judged to be through epigenetics or relational interactions (Isobel et al., 2021; Lev–Wiesel, 2007; Menzies, 2008). Literature indicates that the impact of DVA can be lasting and transfer intergenerationally. This can include intergenerational cycles of abuse whereby as each generation becomes a parent their experiences of abuse contribute to them then enacting abuse (Hoffart and Jones, 2018; Lünnemann et al., 2019; Rees and Evans, 2021).
Adverse Childhood Experience’s (ACE’s) comes from a large-scale study conducted in California (Felitti et al., 1998). Primary care practitioners observed a trend between poor physical health in adulthood and psychologically harmful experiences in childhood and adolescence. They also observed increased poor social and psychological outcomes. The ACE’s that were explored were experiences of physical, emotional and sexual child abuse as well as witnessing domestic abuse, substance misuse, poor mental health, acrimonious parental separation and parental incarceration (Anda et al., 2006; Boullier and Blair, 2018). The idea of ACE’s has attracted a rich evidence base with several systematic reviews (Hardt and Rutter, 2004; Hughes et al., 2017; Kalmakis and Chandler, 2015). However, it has also more recently garnered critique for its utilisation (Kelly-Irving and Delpierre, 2019; Macvarish and Lee, 2019). In particular, it has been observed that ACE’s are used in a predictive fashion with excessive certainty diminishing the agency of individuals and parents to negotiate and resist the impact of these experiences. The use of ACEs has also potentially not considered the different experiences within different cultures and communities. Finally, ACEs have in some cases been used to infer the individual fault of parents when they were intended to be used to highlight societal failings and ensure equity for those who are most disadvantaged.
Attachment theory, ACE’s and intergenerational trauma have been valued contributions to health and social care. Particularly within the context of Children’s Social Care (CSC), they are key ideas frequently used in practice and often cited in court reports (S. Webb and Gray, 2012). Though fundamentally an agency which is trying to ensure the well-being of children and families, and acting in a role of public protection, CSC has received some criticism (Ainsworth and Hansen, 2012). The judgement of whether to remove children from a potentially harmful environment, such as when they are being exposed to domestic abuse, is challenging as due to attachment theory it is understood the removal of a child from a familiar environment with ‘caregivers’ has a profound negative impact. This is often balanced by consideration of ACE’s and intergenerational trauma and searching for examples of ‘dysfunctional’ attachment which are used as justification to remove a child (Crittenden, 2011; Kwako et al., 2010; Spieker and Crittenden, 2018). There are clear examples where the removal of a child has been a necessary step to safeguard children (Forrester, 2017). However, the ethics of this are complex, such as, who gets to judge what is ‘good parenting’ and what is ‘harmful’ (Bornstein, 1991; Chen et al., 2019). Theory can be misused and presented as fact with far greater claims of validity and predictability than it in fact has (Krieg, 2023; Thyer, 2008). Aspects of systemic and personal discrimination might influence choices to remove children, with racism present in social care systems (Bartholet, 2011; Berkman et al., 2022; Rodenborg, 2004). Furthermore, severe and systemic abuse of children who have been taken into care has occurred (Biehal, 2014; Euser et al., 2013; Hobbs et al., 1999). The researcher reflects on the tension between safeguarding children, respecting family life and parenting approaches. They also wonder what opportunities might be limiting opportunities for relational healing, emotionally corrective experiences and catharsis.
Gap in the literature
Given the frequency of DVA and its severe impact, the majority of research, resources and interventions, focus on recognising abuse and supporting people to leave abusive situations. This preventative approach focusses on minimising the opportunities of harm being perpetrated. This approach has been impacted by continued austerity which has seen vast losses in the public sector in service size, staffing and specialism (Bach, 2016; Peters, 2012; Stuckler et al., 2017), especially for specialist DVA services (Donovan and Durey, 2018; Sanders-McDonagh et al., 2016). Though prevention is always preferable the current context does not enable this easily and means many individuals are exposed to DVA.
The focus on prevention means there has been a comparative lack of research on tailoring interventions to support individuals following abuse, especially substantial periods of time after the abuse. There are several approaches which are utilised with individuals who have experienced abuse, supported by a small evidence base. Furthermore, much of this evidence base focuses on individualised psychological interventions. Though people might find great value in individualised interventions, DVA is a fundamentally relational form of harm perpetrated in an environment and relationship in which people should feel safe. The impact of this is often observed intergenerationally from caregiver to child. Traumatic experiences can serve to disconnect people from their relationships and values in a way that isn’t always rectified by traditional interventions (Afuape, 2011, 2016). Relationships are observed to have great influence in mediating the impact and appraisal of abuse in the short term (Bowyer et al., 2015; Jones and Vetere, 2017). However, no literature exists that explores relationships in a longitudinal manner, potentially many years after the DVA. The researcher views DVA as a uniquely relational abuse where the environment and individuals where people should experience the greatest safety is the environment in which they experience severe harm, which has an enormous impact on future relationships.
Therefore, to better understand the relational impact of DVA, this research explored the stories of dyads who had been jointly exposed to DVA as children and caregivers using narrative inquiry (NI).
Research questions
• What narratives are constructed and how have they changed over time? • How have these narratives constructed the abuse and the relationships impacted by the DVA? • What narratives are shared between caregiver and child and what narratives are kept to the individual?
Epistemology and Language
The researcher believes that discourse is socially created, and, in turn, discourse determines the reality in which people engage. Subsequently, those with power influence discourse and, by extension, dictate reality (Foucault, 1977). As Martin Haberman wrote ‘Language is not an innocent reflection of how we think. The terms we use control our perceptions, shape our understanding’. (Haberman, 2000, p. 203). As such, researcher will be explicit in their choices of language. The definition of DVA within this research is an action or inaction that actually or potentially harms another individual from within that family, home or close community. This can be a singular event or many events. The perpetrator of the violence and/or abuse may also no longer be within the same domestic setting when perpetrating harm. The violence and abuse will commonly be within the domains of physical, emotional, psychological, sexual, financial, digital, cultural or spiritual abuse but may be beyond them. The experience of being domestically abused is not restricted to any particular gender, sexuality, age or any other ways individuals can be similar or different in their identity. However, most commonly, it is perpetrated by men.
The language of victim and survivor positions individuals differently with ‘victim’ potentially inferring a lack of agency and ‘survivor’ not capturing the many individuals who do not survive domestic abuse (Hoff, 2016; Jacques, 2021; Little, 2023). The language of survivor-victims will be used to hold greater complexity and nuance of these experiences. This also recognises the fluidity of identity and that an individual’s relationship to either survivorship or victimhood may change based on many factors.
I will be constructing perpetration as harm perpetrated by someone in a position of greater privilege and power, in that moment, against someone with less privilege and power, at that moment. An individual’s relationship to power and privilege is dictated by how they are perceived based on their geographical location, place in time and who they are in a relationship with as all these domains impact the context of power and privilege (Fanon, 2016; Foucault, 2019; Harvey, 2019). Fundamentally a power disparity is necessary to enact abuse meaning no one gender, or any other characteristic, indicates perpetration or victimhood whilst also recognising why DVA is predominantly perpetrated by men.
Method
Therapeutic approaches specific to DVA is an area with limited research, especially when compared to the prevalence of DVA. As such, it is difficult to provide robust and well evidenced theories. Therefore, using inductive methods to generate rich data of people’s experiences of DVA would be the most methodologically sound (Azungah, 2018). Several methodologies were considered. Interpretative Phenomenological Analysis, though well suited to exploring complex experiences, is arguably less well suit to navigating experiences located within nuanced socio-cultural landscapes. Grounded Theory would have produced a rich understanding of a complex social process but would have struggled to address the research questions given the data present. Thematic Analysis was strongly considered but had the potential to struggle with the complexity of such a multidimensional data set with multiple narrators, especially if those narrations had been highly dissonant in a small sample size. Discourse Analysis would have addressed the research questions well from the epistemological and ontological position. It was ultimately not used due to its potential to be overly hermeneutic and overly analytic which was dissonant from the ethical concerns of unintentionally replicating experiences of abuse and gas lighting by minimising, appropriating or altering narratives. Ultimately, Narrative Inquiry was chosen and though not free of limitations appeared the best fit.
Narrative Inquiry refers to a group of qualitative methods that seek to explore stories (Nollaig, 2011). When exploring narratives, NI considers what is being told, how it is being told, to whom it’s being told to and why it’s being told (Riessman, 2008). NI also considers the socio-political context as well as the relationship between the storyteller/s and the interviewer (Greenhalgh, 2016). All these domains come together in NI to produce an understanding of a story that is complex and entirely unique to that telling.
Within this research there was a nuanced additional domain brought by interviewing dyads. It brought another narrator and audience member in each telling, as well as providing opportunity for narratives to converge and diverge. Furthermore, consideration for how narration was co-constructed between the dyad both in the active structuring and telling of the narrative and the absent but implicit in various nonverbal communications and choices not to contribute.
NI maintains whole narratives from the participants which permits a greater degree of influence by participants on findings. This is particularly valuable in contexts where the experiences and stories are silenced, appropriated and otherwise go untold (Daiute, 2013). This occurs in DVA particularly in coercive control. As such, utilising a method that had the least opportunity to replicate this harm was an essential and ethical part of this research. That said NI from a social constructionist frame recognises the subjectivity of research and that in writing this research it is essentially a narrative (understanding the occurrence in the participants lives) within a narrative (the telling of the narrative to the researcher) within a narrative (the writing of this research) (Dubnewick et al., 2018; Trahar, 2006). NI embraces multiplicity in subjective interpretations allowing for pluralistic conclusions (Bhattacharya, 2016).
Ethics
Ethical approval for this study was granted by the University of Hertfordshire ethics committee. Participants provided informed consented and had the capacity to withdraw from the research up to 2 weeks following their last interview.
Though the research itself was not fundamentally exploring experiences of abuse but what followed it, the researcher recognises the content may still have been distressing. As such, a distress protocol was generated to proactively manage participant’s distress. A 45-minute meeting to collaboratively write a safety plan with participants was used to think amount how to navigate potential distress. The interviews themselves incorporated ‘checking-in’ and ‘checking-out’ opportunities to bookend each interview as well as pauses in the interviews to provided agreed opportunities for participants to break. Anonymity was ensured throughout using pseudonyms.
Participants
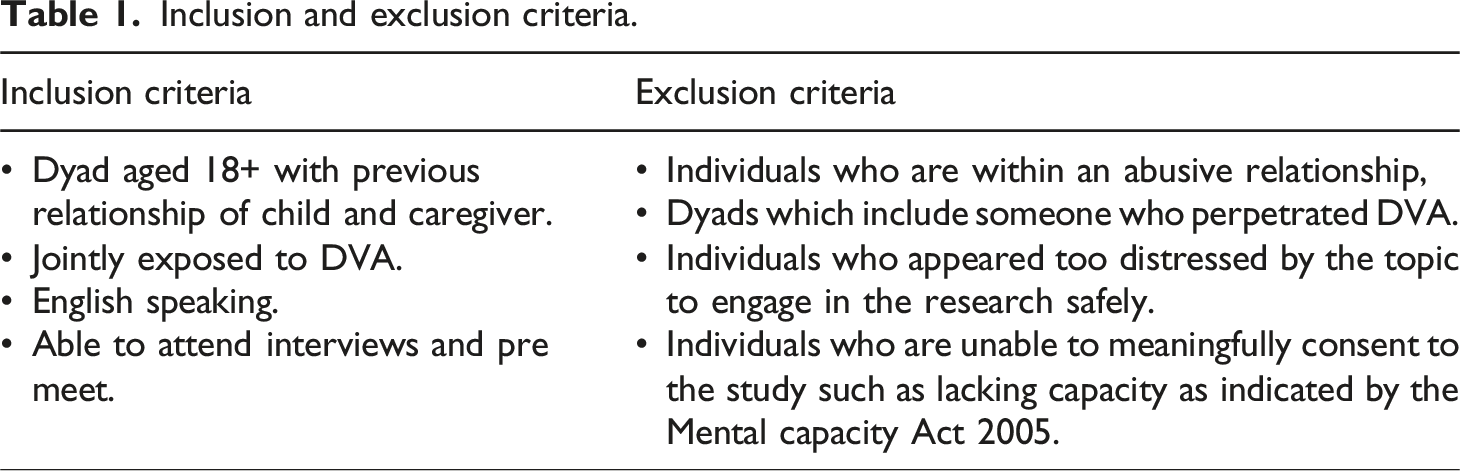
Participants were dyads who jointly experienced perpetration of DVA against them. Examples of this relationship might be parent and child, older and younger sibling or unrelated co-residents. Familial dyads were included to better enable inquiry as to the longitudinal relational impact of DVA as well as the longitudinal coping with that impact. Caregiver and child roles were included to allow opportunity for the consideration of intergenerational impacts of DVA as well as coping with the intergenerational impacts. Caregiver and child was included over parent and child to not unduly privilege the experience of heteronormative families, western families and care inexperienced families. Time passed since the abuse was not utilised as it is not a definitive predictor of processing and emotional distress reducing from what we understand from trauma theory. We also agreed the topic of the study itself is likely to screen out individuals not prepared to discuss this topic. The distress protocol would also act as a safeguard to this.
Inclusion and exclusion criteria.
Data collection
Data collection occurred via semi-structured interviews, two for each individual, three per dyad. After the safety planning, the researcher interviewed the dyad jointly. In the week following, the researcher interviewed each individual in the dyad separately. This novel approach to interviewing dyads and individuals was selected for several reasons. Given the focus on relationships and intergenerational patterns, interviewing participants together appeared to facilitate this discussion more effectively. Interviewing both jointly and individually was intended to provide opportunities to explore the convergence and divergence of narratives the dyad might share. Finally, given the comparatively large time period being explored, multiple interviews were needed to provide adequate space to explore this.
The interview format of dyadic interview followed by individual interview was a lengthy choice made with my research team. The individual interview being placed second allowed the exploration of specific narratives without repetition had the process been reversed. Furthermore, placing the individual interview second allowed opportunity for the researcher to more effectively address any distress.
The option was provided for interviews to be online or in-person based on distance, but all participants opted for video interviews via the video conferencing platform Zoom. Interviews were semi-structured and were video and audio recorded.
The questions posed in the interview were intended to lightly guide participants in their story telling. Questions attempted to explore both the impact of abuse and how it was negotiated. Questions were similar between interview types to elicit both individual and dyadic narratives. Interviews were then transcribed verbatim by the researcher. The data analysis was completed using both word documents and paper and pen.
Approach to inquiry
Following the researcher’s transcription of the interviews they repeatedly listened to the recordings and read the transcript to both confirm the accuracy and immerse themselves in the data. Once a sense of immersion in the data was reached the researcher then passed through the transcripts alongside the audio recordings several times and began to identify narratives. Some of these were located closely together and others were strung out throughout the interviews. Entry and exit talk (Riessman, 2008) was a useful guide to identifying where stories opened, closed or reopened throughout the transcript. Each narrative was mapped out and analysed to explore how they intersected and diverged within the text. Once each narrative was contextualised within the transcripts in relation to different narrators, interviews and other narratives they were categorised as stories and sub-stories.
Following the identification of narratives the researcher then passed through each narrative and the transcripts as a whole attending to analytic categories adapted for this research based on the writing of Andrews (2021), Mik-Meyer and Järvinen (2020) and Nollaig (2011). These categories were thematic, structural and dialogical/performance. Thematic focused on what is being said and what language is being used to do so. To do this the researcher considered questions such as ‘What is being said?’, ‘What is not being said?’ and ‘Where do dyads stories and language converge and diverge?’. Structural focused on how a narrative is organised in terms of its sequencing of information and what domains are being explored. With structural the researcher considered questions such as ‘Is this story coherent when told separately and together?’, ‘Is this story coherent to me? Might it be coherent to others?’ and ‘What parts of the story are given more or less focus by this sequencing?’. Finally, dialogical/performance focused on the co-construction of narratives between individuals. How narratives may or may not change based on the audience present and how these are contextualised in the socio-political world in which people exist. Examples of questions considered by the researcher include ‘Who is this story being told to?’, ‘Who is not telling this story and why?’, ‘How is my identity impacting my listening, what do I privilege?’, ‘How is this narration informed by the narrators and audiences’ context?’ and ‘What does the person narrating privilege?’. By it’s nature this process required ongoing reflection and reflexivity to considered the researchers interpretations and contributions to this process.
It should be recognised that though the analysis was conducted in a rigorous and reflexive manner, other readings of the data might lead to different and equally valid insights. Alternative subjective interpretations are not inherently at odds, simply a different interpretation of a multifaceted experience (Riessman, 2008).
Narrative inquiry
The dyadic interviews wove rich and multifaceted narratives. Some narratives appeared tangential initially due to the dyadic co-narration. A richness in meaning making was generated by attending to who spoke and when, who didn’t contribute, nonverbal communication and the impact of all this on the original narrator. The researcher encourages you, the reader, to care deeply for yourself as you read this. In reading the below stories consider the words of Frank Arthur (2013) ‘stories are not material to be analysed; they are relationships to be entered’.
Context
Within this section there is a brief summary of information about participants to aid the reader in contextualising the narratives present. The individuals who took part in this research are amazing multifaceted individuals who’s context is not just confined to DVA. The brief description and quotes within this manuscript should not be considered the entirety of their rich and unique context. It has been necessary to make some minor changes or withhold certain formation to ensure anonymity of participants. This was done with care to ensure no intended changes to the meaning what was said.
Dyad A consisted of Charlene (mother) and Brooke (daughter). Charlene was care experienced and had herself experienced DVA in her childhood. Brooke still had contact with the perpetrator of the abuse. Brooke was pregnant with her first child at the time of the interview. Brooke had been removed from Charlene’s care for a period of time by the local authority (LA). Brooke had been exposed to further abuse whilst in care. Both Charlene and Brooke felt the local authority had failed them and had also discriminated against Charlene based on her age, gender, skin colour and social class. Both Charlene and Brooke had undertaken extensive personal therapy and had worked within healthcare services.
Table of findings.
Collective narratives
The relationship with DVA
All participants spoke to the innumerable ways in which DVA has impacted their lives and how it has continued to show up. Brooke reflected she didn’t feel she recognised the impact immediately
Angelica reflected on the impact of DVA
Alice shared a similar narrative to Brooke of a safe relationship being an antecedent to the impact of DVA showing up in her life
Participants spoke to the pervasive and invasive impact of DVA in their lives. It had covered substantial spans of time and impacted many domains of life even once the abuse had stopped. The literature supports that the impact of DVA is pervasive and ongoing, often due to the impact on attachment and due to psychological trauma (Fox et al., 2014; Hulley et al., 2023; Tarquinio et al., 2012), but also the material impacts of DVA on finances, housing and physical health (McCaw et al., 2007; Sharp-Jeffs, 2015). There was a collective experience from all participants that it would be an experience that was never ‘gone’. The participants spoke about how the impact of DVA would creep into their lives sometimes at obvious points but also in seemingly unconnected moments, this was often distressing or frustrating when the impact had felt distant. One of the largest concerns about exposure to DVA in adolescence, is the potential for disrupted attachment and how DVA may impact on future relationships (Hou, 2020; Little, 2023). Perhaps the most consistent narrative of when the impact of DVA appeared for participants was in romantic relationships, which either served to elicit similar concerns around trust or created such a safe environment that it permitted unexpected processing of the DVA. Participants navigated this by either finding valued connection in non-romantic relationships and/or continuing their own therapy to aid in the processing and navigate the relational trauma
Sub-story: Acts of resistance
Acts of resistance are actions which directly resist power structures (Bourdieu and Bourdieu, 2004). Given the varied an ongoing impact of DVA, it is only proportionate that the ways of coping and resisting are equally as varied and ongoing. Participants found so many ways to negotiate the impact. Dyad A often spoke about the need for boundaries as resistance due to the ongoing involvement of the individual who perpetrated the DVA
Limiting intergenerational trauma was a defining part of both dyads acts of resistance and their narratives,
Breaking this cycle involved ongoing therapy but also compassion
Understanding and Connection
All participants spoke at length about the importance of understanding and making sense of what happened whether that was better understanding themselves,
Sub-story: Mother and daughter
Both dyads consisted of mothers and daughters; both named how paramount the relationship was to resisting the impact of DVA. Brooke attributed most of her coping to her mother
Right support at the right time
All participants sought different forms of professional support. This involved support for physical, mental, material and spiritual well-being. There were repeated accounts of the value of professional psychological support,
Sub-story: Failure of services
Most participants also spoke about services not being present at times of need, not helping them or actively hindering them. The involvement of the LA appeared a major antagonist in Charlene’s narration. Charlene spoke passionately about the LA and the impact on her children
Sub-story: Embodied lives
Both individuals who were children at the time of abuse, named experiencing physical symptoms in childhood that were not easily medically explained which both felt might have been a response to the DVA (Caldwell and Leighton, 2018; Kozlowska, 2013). They also both explored how movement through sports and dance had enabled easing of tension or enabled expression. There is a growing literature base on embodied response to distress and how to soothe and regulate the body in distressed states (Babbel, 2018; Porges, 2022; van der Kolk, 2014).
Implications
There are several implications that can be taken from this research:
Participants had much expertise to offer about working with survivor-victims and methods of resisting. Given the scope of their resistance, I would propose a change in vernacular from survivor-victim to survivor-victim-resistor. This highlights the capacity to transcend a label predominantly based on another individual’s agency. This vernacular should be seen to imply a fixed hierarchical progression but fluid transitory continuum.
Participants’ distress and growth had limited temporal linearity and appeared relational in nature. From a clinical perspective, this highlights the necessity for repeated access to support for survivor-victim-resistors, not a singular offer of support after leaving the abusive situation. Needs may also vary during each point of access requiring differing therapeutic paradigms, duration and formats. This includes not only psychological support, but physical health given the embodied experiences, as well as some expertise or capacity to refer to support for finances, housing and education. These are unlikely to be individuals who find things resolved from six sessions of low intensity CBT but may well access this as part of their journey.
Given the value participants found in meaning making, use of formulation may aid meaning making (Johnstone et al., 2013). A variety of therapeutic paradigms may be helpful based on individual’s needs. Due to value of embodied experiences and expression by participants utilising art, drama and movement based approaches could be helpful (Feniger-Schaal and Orkibi, 2020; Ritter and Low, 1996). Participants commented on the value of traditional trauma therapies at points so these should also be utilised as appropriate. The relational nature of harm, meaning making and resistance identified by participants could be considered in interventions. A consistent relational experience with a small number of clinicians to enable consistent points of attachment could be helpful (Dozier and Bates, 2003). Family and dyadic approaches, regardless of client age, may also be of value, particularly approaches that privileges attachment and family such as Attachment Narrative Therapy (Dallos and Vetere, 2021). ANT, and similar approaches, could also provide opportunities for individuals to negotiate intergenerational trauma whilst also enabling more opportunities for intergenerational coping and resistance. The approach focuses on considering attachment and family narratives intergenerationally which appears to align with narratives offered by dyads in this research. Particularly ANT’s consideration of replicative and corrective family script (Byng-Hall, 1998). Though ANT appears promising other approaches also appear to align well with the idea of intergenerational trauma and its subsequent healing via relationship. Particularly, community psychology approaches within indigenous communities who have previously been colonised or otherwise persecuted (Hoyt, 2019; Hübl and Avritt, 2020; Radu et al., 2014). Given the substantial intergenerational trauma in these communities retaining community identity, community values and community connection, intergenerationally, has been recognised as important supporting a process of healing and of resistance (Afuape, 2016). Collective narrative practices may also allow for the exploration of intergenerational trauma and resistance to that trauma (Lock, 2016; Ncube, 2006).
As this research highlights relational connection is important in helping people navigate traumatic experiences. Taiwo Afuape (2011, 2016, 2020) evidences the impact of trauma on separating people from each other and values that connect them. She also demonstrates how connective and collective interventions, which enable people to reconnect with each other and their values, aids in their navigation of traumatic experiences and resistance across levels of context. This research aligns with these ideas. The systems used in the UK for child protection did not meet the needs of these participants or others as indicated by the literature. Participants were either too scared of the LA to engage with it or felt harmed by it as it removed resources and discriminated against people. As focus on managing risk can limit opportunities for healing, connection and resourcing (Cottam, 2015; Featherstone et al., 2018). Percy Aggett and Philip Messent (2019) present a relational-collaborative approach for social services and mental health services. This is built upon connection and mutual collaboration with people that services are supporting to increase their agency and aid in resourcing them. Findings of this research may be supportive of this approach.
The experience of discrimination by participants in this research is deeply concerning and potentially mirrors the literature highlighting systemic discrimination in many public services (Bartholet, 2011; Hoosain, 2018; Miller, 2021). Participants in the research were harmed by this experience and worked hard to offset its impact. This research does not offer insight in addressing this but recognises the harm and need for change.
Limitations
This research contained several limitations:
Recruitment for this research had several aforementioned barriers. This led to four participants being recruited which, comparative to most research methods, is a small sample. However, the volume and richness of data these participants provided highlights this sample was large enough for this research using NI (Daiute, 2013; Morse, 2000). The number of participants does generate other challenges though. The participants were homogenous in the gender and relationships within dyads. Though qualitative research values homogeneity in participants this does invite the query around who’s story was not represented. Male candidates did come forward but did not meet the criteria. The findings of this research could look different if considering the narratives of fathers and sons or siblings or involved caregivers who were in a same-sex relationships. Why was this, are stories of women experiencing DVA perhaps less subjugated discourses compared to male experiences of abuse or is it that women are more amenable to engaging in research about the experience together? Perhaps the gendered ways of responding to distress and DVA in particular (Moulding, 2015; Wild, 2022), also meant women found the language to narrate there story more readily available.
It also worth reflecting that people who were willing to come forward as a dyad must have a robust relationship and have found some way to reflect on the experience and may have already had co-created narratives of their experiences. As such, this may have excluded certain individuals from this research.
Though the research was appraised using ‘Big-Tent’ criteria (Tracy, 2010) co-rating and similar approaches to ensuring credibility and rigour was absent from this research due to time and personnel constraints. As such, this should be considered in the applicability of the findings.
Strengths
This research contained several strengths:
This research is timely given the substantial increase in DVA during COVID-19 and offers a valuable addition to the literature where there is a clear gap from both a research and clinical perspective.
There is limited research looking at the relational context of those impacted by DVA and therefore this research allowed narratives that are rarely heard within the literature or therapy context to be voiced.
This research was conducted in a rigorous ethical manner to not replicate abuse. It also offered meaningful and transparent reflexive content to help the reader understand the researcher’s choices.
Future research
Future research in this area would benefit being conducted with a more heterogenous sample providing richer and potentially dissonant narratives to this research. Given the barriers to recruitment heterogeneity might be difficult. Support from charities or third sector organisations could aid in accessing more specific pools of participants and make the research, perhaps, seem more appealing to certain groups. Future research could benefit from exploring differing interview formats, either altering the sequencing or a group format based on role of caregiver or child. Furthermore, inclusion of other data sources such as pictures is common in NI. Participants named preferences for movement and differing expression. As such, introducing additional options for expression, such as images, could be of value and fits with NI (Riessman, 2008).
Conclusion
This research has provided a narrative inquiry, using a novel approach, to explore the experiences of dyads as they’ve navigated DVA. This research brings a unique perspective by capturing the narratives of dyads that have experienced DVA. Participants spoke to the scope of DVA and how it impacted their lives but also the many ways they found to resist that impact. They spoke to the value of the right services, support at the right time, but also the harm of services. They spoke to how the trauma of DVA appeared in unexpected ways. Finally, they spoke to the reciprocal relationship of connection and understanding, particularly between mother and daughter. This provides scope to consider the experiences of dyads and implications this has for therapeutic interventions and services ‘hope is something we do with others’ (Weingarten, 2001).
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.