
Abstract
This study aimed to investigate patients’ clinical, hematologic, and biochemical profiles with pancytopenia. This prospective observational study was conducted at a tertiary care hospital from January 2019 to June 2020 on 80 patients, 39 (48.7%) were males and 41 (51.2%) were females, over the age of 18 presenting with pancytopenia. All the patients were subjected to thorough clinical and physical examinations. A complete blood count (CBC), peripheral smear examination, bone marrow aspiration, and reticulocyte count were performed. The data was analyzed using the IBM SPSS 20.0 software. Most of the cases had moderate (Hb<7-9.9g/dl) anemia (63.7%, 51/80 cases), while severe anemia (<7g/dl) was seen in 31.2% (25/80) cases, and 5% (04/80) cases showed mild anemia (Hb<10-11.9g/dl). Most patients with severe anemia had vitamin B12 deficiency anemia (12/80), that is, 15%. Macrocytic anemia was noted in preponderance (50% cases, 40/80), whereas microcytic hypochromic and normocytic hypochromic anemia constituted 21.3% (17/80), and dimorphic anemia was seen in 7.5% (06/80) cases. Based on WBC counts, 56.3% of cases (45/80) showed counts between 2000 and 4000 cells/cu.mm, while counts between 1000 and 2000 cells/cu.mm were seen in 31.3% of cases (25/80), and 12.5% of cases (10/80) had counts of <1000 cells/cu.mm. The study highlighted that 28.8% (23/80) had a platelet count between 50,000 and 1 lakh/cu.mm (mild thrombocytopenia), 36.3% (29/80) cases had a platelet count between 20,000 and 50,000/cu.mm (moderate thrombocytopenia), and 35% (28/80) cases had a platelet count less than 20,000/cu.mm (severe thrombocytopenia). The most common diagnosis of bone marrow aspiration was megaloblastic anemia, seen in 50.0% (6/12) cases. Megaloblasts were seen in 50.0% (6/12) cases of megaloblast anemia. The bone marrow aspirate of a patient with dengue fever and malaria showed macrophages containing engulfed red blood cells, lymphocytes, and platelets. Myeloblasts (>20%) were seen in 1 (8.3%) case of AML, and decreased myelopoiesis was seen in 25% of cases (two cases of aplastic anemia and one case of MDS). This study concludes that vitamin B12 deficiency is the most common cause, which is more common in people who are strict vegetarians, with a predominance in the younger age group. The study also emphasized the vitality of the physical findings, detailed primary hematologic and biochemical investigations, and peripheral blood pictures, all of which provide precious information in the work-up of pancytopenia patients.
Introduction
Cytopenia is a reduction in any of the three peripheral blood cell types. A reduction in all three types of cellular components is termed pancytopenia, which involves anemia, leucopenia, and thrombocytopenia. Initially, mild impairment in marrow function may go undetected, and pancytopenia may become apparent only during stress or increased demand (e.g., bleeding or infection). 1 The underlying mechanisms other than a decrease in hematopoietic cell production are marrow replacement by abnormal cells, suppression of marrow growth and differentiation, ineffective hematopoiesis, defective stem cell formation, antibody-mediated sequestration, and destruction and trapping of cells in an overactive reticuloendothelial system. 2
Etiologies of this condition can range from common diseases like nutritional anemias, drug-induced myelosuppression, and infections such as malaria, kala-azar, or dengue to life-threatening conditions like aplasia, myelodysplasias, and leukemias. 3 Pancytopenia is a striking feature of many severe and life-threatening illnesses, ranging from simple drug-induced bone marrow hypoplasia and megaloblastic marrow to fatal bone marrow aplasias and leukemias. Early detection of underlying pathology helps in timely diagnosis and therapeutic intervention, favoring a better clinical outcome. 4
The patient usually presents fatigue and weakness due to anemia, increased susceptibility to infections due to leucopenia, and bleeding tendencies due to thrombocytopenia. Physical findings and peripheral blood pictures provide valuable information in the work-up of pan-cytopenic patients and help in planning investigations on bone marrow samples. 5 Bone marrow evaluation is a vital diagnostic procedure that may confirm the cause of suspected cytopenia. 6
Neoplastic diseases and radiation have been reported as the most common cause of pancytopenia in Europe and Israel. 7 Aplastic anemia, followed by infections such as malaria and leishmaniasis, were the significant causes of pancytopenia reported in Bangladesh. 8 In research conducted in Nepal, hypoplastic anemia was reported to be the most prevalent cause of pancytopenia, followed by hematologic malignancies, megaloblastic anemia, leishmaniasis, and Gaucher disease. 9 Variation in the etiologies of pancytopenia is appreciated in different countries and regions of a single country. Studies from North and South India have implicated megaloblastic anemia as the most common cause of ancytopenia. In contrast, a survey conducted in Maharashtra has found hypersplenism and infections to be the most frequently responsible diseases.10–12
As many causes of pancytopenia are treatable and reversible, accurate diagnosis and timely intervention may be life-saving. They will undoubtedly impact the morbidity and mortality of these vulnerable patients. Knowing the exact etiology and presentation is thus vital for specific and timely treatment and prognostication. Therefore, this study aimed to highlight the most common clinical features and hematologic and biochemical findings of patients with pancytopenia.
Methodology
Study Area and Participants
A prospective observational study, a hospital-based study, was carried out at Jawaharlal Nehru Medical College & Hospital, Aligarh Muslim University, Aligarh, Uttar Pradesh, India, from January 2019 to June 2020 on 80 cases.
Inclusion Criteria
This study included patients between the ages of 18 and 70 who had pancytopenia and a hemoglobin level less than 13.3 g/dl in men or 11.5 g/dl in females, total leukocyte counts less than 4 × 109/L, and a platelet count of less than 150 × 109/L.
Exclusion Criteria
Patients receiving chemotherapy for malignant neoplasms and those with pregnancies are excluded.
Data Collection
A physician performed clinical examinations on each study participant. Demographic variables, clinical profiles, dietary history, and history suggestive of previous pancytopenia, aplastic anemia, inherited bone marrow failure syndrome, repeated early fetal loss, cancer, liver disease, metabolic disorders, or connective tissue disorders of study participants were collected using the structured questionnaire. The patients were evaluated by a thorough physical and systematic examination, including BP monitoring, anthropometric determinations, chorionic villus sampling (CVS), respiratory system, and abdomen. A complete blood count (CBC), peripheral smear examination, bone marrow aspiration, reticulocyte count, and serum vitamin B12 level were done in the central lab and department of pathology, biochemistry, and microbiology of the hospital.
Statistical Analysis
All the hematologic, biochemical, and demographic parameters were recorded. The observations and results were tabulated per gender, age group, symptoms, physical signs, bleeding manifestations, bone marrow findings, etiology, and vital hematologic and biochemical parameters. IBM SPSS 20.0 software was used to analyze the data. An ANOVA test and a chi-square test were applied for significance. A p value < .05 is considered significant.
Results
Out of the 80 patients, 39 (48.7%) were males and 41 (51.2%) were females, with a male-to-female ratio of 1:1.05. The age of the patients ranged from 18 years to 70 years. Most cases were from 18 to 30 years old, that is, 57.5% (46/80), whereas the least number was from 61 to 70 years old, that is, 3.7% (03/80). The mean age of the patients was 33 ± 13.23 years, wherein there were 39 males with an average age of 36.23 ± 14.18 and 41 females with an average age of 29.93 ± 11.6.
The majority of the cases presented generalized weakness (37.5%), followed by fever with chills and rigors in 33.7% of cases, only fever in 25% of cases, and abdominal distension in 3.8% of cases (Table 1).
Distribution of Cases Based on Presenting Complaints.
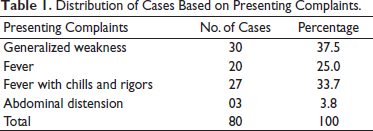
One patient can present multiple clinical findings, but the classification of the patient is done according to the presenting complaint. If a patient presented with a fever, their main complaint would fall under the fever category. In the case of generalized weakness, the only complaint was generalized weakness; there was no fever.
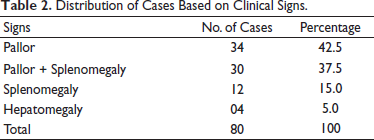
The majority of the cases presented with only pallor in 42.5% of cases (34/80), followed by pallor with splenomegaly in 37.5% (30/80), splenomegaly in 15% of cases (12/80), and hepatomegaly in 5% of cases (04/80) (Table 2).
Distribution of Cases Based on Clinical Signs.
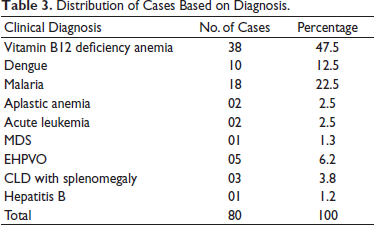
In this study, vitamin B12 deficiency anemia was the most common disorder diagnosed clinically in 47.5% (38/80), followed by malaria in about 22.5% (18/80), dengue in 12.5% cases (10/80), aplastic anemia in 2.5% (02/80), acute leukemia in 2.5% (02/80), MDS in 1.3% (01/80), EHPVO in 6.2% (05/80), CLD with splenomegaly in 3.75% (03/80), and Hepatitis B in 1.25% (01/80) cases (Table 3).
Distribution of Cases Based on Diagnosis.
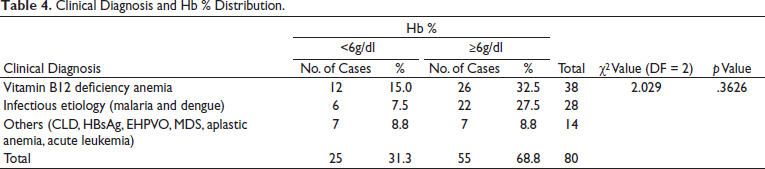
Most of the cases had moderate (Hb level 7-9.9 g/dl) anemia (63.7%, 51/80 cases), while severe anemia (<7 g/dl) was seen in 31.2% (25/80) cases and 5% (04/80) cases showed mild anemia (Hb of 10-11.9 g/dl). There were 25 patients with Hb% less than six gm% and 55 with Hb% more than six gm%, which was not statistically significant among the different diagnoses (p value .3626). The majority of the patients with severe anemia had vitamin B12 deficiency anemia (12/80), that is, 15%, followed by infectious etiology, that is, 7.5% (6/80) (Table 4).
Clinical Diagnosis and Hb % Distribution.
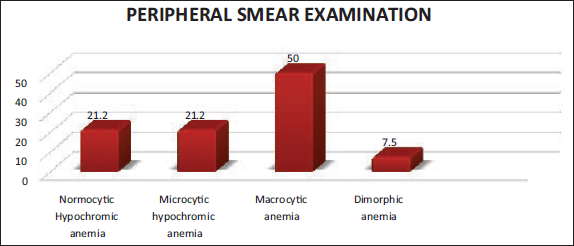
Macrocytic anemia was noted in preponderance (50% cases, 40/80), whereas microcytic hypochromic and normocytic hypochromic anemia constituted 21.3% (17/80), and dimorphic anemia was seen in 7.5% (06/80) cases (Figure 1).
Distribution Based on Peripheral Smear Diagnosis.
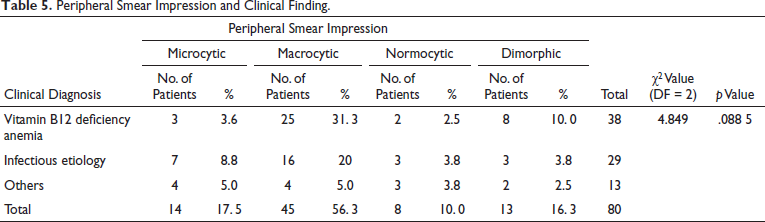
It was found that there were 14 (17.5%) microcytic, 45 (56.3%) macrocytic, 8 (10.0%) normocytic, and 13 (16.3%) dimorphic pictures seen on the peripheral smear, which was not statistically significant among the different diagnoses (p value .0885) (Table 5).
Peripheral Smear Impression and Clinical Finding.
Based on WBC counts, 56.3% of cases (45/80) showed counts between 2000 and 4000 cells/cu.mm, while counts between 1000 and 2000 cells/cu.mm were seen in 31.3% of cases (25/80), and 12.5% of cases (10/80) had counts of <1000 cells/cu.mm. There were 35 patients with a WBC count of less than 2000 and 45 patients with >2000, which was not statistically significant among the different diagnoses (p value .9579); however, the point of significance is that the WBC count was found to be decreased more in infection and vitamin B12 deficiency.
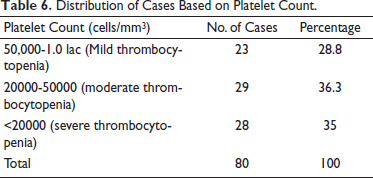
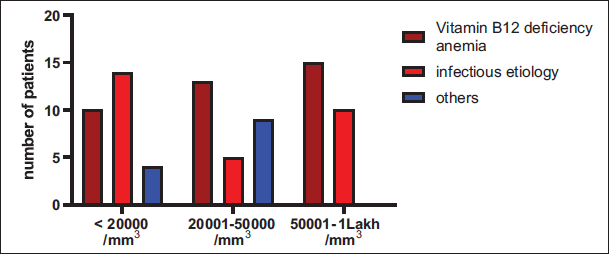
In the context of platelet counts, the study highlighted that 28.8% (23/80) had a platelet count between 50000 and 1 lakh/cu.mm (mild thrombocytopenia), 36.3% (29/80) cases had a platelet count between 20000 and 50000/cu.mm (moderate thrombocytopenia), and 35% (28/80) cases had a platelet count less than 20000/cu.mm (severe thrombocytopenia) (Table 6). Correlating the platelet counts with clinical diagnosis revealed that there were 28 patients with <20000 platelet counts, 27 patients had 20,000–50,000, and 25 patients had 50,000–1 lakh platelet counts, which was not statistically significant among the different diagnoses (p value .129), and severe thrombocytopenia (platelet count<20000/mm3) was primarily seen in the infectious group (malaria and dengue), that is, 17.5% (14/80) cases (Figure 2).
Distribution of Cases Based on Platelet Count.
Platelet Count Distribution and Clinical Diagnosis.
Among the 80 cases of pancytopenia selected randomly for the study, bone marrow aspiration was done in 12 patients in which it was indicated. The most common diagnosis of bone marrow aspiration was megaloblastic anemia, seen in 50.0% (6/12) cases, followed by aplastic anemia and infective etiology in 16.7% (2/12) cases (Figure 3).
Cases Distribution Based on Bone Marrow Aspiration Diagnosis.
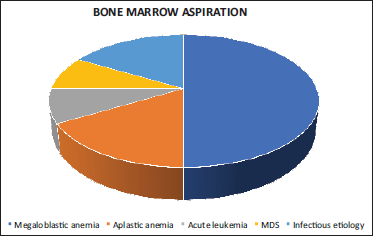
Hypocellular marrow was noted in 16.7% of cases, that is, two cases of aplastic anemia. Hypercellular marrow was noted in all the cases of megaloblastic anemia and in one case of dengue, malaria, and acute leukemia. Normocellular marrow was seen in one case of MDS.
Megaloblasts were seen in 50.0% (6/12) cases of megaloblast anemia. The bone marrow aspirate of a patient with dengue fever and malaria showed macrophages containing engulfed red blood cells, lymphocytes, and platelets. Dyserythropoiesis was seen in the MDS case, and decreased erythropoiesis was noted in all cases of aplastic anemia.
Among all cases, 16.67% showed normal maturation, which was seen in infectious disease, and 50% showed giant metamyelocytes, seen in vitamin B12 deficiency. Myeloblasts (>20%) were seen in 1 (8.3%) case of AML, and decreased myelopoiesis was seen in 25% of cases (two cases of aplastic anemia and one case of MDS).
In the present study, 83.3% of cases showed normal megakaryopoiesis, while 16.6% showed decreased megakaryopoiesis.
Discussion
Pancytopenia is diagnosed with a clinical history and physical examination, followed by hematologic, biochemical, and radiological investigations, bone marrow aspiration, and biopsy. A total of 80 cases of pancytopenia were studied. Most cases were observed among the 18-30 age group, that is, 57.5%, followed by 31-40 years. In a similar study by Mandli (2019), the most prevalent age group impacted was 11-30 years. 13 In a study conducted by Agarwal et al. (2015), the most prevalent age group afflicted was 11-20 years, 14 whereas Rao (2011) discovered a mean age of 41 years across patients aged 2-80 years. 11 As a result, younger age groups have been reported to present to hospitals with pancytopenia more frequently. This is most likely due to increasing awareness and self-concern among the younger age group, fewer hospital visits by the elderly owing to pre-existing diseases, a lack of information and awareness, and a lack of familial and financial support.
In the present study, there were more females than males, with a male-to-female ratio of 1:.05. A study by Rao (2011) reported males to be slightly more affected than females. 11 In contrast, Agarwal et al. (2015) observed female predominance in their study, 14 which corroborates the findings of our research. This finding might be explained by the fact that girls in our study were more nutritionally deficient, resulting in pancytopenia, and hence more females were chosen for the study.
Most cases presented with generalized weakness; the subsequent common complaint was fever, chills, and rigors. Among the signs, pallor was seen in 42.5% of cases (34/80), followed by pallor with splenomegaly, splenomegaly, and hepatomegaly. In a study conducted by Patel et al. (2018), the most common clinical features were weakness (80%), followed by fever (72.1%), pallor (100%), and hepatomegaly (62.8%), 15 which corroborated our findings. In the study by Agarwal et al. (2015), most patients presented with fever and pain in the legs, while the most typical physical finding was pallor. 14
This study highlights that most cases showed moderate anemia (63.7%). In a study by Thakkar et al. (2011), mild anemia was observed in 25% of cases, moderate in 51%, and severe in 24% of cases, respectively. 16 Patel et al. (2018) reported mild, moderate, and severe anemia was noted in 22.1%, 70.8%, and 7.1%, respectively, 15 which validates the findings of our study.
In this study, a large portion of the population showed macrocytic anemia (50% cases). Microcytic and normocytic hypochromic anemia constituted 21.2% and Dimorphic anemia in 7.5% of cases. In contrast, in the study conducted by Patel et al. (2018), the predominant blood picture was normocytic normochromic (38.5%), followed by dimorphic (32.7%), macrocytic (17.3%), microcytic hypochromic (5.8%) and normocytic hypochromic (5.8%). Jha et al. (2008) 17 and Rao (2011) 11 showed a dimorphic picture as the predominant blood picture. Herewith our study concludes that macrocytic anemia was the most common general blood picture, corroborating with some of the previous studies.
The present study reported hyper-segmented neutrophils in 34 macrocytic anemia cases and one case of iron deficiency anemia. In contrast, Patel et al. (2018) study reported hyper-segmented neutrophils in 40 cases of megaloblastic anemia and one case of iron deficiency anemia. 15 Rani and Sureshkumar (2017) said hyper-segmented neutrophils (92%) in the 251 peripheral smears of patients with megaloblastic anemia. 18 Hyper-segmented neutrophils are primarily seen in megaloblastic anemia, which relates to our study’s vitamin B12 deficiency.
Most of the cases (56.2%) showed mild leucopenia (WBC count between 2000-4000 cells/cu.mm), while severe leucopenia (WBC Counts of <1000 cells/cu.mm) was present in 12.5% cases of the present study. Thakkar et al. (2013) observed mild, moderate, and severe leucopenia in 46%, 52%, and 2%, respectively. 19
The present study observed that relative lymphocytosis was seen in dengue (10 cases) and malaria (18 cases). Relative lymphocytosis was reported by Tilak and Jain (1992) in 11 cases 20 and Khunger et al. (2002) in 38 cases. 21
In the present study, the fall in platelet counts demonstrates very close variations with 36.2%, 35%, and 28.5% cases with moderate, severe, and mild thrombocytopenia, respectively, in the decreasing order. In the study by Patel et al. (2018), severe thrombocytopenia in 8% of cases, mild thrombocytopenia in 66% of cases, and moderate thrombocytopenia in 26% was noted. 15
Vitamin B12 deficiency anemia was the most common disorder diagnosed clinically, that is, 47.5% (38/80) in the present study, followed by malaria. In a study conducted by Varma et al. (2018), among all the hematological disorders causing pancytopenia, the most common noted was megaloblastic anemia (98/202, 48.51%) followed by dimorphic anemia (36/202, 17.8%) and aplastic anemia (18/202, 8.9%). 22 The least common causes included hemolytic anemia (2/202) and disseminated intravascular coagulation (2/202), that is, 0.99% each. In a study conducted by Patel et al. (2018), the most common causes of pancytopenia were malaria (50%), megaloblastic anemia (18.6%), and dengue (18.1%), followed by aplastic anemia (1.3%), leptospirosis (0.9%), dimorphic anemia (0.9%), dyskeratosis congenital (0.4%) and myelodysplastic syndrome (0.4%). In Rao’s (2011) study, the most typical cause of pancytopenia was megaloblastic anemia (74.04%), followed by aplastic anemia (18.26%). 11 These studies highlight that megaloblastic anemia has been the most typical cause of pancytopenia. The most common etiology among males and females was vitamin B12 deficiency anemia.
In the present study, Hypocellular marrow was noted in one case of aplastic anemia and one of MDS. Hypercellular marrow was reported mainly in all megaloblastic anemia cases (06) and one case of Iron deficiency anemia. In a study conducted by Graham et al. (2015), the most common etiology of pancytopenia was normoblasts erythroid hyperplasia (30%), followed by megaloblastic anemia (20%), this was followed by acute myeloid leukemia (13.3%) and closely by micronormoblastic erythroid maturation (10%).
Conclusion
Pancytopenia is not an uncommon hematologic problem encountered in clinical practice. It should be suspected on clinical grounds when a patient presents unexplained anemia, prolonged fever, and a tendency to bleed.
The etiology of pancytopenia varies from one geographical area to another. Some reversible causes of pancytopenia include megaloblastic anemia, malaria, dengue, and sepsis. Conditions, like disseminated TB and collagen vascular diseases, can also be treated with specific treatments if diagnosed early to avoid further complications. Studies with many patients in different geographical areas are required to detect different causes of anemia, especially reversible, rare causes.
The present study concludes that vitamin B12 deficiency is the most common cause, which was more common in strict vegetarians, with a predominance in the younger age group who presented to the hospital. It was observed to be more common in females compared to males. However, it contrasts with other studies conducted in the same context; the probable reason is a different geographical distribution. The primary complaint was generalized weakness and fatigue, and the most common symptom was pallor. It emphasized that vitamin B12 deficiency is a common, preventable, yet underdiagnosed, and neglected disorder in many parts of India, including the very epicenter of the study. It brings to light that much more research is required for proper data collection, considering all the realms of its etiology, genetic predisposition, clinical features, and laboratory studies.
The study also emphasized the vitality of the physical findings, detailed primary hematologic and biochemical investigations, and peripheral blood pictures, all of which provide precious information in the work-up of pancytopenia patients. A complete hematologic examination, including bone marrow aspiration, should be done in these patients to recognize and diagnose this disease early so that proper intervention and medical treatment can be done.
Severe pancytopenia is significantly related to clinical outcomes and can be used as a prognostic indicator. Regarding future courses, it could be suggested that early identification of this disease would help in early planning for management, thereby improving survival rates. However, further studies with larger sample sizes are still needed to know the various etiologies of pancytopenia as soon as possible so that timely intervention can be done.
Limitations of the Study
The current study is a brief hospital-based investigation with a limited sample size. A larger sample size and follow-up investigation might have aided in properly evaluating the various causes. The study is limited by a lack of follow-up among a small fraction of patients. A larger multicentric prospective study emphasizing follow-up for hematologic blood count recovery might help enhance knowledge of clinical outcomes in diverse causes of pancytopenia. This study was done in a specific location and, hence, cannot be generalized to the entire population. Not all confounding variables were eliminated. Because a small number of patients in this study refused bone marrow aspiration and biopsy, those findings were not included in this study. Few of these patients were followed because of poor patient compliance; thus, the response to therapy was not thoroughly investigated. Furthermore, more specific functional tests and biomarkers for individual diseases must be developed.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Authors’ Contributions
Study conception and design: DCS, RV, SMKA, KA; data collection: DCS, SMKA, KA; analysis and interpretation of results: SMKA, KK, MV, PB; draft manuscript preparation: RV, KK, MV, PB. All authors reviewed the results and approved the final version of the manuscript
Ethical Approval
Study is approved the institutional ethics committee.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Statement for the Patient Consent
Informed consent is obtained from the subjects.