
Abstract
Background
A short patient reported outcome measure (PROM) could help identify people experiencing high treatment burden.
Objectives
To develop the Short Treatment Burden Questionnaire (STBQ), a novel PROM comprising a Global Treatment Burden Question (GTBQ) and items to identify areas of difficulty; improve its understandability and face validity; and explore patient views on using it in clinical practice.
Methods
Prototype development drew on the validated Multimorbidity Treatment Burden Questionnaire (MTBQ) and a single-item global measure. Adults, aged 18–65, living with multimorbidity were recruited from English general practices. Three rounds of cognitive interviews, with think-aloud and prompts, were conducted (July–October 2023). After each round, data were analysed, suggested changes and uncertainties discussed and modifications made. Public contributors were involved throughout.
Results
Participants (n = 15) were predominantly female (67%) and White British (87%). Issues were identified with the layout, instructions, and order and wording of response options, with some aspects interpreted in unintended ways. The number of issues and consequent changes reduced with each round of interviews. Participants highlighted potential benefits of using the STBQ in clinical practice, including encouraging patients to mention things they may not otherwise bring up. They suggested the STBQ could inform both individual patient care and practice-level service improvement.
Conclusions
Robust qualitative methods were used to develop a novel PROM for use in clinical practice and research. The STBQ demonstrated face validity and was relatively easy to use. Further work has been undertaken to validate the GTBQ. Guidance will outline how the STBQ could support patient care.
Keywords
Background
Treatment burden describes the work undertaken to manage health conditions, and the impact of the effort required to undertake that work. 1 Having multimorbidity (multiple long-term conditions: MLTC) is associated with increased treatment burden and reduced health-related quality of life. 2 A recent systematic review of qualitative studies concluded that the health-related workload of people living with multimorbidity is complex and multifaceted, and much of this may not be recognised or acknowledged by healthcare staff or within healthcare systems. 3
The prevalence of multimorbidity increases with age. 4 More than 50% of people aged 65+ live with two or more long-term conditions. 5 However, due to the size of the population, the absolute number of people living with multimorbidity is higher in those aged under 65. Multimorbidity and complex multimorbidity (three or more long-term conditions affecting three or more body systems) is associated with socio-economic deprivation, occurring with greater prevalence and 7–15 years earlier among those living in the most deprived areas.5,6 The prevalence of multimorbidity is also increasing over time, and the age and ethnicity of the population living with multimorbidity is changing to reflect a younger group with a higher proportion of people from Black and Asian ethnicities. 7
People living with multimorbidity often experience disjointed care, seeing a range of different healthcare providers and having different appointments for each of their conditions. 8 Providing care for people living with multimorbidity accounts for more than half of the costs of primary and secondary care. 9 Assessing and addressing treatment burden has the potential to make healthcare more patient-centred, effective and efficient. 10
While there is recognition of the need to reduce treatment burden for people living with multimorbidity, there are a lack of tools to help clinicians identify people who are experiencing high treatment burden. In the UK, the National Institute for Health and Care Excellence (NICE) guidance for the assessment and treatment of multimorbidity recommends a tailored approach to care, considering treatment burden, for any adult “prescribed 15 or more regular medicines”. 11 However, such categorisations will exclude a range of individuals with high treatment burden, and burden not related to medication use.
Several patient reported outcome measures (PROMs) have been developed to assess treatment burden. 12 PROMs developed for use in research can be relatively long and often require a calculation to determine a global treatment burden score, for example, the Patient Experience with Treatment and Self-management (PETS) PROM consists of 60-questions and the brief version consists of 32 items.13,14 Such lengthy measures are unlikely to be incorporated into routine clinical practice due to time constraints. A short PROM is needed, with a single-item global measure of treatment burden, to quickly and easily identify people who most need support. Whilst a few short PROMs do exist, none are routinely used in clinical practice in the UK.
The ICAN discussion aid was developed specifically for use in clinical practice. 15 Prior to a consultation, patients are invited to list “the things that your doctors or clinic have asked you to do to care for your health” and identify (by ticking a box) whether they are “a help” and/or “a burden”. Within the consultation, clinicians are encouraged to ask one or more questions about what is on their patient’s mind and what brings them joy. A small feasibility study, conducted in the US, reported that clinicians found this easy or very easy to use in 62% of consultations and noted that further training may help address any difficulties experienced. 16 While the ICAN has potential to focus the content of a consultation, it does not provide a global score and so cannot be used to identify and distinguish those experiencing high treatment burden.
The Multimorbidity Treatment Burden Questionnaire (MTBQ) is a brief PROM that was developed and validated as part of a multicentre cluster-randomised controlled trial in the UK (the 3D Study). 17 Its development was based on a treatment burden framework informed by qualitative research. 18 The MTBQ comprises 10 questions (with three further optional questions), each requiring a response on a 5-point Likert scale. 19 Global scores over 22 indicate high treatment burden. The MTBQ demonstrated good content and construct validity, as well as internal consistency, reliability and evidence of responsiveness.19,20 It is now a widely used measure in research settings, and has been translated into multiple languages and culturally adapted for use in a range of locations.21–23 Despite its potential, it has not been incorporated into clinical practice, perhaps because of the need to calculate a global score.
There is one existing single-item global measure of treatment burden for people living with multimorbidity. 24 Respondents are invited to rate “the amount of effort [they] have to put in to manage [their] health conditions”, “On a scale of 0–10, where 0 is no effort and 10 is the highest effort you can imagine”. This measure performed moderately in its ability to distinguish between people experiencing high and non-high treatment burden, indicating further development or an alternative measure is required, especially for use in clinical practice where it may usefully inform healthcare discussions.
The aims of this study were to develop the Short Treatment Burden Questionnaire (STBQ), a novel PROM, addressing the limitations of existing measures by comprising a Global Treatment Burden Question (GTBQ) and items to identify areas of difficulty; improve its understandability and face validity; and explore patient views on how it could be used in clinical practice.
Methods
Study design and setting
We conducted a cognitive interview study within a mixed-methods study exploring treatment burden for adults (aged 18–65 years) living with multimorbidity (the Supporting People to Live Well with Multiple Long-Term Conditions: SPELL study). 25 The cognitive interviewing methods employed were think-aloud with concurrent and retrospective prompts. 26 These methods enable researchers to understand how potential users of a questionnaire understand and respond to each aspect, and identify issues that may not otherwise be apparent. 27 The think-aloud involved encouraging participants to verbalise their thoughts as they read through and answered the Short Treatment Burden Questionnaire (STBQ). Prompts were used to clarify participants’ understanding and explore their views on the PROM, as well as address the requirements of the face validity section of the COnsensus-based Standards for the selection of health status Measurement INstruments (COSMIN) checklist. 28 This manuscript has been written in accordance with the Standards for Reporting Qualitative Research (SRQR). 29
General practices in two areas of England - Bristol, North Somerset and South Gloucestershire and Greater Manchester - were invited to take part in the study. Practices were selected to achieve variation in socio-economic deprivation (as defined by the Index of Multiple Deprivation: IMD), ethnic diversity and rurality.30,31 Practices not using the EMIS health records system were excluded.
Development of the short treatment burden questionnaire (STBQ) prototype
A STBQ prototype was developed by the research team. As treatment burden is an unfamiliar term to most individuals, the concept was to include a short description of treatment burden, followed by a single Global Treatment Burden Question (GTBQ) to support the identification of individuals experiencing high treatment burden, and a tick list of different sources of treatment burden to enable those completing the measure to highlight areas of difficulty. The initial prototype was developed by PD, drawing on the validated theory-based Multimorbidity Treatment Burden Questionnaire (MTBQ) which she had previously developed, and the single-item treatment burden question, developed by co-applicant, SF.19,20,24 It was then revised through discussion with members of the research team, including academic GPs (including PD, RJ, JV), an academic public health doctor (SF), a behaviour change researcher (AK) and lay co-applicant (SC). Prior to the start of the cognitive interviews, following discussions with the wider research team and study patient and public involvement (PPI) group, a final iteration of the prototype was created.
Recruitment
Eligible patients were identified through an electronic health records search developed for EMIS. Inclusion criteria: adults, aged 18–65, with two or more long-term conditions from the 20-condition Cambridge Multimorbidity Score. 32 Exclusion criteria: diagnosis of dementia, receiving palliative care, resident in a care home and/or lack capacity to provide informed consent.
Using tools and materials provided by the research team (including a guidance document, search to run on EMIS, spreadsheet to select a random sample of participants from the output of the search and text for the invitations), each practice randomly selected 60 patients from the search results, screened this list to confirm eligibility, and sent study invitations to the first 40 eligible patients by post and/or text message. These included a copy of or link to the participant information sheet, and contact details for the research team.
Following contact, the research team checked eligibility and purposively sampled 33 to achieve maximum variation in terms of socio-economic deprivation (based on general practice postcode), and self-reported rurality, age group, gender identity, number and type of long-term conditions, employment status and carer status. While language did not restrict participation in the wider SPELL study, for the cognitive interviews we focused recruitment on those who could read and respond to the prototype STBQ, which was written in English. Consent was obtained immediately prior to the interview, which took place via videocall, telephone or in-person according to the participants preference.
Participants were offered a £25 shopping voucher for taking part in the qualitative interview.
Data collection
A cognitive interview guide was developed and piloted with input from the wider research team and PPI group. Three rounds of five cognitive interviews were conducted between July and October 2023. Data collection was stopped after the third round as few issues were being identified at this stage. Nine of the interviews were conducted by AK, a health behaviour change researcher, and six by RG, a health services and health communication researcher. Eight were conducted via videocall, six by telephone and one in-person. They lasted an average of 47 minutes (range 23–67 minutes).
Demographic data were collected through an initial, opening question. After this, participants were shown the STBQ (on paper, via email or screen sharing) and encouraged to ‘think-aloud’ while reading and answering the PROM.
27
Researchers did not interrupt participants during a ‘think-aloud’. Verbal prompts were used concurrently and retrospectively to encourage participants to continue talking and further explore their thoughts about the PROM.
26
Finally, participants were asked whether it would be useful for general practice staff to ask patients to complete the STBQ and, if collected, how practices could use the data. The interview guide was amended following the first round of cognitive interviews, to make the think-aloud instructions shorter and clearer. “How do you think it should be used?” was also added as a follow-up question. The final interview guide is shown in Figure 1. Cognitive interview guide.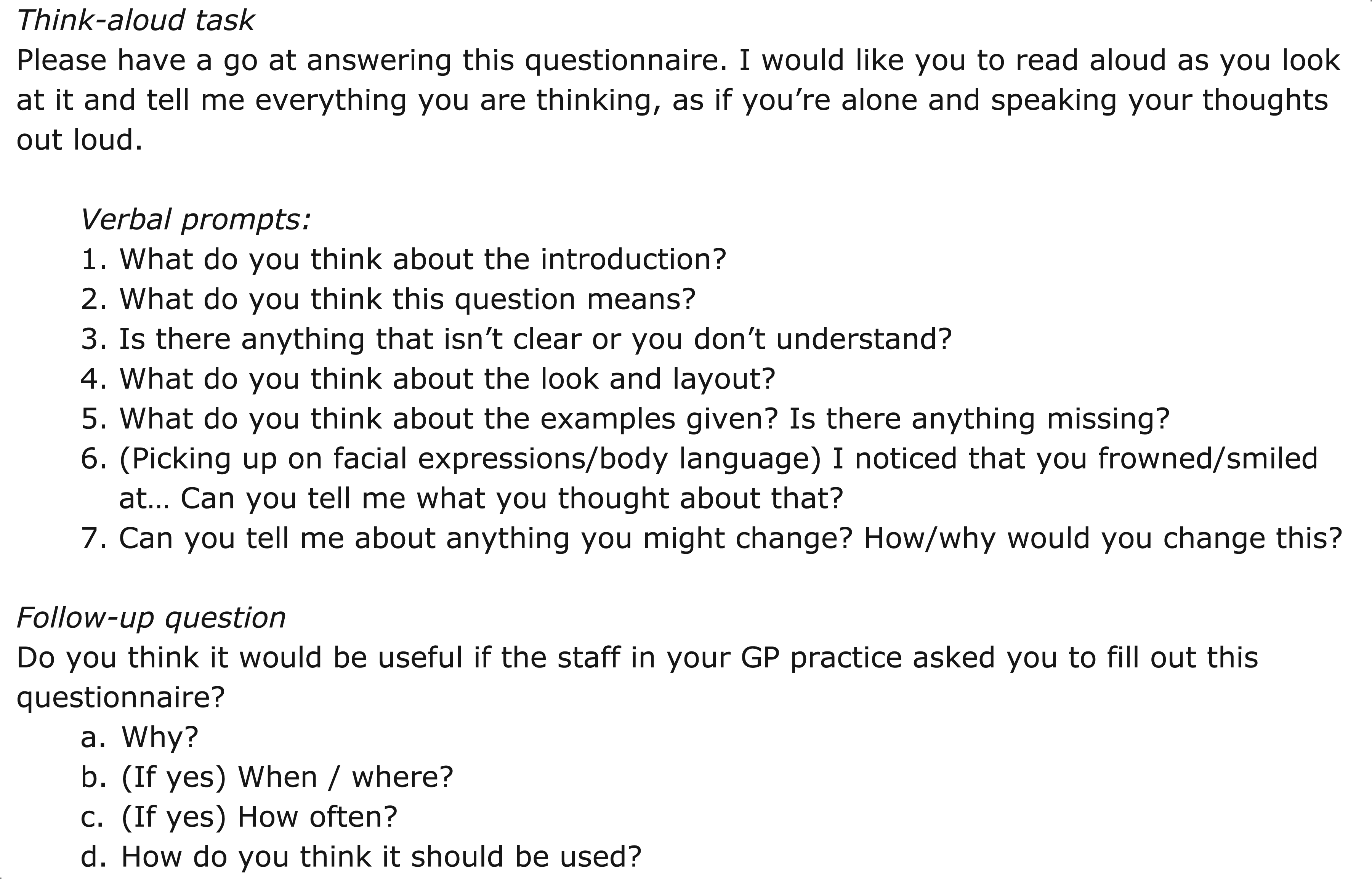
The cognitive interviews were audio-recorded and professionally transcribed verbatim. The researchers took detailed field notes, highlighting long pauses and non-verbal utterances. Where possible, they also noted facial expressions and how the participant completed the STBQ (e.g. what marks they made on the page). Alternatively, the researcher asked the participant how they completed the STBQ or, when screen sharing, asked them to explain how they would compete it and did this for them.
Data analysis
At the end of each round of cognitive interviews, all data were analysed and the PROM was modified. To facilitate rapid analysis, AK and RG listened to the audio-recordings of their respective cognitive interviews and expanded on their fieldnotes. They then summarised the data within a matrix, with columns representing participants, and rows representing different components of the STBQ, including overarching aspects such as language and layout (Supplemental material 1).
Initially, RG and AK reviewed the data and highlighted all potential issues with the STBQ, including instances where aspects had been missed or interpreted in a different way than intended. Potential issues were discussed with other members of the research team (PD, RJ) to determine whether modification was needed, more data were required or changes were likely to introduce more problems than they resolved. 34 Interview transcripts were checked and anonymised, then reviewed to determine whether anything had been missed, and to extract and add direct quotes.
All proposed changes were discussed with the wider research team and PPI group. This included seeking input and a deciding vote in instances where there was a lack of consensus among the team. Agreed changes were categorised into five outcome types: 1) item-specific wording, 2) questionnaire objectives, 3) ordering/interactions between questions, 4) reduction in length/burden, and 5) visual layout. 27 The STBQ was modified in line with the decisions made, prior to the next round of interviews. The final version was included in the survey component of the mixed-methods SPELL study, reported separately. 35
Patient and public involvement
A PPI group, consisting of eight people with lived experience of multimorbidity, was established at the outset of the SPELL study. The members of this group contributed to the development of the research questions, design of the study and creation of study documents including the initial, interim and final versions of the STBQ.
Ethics
The SPELL study received a favourable ethical opinion from the London – Westminster Research Ethics Committee (REC reference 22/PR/1750) on February 09, 2023. For in-person interviews, all participants provided written informed consent prior to participating. For remote interviews, informed consent was obtained verbally before participation, with the researcher reading the consent form out loud and participants responding to each statement. Verbal consent was audio-recorded. Consent included agreement to take part in the study and for anonymised quotes to be published.
Results
Participant characteristics
Participant demographic characteristics (N = 15).

Abbreviations: LTC = long-term condition, IMD = Index of Multiple Deprivation.
All data, except ‘IMD decile for general practice’, self-reported by the participants.
Similar conditions were grouped and counted together e.g. anxiety and depression.
Improving the understandability and face validity of the Short Treatment Burden Questionnaire (STBQ)
Summary of changes to the Short Treatment Burden Questionnaire (STBQ) following each round of cognitive interviews.

The text in brackets shows the cognitive interview round, participant gender and participant ID, for example, 2F06 refers to participant 06 who is female and took part in the second round of cognitive interviews.
In each round of cognitive interviews, the changes, or outcomes, related to ‘item-specific wording’ (10/17) and ‘ordering/interactions between questions’ (4/17). For the first round only, they also concerned the ‘visual layout’ (2/17) and ‘questionnaire objectives’ (1/17).
Round one - layout and instructions
Following round one, changes were made to the layout of the STBQ, to improve readability (change 1) and make it clear that there were two separate questions (changes 2, 3). To further these goals, the research team initially agreed on two additional changes: a) increase the font size of the questions relative to the response options, and b) add more space between the questions and response options. These were tried but ultimately not implemented as the research team agreed they did not improve the layout.
Changes were also made to encourage questionnaire respondents to focus on their actual rather than hypothetical experience (change 4) and provide space for respondents to provide further information (change 8). These were achieved by adding ‘in the last three months’ to the second, list question and adding a third, open-ended question (the wording of which was revised in round 2 - change 14).
Round two - order and wording of response options
In round two, following the first set of modifications, participants read and responded to each STBQ question separately. However, the list of response options for the second, list question was considered disjointed. The response options were originally presented in alphabetical order, in line with questionnaire development guidance. 36 This appeared to limit participants ability to understand the difference between similar items, such as ’Remembering to take my medicines’ and ‘Taking my medicines’. As such, the response options were re-organised so similar items were presented next to one-another (change 9).
Across the first two rounds, participants questioned the meaning of some response options in the second, list question and/or interpreted them in ways that had not been intended (changes 5, 6, 7, 12, 13). The wording of these items was revised to reduce ambiguity. One item was changed following both rounds one and two. ‘Seeing different healthcare professionals’ was initially interpreted by some as seeing any health professional, rather than the intended meaning of several different health professionals. The revised wording of ‘Seeing lots of health professionals’ helped to resolve this issue but further cognitive interviews highlighted that the term ‘seeing’ was understood to mean in-person. Thus, the wording was changed again, to ‘Speaking to lots of different health professionals’.
Round three - instructions and response options
The introduction to the STBQ was revised following rounds two and three. This text, explaining the concept of treatment burden and setting the context for the questions, was often not read (change 15). Feedback from participants who did read it was that the wording ‘can be hard work’ was leading (change 10). Thus, the text ‘Please read BEFORE answering the questions’ was added to the start of the introduction, in bold, and the existing text was changed to ‘can sometimes be hard work’.
Following round three, the research team explored the pros and cons of changing the response options for the first, Global Treatment Burden Question (GTBQ), from a 5- to 4-point Likert scale. This was because the middle option, ‘Quite hard’, was the most common response option and, despite an earlier change to the wording of these response options (change 11), there was a lack of a clear difference between ‘A bit hard’/‘A little hard’ and ‘Quite hard’. Following discussion with co-investigators and public contributors, the 5-point Likert scale was retained, as it was agreed that having more response options typically ensures a better distribution of data. Instead, to address the issues with this question the response options were amended from ‘A little hard’ to ‘Slightly hard’, and ‘Quite hard’ to ‘Moderately hard’. This wording reflects that used in other 5-point Likert scales, and these terms were considered more distinct from one another than those previously used (change 16).
The complexity of the language used in the STBQ was discussed in the cognitive interviews and in meetings with the research team and PPI group. Most interview participants reported the STBQ was easy to understand. One participant, with a learning difficulty, faltered and repeated some words while reading the STBQ but stated that, overall, they understood the PROM. As such, no further changes were made to the language.
Finally, informed by a study led by PD to further develop and validate the Multimorbidity Treatment Burden Questionnaire (MTBQ), which found that ordering responses from ‘Extremely difficult’ to ‘Not difficult’ did not reduce the skewness of the data, the order of the response options to the Global Treatment Burden Question (GTBQ) were reversed (change 17).
20
The initial and final versions of the STBQ, including the GTBQ, can be seen in Figure 2. Short Treatment Burden Questionnaire (STBQ) before and after the cognitive interviews.
Patient views on how the Short Treatment Burden Questionnaire (STBQ) could be used in clinical practice
Overall, it was considered a good idea for general practice staff to ask registered patients to complete the STBQ. It was seen as a ‘conversation starter’ that could both encourage patients to mention things they may not otherwise bring up, and help staff understand the patient experience.
The STBQ was considered useful in the context of individual patient care and consultations, providing a basis for adjusting care plans to make things easier for patients, and as a means of providing practice-level feedback, to inform what services are offered. Such practice-level feedback could be provided anonymously to reduce patient anxiety that their responses would be seen as critical, and that this would negatively impact their future care. “…if something was actually happening in the background to actually help after people ended up filling these out, then it quite possibly could make a difference. Knowing is half the battle.” (2M07)
Some participants questioned the usefulness of the STBQ in general practice, suggesting that their healthcare providers were too busy and lacked the resources to take account of the information. Additionally, some aspects of treatment burden, such as availability of medications, were seen as outside of the control of general practice. “…the GP - to be honest, I don’t think they care about a lot of this stuff. I think they’re either so busy or so focused that they’re not really interested about whether I can get my medication or not…” (1M02)
In relation to the practicalities of completing the questionnaire, participants suggested making it available in different formats and different ways, such as on paper or online, sent by post, email or text, or even by telephone depending on individual patient preferences and digital literacy.
Participants acknowledged that there was no time to complete the STBQ within an appointment but it could be completed before or after. It could also be handed out by reception staff at other times, for example, when a patient is booking an appointment or ordering a prescription.
Participants views differed on how often the STBQ should be completed, with some suggesting every 3–6 months, particularly as the questionnaire focuses on people’s experiences over the last 3 months. Others suggested once or twice a year, or when joining the general practice and every 2–3 years thereafter. While treatment burden was seen as something that will not change overnight, the STBQ itself was not considered burdensome and could be used to check for improvement. “Obviously, you do your first one, you’re not gonna change it overnight, but if you do it like three to six months, you can then compare from before to see whether improvement has been made from people’s original answers.” (1F01)
Discussion
The Short Treatment Burden Questionnaire (STBQ) is a novel measure of treatment burden, comprising a Global Treatment Burden Question (GTBQ) and items to identify areas of difficulty. To improve the understandability and face validity of this patient reported outcome measure (PROM), we conducted cognitive interviews with adults (aged 18-65) with multimorbidity, recruited from general practices in socio-economically diverse areas. We also explored participants’ views on the STBQ being used in clinical practice.
The STBQ demonstrated face validity and, after modification, participants found it easy to understand and complete. Participants suggested the STBQ could be used in general practice to inform individual patient care and service improvement. However, some voiced concerns that general practice staff lack the time and resources to take account of the information this PROM would provide.
The final version of the STBQ consists of three questions. The first is the single-item GTBQ, which provides an overall rating of treatment burden on a 5-point Likert-scale. Text response options are accompanied by visual representations, in the form of smiling to distressed faces, to support understanding. The second question lists 13 different aspects of treatment burden and invites respondents to tick those they have found hard in the last three months. A final, free-text question provides the respondent with space to elaborate on any of the above. The PROM fits on a single side of A4.
Participants saw the STBQ as a tool to help start conversations about treatment burden. They thought it would be useful to complete the STBQ at least annually and perhaps every six months to see whether things were improving. The brevity and simplicity of the PROM would make it suitable for use in clinical practice - either at the individual patient or practice level - to quickly understand the extent to which a person or group of people is/are experiencing treatment burden, and highlight areas for further evaluation and intervention. However, despite its brevity, some participants wondered whether their primary care providers had time to have conversations about treatment burden.
Some participants expressed concern that their responses to the STBQ would be taken as criticism so would only be happy to complete this anonymously. Such use of the STBQ, at a general practice rather than individual level, was seen as potentially useful for informing service improvement and development. Alongside the STBQ, the research team propose to develop an implementation guide, to highlight the different ways in which practices could use the STBQ, how they might alleviate patient concerns, and how they might support any patients who struggle to complete the STBQ independently.
As the STBQ was being developed, an alternative brief measure of treatment burden, with the potential to be used in clinical practice, was published. PETS-Now 37 is a web-based, electronic point-of-care tool, adapted from the validated 60-item PETS. 14 When completing PETS-Now, respondents are asked to select one of eight domains of treatment burden – the one causing the most concern - then complete a checklist related to that domain. This is designed to generate discussion between patients and their healthcare providers. Most study participants reported that this web-based measure was easy to complete, although some struggled with the technology and missed the full range of buttons depicting survey options. Despite this, there was a clear appetite for use of such a measure, with 98% of the patients participating in the pilot expressing willing to use a treatment burden measure in future routine healthcare appointments.
The results of the PETS-Now development studies reflect our findings that there is a desire among patients to incorporate a brief measure of treatment burden into clinical practice.14,37 One advantage of the STBQ is that it includes a single-item Global Treatment Burden Question (GTBQ). This can be completed as a standalone measure to identify patients with high treatment burden. Additionally, the STBQ allows respondents to identify multiple areas of concern. It can be completed in a variety of ways, including on paper, making it easier for people with limited digital literacy. However, it may need to be further simplified to enable all individuals to complete the full PROM independently.
Strengths and limitations
The STBQ was developed from the Multimorbidity Treatment Burden Questionnaire (MTBQ), a PROM that has been extensively validated and translated.19,20 The STBQ was developed and subsequently iterated using rigorous cognitive interviewing methods, and with public contributor input throughout. It is recognised that multimorbidity is more prevalent among people living in deprived areas, and that people aged 18-65 may experience higher treatment burden than those in older age groups. Few studies of treatment burden in multimorbidity have focussed on this age group. Our interview sample was varied in age, gender, number of LTCs, and included people from general practices in areas of socio-economic deprivation.
The cognitive interviews were conducted in the initial stages of the wider SPELL study, so the modified STBQ could be included within and validated through a subsequent survey. While attempts were made to recruit a varied sample, at this early stage, the pool of potential participants was relatively small. Thus, the sample was not varied in all respects. Most participants were White British (87%) and did not require a carer (87%). As such, and as the SPELL study focused on people with multimorbidity and excluded people over the age of 65, further work is required to explore its validity in other groups, including older adults. Additionally, while language did not restrict participation in the wider SPELL study, for the cognitive interviews recruitment focused on those who could read and respond to the prototype STBQ, which was written in English. However, the sample was well distributed across urban, rural and geographical locations and recruited from general practices in areas with different levels of deprivation.
Conclusions
Robust qualitative methods were used to develop a novel measure of treatment burden. The Short Treatment Burden Questionnaire (STBQ) demonstrated face validity, and people with multimorbidity found it relatively easy to use. Further work has been undertaken to validate the Global Treatment Burden Question (GTBQ; part of the STBQ) 35 and guidance will be produced to highlight the ways in which the STBQ can be used to support patient care. The STBQ has a range of potential uses in healthcare settings and research, pending further validation and feasibility testing.
By identifying people experiencing high treatment burden, and the areas in which they are having difficulties, healthcare services can offer support to meet their needs, and models of care can be developed that do not exacerbate burden. Methods to identify people within routine clinical practice, such as the STBQ, are essential.
Supplemental material
Supplemental Material - Development of the short treatment burden questionnaire (STBQ) including a global treatment burden question (GTBQ): Cognitive interviews with adults living with multimorbidity
Supplemental material for Development of the short treatment burden questionnaire (STBQ) including a global treatment burden question (GTBQ): Cognitive interviews with adults living with multimorbidity by Rebecca Goulding, Polly Duncan, Anastasiia G. Kovalenko, Chloe Gamlin, Simon Chilcott, Simon D. S. Fraser, Jose M. Valderas, Rachel Johnson in Journal of Multimorbidity and Comorbidity.
Footnotes
Acknowledgements
The authors would like to thank the other members of the Supporting People to Live Well with Multiple Long-Term Conditions (SPELL) research team who were involved in initial discussions about and helped develop the first prototype of the Short Treatment Burden Questionnaire (STBQ): Prof Chris Salisbury, Dr Michael Lawton and Dr Thomas Blakeman. The authors acknowledge the contribution of all members of the patient and public involvement (PPI) group for the SPELL study, to the design of the study and study materials, and the design and modification of the STBQ. They would also like to thank the general practice staff who supported recruitment to this study and everyone who took part.
Ethical considerations
This study was approved by the London – Westminster Research Ethics Committee (REC reference 22/PR/1750) on February 09, 2023.
Consent to participate
For in-person interviews, all participants provided written informed consent prior to participating. For remote interviews, informed consent was obtained verbally before participation, with the researcher reading the consent form out loud and participants responding to each statement. Verbal consent was audio-recorded.
Consent for publication
Informed consent for publication of anonymised quotes was obtained from all participants.
Author contributions
RJ, PD, SF, JV designed the SPELL study. AK, SC and RG contributed to protocol development. AK and RG collected and summarised the data. RG, AK, PD and RJ interpreted the results. RG drafted the manuscript. All authors reviewed and revised the manuscript and approved the final version.
Funding
This work was supported by the NIHR School for Primary Care Research [grant reference number 564].
Declaration of conflicting interests
Dr Polly Duncan developed and validated the Multimorbidity Treatment Burden Questionnaire (MTBQ).
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available via the corresponding author on reasonable request.
Supplemental material
Supplemental Material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.