
Abstract
Aim
The aim of this study was to determine the prevalence of fecal incontinence (FI) in post-menopausal women and its risk factors.
Methods
This cross-sectional study was carried out from May 2022 to May 2023. All women in the post-menopausal age group attending outpatient services were given a simple questionnaire to assess the presence of FI and likely risk factors.
Results
A total of 728 women formed the study group (median age 58, range 45-84 years). FI was reported by 10.1 % of respondents. Women with FI were significantly more likely to have vaginal delivery (P < .0001), presence of one or more comorbid diseases (P = .0001), previous abdominal surgery (P = .01), and diarrheal stools (P = .0009). The odds of developing FI were highest for vaginal delivery, followed by the presence of co-morbid diseases.
Conclusion
The prevalence of FI was 10.1%. History of vaginal delivery, previous abdominopelvic surgery, diarrheal stools, and comorbid diseases were significantly associated with FI.
Introduction
Fecal incontinence (FI) is a common, yet underreported problem. It results in significant physical and psychological impacts on patients.1–3 FI is defined as recurrent uncontrolled passage of solid or liquid fecal material for at least 3 months. The definition excludes passage of flatus alone. 4 It is further categorized as urgency FI where patients are not able to hold feces for a prolonged period of time and passive FI in which patients are unable to sense the presence of feces in the rectum. 5 The prevalence of FI is reported to be between 2% and 18% in western data and it is increased among nursing home residents.3, 6–11 Risk factors predictive of FI include age, obstetric and gynecological factors, comorbid diseases, and poor general health.12, 13 It is commoner in women. 14 Various professional bodies in the West have published guidelines regarding the diagnosis and treatment of FI.15, 16 However, there is scant data from India on this clinical problem. Research is required to understand the magnitude, prevalence, and risk factors of FI in Indian subcontinent. Thus, this study was planned to determine the prevalence of FI in post-menopausal women and its risk factors.
Methods
This cross-sectional study was done from May 2022 to May 2023. All women in the post-menopausal age group attending outpatient services of the gastroenterology department were told about the study. Those willing to participate were given a simple questionnaire to assess the presence of FI and risk factors leading to FI. We excluded women who were under 45 years of age and those unwilling to participate (Figure 1).
Study Flowchart
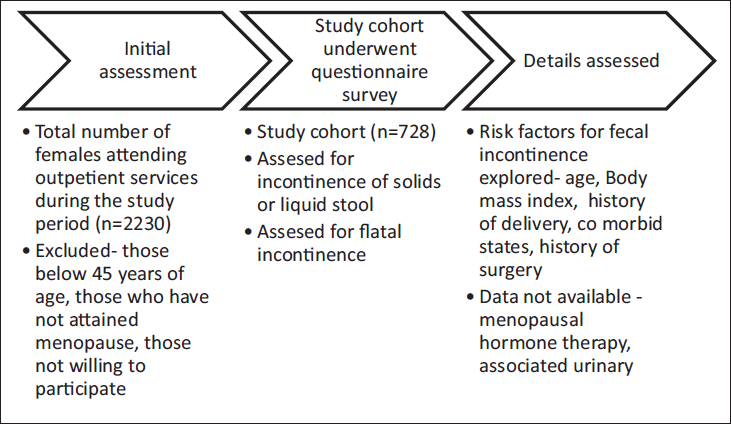
Data on FI was collected using a simple questionnaire and subjects were assisted by the authors to fill the questionnaire. Questions pertaining to incontinence of solid and liquid stools were followed by questions pertaining to flatal incontinence. Impact of incontinence on day-to-day activity and need to wear pads was assessed. FI was defined as per Rome IV criteria. 17
Factors potentially associated with FI were assessed. These included age, body mass index (BMI), parity, detailed history of delivery, presence of selected comorbid states (diabetes, hypertension, hypothyroidism, irritable bowel syndrome, inflammatory bowel disease), and history of surgeries (hysterectomy, cholecystectomy, appendectomy, colectomy, pelvic organ prolapse repair). BMI was calculated (kg/m2) based on the participant’s weight and height measured at the time of the interview. Method of delivery (vaginal or cesarean delivery) was collected and categorized as none, at least one cesarean delivery, or only vaginal delivery (ies). Stool forms were assessed using Bristol stool charts and classified as constipation (types 1-3), normal (types 4 and 5), and diarrhea (types 6 and 7) based on Indian data.18–20
Statistics
The collected data were entered in a Microsoft Excel sheet and interpreted as median, range, and percentages. Comparison of medians was done using the ANOVA test, and for proportions, the chi-square test was used. Odds ratio was calculated for factors found to be significant in univariate analysis. A value of P < .05 was considered statistically significant. Statistical analysis was performed using IBM Statistical Package for the Social Sciences (SPSS) version 20 (IBM, Armonk, NY, USA).
Results
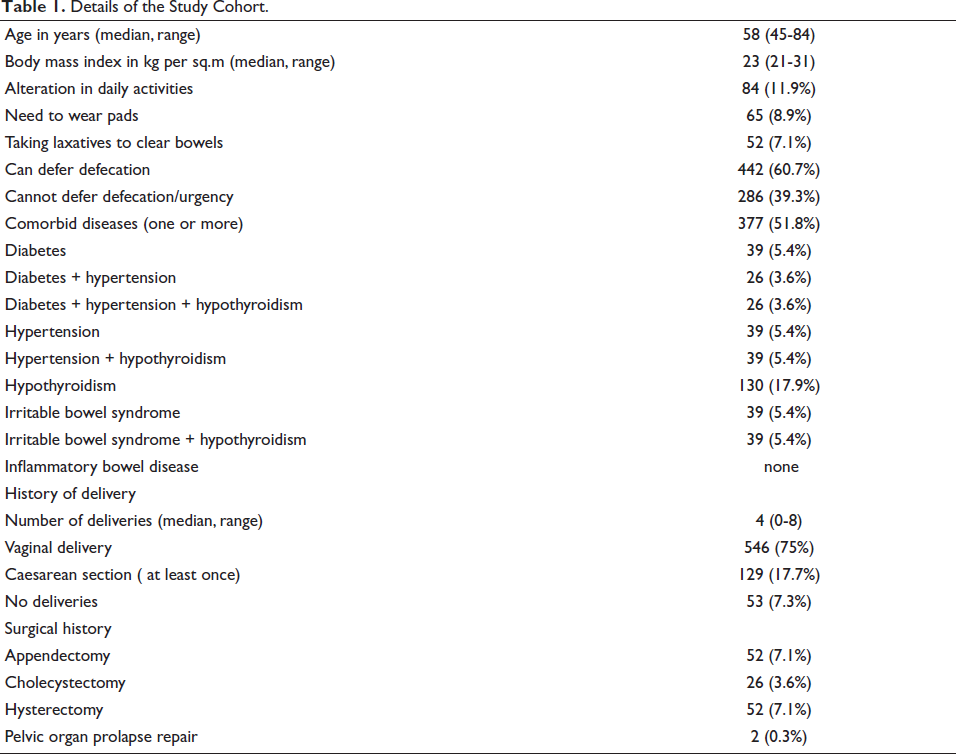
A total of 728 women formed the study group (median age 58, range 45-84 years). Approximately 9% subjects reported use of pads to prevent soiling of clothes (Table 1). Nearly half of the respondents had associated comorbid diseases which included hypothyroidism, diabetes, hypertension, and irritable bowel syndrome in various combinations. The median number of deliveries per subject was 4 and three-fourth of subjects reported vaginal deliveries. History of abdominopelvic surgery was noted in less than 10% of cases.
Details of the Study Cohort.
FI was reported by 10.1 % of respondents. This included solid and liquid FI by 14(1.9%) and 60 (8.2%) subjects, respectively (Table 2). Flatal incontinence was reported by 168 (23.1%) respondents.
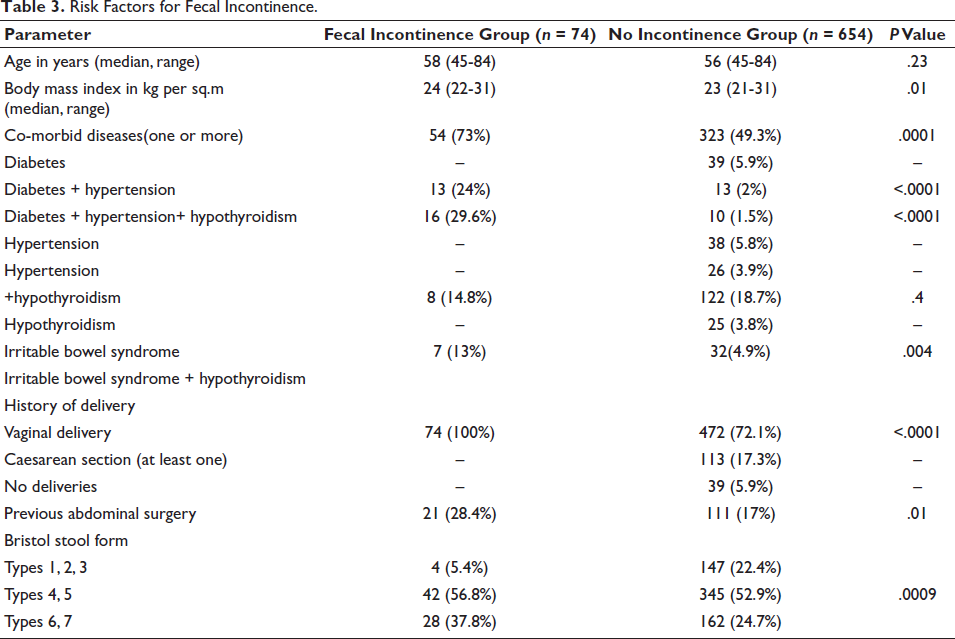
We compared subjects with and without FI (Table 3). Women with FI were significantly more likely to have vaginal delivery (P < .0001), presence of one or more comorbid diseases (P = .0001), previous abdominal surgery (P = .01) and diarrheal stools (0.0009). The odds for developing FI were highest for vaginal delivery, followed by the presence of comorbid diseases (Table 4).
Prevalence and Frequency of Incontinence Among the Study Cohort.

Risk Factors for Fecal Incontinence.
Odds Ratio for Development of Fecal Incontinence with Presence of Vaginal Delivery, Comorbid Diseases, Previous Surgery, and Diarrheal Stool Forms.

Discussion
Among this cohort of 728 post-menopausal women interviewed at a single center, the prevalence of FI was 10.1%. Flatal incontinence was much more common and reported by nearly twice as many women (23.1%). It caused alteration in daily activities in 11.9% of respondents and nearly 9% resorted to wearing pads. History of vaginal delivery, previous abdominopelvic surgery, diarrheal stools, and comorbid diseases were significantly associated with FI.
Western studies have highlighted several independent risk factors for FI which include obesity, chronic obstructive pulmonary disease, irritable bowel syndrome, urinary incontinence, and colectomy. These lead to FI due to increase in abdominal pressure, increase in intestinal motility, and sphincter or pelvic floor weakness. 20 We did not find higher BMI or age to be associated with a higher risk of FI unlike western data.6, 21, 22
Vaginal deliveries are likely to cause weakness of the pelvic floor muscles and thus lead to FI. Long-term studies from the west have noted that menopausal hormone treatment may predispose to FI. 23 However, this factor was not assessed in this study. Diabetes mellitus may contribute to development of FI through neurologic and microvascular pathways. Majority of our respondents with FI had presence of diabetes along with other comorbid diseases such as hypertension and hypothyroidism. Long-standing diabetes may cause damage to rectal nerves and pelvic floor musculature. Moreover, hyperglycemia may inhibit external sphincter function and diminish the rectal compliance.21, 24 Diarrheal stool forms were significantly associated with FI. It may be related to irritable bowel, diabetes and bacterial overgrowth. Management of diarrhea benefits most patients with FI. 25
This study has several limitations. Being a cross-sectional study, it cannot determine causal associations. We used self-reported data rather than objective tests to document FI. The study population consisted of postmenopausal women attending outpatient services of gastroenterology department. This may not reflect the true prevalence of the problem in the community. Currently, there are no standardized definitions or scoring systems for assessment of severity of incontinence and this has led to significant impact on research in this field. Impact on quality of life was not assessed. Details of menopausal hormone therapy were not available for majority of the respondents and hence were not assessed.
To conclude, FI affects 10.1% of post-menopausal women in gastroenterology outpatient clinics. It is highly bothersome for affected women and several risk factors for this problem are preventable or modifiable. Further research is needed on this often-neglected problem.
Footnotes
Author Contributions
SS and MJ helped in data collection, analysis, and writing of the article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethics clearance was obtained from Institutional Ethics Committee via letter no. AHRC/IEC/2022/08.
Informed Consent
Patient consent was taken prior to administration of questionnaire.